Patient Satisfaction with Rural Medical Services: A Cross-Sectional Survey in 11 Western Provinces in China


Abstract
:1. Introduction
2. Materials and Methods
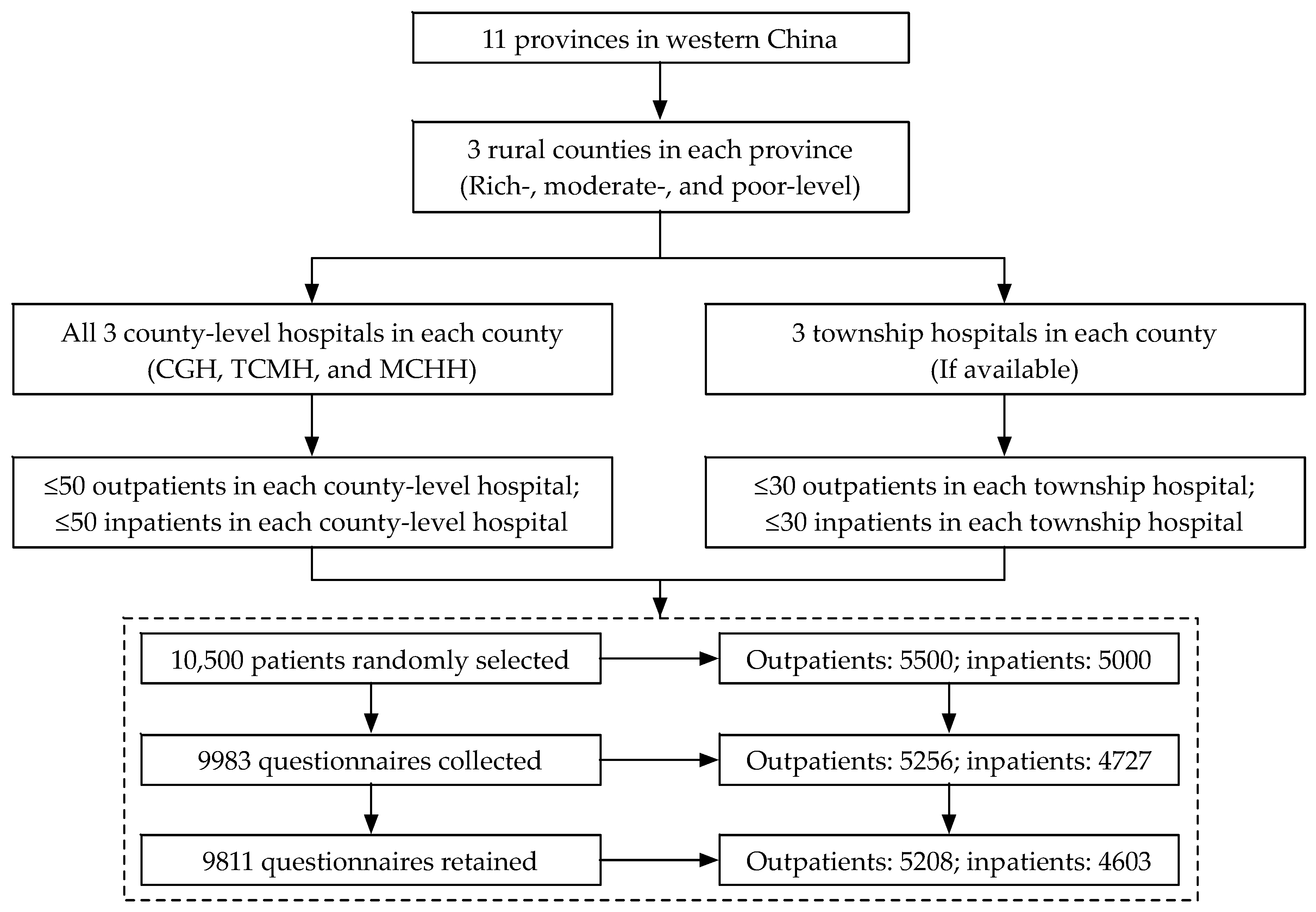
2.1. Study Design and Participants
2.2. Data and Variables
2.3. Statistical Methods
2.4. Ethics
3. Results
3.1. Sociodemographic Characteristics
3.2. Patient Satisfaction with Rural Medical Services
3.3. Influencing Factors of Patients’Overall Stisfaction with Rural Medical Services
4. Discussion
5. Conclusions
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- World Health Organization. Health in 2015: From MDGs to SDGs; World Health Organization: Geneva, Switzerland, 2015. [Google Scholar]
- World Health Organization. 2018 Global Reference list of 100 Core Health Indictors (Plus Health-Related SDGs); World Health Organization: Geneva, Switzerland, 2018. [Google Scholar]
- Olmsted, M.; Powell, R.; Murphy, J.; Bell, D.; Morley, M.; Stanley, M. Methodology: U.S. News & World Report 2019-2020 Best Hospitals; U.S. News & World Report: New York, NY, USA, 2019. [Google Scholar]
- General Office of the State Council of the People’s Republic of China. Opinions on Strengthening the Performance Assessment of Tertiary Public Hospitals. In State Council Communique of the People’s Republic of China; National Bureau of Statistics of China: Beijing, China, 2019; pp. 22–30. [Google Scholar]
- Sitzia, J.; Wood, N. Patient satisfaction: A review of issues and concepts. Soc. Sci. Med. 1997, 45, 1829–1843. [Google Scholar] [CrossRef]
- Risser, N.L. Development of an Instrument to Measure Patient Satisfaction with Nurses and Nursing Care in Primary Care Settings. Nurs. Res. 1975, 24, 45–51. [Google Scholar] [CrossRef] [PubMed]
- Greene, J.Y.; Weinberger, M.; Mamlin, J.J. Patient attitudes toward health care: Expectations of primary care in a clinic setting. Soc. Sci. Med. Med. Psychol. Med. Sociol. 1980, 14, 133–138. [Google Scholar] [CrossRef]
- Ware, J.E.; Snyder, M.K.; Wright, W.R.; Davies, A.R. Defining and measuring patient satisfaction with medical care. Eval. Program Plan. 1983, 6, 247–263. [Google Scholar] [CrossRef]
- Donabedian, A. Evaluating the Quality of Medical Care. Milbank Q. 2005, 83, 691–729. [Google Scholar] [CrossRef] [Green Version]
- Donabedian, A. The quality of care. How can it be assessed? JAMA J. Am. Med. Assoc. 1988, 260, 1743–1748. [Google Scholar] [CrossRef]
- Health Boards Executive. Measurement of Patient Satisfaction Guidelines: Health Strategy Implementation Project 2003; Lenus the Irish Health Repository: Dublin, Ireland, 2003. [Google Scholar]
- Senitan, M.; Alhaiti, A.H.; Gillespie, J. Patient satisfaction and experience of primary care in Saudi Arabia: A systematic review. Int. J. Qual. Health Care 2018, 30, 751–759. [Google Scholar] [CrossRef]
- Aiken, L.H.; Sloane, D.M.; Ball, J.; Bruyneel, L.; Rafferty, A.M.; Griffiths, P. Patient satisfaction with hospital care and nurses in England: An observational study. BMJ Open 2018, 8, e019189. [Google Scholar] [CrossRef]
- Hussain, A.; Sial, M.; Usman, S.; Hwang, J.; Jiang, Y.; Shafiq, A. What Factors Affect Patient Satisfaction in Public Sector Hospitals: Evidence from an Emerging Economy. Int. J. Environ. Res. Public Health 2019, 16, 994. [Google Scholar] [CrossRef]
- Aziz, M.; Ji, W.; Masood, I.; Farooq, M.; Malik, M.; Chang, J.; Jiang, M.; Atif, N.; Fang, Y. Patient Satisfaction with Community Pharmacies Services: A Cross-Sectional Survey from Punjab; Pakistan. Int. J. Environ. Res. Public Health 2018, 15, 2914. [Google Scholar] [CrossRef]
- Sun, J.; Hu, G.; Ma, J.; Chen, Y.; Wu, L.; Liu, Q.; Hu, J.; Livoti, C.; Jiang, Y.; Liu, Y. Consumer satisfaction with tertiary healthcare in China: findings from the 2015 China National Patient Survey. Int. J. Qual. Health Care 2017, 29, 213–221. [Google Scholar] [CrossRef] [PubMed]
- Yin, T.; Yin, D.-L.; Xiao, F.; Xin, Q.-Q.; Li, R.-L.; Zheng, X.-G.; Yang, H.-M.; Wang, L.-H.; Ding, X.-Y.; Chen, B.-W. Socioeconomic status moderates the association between patient satisfaction with community health service and self-management behaviors in patients with type 2 diabetes: A cross-sectional survey in China. Medicine 2019, 98, e15849. [Google Scholar] [CrossRef] [PubMed]
- Xiong, C.; Chen, X.; Zhao, X.; Liu, C. Patient satisfaction and gender composition of physicians—A cross-sectional study of community health services in Hubei, China. BMC Health Serv. Res. 2018, 18, 217. [Google Scholar] [CrossRef] [PubMed]
- Ren, J.; Huang, X.; Zhang, T.; Zhou, X.; Liu, C.; Wang, X. Patient satisfaction with prescribed medicines in community health services in China: A cross-sectional survey 6 years after the implementation of the national essential medicines policy. Health Soc. Care Community 2018, 26, 495–506. [Google Scholar] [CrossRef] [Green Version]
- Dong, W.; Zhang, Q.; Yan, C.; Fu, W.; Xu, L. Residents’ satisfaction with primary medical and health services in Western China. BMC Health Serv. Res. 2017, 17, 298. [Google Scholar] [CrossRef]
- Weinhold, I.; Gurtner, S. Rural—Urban differences in determinants of patient satisfaction with primary care. Soc. Sci. Med. 2018, 212, 76–85. [Google Scholar] [CrossRef]
- Alrasheedi, K.F.; AL-Mohaithef, M.; Edrees, H.H.; Chandramohan, S. The Association Between Wait Times and Patient Satisfaction: Findings from Primary Health Centers in the Kingdom of Saudi Arabia. Health Serv. Res. Manag. Epidemiol. 2019, 6, 233339281986124. [Google Scholar] [CrossRef]
- Anderson, R.T.; Camacho, F.T.; Balkrishnan, R. Willing to wait: The influence of patient wait time on satisfaction with primary care. BMC Health Serv. Res. 2007, 7, 31. [Google Scholar] [CrossRef]
- Emberley-Burke, W.; Meadus, R.J.; Twomey, J.C.; Kean, K.P. Patient satisfaction with nurse practitioner care in Newfoundland and Labrador. Clin. Nurs. Stud. 2018, 6, 101. [Google Scholar] [CrossRef]
- Messina, G.; Vencia, F.; Mecheroni, S.; Dionisi, S.; Baragatti, L.; Nante, N. Factors Affecting Patient Satisfaction with Emergency Department Care: An Italian Rural Hospital. Glob. J. Health Sci. 2014, 7, 30. [Google Scholar] [CrossRef]
- Chimbindi, N.; Bärnighausen, T.; Newell, M.-L. Patient satisfaction with HIV and TB treatment in a public programme in rural KwaZulu-Natal: Evidence from patient-exit interviews. BMC Health Serv. Res. 2014, 14, 32. [Google Scholar] [CrossRef] [PubMed]
- Batbaatar, E.; Dorjdagva, J.; Luvsannyam, A.; Savino, M.M.; Amenta, P. Determinants of patient satisfaction: A systematic review. Perspect Public Health 2017, 137, 89–101. [Google Scholar] [CrossRef] [PubMed]
- Schmets, G.; Rajan, D.; Kadandale, S. Strategizing National Health in the 21st Century: A Handbook; World Health Organization: Geneva, Switzerland, 2016. [Google Scholar]
- United Nations, Department of Economic and Social Affairs, Population Division. World Urbanization Prospects: The 2018 Revision; United Nations: New York, NY, USA, 2018. [Google Scholar]
- Aldana, J.M.; Piechulek, H.; Al-Sabir, A. Client satisfaction and quality of health care in rural Bangladesh. Bull. World Health Organ. 2001, 79, 512–517. [Google Scholar]
- Smith, K.B.; Humphreys, J.S.; Jones, J.A. Essential tips for measuring levels of consumer satisfaction with rural health service quality. Rural Remote Health 2006, 6, 594. [Google Scholar]
- Boovaragasamy, C.; Narayanan, S. Patients’ satisfaction regarding facilities and services provided at AYUSH clinics of primary health centres in rural Puducherry. Int. J. Community Med. Public Health 2019, 6, 2498. [Google Scholar] [CrossRef]
- Enakshi, G.; Pawan, K.S. Client satisfaction with quality of health care in a rural area in Southern India. J. Public Health Epidemiol. 2014, 6, 239–245. [Google Scholar] [CrossRef] [Green Version]
- Mutaganzwa, C.; Wibecan, L.; Iyer, H.S.; Nahimana, E.; Manzi, A.; Biziyaremye, F.; Nyishime, M.; Nkikabahizi, F.; Hirschhorn, L.R.; Magge, H. Advancing the health of women and newborns: Predictors of patient satisfaction among women attending antenatal and maternity care in rural Rwanda. Int. J. Qual. Health Care 2018, 30, 793–801. [Google Scholar] [CrossRef]
- Roy, A.; van der Weijden, T.; de Vries, N. Predictors and consequences of rural clients’ satisfaction level in the district public-private mixed health system of Bangladesh. Glob. Health Res. Policy 2017, 2, 31. [Google Scholar] [CrossRef]
- López-Cevallos, D.F.; Harvey, S.M.; Warren, J.T. Medical Mistrust, Perceived Discrimination, and Satisfaction with Health Care Among Young-Adult Rural Latinos: Satisfaction with Care Among Rural Latinos. J. Rural Health 2014, 30, 344–351. [Google Scholar] [CrossRef]
- Ryan, K.; Rahman, A. Examining factors influencing patient satisfaction with nurse practitioners in rural urgent care centers: Patient satisfaction among users of rural UCCs. J. Am. Acad. Nurse Pract. 2012, 24, 77–81. [Google Scholar] [CrossRef]
- Gu, D.; Yang, X.; Li, X.; Liang, C.; Zhong, J.; Feng, N. Innovating New Rural Cooperative Medical Scheme (NCMS) for Better Patient Satisfaction in Rural China. Int. J. Environ. Res. Public Health 2018, 15, 2007. [Google Scholar] [CrossRef] [PubMed]
- Liu, Y.; Yuan, Z.; Liu, Y.; Jayasinghe, U.W.; Harris, M.F. Changing community health service delivery in economically less-developed rural areas in China: Impact on service use and satisfaction. BMJ Open 2014, 4, e004148. [Google Scholar] [CrossRef] [PubMed]
- Yan, Z.; Wan, D.; Li, L. Patient satisfaction in two Chinese provinces: Rural and urban differences. Int. J. Qual. Health Care 2011, 23, 384–389. [Google Scholar] [CrossRef] [PubMed]
- Godley, M.; Jenkins, J.B. Decreasing Wait Times and Increasing Patient Satisfaction: A Lean Six Sigma Approach. J. Nurs. Care Qual. 2019, 34, 61–65. [Google Scholar] [CrossRef]
- Wu, J.; Zhang, S.; Chen, H.; Lin, Y.; Dong, X.; Yin, X.; Lu, Z.; Cao, S. Patient Satisfaction with Community Health Service Centers as Gatekeepers and the Influencing Factors: A Cross-Sectional Study in Shenzhen, China. PLoS ONE 2016, 11, e0161683. [Google Scholar] [CrossRef]
- Shan, L.; Li, Y.; Ding, D.; Wu, Q.; Liu, C.; Jiao, M.; Hao, Y.; Han, Y.; Gao, L.; Hao, J.; et al. Patient Satisfaction with Hospital Inpatient Care: Effects of Trust, Medical Insurance and Perceived Quality of Care. PLoS ONE 2016, 11, e0164366. [Google Scholar] [CrossRef]
- Huerta, T.R.; Harle, C.A.; Ford, E.W.; Diana, M.L.; Menachemi, N. Measuring Patient Satisfaction’s Relationship to Hospital Cost Efficiency: Can Administrators Make a Difference? Health Care Manag. Rev. 2016, 41, 56–63. [Google Scholar] [CrossRef]
- National Health Commission of the People’s Republic of China. China Health Statistical Yearbook 2018; Peking Union Medical College Press: Beijing, China, 2018. [Google Scholar]
- Lv, Y.; Xue, C.; Ge, Y.; Ye, F.; Liu, X.; Liu, Y.; Zhang, L. Analysis of Factors Influencing Inpatient and Outpatient Satisfaction with the Chinese Military Health Service. PLoS ONE 2016, 11, e0151234. [Google Scholar] [CrossRef]
- Tang, L. The influences of patient’s trust in medical service and attitude towards health policy on patient’s overall satisfaction with medical service and sub satisfaction in China. BMC Public Health 2011, 11, 472. [Google Scholar] [CrossRef]
- Platonova, E.A.; Kennedy, K.N.; Shewchuk, R.M. Understanding Patient Satisfaction, Trust, and Loyalty to Primary Care Physicians. Med. Care Res. Rev. 2008, 65, 696–712. [Google Scholar] [CrossRef]
- Munro, N.; Duckett, J. Explaining public satisfaction with health-care systems: Findings from a nationwide survey in China. Health Expect. 2016, 19, 654–666. [Google Scholar] [CrossRef] [PubMed]
- Bjertnaes, O.A.; Sjetne, I.S.; Iversen, H.H. Overall patient satisfaction with hospitals: Effects of patient-reported experiences and fulfilment of expectations. BMJ Qual. Saf. 2012, 21, 39–46. [Google Scholar] [CrossRef] [PubMed]
- Knudtson, N. Patient Satisfaction with Nurse Practitioner Service in a Rural Setting. J. Am. Acad. Nurse Pract. 2000, 12, 405–412. [Google Scholar] [CrossRef] [PubMed]
- Xiao, H.; Barber, J.P. The Effect of Perceived Health Status on Patient Satisfaction. Value Health 2008, 11, 719–725. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Becker, G.; Newsom, E. Socioeconomic Status and Dissatisfaction with Health Care Among Chronically Ill African Americans. Am. J. Public Health 2003, 93, 742–748. [Google Scholar] [CrossRef] [PubMed]
- Findik, U.Y.; Unsar, S.; Sut, N. Patient satisfaction with nursing care and its relationship with patient characteristics. Nurs. Health Sci. 2010, 12, 162–169. [Google Scholar] [CrossRef] [PubMed]



{kind=link}
{kind=link}
| Characteristics | Rural Outpatients (N = 5208) | Rural Inpatients (N = 4603) | ||||||
|---|---|---|---|---|---|---|---|---|
| N (%) | Overall Satisfaction with Medical Services | N (%) | Overall Satisfaction with Medical Services | |||||
| Mean + SD | One-Way ANOVA | Mean + SD | One-Way ANOVA | |||||
| F-value | p-value | F-value | p-value | |||||
| Gender | 0.003 | 0.954 | 0.038 | 0.845 | ||||
| Female | 2953 (57.0) | 3.61 ± 0.853 | 2542 (55.8) | 3.80 ± 0.809 | ||||
| Male | 2232 (43.0) | 3.61 ± 0.862 | 2014 (44.2) | 3.79 ± 0.849 | ||||
| Age | 12.924 | <0.001 | 6.940 | 0.001 | ||||
| ≤30 years | 1898 (36.9) | 3.54 ± 0.866 | 1380 (30.4) | 3.73 ± 0.895 | ||||
| 31–45 years | 1706 (33.2) | 3.63 ± 0.894 | 1176 (25.9) | 3.80 ± 0.833 | ||||
| ≥46 years | 1537 (29.9) | 3.69 ± 0.795 | 1984 (43.7) | 3.84 ± 0.774 | ||||
| Education | 0.545 | 0.651 | 0.389 | 0.761 | ||||
| Illiteracy | 700 (13.5) | 3.60 ± 0.872 | 742 (16.2) | 3.77 ± 0.825 | ||||
| Primary school | 1126 (21.7) | 3.63 ± 0.826 | 1277 (27.9) | 3.80 ± 0.778 | ||||
| Junior high school | 1693 (32.6) | 3.60 ± 0.840 | 1281 (28.0) | 3.79 ± 0.832 | ||||
| ≥ Senior high school | 1674 (32.2) | 3.63 ± 0.888 | 1276 (27.9) | 3.81 ± 0.881 | ||||
| Occupation | 9.457 | 0.002 | 1.512 | 0.219 | ||||
| Nonfarmer | 2987 (57.8) | 3.58 ± 0.863 | 2337 (51.0) | 3.78 ± 0.869 | ||||
| Farmer | 2182 (42.2) | 3.66 ± 0.849 | 2248 (49.0) | 3.81 ± 0.787 | ||||
| Income | 4.690 | 0.009 | 0.877 | 0.416 | ||||
| No regular income | 1328 (25.7) | 3.57 ± 0.831 | 1503 (32.9) | 3.78 ± 0.844 | ||||
| ≤2000 Yuan | 2362 (45.7) | 3.60 ± 0.867 | 1914 (41.9) | 3.79 ± 0.806 | ||||
| ≥2001 Yuan | 1482 (28.7) | 3.67 ± 0.866 | 1152 (25.2) | 3.82 ± 0.846 | ||||
| Type of hospital * | 4.089 | 0.007 | 20.807 | <0.001 | ||||
| TH | 2040 (39.2) | 3.63 ± 0.870 | 1573 (34.2) | 3.67 ± 0.777 | ||||
| MCHH | 835 (16.0) | 3.66 ± 0.800 | 669 (14.5) | 3.88 ± 0.815 | ||||
| TCMH | 896 (17.2) | 3.64 ± 0.863 | 876 (19.0) | 3.85 ± 0.853 | ||||
| CGH | 1437 (27.6) | 3.55 ± 0.861 | 1485 (32.3) | 3.87 ± 0.858 | ||||
| Indicators | Likert 5-Point Scale of Outpatient Satisfaction, N (%) | Satisfaction Score | Spearman Correlation with Overall Satisfaction | |||||
|---|---|---|---|---|---|---|---|---|
| Strongly Dissatisfied | Dissatisfied | Neither Dissatisfied nor Satisfied | Satisfied | Strongly Satisfied | Mean ± SD | Coefficient | p-value | |
| Travel time | 160 (3.1) | 569 (11.0) | 2446 (47.1) | 1407 (27.1) | 613 (11.8) | 3.34 ± 0.929 | 0.121 | <0.001 |
| Waiting time | 237 (4.6) | 840 (16.2) | 2379 (45.8) | 1337 (25.7) | 403 (7.8) | 3.16 ± 0.941 | 0.178 | <0.001 |
| Illness explanation | 85 (1.6) | 206 (4.0) | 1851 (35.6) | 2294 (44.1) | 760 (14.6) | 3.66 ± 0.833 | 0.331 | <0.001 |
| Treatment consultation | 161 (3.1) | 223 (4.3) | 2042 (39.3) | 2086 (40.1) | 686 (13.2) | 3.56 ± 0.884 | 0.316 | <0.001 |
| Medical technology | 55 (1.1) | 194 (3.7) | 2447 (47.0) | 1966 (37.8) | 541 (10.4) | 3.53 ± 0.772 | 0.376 | <0.001 |
| Medical service attitude | 71 (1.4) | 204 (3.9) | 1624 (31.2) | 2176 (41.9) | 1124 (21.6) | 3.78 ± 0.873 | 0.352 | <0.001 |
| Medical facility | 95 (1.9) | 458 (9.0) | 2560 (50.3) | 1637 (32.2) | 335 (6.6) | 3.33 ± 0.802 | 0.283 | <0.001 |
| Hospital environment | 193 (3.7) | 484 (9.3) | 2519 (48.5) | 1639 (31.5) | 363 (7.0) | 3.29 ± 0.868 | 0.290 | <0.001 |
| Medical expenses | 112 (2.2) | 820 (15.8) | 2420 (46.5) | 1421 (27.3) | 431 (8.3) | 3.24 ± 0.890 | 0.217 | <0.001 |
| Overall satisfaction | 117 (2.2) | 322 (6.2) | 1635 (31.4) | 2514 (48.3) | 620 (11.9) | 3.61 ± 0.857 | N/A | |
| Indicators | Likert 5-point Scale of Inpatient Satisfaction, N (%) | Satisfaction Score | Spearman Correlation with Overall Satisfaction | |||||
|---|---|---|---|---|---|---|---|---|
| Strongly Dissatisfied | Dissatisfied | Neither Dissatisfied nor Satisfied | Satisfied | Strongly Satisfied | Mean ± SD | Coefficient | p-value | |
| Illness explanation | 37 (0.8) | 73 (1.6) | 1042 (22.7) | 1899 (41.4) | 1540 (33.5) | 4.05 ± 0.834 | 0.395 | <0.001 |
| Treatment consultation | 67 (1.5) | 114 (2.5) | 1138 (24.8) | 1929 (42.1) | 1335 (29.1) | 3.95 ± 0.877 | 0.378 | <0.001 |
| Medical technology | 52 (1.1) | 124 (2.7) | 1490 (32.4) | 2153 (46.8) | 778 (16.9) | 3.76 ± 0.803 | 0.430 | <0.001 |
| Medical service attitude | 147 (3.2) | 152 (3.3) | 970 (21.2) | 1997 (43.5) | 1320 (28.8) | 3.91 ± 0.956 | 0.449 | <0.001 |
| Trust in physicians | 68 (1.6) | 116 (2.7) | 910 (21.3) | 2045 (47.9) | 1134 (26.5) | 3.95 ± 0.853 | 0.463 | <0.001 |
| Medical facility | 65 (1.4) | 278 (6.1) | 1897 (41.3) | 1632 (35.6) | 717 (15.6) | 3.58 ± 0.873 | 0.343 | <0.001 |
| Hospital environment | 85 (2.0) | 236 (5.5) | 1694 (39.6) | 1528 (35.8) | 730 (17.1) | 3.60 ± 0.900 | 0.388 | <0.001 |
| Medical expenses | 151 (3.3) | 669 (14.6) | 2414 (52.7) | 982 (21.4) | 368 (8.0) | 3.16 ± 0.887 | 0.205 | <0.001 |
| Overall satisfaction | 98 (2.1) | 157 (3.4) | 1082 (23.5) | 2505 (54.4) | 761 (16.5) | 3.80 ± 0.829 | N/A | |
| Variables | Multiple Linear Regression | Binary Logistic Regression | ||||||
|---|---|---|---|---|---|---|---|---|
| B (95% CI) | S.E. 1 | t-Value | p-Value | B | S.E. 1 | OR (95% CI) | p-Value | |
| Travel time | 0.050 (0.024, 0.076) | 0.013 | 3.798 | <0.001 | 0.168 | 0.040 | 1.18 (1.09, 1.28) | <0.001 |
| Waiting time | 0.033 (0.007, 0.060) | 0.013 | 2.480 | 0.013 | 0.142 | 0.040 | 1.15 (1.07, 1.25) | <0.001 |
| Illness explanation | 0.053 (0.019, 0.088) | 0.018 | 3.019 | 0.003 | 0.207 | 0.052 | 1.23 (1.11, 1.36) | <0.001 |
| Treatment consultation | 0.024 (−0.008, 0.056) | 0.016 | 1.446 | 0.148 | 0.031 | 0.048 | 1.03 (0.94, 1.13) | 0.522 |
| Medical technology | 0.181 (0.147, 0.215) | 0.017 | 10.495 | <0.001 | 0.550 | 0.052 | 1.73 (1.57, 1.92) | <0.001 |
| Medical service attitude | 0.129 (0.099, 0.159) | 0.015 | 8.396 | <0.001 | 0.411 | 0.045 | 1.51 (1.38, 1.65) | <0.001 |
| Medical facility | 0.097 (0.064, 0.129) | 0.017 | 5.831 | <0.001 | 0.241 | 0.051 | 1.27 (1.15, 1.41) | <0.001 |
| Hospital environment | 0.100 (0.067, 0.133) | 0.017 | 5.976 | <0.001 | 0.205 | 0.050 | 1.23 (1.11, 1.36) | <0.001 |
| Medical expenses | 0.071 (0.044, 0.097) | 0.013 | 5.279 | <0.001 | 0.141 | 0.041 | 1.15 (1.06, 1.25) | 0.001 |
| Age (31–45 years) | 0.035 (−0.018, 0.088) | 0.027 | 1.302 | 0.193 | 0.120 | 0.080 | 1.13 (0.96, 1.32) | 0.133 |
| Age (≥46 years) | 0.074 (0.018, 0.130) | 0.029 | 2.573 | 0.010 | 0.228 | 0.086 | 1.26 (1.06, 1.49) | 0.008 |
| Occupation (Farmer) | 0.045 (−0.004, 0.095) | 0.025 | 1.788 | 0.074 | 0.043 | 0.076 | 1.04 (0.90, 1.21) | 0.574 |
| Income (≤2000 Yuan) | 0.020 (−0.033, 0.074) | 0.027 | 0.738 | 0.461 | 0.156 | 0.081 | 1.17 (1.00, 1.37) | 0.055 |
| Income (≥2001 Yuan) | 0.104 (0.042, 0.166) | 0.032 | 3.270 | 0.001 | 0.223 | 0.095 | 1.25 (1.03, 1.51) | 0.019 |
| Type of hospital (MCHH 2) | 0.050 (−0.017, 0.116) | 0.034 | 1.459 | 0.145 | 0.001 | 0.102 | 1.00 (0.82, 1.22) | 0.993 |
| Type of hospital (TCMH 3) | 0.063 (0.000, 0.126) | 0.032 | 1.951 | 0.051 | 0.006 | 0.096 | 1.01 (0.83, 1.22) | 0.950 |
| Type of hospital (CGH 4) | −0.063 (−0.118, −0.007) | 0.028 | −2.214 | 0.027 | −0.283 | 0.085 | 0.75 (0.64, 0.89) | 0.001 |
| Variables | Multiple Linear Regression | Binary Logistic Regression | ||||||
|---|---|---|---|---|---|---|---|---|
| B (95% CI) | S.E. 1 | t-Value | p-Value | B | S.E. 1 | OR (95% CI) | p-Value | |
| Illness explanation | 0.130 (0.096, 0.165) | 0.018 | 7.362 | <0.001 | 0.485 | 0.066 | 1.62 (1.43, 1.85) | <0.001 |
| Treatment consultation | 0.010 (−0.024, 0.043) | 0.017 | 0.559 | 0.576 | −0.026 | 0.064 | 0.97 (0.86, 1.10) | 0.681 |
| Medical technology | 0.084 (0.051, 0.117) | 0.017 | 4.985 | <0.001 | 0.359 | 0.064 | 1.43 (1.26, 1.62) | <0.001 |
| Medical service attitude | 0.151 (0.127, 0.175) | 0.012 | 12.226 | <0.001 | 0.591 | 0.046 | 1.81 (1.65, 1.98) | <0.001 |
| Trust in physicians | 0.218 (0.190, 0.246) | 0.014 | 15.459 | <0.001 | 0.718 | 0.054 | 2.05 (1.85, 2.28) | <0.001 |
| Medical facility | 0.029 (−0.002, 0.060) | 0.016 | 1.845 | 0.065 | 0.044 | 0.063 | 1.05 (0.93, 1.18) | 0.480 |
| Hospital environment | 0.115 (0.085, 0.145) | 0.015 | 7.434 | <0.001 | 0.403 | 0.061 | 1.50 (1.33, 1.69) | <0.001 |
| Medical expenses | 0.086 (0.061, 0.110) | 0.013 | 6.871 | <0.001 | 0.446 | 0.052 | 1.56 (1.41, 1.73) | <0.001 |
| Age (31–45 years) | 0.059 (0.003, 0.116) | 0.029 | 2.072 | 0.038 | 0.225 | 0.110 | 1.25 (1.01, 1.55) | 0.042 |
| Age (≥46 years) | 0.065 (0.013, 0.117) | 0.027 | 2.434 | 0.015 | 0.326 | 0.103 | 1.39 (1.13, 1.70) | 0.002 |
| Type of hospital (MCHH 2) | 0.185 (0.116, 0.254) | 0.035 | 5.252 | <0.001 | 0.514 | 0.137 | 1.67 (1.28, 2.19) | <0.001 |
| Type of hospital (TCMH 3) | 0.097 (0.035, 0.159) | 0.032 | 3.075 | 0.002 | 0.669 | 0.128 | 1.95 (1.52, 2.51) | <0.001 |
| Type of hospital (CGH 4) | 0.072 (0.019, 0.125) | 0.027 | 2.678 | 0.007 | 0.286 | 0.103 | 1.33 (1.09, 1.63) | 0.006 |
© 2019 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Liu, J.; Mao, Y. Patient Satisfaction with Rural Medical Services: A Cross-Sectional Survey in 11 Western Provinces in China. Int. J. Environ. Res. Public Health 2019, 16, 3968. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph16203968
Liu J, Mao Y. Patient Satisfaction with Rural Medical Services: A Cross-Sectional Survey in 11 Western Provinces in China. International Journal of Environmental Research and Public Health. 2019; 16(20):3968. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph16203968
Chicago/Turabian StyleLiu, Jinlin, and Ying Mao. 2019. "Patient Satisfaction with Rural Medical Services: A Cross-Sectional Survey in 11 Western Provinces in China" International Journal of Environmental Research and Public Health 16, no. 20: 3968. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph16203968