Adult E-Cigarettes Use Associated with a Self-Reported Diagnosis of COPD


Abstract
:1. Introduction
2. Materials and Methods
2.1. Measures of Independent Variables
2.2. Measure of Dependent Variable
2.3. Statistical Analysis
3. Results
3.1. Study Sample Characteristics
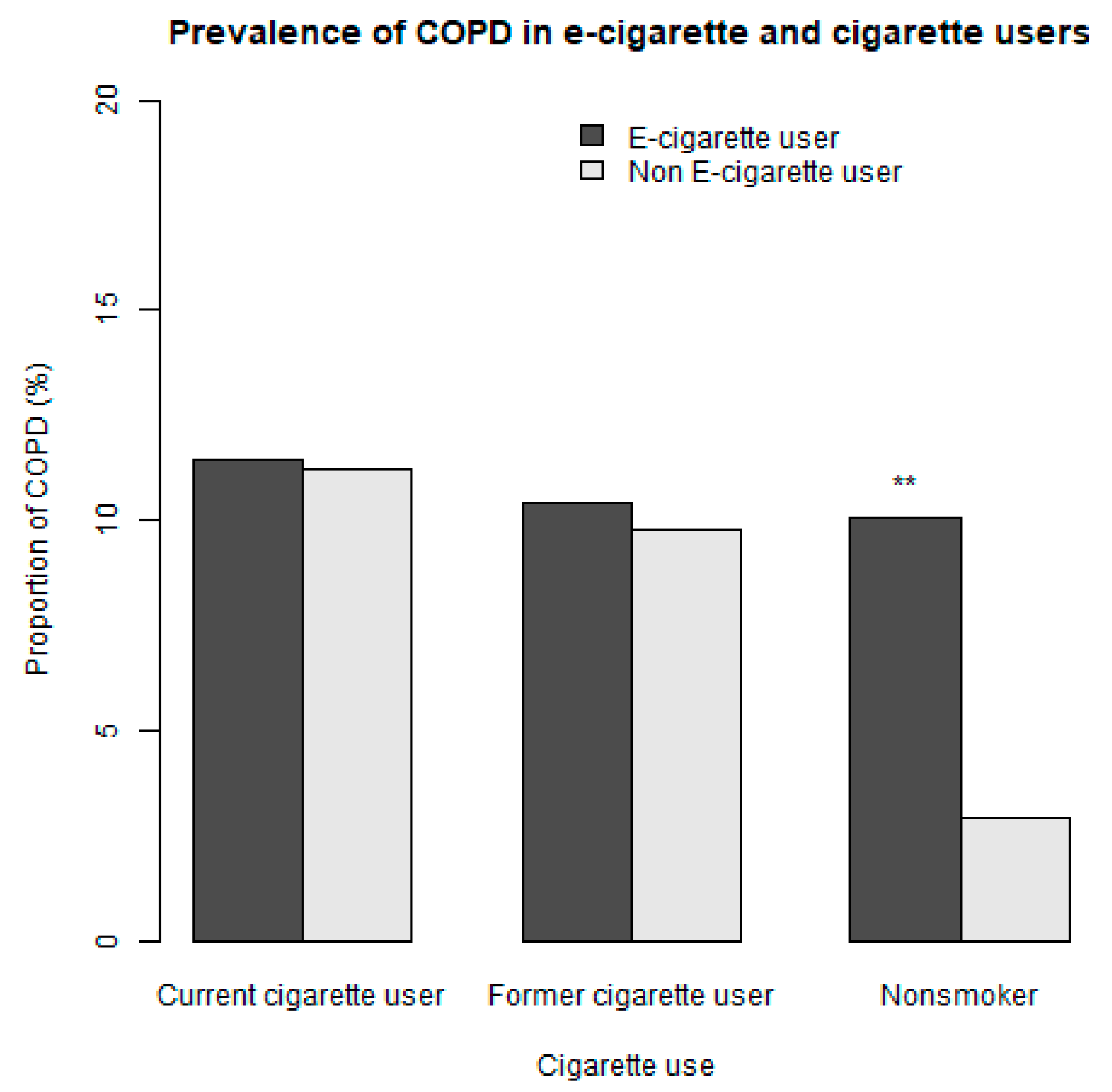
3.2. Association between E-Cigarette Use and Reporting COPD
4. Discussion
5. Conclusions
Author Contributions
Funding
Conflicts of Interest
References
- E-Cigarette Use among Youth and Young Adults: A Report of the Surgeon General. Available online: https://0-www-ncbi-nlm-nih-gov.brum.beds.ac.uk/books/NBK538680/ (accessed on 20 September 2019).
- Dai, H.; Leventhal, A.M. Prevalence of E-Cigarette Use Among Adults in the United States, 2014–2018. JAMA 2019. [Google Scholar] [CrossRef] [PubMed]
- Cullen, K.A.; Ambrose, B.K.; Gentzke, A.S.; Apelberg, B.J.; Jamal, A.; King, B.A. Notes from the Field: Use of Electronic Cigarettes and Any Tobacco Product Among Middle and High School Students–United States, 2011–2018. MMWR Morb. Mortal. Wkly. Rep. 2018, 67, 1276–1277. [Google Scholar] [CrossRef] [PubMed]
- Dinakar, C.; O’Connor, G.T. The Health Effects of Electronic Cigarettes. N. Engl. J. Med. 2016, 375, 1372–1381. [Google Scholar] [CrossRef] [PubMed]
- Cheng, T. Chemical evaluation of electronic cigarettes. Tob. Control 2014, 23, 11–17. [Google Scholar] [CrossRef] [PubMed]
- Goniewicz, M.L.; Knysak, J.; Gawron, M.; Kosmider, L.; Sobczak, A.; Kurek, J.; Prokopowicz, A.; Jablonska-Czapla, M.; Rosik-Dulewska, C.; Havel, C.; et al. Levels of selected carcinogens and toxicants in vapour from electronic cigarettes. Tob. Control 2014, 23, 133–139. [Google Scholar] [CrossRef] [PubMed]
- Goniewicz, M.L.; Smith, D.M.; Edwards, K.C.; Blount, B.C.; Caldwell, K.L.; Feng, J.; van Bemmel, D. Comparison of nicotine and toxicant exposure in users of electronic cigarettes and combustible cigarettes. JAMA Netw. Open 2018, 1, e185937. [Google Scholar] [CrossRef] [PubMed]
- Layden, J.E.; Ghinai, I.; Pray, I.; Kimball, A.; Layer, M.; Tenforde, M.; Navon, L.; Hoots, B.; Salvatore, P.P.; Elderbrook, M.; et al. Pulmonary Illness Related to E-Cigarette Use in Illinois and Wisconsin–Preliminary Report. N. Engl. J. Med. 2019. [Google Scholar] [CrossRef]
- Morjaria, J.B.; Mondati, E.; Polosa, R. E-cigarettes in patients with COPD: Current perspectives. Int. J. Chron. Obstruct Pulmon. Dis. 2017, 12, 3203–3210. [Google Scholar] [CrossRef]
- Coleman, B.N.; Rostron, B.; Johnson, S.E.; Ambrose, B.K.; Pearson, J.; Stanton, C.A.; Wang, B.; Delnevo, C.; Bansal-Travers, M.; Kimmel, H.L.; et al. Electronic cigarette use among US adults in the Population Assessment of Tobacco and Health (PATH) Study, 2013–2014. Tob. Control 2017, 26, e117–e126. [Google Scholar] [CrossRef]
- Foulds, J.; Veldheer, S.; Berg, A. Electronic cigarettes (e-cigs): Views of aficionados and clinical/public health perspectives. Int. J. Clin. Pract. 2011, 65, 1037–1042. [Google Scholar] [CrossRef]
- Etter, J.F. Electronic cigarettes: A survey of users. BMC Public Health 2010, 10, 231. [Google Scholar] [CrossRef] [PubMed]
- Walker, N.; Parag, V.; Verbiest, M.; Laking, G.; Laugesen, M.; Bullen, C. Nicotine patches used in combination with e-cigarettes (with and without nicotine) for smoking cessation: A pragmatic, randomised trial. Lancet Respir. Med. 2019. [Google Scholar] [CrossRef]
- Hajek, P.; Phillips-Waller, A.; Przulj, D.; Pesola, F.; Myers Smith, K.; Bisal, N.; Li, J.; Parrott, S.; Sasieni, P.; Dawkins, L.; et al. A Randomized Trial of E-Cigarettes versus Nicotine-Replacement Therapy. N. Engl. J. Med. 2019, 380, 629–637. [Google Scholar] [CrossRef] [PubMed]
- Bullen, C.; Howe, C.; Laugesen, M.; McRobbie, H.; Parag, V.; Williman, J.; Walker, N. Electronic cigarettes for smoking cessation: A randomised controlled trial. Lancet 2013, 382, 1629–1637. [Google Scholar] [CrossRef]
- Outbreak of Lung Injury Associated with E-Cigarette Use, or Vaping. Available online: https://www.cdc.gov/tobacco/basic_information/e-cigarettes/severe-lung-disease.html (accessed on 19 September 2019).
- Baldassarri, S.R.; Chupp, G.L.; Leone, F.T.; Warren, G.W.; Toll, B.A. Practice Patterns and Perceptions of Chest Health Care Providers on Electronic Cigarette Use: An In-Depth Discussion and Report of Survey Results. J. Smok. Cessat. 2018, 13, 72–77. [Google Scholar] [CrossRef]
- Schraufnagel, D.E.; Blasi, F.; Drummond, M.B.; Lam, D.C.; Latif, E.; Rosen, M.J.; Sansores, R.; Van Zyl-Smit, R. Electronic cigarettes. A position statement of the forum of international respiratory societies. Am. J. Respir. Crit. Care Med. 2014, 190, 611–618. [Google Scholar] [CrossRef]
- Perez, M.F.; Atuegwu, N.C.; Oncken, C.M.; Mead, E.L.; Mortensen, E.M. Association of Electronic Cigarette Use and Asthma in Never Smokers. Ann. Am. Thorac. Soc. 2019. [Google Scholar] [CrossRef]
- Cho, J.H.; Paik, S.Y. Association between Electronic Cigarette Use and Asthma among High School Students in South Korea. PLoS ONE 2016, 11, e0151022. [Google Scholar] [CrossRef]
- Choi, K.; Bernat, D. E-Cigarette Use among Florida Youth with and Without Asthma. Am. J. Prev. Med. 2016, 51, 446–453. [Google Scholar] [CrossRef]
- Schweitzer, R.J.; Wills, T.A.; Tam, E.; Pagano, I.; Choi, K. E-cigarette use and asthma in a multiethnic sample of adolescents. Prev. Med. 2017, 105, 226–231. [Google Scholar] [CrossRef]
- Vogelmeier, C.F.; Criner, G.J.; Martinez, F.J.; Anzueto, A.; Barnes, P.J.; Bourbeau, J.; Celli, B.R.; Chen, R.; Decramer, M.; Fabbri, L.M.; et al. Global Strategy for the Diagnosis, Management and Prevention of Chronic Obstructive Lung Disease 2017 Report: GOLD Executive Summary. Respirology 2017, 22, 575–601. [Google Scholar] [CrossRef] [PubMed]
- Sullivan, J.; Pravosud, V.; Mannino, D.M.; Siegel, K.; Choate, R.; Sullivan, T. National and State Estimates of COPD Morbidity and Mortality–United States, 2014–2015. Chronic Obstr. Pulm. Dis. 2018, 5, 324–333. [Google Scholar] [CrossRef] [PubMed]
- Ramsey, S.D.; Hobbs, F.D. Chronic obstructive pulmonary disease, risk factors, and outcome trials: Comparisons with cardiovascular disease. Proc. Am. Thorac. Soc. 2006, 3, 635–640. [Google Scholar] [CrossRef] [PubMed]
- Buist, A.S.; McBurnie, M.A.; Vollmer, W.M.; Gillespie, S.; Burney, P.; Mannino, D.M.; Menezes, A.M.; Sullivan, S.D.; Lee, T.A.; Weiss, K.B.; et al. International variation in the prevalence of COPD (the BOLD Study): A population-based prevalence study. Lancet 2007, 370, 741–750. [Google Scholar] [CrossRef]
- Larcombe, A.N.; Janka, M.A.; Mullins, B.J.; Berry, L.J.; Bredin, A.; Franklin, P.J. The effects of electronic cigarette aerosol exposure on inflammation and lung function in mice. Am. J. Physiol. Lung Cell Mol. Physiol. 2017, 313, L67–L79. [Google Scholar] [CrossRef]
- Lerner, C.A.; Sundar, I.K.; Yao, H.; Gerloff, J.; Ossip, D.J.; McIntosh, S.; Robinson, R.; Rahman, I. Vapors produced by electronic cigarettes and e-juices with flavorings induce toxicity, oxidative stress, and inflammatory response in lung epithelial cells and in mouse lung. PLoS ONE 2015, 10, e0116732. [Google Scholar] [CrossRef]
- Garcia-Arcos, I.; Geraghty, P.; Baumlin, N.; Campos, M.; Dabo, A.J.; Jundi, B.; Cummins, N.; Eden, E.; Grosche, A.; Salathe, M.; et al. Chronic electronic cigarette exposure in mice induces features of COPD in a nicotine-dependent manner. Thorax 2016, 71, 1119–1129. [Google Scholar] [CrossRef] [Green Version]
- Lim, H.B.; Kim, S.H. Inhallation of e-Cigarette Cartridge Solution Aggravates Allergen-induced Airway Inflammation and Hyper-responsiveness in Mice. Toxicol Res. 2014, 30, 13–18. [Google Scholar] [CrossRef] [Green Version]
- Barnes, P.J. Immunology of asthma and chronic obstructive pulmonary disease. Nat. Rev. Immunol. 2008, 8, 183–192. [Google Scholar] [CrossRef]
- Wills, T.A.; Pagano, I.; Williams, R.; Tam, E. E-cigarette use and respiratory disorder in an adult sample. Drug Alcohol Depend. 2018, 194, 363–370. [Google Scholar] [CrossRef]
- Polosa, R.; Cibella, F.; Caponnetto, P.; Maglia, M.; Prosperini, U.; Russo, C.; Tashkin, D. Health impact of E-cigarettes: A prospective 3.5-year study of regular daily users who have never smoked. Sci. Rep. 2017, 7, 13825. [Google Scholar] [PubMed]
- Hyland, A.; Ambrose, B.K.; Conway, K.P.; Borek, N.; Lambert, E.; Carusi, C.; Taylor, K.; Crosse, S.; Fong, G.T.; Cummings, K.M.; et al. Design and methods of the Population Assessment of Tobacco and Health (PATH) Study. Tob. Control 2017, 26, 371–378. [Google Scholar] [CrossRef] [PubMed]
- Population Assessment of Tobacco and Health (PATH) Study Series. Available online: https://www.icpsr.umich.edu/icpsrweb/NAHDAP/series/606 (accessed on 18 September 2019).
- CDC. NHIS–Adult Tobacco Use–Glossary. Available online: https://www.cdc.gov/nchs/nhis/tobacco /tobacco_glossary.htm (accessed on 1 October 2019).
- Rosenbaum, P.R.; Rubin, D.B. The Central Role of the Propensity Score in Observational Studies for Causal Effects. Biometrika 1983, 70, 41–55. [Google Scholar] [CrossRef]
- Lenis, D.; Nguyen, T.Q.; Dong, N.; Stuart, E.A. It’s all about balance: Propensity score matching in the context of complex survey data. Biostatistics 2017, 20, 147–163. [Google Scholar] [CrossRef]
- R Core Team. R: A Language and Environment for Statistical Computing; R Foundation for Statistical Computing: Vienna, Austria, 2013. [Google Scholar]
- Lappas, A.S.; Tzortzi, A.S.; Konstantinidi, E.M.; Teloniatis, S.I.; Tzavara, C.K.; Gennimata, S.A.; Koulouris, N.G.; Behrakis, P.K. Short-term respiratory effects of e-cigarettes in healthy individuals and smokers with asthma. Respirology 2018, 23, 291–297. [Google Scholar] [CrossRef]
- McConnell, R.; Barrington-Trimis, J.L.; Wang, K.; Urman, R.; Hong, H.; Unger, J.; Samet, J.; Leventhal, A.; Berhane, K. Electronic Cigarette Use and Respiratory Symptoms in Adolescents. Am. J. Respir. Crit. Care Med. 2017, 195, 1043–1049. [Google Scholar] [CrossRef] [Green Version]
- Bowler, R.P.; Hansel, N.N.; Jacobson, S.; Graham Barr, R.; Make, B.J.; Han, M.K.; O’Neal, W.K.; Oelsner, E.C.; Casaburi, R.; Barjaktarevic, I.; et al. Electronic Cigarette Use in US Adults at Risk for or with COPD: Analysis from Two Observational Cohorts. J. Gen. Intern Med. 2017, 32, 1315–1322. [Google Scholar] [CrossRef] [Green Version]
- Department of Health. New York State Department of Health Announces Update on Investigation into Vaping-Associated Pulmonary Illnesses. Available online: https://www.health.ny.gov/press/releases/2019/2019-09-05_vaping.htm (accessed on 14 September 2019).
- Farsalinos, K.E.; Romagna, G.; Tsiapras, D.; Kyrzopoulos, S.; Voudris, V. Characteristics, perceived side effects and benefits of electronic cigarette use: A worldwide survey of more than 19,000 consumers. Int. J. Environ. Res. Public Health 2014, 11, 4356–4373. [Google Scholar] [CrossRef]
- Polosa, R.; Morjaria, J.B.; Caponnetto, P.; Prosperini, U.; Russo, C.; Pennisi, A.; Bruno, C.M. Evidence for harm reduction in COPD smokers who switch to electronic cigarettes. Respir Res. 2016, 17, 166. [Google Scholar] [CrossRef]
- Polosa, R.; Morjaria, J.B.; Prosperini, U.; Russo, C.; Pennisi, A.; Puleo, R.; Caruso, M.; Caponnetto, P. Health effects in COPD smokers who switch to electronic cigarettes: A retrospective-prospective 3-year follow-up. Int. J. Chron. Obstruct Pulmon. Dis. 2018, 13, 2533–2542. [Google Scholar] [CrossRef]
- Kasza, K.A.; Ambrose, B.K.; Conway, K.P.; Borek, N.; Taylor, K.; Goniewicz, M.L.; Cummings, K.M.; Sharma, E.; Pearson, J.L.; Green, V.R.; et al. Tobacco-Product Use by Adults and Youths in the United States in 2013 and 2014. N. Engl. J. Med. 2017, 376, 342–353. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Bhatt, S.P.; Kim, Y.I.; Harrington, K.F.; Hokanson, J.E.; Lutz, S.M.; Cho, M.H.; DeMeo, D.L.; Wells, J.M.; Make, B.J.; Rennard, S.I.; et al. Smoking duration alone provides stronger risk estimates of chronic obstructive pulmonary disease than pack-years. Thorax 2018, 73, 414–421. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Akinbami, L.J.; Moorman, J.E.; Liu, X.; National Center for Health Statistics (U.S.). Asthma Prevalence, Health Care Use, and Mortality: United States, 2005–2009; Department of Health and Human Services, Centers for Disease Control and Prevention, National Center for Health Statistics: Hyattsville, MD, USA, 2011.



{kind=link}
{kind=link}
| Variable | Controls a | E-Cigarette Users a | Sample Balance | Population Balance c | ||
|---|---|---|---|---|---|---|
| p-Value | SMD b | p-Value | SMD b | |||
| Number of Individuals | 2727 | 2727 | ||||
| BMI | 27.5 (6.7) | 27.7 (6.8) | 0.38 | 0.02 | 0.74 | 0.01 |
| Years of conventional cigarette use | 14.2 (14.4) | 13.9 (13.7) | 0.37 | 0.02 | 0.80 | 0.01 |
| Age Group | 0.85 | 0.04 | 0.86 | 0.04 | ||
| 18 to 24 years old | 793 (29.1) | 830 (30.4) | ||||
| 25 to 34 years old | 685 (25.1) | 685 (25.1) | ||||
| 35 to 44 years old | 475 (17.4) | 478 (17.5) | ||||
| 45 to 54 years old | 419 (15.4) | 394 (14.4) | ||||
| 55 to 65 years old | 265 (9.7) | 256 (9.4) | ||||
| 65 years old or older | 90 (3.3) | 84 (3.1) | ||||
| Male | 1493 (54.7) | 1451 (53.2) | 0.27 | 0.03 | 0.15 | 0.04 |
| Hispanic | 396 (14.5) | 396 (14.5) | 1.00 | <0.001 | 0.92 | 0.003 |
| Race | 0.78 | 0.02 | 0.12 | 0.06 | ||
| White | 2171 (79.6) | 2155 (79.0) | ||||
| Black | 257 (9.4) | 272 (10.0) | ||||
| Other | 299 (11.0) | 300 (11.0) | ||||
| Grade of Highest Education | 0.37 | 0.06 | 0.29 | 0.07 | ||
| Less than High School | 312 (11.4) | 306 (11.2) | ||||
| GED | 289 (10.6) | 271 (9.9) | ||||
| High school graduate | 633 (23.2) | 664 (24.3) | ||||
| Some college (no degree) or associates degree | 1096 (40.2) | 1131 (41.5) | ||||
| Bachelor’s degree or higher | 397 (14.6) | 355 (13.0) | ||||
| Census Region | 0.84 | 0.03 | 0.75 | 0.04 | ||
| Northeast | 301 (11.0) | 310 (11.4) | ||||
| Midwest | 718 (26.3) | 692 (25.4) | ||||
| South | 1059 (38.8) | 1081 (39.6) | ||||
| West | 649 (23.8) | 644 (23.6) | ||||
| Second Hand Exposure During Childhood | 1747 (64.1) | 1767 (64.8) | 0.59 | 0.02 | 0.72 | 0.01 |
| History of Asthma | 356 (13.1) | 371 (13.6) | 0.58 | 0.02 | 0.78 | 0.01 |
| Poverty level | 0.69 | 0.02 | 0.48 | 0.04 | ||
| 100% of poverty guideline | 985 (36.1) | 987 (36.2) | ||||
| 100-199% of poverty guideline | 674 (24.7) | 698 (25.6) | ||||
| ≥200% of poverty guideline | 1068 (39.2) | 1042 (38.2) | ||||
| History of Blunt Use | 1097 (40.2) | 1107 (40.6) | 0.80 | 0.01 | 0.29 | 0.03 |
| Current Secondhand Smoke Exposure in Household | 1366 (50.1) | 1351 (49.5) | 0.71 | 0.01 | 0.82 | 0.01 |
| Never Used Cigars d | 1193 (43.7) | 1197 (43.9) | 0.94 | 0.003 | 0.40 | 0.03 |
| Never Used Cigarillos | 968 (35.5) | 969 (35.5) | 1.00 | 0.001 | 0.97 | 0.001 |
| Never Used Pipe | 1762 (64.6) | 1773 (65.0) | 0.78 | 0.01 | 0.40 | 0.03 |
| Never Used Hookah | 1442 (52.9) | 1412 (51.8) | 0.43 | 0.02 | 0.48 | 0.03 |
| Never Used Oral Tobacco | 1729 (63.4) | 1703 (62.4) | 0.48 | 0.02 | 0.81 | 0.01 |
| Current conventional cigarette use | 1880 (68.9) | 1899 (69.6) | 0.60 | 0.02 | 0.08 | 0.05 |
| Former conventional cigarette use | 395 (14.5) | 368 (13.5) | 0.31 | 0.03 | 0.11 | 0.05 |
| History of High Blood Pressure | 519 (19.0) | 527 (19.3) | 0.81 | 0.01 | 0.32 | 0.03 |
| History of High Cholesterol | 376 (13.8) | 369 (13.5) | 0.81 | 0.01 | 0.98 | 0.001 |
| History of Congestive Heart Failure | 35 (1.3) | 42 (1.5) | 0.75 | 0.02 | 0.67 | 0.01 |
| History of Stroke | 47 (1.7) | 43 (1.6) | 0.52 | 0.01 | 0.92 | 0.003 |
| History of Heart Attack | 40 (1.5) | 47 (1.7) | 0.75 | 0.02 | 0.85 | 0.01 |
| History of Heroin, Inhalants or Hallucinogens | 482 (17.7) | 462 (16.9) | 0.50 | 0.02 | 0.58 | 0.02 |
| History of Diabetes | 257 (9.4) | 261 (9.6) | 0.89 | 0.01 | 0.98 | 0.001 |
| Category | Entire Cohort | Nonsmokers a | Subjects ≥35 b | Subjects ≥45 b | Subjects ≥55 b |
|---|---|---|---|---|---|
| Not users | Reference | Reference | Reference | Reference | Reference |
| E-cigarette user | 1.47 (1.21–1.79) | 2.94 (1.73–4.99) | 1.57(1.27–1.95) | 1.57 (1.20–2.06) | 1.62 (1.14–2.31) |
| Age groups b | |||||
| 18 to 24 | Reference | Reference | |||
| 25 to 34 | 1.03 (0.70–1.52) | 1.29 (0.68–2.42) | |||
| 35 to 44 | 1.79 (1.21–2.63) | 1.97 (0.87–4.45) | Reference | - | - |
| 45 to 54 | 2.37(1.67–3.37) | 1.96 (1.03–3.71) | 1.33 (0.96–1.85) | Reference | - |
| 55 to 65 | 3.15 (2.18–4.54) | 4.06 (2.07–7.97) | 1.79 (1.25–2.58) | 1.35 (1.03–1.77) | Reference |
| >65 | 3.79 (2.55–5.65) | 5.96 (3.31–10.74) | 2.15 (1.38–3.37) | 1.64 (1.18–2.26) | 1.25 (0.91–1.72) |
© 2019 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Perez, M.F.; Atuegwu, N.C.; Mead, E.L.; Oncken, C.; Mortensen, E.M. Adult E-Cigarettes Use Associated with a Self-Reported Diagnosis of COPD. Int. J. Environ. Res. Public Health 2019, 16, 3938. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph16203938
Perez MF, Atuegwu NC, Mead EL, Oncken C, Mortensen EM. Adult E-Cigarettes Use Associated with a Self-Reported Diagnosis of COPD. International Journal of Environmental Research and Public Health. 2019; 16(20):3938. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph16203938
Chicago/Turabian StylePerez, Mario F., Nkiruka C. Atuegwu, Erin L. Mead, Cheryl Oncken, and Eric M. Mortensen. 2019. "Adult E-Cigarettes Use Associated with a Self-Reported Diagnosis of COPD" International Journal of Environmental Research and Public Health 16, no. 20: 3938. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph16203938