1. Introduction
Numerous countries have begun prioritizing cost-effectiveness when assessing new medical technologies to more effectively allocate limited health resources given the rising public sector costs associated with an aging population, increased prevalence of patients with chronic diseases, and the introduction of costly new drugs [
1,
2,
3]. It is often difficult to determine reimbursement prices for newly developed drugs when the cost-effectiveness of these drugs in clinical practice remain unclear [
4,
5]. While pharmaceutical companies are demanding a premium to recover their development costs and fund ongoing investments in research and development (R&D), patients are requesting rapid reimbursement decisions to improve their access to new drugs [
6]. Evidence-based evaluation is often difficult for costly new drugs with low demand and no alternatives (this is particularly evident for anticancer drugs and drugs for rare diseases). Therefore, listing new drugs under the public health insurance system without evaluating them can be criticized as a waste of financial resources, whereas designating the drugs as non-reimbursable can lower patient access to them [
7,
8]. Although recently developed drugs, including cell and gene therapy drugs, have optimal beneficial effects and minimal side effects, their timely delivery can be challenging; there may also be insufficient evidence regarding their efficacy because of the difficulties in recruiting sufficient participants for clinical trials. Moreover, because of the high prices of such drugs, decisions about reimbursement are made while considering a variety of factors, including incentives to improve treatment methods, financial resources available for health insurance, and access to treatment methods [
9,
10,
11,
12].
Many countries have begun to employ risk-sharing agreements as a new approach to improve patient access to new drugs. Under these agreements, pharmaceutical companies and insurance payers mutually agree to share the financial burdens or uncertainties regarding clinical outcomes [
3,
13,
14,
15]. Countries such as Australia, Great Britain, and Canada have separate organizations or expedited assessment pathways for costly anticancer drugs during the technology assessment and reimbursement decision-making processes [
16,
17,
18,
19]. Furthermore, many countries (e.g., Australia, Belgium, Italy, and Great Britain) also possess various drug funds for rare diseases or anticancer drugs to improve patient access to novel drugs [
20,
21,
22,
23]. Despite these efforts, many countries have failed to provide possible alternatives for a more comprehensive assessment method that can satisfy all concerned parties.
South Korea implemented a positive listing system policy on 31 December 2006 to allocate financial resources more effectively for medications. Under this new system, only cost-effective drugs can be reimbursed at a premium. The policy also required evidence-based evaluation of new drugs and improved the transparency and consistency in the decision-making process [
24,
25]. However, such evidence-based evaluations have lowered access to novel drugs which are essential to patients but cannot be subjected to a cost-effectiveness analysis because of challenges in producing clinical evidence and high costs which may not necessarily be reimbursed by insurance [
26]. Listing of these drugs to improve patient access would require additional financial resources, thus necessitating the introduction of new policies, such as risk-sharing agreements. This study aims to review the policies currently being implemented for improving patient access to novel drugs by including new drugs under the health insurance system in South Korea and to discuss their outcomes and relevant issues as well as to recommend future policy prospects.
1.1. Pharmaceutical Insurance System in South Korea
1.1.1. Drug Expenditures in South Korea
Public health expenditure in South Korea accounts for 7.4% of its gross domestic product (GDP). In general, health expenditure increases as a function of income, which means that Organization for Economic Co-operation and Development (OECD) nations with high GDPs per capita tend to have high health expenditures. When calculated in relation to purchasing power parity, the healthcare expenditure per person in South Korea is
$2535, which is lower than the OECD average of
$3848 (as of 2015); in fact, South Korea is ranked 25th out of the 35 OECD nations, and therefore South Korean health expenditure is not very high. In contrast, drug expenditures in South Korea for 21.4% of the total healthcare expenditure, which is higher than the OECD average of 16.2%; this puts South Korea as the 6th highest in this category among OECD countries [
27]. During South Korea’s decision-making process involving budget allocation, the proportion of drug expenditures constituting the total health budget in comparison with the proportion of drug expenditure of healthcare expenditures in other OECD countries is used as an important index for determining the direction of public health insurance policy. However, use of this proportion is controversial because it can be influenced by healthcare expenditures.
1.1.2. Listing System for the Price of New Drugs in South Korea
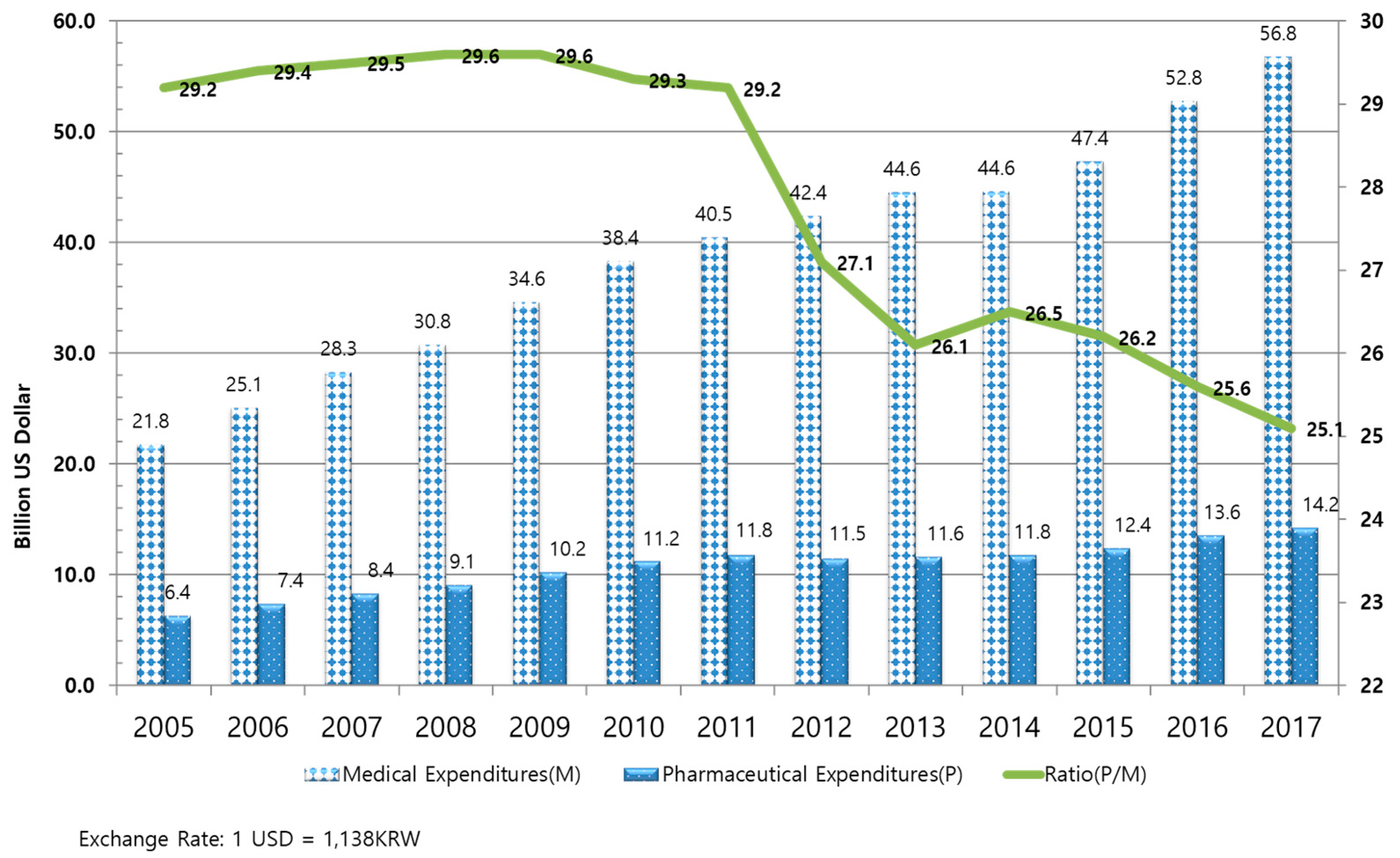
In South Korea, when listing new drugs for coverage under public health insurance, a negative list system had been implemented until the application of a positive listing system on 31 December 2006. When the financial deficit for public health insurance previously peaked in 2001, drug expenditure accounted for 23.5% of total health expenditure. However, this proportion increased to 29.2% in 2005, thereby suggesting issues in drug expenditure management (see
Figure 1).
The South Korean government adopted the positive listing system for new drugs in order to allow for more rational management of drug expenditure. Since then, only cost-effective drugs have been listed in the national drug formulary. Moreover, the price–volume agreement system was implemented to manage drug use. Under this system, the prices for drugs whose use increased by 30–60% were reduced by up to 10% according to an agreement between the National Health Insurance Service (NHIS) and the pharmaceutical companies [
24,
28].
The Ministry of Health and Welfare oversees the listing of new drugs as reimbursable drugs. When pharmaceutical companies submit the price of a new drug to the Health Insurance Review and Assessment (HIRA), a Drug Reimbursement Evaluation Committee (DREC) of HIRA evaluates the cost and clinical effectiveness of that drug. For drugs determined to be reimbursable, the NHIS and pharmaceutical companies negotiate drug prices after estimating the financial impact of the addition of a new drug. When the prices are determined, the Health Insurance Policy Deliberative Committee, which serves under the Ministry of Health and Welfare, reviews and approves the prices, after which the drugs are listed as reimbursable drugs [
28] (please see
Figure 2).
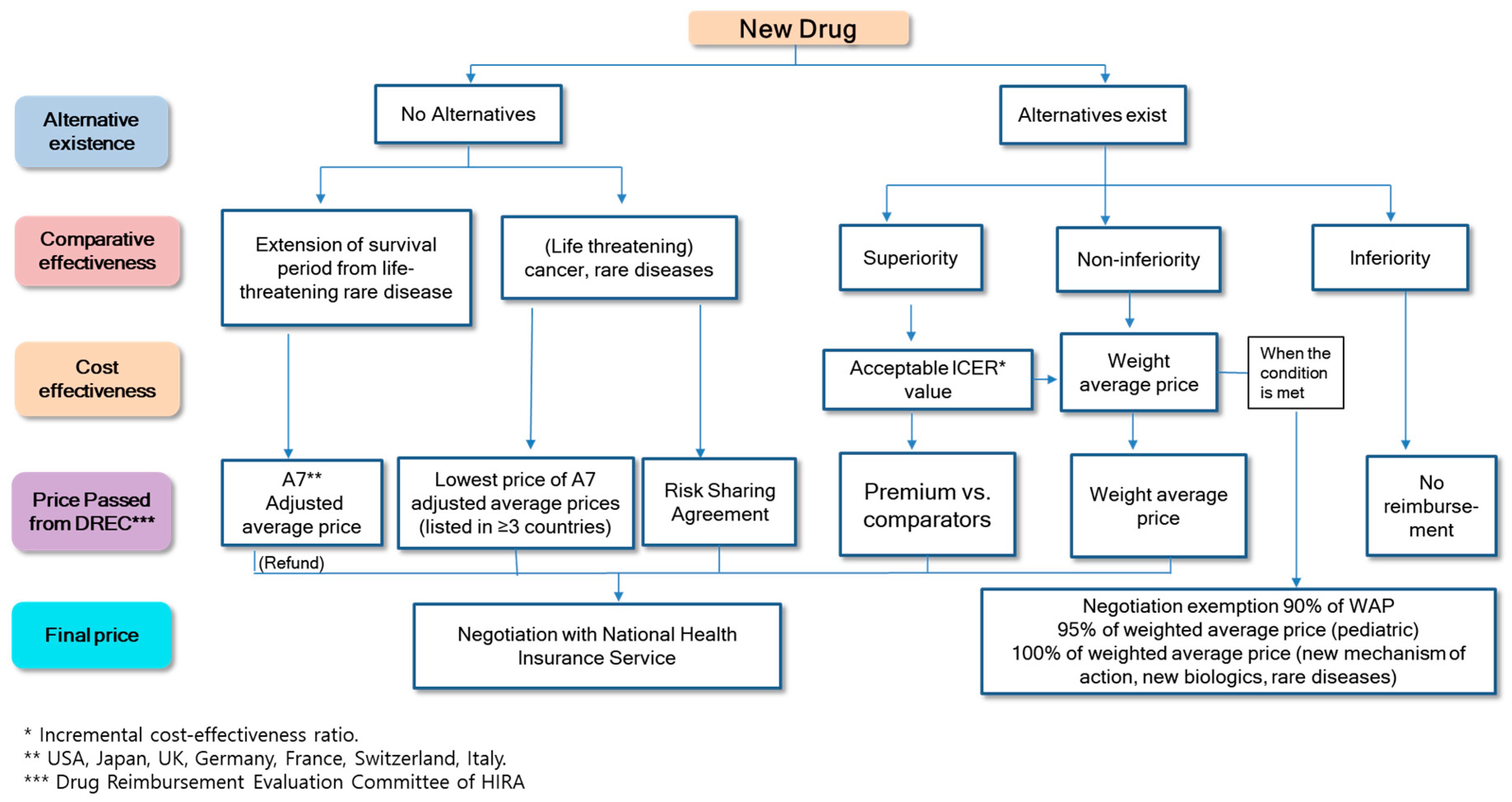
For the evaluation of new drugs, the availability of alternative drugs is initially considered. When alternative drugs are available, the clinical effectiveness of the new drug is evaluated in comparison with these alternative drugs and determined to be non-inferior, superior, or inferior in efficacy. If the new drug is not found to be superior in terms of clinical effectiveness in comparison to the alternative drugs, the drug prices are, in principle, negotiated below the weighted average price of the alternatives for reimbursement. However, the prices of drugs are determined without negotiation if pharmaceutical companies accept 90–95% of the weighted average price of the alternative drugs.
If the drugs are found to be superior to their alternatives, the drug prices are determined based on a cost-effectiveness evaluation. Even when drugs are found to be cost-effective, reimbursement cannot be made unless a financial agreement is reached after negotiation with the NHIS. Drugs considered inferior in comparison with their alternatives remain as non-reimbursable drugs. For new drugs with no available alternatives, drugs that are determined to be essential for treating of patients (thereby classified as essential drugs) by the drug review committee of HIRA are exempted from a cost-effectiveness evaluation. The prices are determined by negotiating with the NHIS based on the prices in A7 countries (i.e., U.S., Japan, Great Britain, France, Germany, Switzerland, and Italy) (see
Figure 3).
2. Ways of Improving Access to New Drugs in South Korea
In the current South Korean positive listing system, even drugs that are essential for patients may become non-reimbursable if they fail to demonstrate their cost-effectiveness or if the NHIS and pharmaceutical companies fail to reach a financial agreement. It can be difficult for anticancer drugs or orphan drugs to statistically demonstrate their clinical value or cost-effectiveness because of their high costs. Even if drugs are found to be cost-effective, they may remain non-reimbursable if no financial agreement is reached with the insurance payer. In fact, among the drugs evaluated as non-reimbursable between 2007 and 2012, 10 new drugs for advanced-stage or rare diseases became non-reimbursable despite the fact that they were clinically useful and lacked alternatives [
29]. Although essential drugs are typically exempted from cost-effectiveness evaluations, the criteria for essential drugs are very specific; consequently, the system was not effective for improving patient access to these new drugs. Accordingly, the South Korean government has introduced new tracks for a risk-sharing agreement as well as a cost-effectiveness analysis waiver to further improve patient access to new drugs.
2.1. Designation as Essential Drugs
Drugs are designated by the Drug Review Committee of the HIRA as essential for treatment if it meets all of the following criteria [
30]: (a) it has no alternatives (including alternative drugs and treatment methods); (b) it is used for treating serious life-threatening conditions; (c) it is used to treat small patient groups, such as those with rare diseases; and (d) it demonstrates significant improvement in clinical efficacy or survival.
When a drug is designated as essential for treatment, it is exempted from a cost-effectiveness evaluation, and the price for reimbursement is determined by negotiating with the NHIS based on the prices established in the A7 nations. If a pharmaceutical company does not agree to the price of a drug suggested by the NHIS, the drug is not listed as non-reimbursable. In this instance, the reimbursement adjustment committee under the Ministry of Health and Welfare reviews the case, and they may ultimately list the drug as reimbursable. Therefore, listing for reimbursement is considerably easier for essential drugs. Thus far, 10 essential drugs have been listed (see
Table 1).
2.2. The Risk-Sharing Agreement System
The South Korean government implemented the risk-sharing agreement system in December 2013. Under this system, the government and pharmaceutical companies share the uncertainties regarding the clinical outcomes of new drugs and their influence on the budget, thereby making it easier for drugs to be listed. This risk-sharing agreement system was implemented for adhering to the positive reimbursement of cost-effective drugs while also improving patient access to new drugs and promoting the development of the pharmaceutical industry; it is particularly relevant for cases involving costly anticancer drugs and orphan drugs that lack alternative drugs or treatments.
A drug is eligible for a risk-sharing agreement if it satisfies the following criteria [
30]: (a) it should either be an anticancer agent or be used to treat serious, life-threatening conditions and should also lack alternatives or clinically equivalent drugs or treatments; and (b) the drug review committee concludes that further agreement on additional conditions is necessary after considering the severity of the disease, social influences, and other influences on public health. Even when drugs are eligible for a risk-sharing agreement, they are still evaluated according to the same procedures as other drugs. The specifics of the risk-sharing agreement are reflected in the cost-effectiveness evaluation, and the agreement is only reached during the drug price negotiation phase prior to its listing under the public health insurance system.
There are four types of risk-sharing agreements available: refunds, expenditure caps, utilization caps per patient, and refund/expenditure caps. Thus far, 33 drugs have been considered eligible for risk-sharing agreements, and most were finance-based agreements in the form of a refund or expenditure cap, in which an agreement on the refund rate was reached and drug prices corresponding to the refund rate were collected back ex-facto (see
Table 2 and
Table 3).
2.3. Cost-Effectiveness Analysis Waiver System
Although the risk-sharing agreement system was implemented to improve patient access to new drugs, some drugs are not eligible under this system because they are not considered cost-effective. In particular, evidence of cost-effectiveness could not be generated for anticancer agents or orphan drugs [
31]. To overcome this shortcoming, the cost-effectiveness analysis waiver system was introduced in February 2015. This system allows drugs that do not satisfy the criteria for essential drugs to be exempted from a cost-effectiveness evaluation if the drug satisfies the strict criteria of the cost-effectiveness analysis waiver system.
For cancer or orphan drugs that are clinically essential but cannot be proven to have a significant improvement in clinical outcomes, only those that are listed in at least three A7 nations can be included (after negotiation with the NHIS) without a cost-effectiveness evaluation. Since September 2016, all new drugs listed under the cost-effectiveness analysis waiver system are required to reach an expenditure cap risk-sharing agreement with the NHIS (i.e., the pharmaceutical companies share the financial risks of the listed drugs). Thus far, 15 new drugs have been listed under the cost-effectiveness analysis waiver system, and 11 of them have an expenditure cap risk-sharing agreement (see
Table 4).
3. The Impact of Policy on Improvement of Patient Access to New Drugs
Lowering patients’ cost-sharing rates (e.g., 5% for cancer and 10% for rare diseases) can improve patients’ access to new drugs; however, it can also lead to unintended moral hazards [
33]. Furthermore, because there is a copayment cap for reimbursable treatment, the maximum copayment per patient cannot exceed an annual limit which is determined based on income (i.e., 1.21–5.09 million Korean won (KRW) which equates to U.S.
$1,052–4,426).
Because patients need to pay out-of-pocket for non-reimbursable, it is difficult for patients with cancer or rare diseases to receive treatments with new drugs, which are not listed on the national positive listing formulary because of their high costs. It is imperative to list new drugs on the national drug formulary to reduce patients’ copayment burden and improve their access to these new drugs. However, reduction in the cost-sharing rates inevitably leads to increases in national healthcare budget. It is necessary to continuously monitor the effects of such policies on the financial resources available to ensure stable management of the health insurance system.
3.1. The Effects of Policies to Improve Patient Access
The Korean government introduced policies such as listing essential drugs, a risk-sharing agreement, and a cost-effectiveness analysis waiver track to improve patients’ drug access. As of 2017, a total of 15,860 patients have taken advantage of early access to new drugs through these policies, and this number is expected to continuously increase. Total savings by patients amounted to nearly 341 billion KRW; in essence, each patient paid 21 million KRW less as part of copayments compared to what would have been paid without these policies (see
Table 5).
3.2. The Influence of Policies Aimed at Improving Patient Access to New Drugs on the Financial Resources of Health Insurance
When new drugs are listed as part of the health insurance system, patients’ cost-sharing rates are lowered because majority of the costs are paid by the public health insurance system. In 2017, 62.6 billion KRW were claimed for essential drugs, whereas 260 billion KRW and 39.6 billion KRW were claimed for drugs listed under the risk-sharing agreement system and for cost-effectiveness analysis under the waiver system, respectively. The expenditures are rapidly increasing each year, such that these drugs are thought to exert significant influence on the financial resources available for health insurance (see
Table 5). Most of the drugs which have significant government financial burdens are listed under the refund agreement of the risk-sharing agreement system. Therefore, based on the assumption that the refund risk-sharing agreements were made for refunds of 30–50%, at least 78–130 billion KRW would have been collected through paybacks. Conversely, drugs listed under the cost-effectiveness analysis waiver system were often listed under the expenditure cap risk-sharing agreement to control financial risks; thus, their influence is comparatively limited. In 2017, the claimed expenses for drugs listed under the essential drug, risk-sharing agreement, and cost-effectiveness analysis waiver policies accounted for only 0.4%, 1.6%, and 0.2% of the total drug expenses, respectively; therefore, currently, they are not significant threats to the financial resources of the public health insurance system.
4. Evaluation of the Policies by Stakeholders
4.1. Patients
Patients with serious diseases argue that the time required to list new drugs should be expedited and the listing rate of new drugs should be increased to improve patient access to new drugs [
34]. They claim that very few new anticancer drugs are listed under the South Korean health insurance system as compared to the health insurance systems of other advanced countries which makes access to new drugs more difficult. Although many new drugs that were previously non-reimbursable have now become reimbursable under the risk-sharing agreement and cost-effectiveness analysis waiver systems, patients argue that many innovative drugs, including newly developed cell therapy drugs and certain drugs for infectious or rare diseases, should be made eligible under either of these systems to improve drug access.
4.2. Insured Persons
Patient advocacy groups agree with the need to increase the reimbursement for advanced cancer and orphan drugs. These groups are comprised of people who pay health insurance costs and monitor whether the government manages health insurance funds appropriately and transparently. They act as vital decision makers in promoting health insurance policies that may need significant financial resources. However, the patient advocacy groups have raised concerns about how listing expensive drugs can induce financial burden and argue that expanding existing systems to improve patient access (i.e., the risk-sharing agreement and cost-effectiveness analysis waiver systems) without thorough preparation for the potential problems in doing so—in particular, problems related to the transparency of drug expenditure and indeterminate clinical efficacy—would only benefit multi-national pharmaceutical companies. The advocate groups have noted that certain expensive anticancer drugs may have questionable clinical efficacy and that patients may expect too much from these drugs because they have not been provided with a detailed explanation regarding the actual drugs’ efficacy or effectiveness.
4.3. Pharmaceutical Companies
The pharmaceutical industry argues that South Korea’s complicated procedure for listing drugs and excessively low drug prices restrict competitiveness in the industry. Although it views improved access to new drugs through the various abovementioned policies (e.g., risk-sharing agreement system) as a positive outcome, the pharmaceutical industry still advocates for further improvements in these systems. Many companies claimed that since HIRA requested much lower prices for drugs than the prices established in other countries, they gave up listing the drug in the national drug formulary. Similarly, the excessive government control on drug prices may cause new innovative drugs to be non-reimbursable in South Korea; again, companies argue that this would lower not only patient access to advanced care but also competition in the industry due to low interest in drug development. The pricing policy should be balanced between pricing new medications appropriately in consideration of a national drug budget and allowing for patients’ access to new medication.
Moreover, pharmaceutical companies argue that the scope of application of the essential drug, risk-sharing agreement, and cost-effectiveness analysis waiver systems, which are intended to improve patient access to new drugs, is limited and that the manner in which the systems are currently being implemented does not reflect the intended goal of these systems; therefore, improvements including the expansion of the application scope are necessary [
35]. Although the risk-sharing agreement system applies to drugs without alternatives, it still requires a cost-effectiveness evaluation; in addition. Furthermore, because most drugs under the risk-sharing agreements are also a part of the refund agreement, the companies claim that the system should be expanded to include more varied types of agreements.
4.4. Insurance Payer (Government)
The government recently reported that patient access to new drugs, particularly to new anticancer drugs, has greatly improved through numerous efforts. According to the government’s analysis conducted between 2014 and 2016 regarding the time required to list new drugs in the national formulary, new drugs without anticancer activity were listed after 269 days of the initial application, while new anticancer drugs were listed after 348 days of the application’s submission. Therefore, more time is needed for listing new anticancer drugs than that required for other new drugs, presumably because anticancer drugs have more issues related to risk-sharing agreements and cost effectiveness studies as opposed to other classes of new drugs. The South Korean government has sought to decrease the listing time of new anticancer drugs to 240 days. Moreover, the listing rate of new anticancer drugs (i.e., the percentage of drugs that were listed among all drugs applied for listing) increased from 43% between 2008 and 2013 to 53% between 2014 and 2016, and the number of listed drugs increased from 3.5 drugs per year between 2008 and 2013 to 11 per year between 2014 and 2015. Thus, the government has deemed the policies directed towards improving access to new drugs as effective. The government is further striving to improve the risk-sharing agreement and cost-effectiveness analysis waiver systems to further optimize the listing rates.
The argument put forward by the pharmaceutical industry—that the prices for new drugs are lower in South Korea than in other countries—has been countered by the South Korean government; the government states that there are various discount or refund agreements hidden behind the listed prices in other countries. Furthermore, because the South Korean government views the listed prices in other countries as an inaccurate reflection of the actual drug purchase price after adjustments (i.e., post-rebate), they determine drug prices according to the prices of available alternatives and the results of cost-effectiveness analyses rather than the prices adopted in other countries. Patient access to new drugs and industrial development can suffer if innovative new drugs essential for patient treatment are not listed in the national drug formulary or if there is a delay in listing such drugs, thus, the government is willing to develop more flexible regulations for the listing of new drugs as well as implement a more thorough post-listing management strategy [
36,
37].
5. Discussion
In 2017, the South Korean government announced a proposal to expand the coverage of medical services and drugs, which involved providing reimbursement for all currently non-reimbursable drugs. Under this system, reimbursement is provided if a certain level of cost-effectiveness is achieved, but different copayment rates are applicable depending on the disease characteristics and patients’ needs. The system aims to relieve financial burdens by increasing patients’ copayment rates for drugs whose cost-effectiveness has not been verified while also increasing patient access to new drugs. For example, instead of the current rate of 5% copayment for cancer drugs, a higher copayment can be implemented to relieve the government’s financial burden resulting from the rapid reimbursement process to improve patients’ access to new medications [
38].
The government is currently discussing a “pre-listing and post-cost effectiveness evaluating system,” according to which drugs will be listed under the health insurance system at temporary prices without undergoing a cost-effectiveness evaluation, and reimbursement and prices will be determined later through a follow-up evaluation process. This method would be applied to drugs that have high demand but also pose an economic burden, and the costs spent until evaluation would, in part, be reclaimed for drugs which were ultimately not found to be cost-effective. However, it is still uncertain whether this system will be implemented.
Whether the clinical efficacy evaluated at the time of listing new drugs remains consistent with their actual clinical effectiveness contributes to the uncertainty in the decision making process about insurance coverage and drug prices. Therefore, it is necessary to verify and re-evaluate whether clinical outcomes remain consistent at the initially appraised level of impact. In particular, the societal need to re-evaluate the clinical utility of drugs which are in high demand for patient care and that represent a substantial financial burden, such as recently listed targeted anticancer drugs and cancer immunotherapy drugs, has increased [
39]. Because the analysis of health insurance claims data offers limited information for the evaluation of actual clinical efficacy, methods of preparing a system to analyze the cost-effectiveness by investigating the clinical efficacy and cost in real-world clinical settings are being sought.
5.1. Policy Suggestions
5.1.1. Increase the Transparency and Rationality of Cost-Effectiveness Analysis
Although performing a review of the data obtained from cost-effectiveness analyses conducted in South Korea may be a time-consuming process, it is nevertheless considered the most important factor for decision-making. Improvements to reduce the time costs of reviewing such studies and solve issues regarding the transparency and efficacy of the review process are warranted.
The acceptable threshold for the incremental cost-effectiveness ratio (ICER) for most new drugs is often below 25,000,000 KRW (USD 21,968, which is equivalent to Korea’s per capita GDP) per quality-adjusted life year. This threshold value was created based on per capita GDP in Korea at the time in 2016. Since then, the value has not been adjusted for changes in per capita GDP in Korea. Thus, adjustments should be made to the acceptable threshold value to account for changes in per capita GPD, and more flexible ICER thresholds for reimbursement should be implemented based on diseases’ severities or societal impacts to improve patient access to care. Currently, for a limited number of anticancer drugs and orphan drugs, a flexible incremental cost-effectiveness ratio threshold of up to 50,000,000 KRW (USD 43,936; two times GDP) per quality-adjusted life year has recently begun to be applied.
The WHO recommended a threshold value of 1–3 times a country’s per capita GDP but they did not provide additional justification for this value [
40]. The decision process of medication selection based on ICERs often raises questions about a society’s willingness to pay for increased QALYs. For example, National Institute for Health and Care Excellence (NICE) in the UK has explicitly used a willingness to pay threshold ranging from £20,000/QALY (U.S.
$25,000) to £50,000 (U.S.
$62,500) for life-threatening conditions. Australia does not have an explicit threshold but accepted new medications which have thresholds ranging from AUD45,000 to AUD60,000 per QALY (U.S.
$31,500–U.S.
$42,500) [
41]. The U.S. uses a wide range of thresholds from U.S.
$50,000/QALY to
$150,000/QALY depending on individual preferences or disease severity.
5.1.2. Improvement of the Risk-Sharing Agreement System
For chronic diseases such as osteoarthritis, and acute infectious diseases such as hepatitis C, only symptom relief or temporary treatments were available in the past. However, recent improvements have led to the development of innovative new drugs that can increase survival and possibly lead to a complete recovery; hence, the frequency of requests pertaining to the listing of these drugs has increased. Compared to other countries, South Korea has a more limited scope for entering into risk-sharing agreements because only certain anticancer or orphan drugs are listed under this system. Most drugs under the risk-sharing agreement system are also associated with refund agreements because of considerable uncertainty that results from the paucity of explicit guidelines on outcome-based risk-sharing agreements.
There is a lack of agreement among the government, manufacturers, and patient advocate groups on the eligibility criteria of a risk-sharing agreement. Patient advocate groups are concerned about the lack of transparency of the list price and the actual price after rebate. The risk-sharing agreement application should be expanded to include medications that do not have alternatives or diseases such as acute attacks of hereditary angioedema, moderate to severe asthma, systemic lupus erythematosus, and cryopyrin-associated periodic syndromes. In addition, the Korean government should provide clearer guidelines on how various forms of outcome-based risk-sharing agreements can be employed for each drug.
5.1.3. Improvement of the Drug Price Listing Process
The prices of new drugs in South Korea are determined based on two steps: first, the cost-effectiveness evaluation (i.e., suitability for reimbursement) is performed by HIRA followed by a financial agreement (i.e., negotiation on drug prices based on budget impact analysis and referencing price, and price-volume agreement, etc.) with the NHIS. There is mounting criticism that these two-step procedures lowered the viability and transparency of the drug pricing system [
42,
43]. As a result, some experts suggested that the procedures followed by HIRA and NHIS for determining drug prices should be combined. However, a rebuttal for this argument is that the current two-step approach is useful for checking and balancing the powers of HIRA and NHIS in the process of listing new medications; as such, it is unlikely that the tasks will ever be combined. Therefore, to ensure that each organization achieves its own goals, the roles of the HIRA and NHIS should be clearly defined.
To improve patient access to care as well as determine the appropriate value of novel medications, a package negotiation system with the NHIS—where prices are negotiated for a group of drugs with similar purposes made by one company—could be implemented rather than negotiating individual prices for each drug. This package system could improve the current system and prevent drugs from failing to be listed because of the lack of a financial agreement, despite the drugs being considered suitable for reimbursement. Varying the negotiation methods to more effectively manage financial resources may also be a way for insurance providers to better fulfill their roles [
44]. The Korean government recently implemented a new policy to expedite the review process period of NHIS from 60 days to 30 days. If the efficacy of a new medication is similar to those of comparators’ and a manufacturer accepts a price lower than the weighted average price in the market, the negotiation process is skipped entirely.
5.1.4. The Necessity of External Financial Resources for Orphan and Anticancer Drugs Independent of the NHIS
Countries such as the UK and Australia have separate cancer drug funds to provide patients with access to drugs that have clinically plausible potential with additional data but have not yet been appraised [
20,
21,
22,
23]. The funds improve patients’ access to new innovative drugs to treat rare diseases or cancers that satisfy specific criteria while adhering to the rules of the health insurance system. Because South Korea does not have a similar policy and relies only on health insurance premiums, it is exceedingly difficult to provide reimbursement for costly cancer or orphan drugs that have a high societal demand and need but uncertain clinical outcomes. Covering these drugs under the health insurance system would contradict the principles of universal insurance and may lower equity. Therefore, additional funding sources outside of health insurance should be procured.
6. Conclusions
The national health insurance system in South Korea has gradually improved quality medical services and access to medications at reasonable prices. However, the health insurance coverage rate is currently only 63%, which falls well short of the OECD average of 80%. In order to improve the coverage rate, the government recently announced a roadmap to provide reimbursement for all currently non-reimbursable treatments and medications. It is expected to make significant changes in the scope, reimbursement type, and price determination processes.
Several policies have been implemented after the introduction of the positive formulary listing system in 2007, and both cost-effectiveness evaluations by HIRA and financial agreements with the NHIS have played, and will continue to play, vital roles with regards to listing of drugs in the national formulary. Continued improvement in current policies and the introduction of new policies is likely to improve patient access to new and advanced drugs in South Korea, and recommendations to implement financial management policies to ensure sustainability of financial resources for insurance will further balance these two aspects.
Author Contributions
S.-L.Y., D.-J.K., and S.-M.L. contributed equally to the study design, statistical analysis, and manuscript development under the guidance of D.-C.S. and J.H.L., S.-L.Y., D.-J.K., S.-M.L., and J.H.L. participated in data collection, data analysis, and manuscript review. W.-G.K. and S.-Y.K. participated in collecting data and revising the manuscript. D.-C.S. and J.H.L. supervised the entirety of the study right from study designing, data collection and analysis, and manuscript editing to manuscript submission. All the authors have read and approved the final version of the manuscript.
Funding
This research received no external funding.
Conflicts of Interest
The authors have no conflicts of interest to declare.
References
- Vitry, A.; Roughead, E. Managed entry agreements for pharmaceuticals in Australia. Health Policy 2014, 117, 345–352. [Google Scholar] [CrossRef] [PubMed]
- Sorenson, C.; Drummond, M.; Bhuiyan Khan, B. Medical technology as a key driver of rising health expenditure: Disentangling the relationship. Clin. Outcomes Res. 2013, 5, 223–234. [Google Scholar] [CrossRef] [PubMed]
- Rotar, A.M.; Preda, A.; Löblová, O.; Benkovic, V.; Zawodnik, S.; Gulacsi, L.; Niewada, M.; Boncz, I.; Petrova, G.; Dimitrova, M.; et al. Rationalizing the introduction and use of pharmaceutical products: The role of managed entry agreements in central and eastern european countries. Health Policy 2018, 122, 230–236. [Google Scholar] [CrossRef] [PubMed]
- Ferrario, A.; Kanavos, P. Dealing with uncertainty and high prices of new medicines: A comparative analysis of the use of managed entry agreements in belgium, england, the netherlands and sweden. Soc. Sci. Med. 2015, 124, 39–47. [Google Scholar] [CrossRef]
- Walker, S.; Sculpher, M.; Claxton, K.; Palmer, S. Coverage with evidence development, only in research, risk sharing, or patient access scheme? A framework for coverage decisions. Value Health 2012, 15, 570–579. [Google Scholar] [CrossRef] [PubMed]
- Golec, J.; Vernon, J.A. Financial effects of pharmaceutical price regulation on r&d spending by eu versus us firms. Pharmacoeconomics 2010, 28, 615–628. [Google Scholar]
- Ermisch, M.; Bucsics, A.; Vella Bonanno, P.; Arickx, F.; Bybau, A.; Bochenek, T.; van de Casteele, M.; Diogene, E.; Fürst, J.; Garuolienė, K.; et al. Payers’ views of the changes arising through the possible adoption of adaptive pathways. Front. Pharmacol. 2016, 7, 305. [Google Scholar] [CrossRef] [PubMed]
- Carrera, P.M.; Kantarjian, H.M.; Blinder, V.S. The financial burden and distress of patients with cancer: Understanding and stepping-up action on the financial toxicity of cancer treatment. CA Cancer J. Clin. 2018, 68, 153–165. [Google Scholar] [CrossRef] [Green Version]
- Degtiar, I. A review of international coverage and pricing strategies for personalized medicine and orphan drugs. Health Policy 2017, 121, 1240–1248. [Google Scholar] [CrossRef]
- Ronfard, V.; Vertès, A.A.; May, M.H.; Dupraz, A.; van Dyke, M.E.; Bayon, Y. Evaluating the past, pesent, and future of regenerative medicine: A global view. Tissue Eng. Part B Rev. 2017, 23, 199–210. [Google Scholar] [CrossRef]
- Garrison, L.P.; Towse, A. Value-based pricing and reimbursement in personalised healthcare: Introduction to the basic health economics. J. Pers. Med. 2017, 7, 10. [Google Scholar] [CrossRef]
- Mahalatchimy, A. Reimbursement of cell-based regenerative therapy in the uk and france. Med. Law Rev. 2016, 24, 234–258. [Google Scholar] [CrossRef]
- Adamski, J.; Godman, B.; Ofierska-Sujkowska, G.; Osińska, B.; Herholz, H.; Wendykowska, K.; Laius, O.; Jan, S.; Sermet, C.; Zara, C.; et al. Risk sharing arrangements for pharmaceuticals: Potential considerations and recommendations for european payers. BMC Health Serv. Res. 2010, 10, 153. [Google Scholar] [CrossRef] [PubMed]
- Klemp, M.; Frønsdal, K.B.; Facey, K. What principles should govern the use of managed entry agreements? Int. J. Technol. Assess. Health Care 2011, 27, 77–83. [Google Scholar] [CrossRef] [Green Version]
- Wonder, M.; Backhouse, M.E.; Sullivan, S.D. Australian managed entry scheme: A new manageable process for the reimbursement of new medicines? Value Health 2012, 15, 586–590. [Google Scholar] [CrossRef] [PubMed]
- Neumann, P.J.; Bliss, S.K.; Chambers, J.D. Therapies for advanced cancers pose a special challenge for health technology assessment organizations in many countries. Health Aff. (Millwood) 2012, 31, 700–708. [Google Scholar] [CrossRef]
- Chim, L.; Salkeld, G.; Kelly, P.; Lipworth, W.; Hughes, D.A.; Stockler, M.R. Societal perspective on access to publicly subsidised medicines: A cross sectional survey of 3080 adults in australia. PLoS ONE 2017, 12, e0172971. [Google Scholar] [CrossRef] [PubMed]
- Cookson, R. Can the nice “end-of-life premium” be given a coherent ethical justification? J. Health Politcs Policy Law 2013, 38, 1129–1148. [Google Scholar] [CrossRef]
- Brock, D.W. Ethical and value issues in insurance coverage for cancer treatment. Oncologist 2010, 15 (Suppl. 1), 36–42. [Google Scholar] [CrossRef] [PubMed]
- Aggarwal, A.; Fojo, T.; Chamberlain, C.; Davis, C.; Sullivan, R. Do patient access schemes for high-cost cancer drugs deliver value to society?-lessons from the nhs cancer drugs fund. Ann. Oncol. 2017, 28, 1738–1750. [Google Scholar] [CrossRef] [PubMed]
- Dixon, P.; Chamberlain, C.; Hollingworth, W. Did it matter that the cancer drugs fund was not nice? A retrospective review. Value Health 2016, 19, 879–884. [Google Scholar] [CrossRef] [PubMed]
- Taylor, C.; Jan, S.; Thompson, K. Funding therapies for rare diseases: An ethical dilemma with a potential solution. Aust. Health Rev. 2018, 42, 117–119. [Google Scholar] [CrossRef] [PubMed]
- Sylvia, P.A. Comparative study on the system of rare medicine by country. Health Soc. Welf. Rev. 2013, 33, 525–548. [Google Scholar]
- Ministry of Health and Welfare. Policy Report: Drug Expenditure Optimization System in National Health Insurance Services; Ministry of Health and Welfare: SeJong, Korea, 2006.
- Bae, E.-Y.; Hong, J.-M.; Kwon, H.-Y.; Jang, S.; Lee, H.-J.; Bae, S.; Yang, B.-M. Eight-year experience of using hta in drug reimbursement: South korea. Health Policy 2016, 120, 612–620. [Google Scholar] [CrossRef] [PubMed]
- Ministry of Health and Welfare. Policy Report: A Study on the Improvement of Drug Price System for the Improvement of Accessibility of New Products; Ministry of Health and Welfare: Seoul, Korea, 2014.
- OECD. Health at a Glance 2017; OECD: Paris, France, 2017. [Google Scholar]
- National Health Insurance Service. Ppri Pharma Profile Report: Korean Pharmaceutical Pricing and Repayment Policies; National Health Insurance Service: Won-ju, Korea, 2017. [Google Scholar]
- National Health Insurance Service. Policy Report: A Study on the Introduction of Risk Sharing Contract; National Health Insurance Service: SeJong, Korea, 2012. [Google Scholar]
- Health Insurance Review Assessment Service. Hira Notification: Detailed Evaluation Criteria for New Drugs Subject to Negotiation; Health Insurance Review Assessment Service: Seoul, Korea, 2017. [Google Scholar]
- Korean Pharmaceutical Manufacturers Association. Kpma Policy Report: Korean Pharmaceutical Manufacturers Association; Korean Pharmaceutical Manufacturers Association: Seoul, Korea, 2016. [Google Scholar]
- Health Insurance Review Assessment Service. List of Reimbursable Drugs. 2018. Available online: https://www.hira.or.kr/bbsDummy.do?pgmid=HIRAA030014050000 (accessed on 30 November 2018).
- Lee, W.-Y.; Shaw, I. The impact of out-of-pocket payments on health care inequity: The case of national health insurance in south korea. Int. J. Environ. Res. Public Health 2014, 11, 7304–7318. [Google Scholar] [CrossRef]
- Korea Institute for Health Social Affairs. Policy Report: Policy Measures to Enhance Access to Drugs for Rare Diseases; Korea Institute for Health Social Affairs: SeJong, Korea, 2010. [Google Scholar]
- Korean Research-based Pharmaceutical Industry Association. A Study on the Improvement of Drug Price System for the Improvement of Pharmaceutical Industry and the Improvement of Patient Access; Korea Institute for Health Social Affairs: SeJong, Korea, 2016. [Google Scholar]
- Korea Institute for Health Social Affairs. Policy Report: A Study on the Rationalization of Drug Price Management System; Korea Institute for Health Social Affairs: SeJong, Korea, 2015. [Google Scholar]
- Korea Institute for Health Social Affairs. Policy Report: The Problems and Improvement of the Payment System; Korea Institute for Health Social Affairs: SeJong, Korea, 2014. [Google Scholar]
- Ministry of Health and Welfare. A Proposal for the Reform of the Drug Price System to Strengthen Health Insurance Coverage (Moon Care); Ministry of Health and Welfare: SeJong, Korea, 2018.
- Health Insurance Policy Institute. Policy Report: A Study on the Health Insurance High-Cost Medicine; Health Insurance Policy Institute: Won-Ju, Korea, 2017. [Google Scholar]
- Leech, A.A.; Kim, D.D.; Cohen, J.T.; Neumann, P.J. Use and misuse of cost-effectiveness analysis thresholds in low- and middle-income countries: Trends in cost-per daly studies. Value Health 2018, 21, 759–761. [Google Scholar] [CrossRef]
- Wang, S.; Gum, D.; Merlin, T. Comparing the icers in medicine reimbursement submissions to nice and pbac-does the presence of an explicit threshold affect the icer proposed? Value Health 2018, 21, 938–943. [Google Scholar] [CrossRef]
- National Health Insurance Service. A Study on the Improvement of Drug Price Negotiation and Drug Price Management System; National Health Insurance Service: Seoul, Korea, 2013. [Google Scholar]
- National Health Insurance Service. Policy Report: A Study on the Promotion of Transparency in Price Negotiation; National Health Insurance Service: Seoul, Korea, 2013. [Google Scholar]
- Health Insurance Policy Institute. Policy Report: A Study on the Establishment of Roadmap for Systematic Management of Health Insurance Pharmaceuticals; Health Insurance Policy Institute: Seoul, Korea, 2012. [Google Scholar]
© 2019 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).

 and
and 



{kind=link}
{kind=link}
{kind=link}