Parental Declaration of Adverse Event Following Immunization in a Cross-Sectional Study in Poland


Abstract
:1. Introduction
2. Material and Methods
- Did your child/children ever have a post-vaccination reaction after immunization? If yes, what were the symptoms?
- Has your child/children ever had any medical contraindications for vaccinations diagnosed by a physician?
- Do you think that qualifying tests for vaccination among children in Poland are carried out?
- Do you think that current childhood vaccinations are safe enough?
- Which of the following sources of knowledge about immunization is currently the source of your perception?
2.1. Statistical Analysis
3. Results
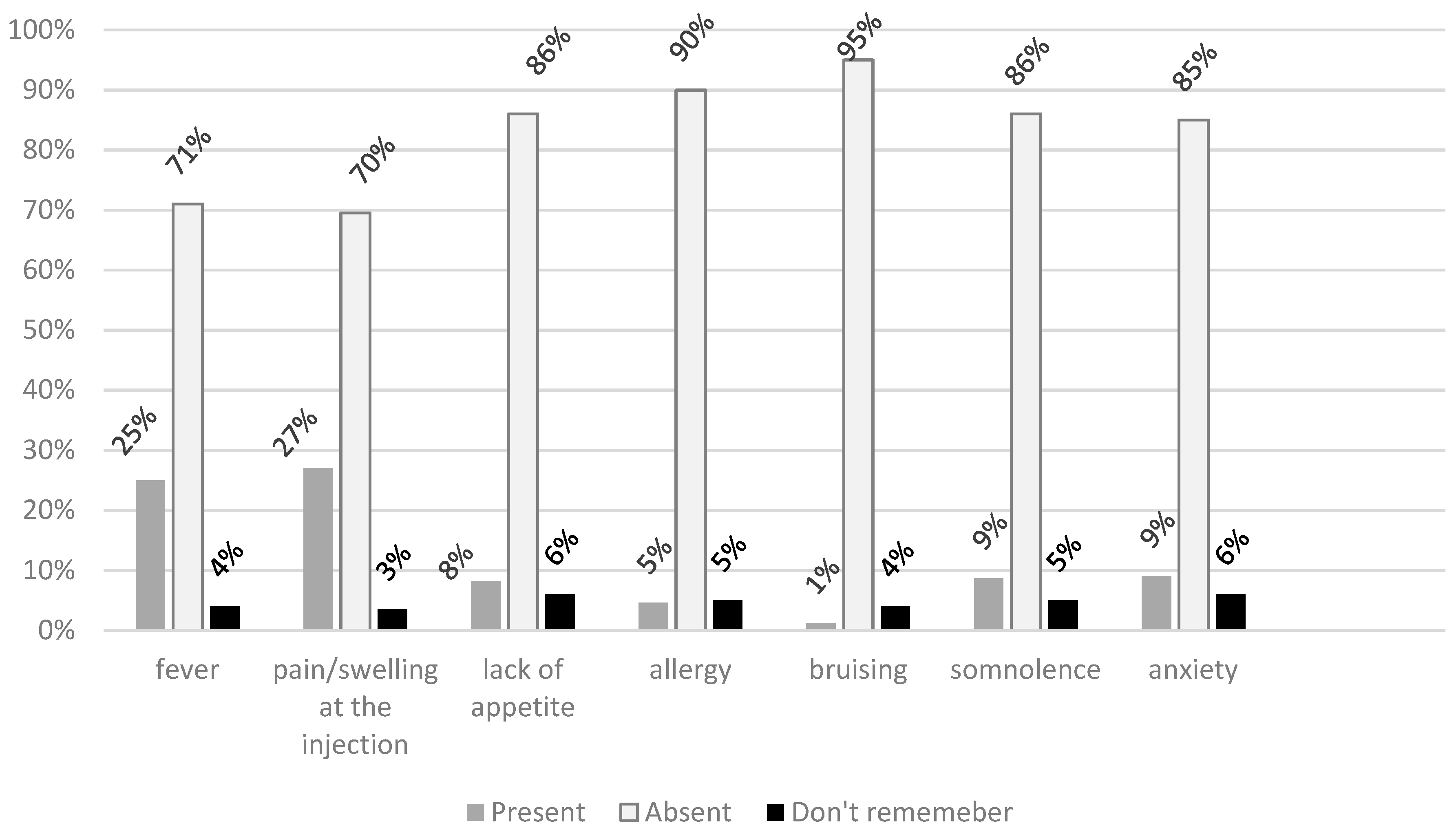
3.1. Frequency of Reported AEFI
3.2. Characteristics of Respondents and their Relation to AEFI
3.3. Reported AEFI according to the Respondent’s Perception of Vaccination
4. Discussion
4.1. Frequency of Declared AEFI and Demographic Profile of AEFI Reporters
4.2. Factors Associated with Reported AEFI
4.3. Surveillance and Physician’s Role in Reporting AEFI
4.4. Limitations of the Study
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- Plotkin, S. History of vaccination. Proc. Natl. Acad. Sci. USA 2014, 111, 12283–12287. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Lane, J.M.; Ruben, F.L.; Neff, J.M.; Millar, J.D. Complications of Smallpox Vaccination, 1968: Results of Ten Statewide Surveys. J. Infect. Dis. 1970, 122, 303–309. [Google Scholar] [CrossRef] [PubMed]
- Czarkowski, M.P.; Kondej, B.; Staszewska-Jakubik, E.; Cielebąk, E. Vaccinations in Poland in the years 2000–2016. National Institute of Public Health—State Institute of Hygiene—Department of Epidemiology. Available online: http://wwwold.pzh.gov.pl/oldpage/epimeld/2016/Sz_2016.pdf (accessed on 11 March 2019).
- WHO. Adverse Events Following Immunization (AEFI) Global Vaccine Safety. Available online: https://www.who.int/vaccine_safety/initiative/detection/AEFI/en/ (accessed on 9 June 2019).
- Parrella, A.; Gold, M.; Marshall, H.; Braunack-Mayer, A.; Baghurst, P. Parental perspectives of vaccine safety and experience of adverse events following immunisation. Vaccine 2013, 31, 2067–2074. [Google Scholar] [CrossRef] [PubMed]
- Regulation of the Minister of Health on adverse post-vaccination reactions and criteria for their recognition from 21th December, 2010, Dz.U. J. Laws 2010, 254, 1711.
- Central Statistical Office Local Data Bank. Available online: https://bdl.stat.gov.pl/BDL/start (accessed on 28 March 2019).
- Braczkowska, B.; Kowalska, M.; Baranski, K.; Gajda, M.; Kurowski, T.; Zejda, J.E. Parental Opinions and Attitudes about Children’s Vaccination Safety in Silesian Voivodeship, Poland. Int. J. Environ. Res. Public Health 2018, 15, 756. [Google Scholar] [CrossRef] [PubMed]
- Koperny, M.; Bała, M.; Bandoła, K.; Seweryn, M.; Żak, J. Analysis of adverse events following immunization in Poland between 2003–2012. ProblHig Epidemiol. 2014, 95, 609–615. [Google Scholar]
- Newes-Adeyi, G.; Greece, J.; Bozeman, S.; Walker, D.K.; Lewis, F.; Gidudu, J. Active surveillance for influenza vaccine adverse events: The integrated vaccine surveillance system. Vaccine 2012, 30, 1050–1055. [Google Scholar] [CrossRef] [PubMed]
- Ahmadipour, N.; Watkins, K.; Fréchette, M.; Coulby, C.; Anyoti, H.; Johnson, K. Vaccine safety surveillance in Canada: Reports to CAEFISS, 2013–2016. Can. Commun. Dis. Rep. 2018, 44, 206–214. [Google Scholar] [CrossRef] [PubMed]
- Patterson, J.; Kagina, B.M.; Gold, M.; Hussey, G.D.; Muloiwa, R. Comparison of adverse events following immunization with acellular and whole-cell pertussis vaccines: A systematic review. Vaccine 2018, 36, 6007–6016. [Google Scholar] [CrossRef] [PubMed]
- Parrella, A.; Gold, M.; Braunack-Mayer, A.; Baghurts, P.; Marshall, H. Consumer reporting of adverse events following immunization (AEFI) Identifying predictors of reporting an AEFI. Hum. VaccinImmunother. 2014, 10, 747–754. [Google Scholar] [CrossRef]
- Kata, A. Anti-vaccine activists, Web 2.0, and the postmodern paradigm—An overview of tactics and tropes used online by the anti-vaccination movement. Vaccine 2012, 30, 3778–3789. [Google Scholar] [CrossRef] [PubMed]
- Danova, J.; Kocourkova, A.; Celko, A.M. Active surveillance study of adverse events following immunisation of children in the Czech Republic. BMC Public Health 2017, 17, 167. [Google Scholar] [CrossRef] [PubMed]
- United States Department of Health and Human Services (DHHS), Public Health Service (PHS), Centers for Disease Control (CDC)/Food and Drug Administration (FDA), Vaccine Adverse Event Reporting System (VAERS). 1990—Last Month, CDC WONDER On-line Database. Available online: http://wonder.cdc.gov/vaers.html (accessed on 15 May 2019).
- Bosch-Capblanch, X.; Banerjee, K.; Burton, A.; Bosch-Capblanch, X. Unvaccinated children in years of increasing coverage: How many and who are they? Evidence from 96 low- and middle-income countries. Trop. Med. Int. Health 2012, 17, 697–710. [Google Scholar] [CrossRef] [PubMed]
- Parrella, A.; Braunack-Mayer, A.; Gold, M.; Marshall, H.; Baghurst, P. Healthcare providers’ knowledge, experience and challenges of reporting adverse events following immunisation: A qualitative study. BMC Health Serv. Res. 2013, 13, 313. [Google Scholar] [CrossRef] [PubMed]
- Gorman, D.; Bielecki, K.; Willocks, L.; Pollock, K. A qualitative study of vaccination behaviour amongst female Polish migrants in Edinburgh, Scotland. Vaccine 2019, 37, 2741–2747. [Google Scholar] [CrossRef] [PubMed] [Green Version]


{kind=link}
| Variable | Value | Level of Education | Number of Children | Place of Residence | Financial Situation | ||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Lower | Higher | p | One | More | p | Small City | Big City | p | Bad | Better | p | ||
| N = 597 | N = 642 | N = 390 | N = 849 | N = 168 | N = 1071 | N = 25 | N = 1214 | ||||||
| Any AEFI | Yes | 162; 27.1% | 232; 36.1% | ** | 98; 25.2% | 296; 34.9% | ** | 57; 34.0 | 337; 31.5 | NS | 7; 28.0 | 387; 31.9 | NS |
| No | 435; 72.9% | 410; 63.9% | 292; 74.8% | 553; 65.1% | 111; 66.0 | 734; 68.5 | 18; 72.0 | 808; 68.1 | |||||
| Fever | Yes | 132; 22.1 | 177; 27.6 | ** | 74; 19.0 | 235; 27.7 | ** | 52; 31.0 | 257; 24.0 | NS | 4; 16.0 | 305; 25.1 | NS |
| No | 465; 77.9 | 465; 72.4 | 316; 81.0 | 614; 72.3 | 116; 69.0 | 814; 76.0 | 21; 84.0 | 909; 74.9 | |||||
| At the injection | Yes | 143; 23.9 | 192; 29.9 | ** | 83; 21.3 | 252; 29.7 | ** | 47; 28.0 | 288; 26.9 | NS | 6; 24.0 | 329; 27.1 | NS |
| No | 454; 76.1 | 450; 70,1 | 307; 78.7 | 597; 70.3 | 121; 72.0 | 783; 73.1 | 19; 76.0 | 885; 72.9 | |||||
| Lack of appetite | Yes | 45; 7.5 | 57; 8.9 | NS | 17; 4.4 | 85; 10.0 | ** | 10; 5.9 | 92; 8.6 | NS | 4; 16.0 | 98; 8.1 | NS |
| No | 552; 92.5 | 585; 91.1 | 373; 95.6 | 764; 90.0 | 158; 94.1 | 979; 91.4 | 21; 84.0 | 91.9 | |||||
| Allergy | Yes | 21; 3.5 | 36; 5.6 | NS | 11; 2.8 | 46; 5.4 | ** | 10; 5.9 | 47; 4.4 | NS | 0 | 57; 4.7 | N/A |
| No | 576; 96.5 | 606; 94.4 | 379; 97.2 | 803; 95.6 | 158; 94.1 | 1024; 95.6 | 25 | 1157; 95.3 | |||||
| Bruising | Yes | 11; 1.8 | 4; 0.6 | NS, F | 1; 0.2 | 14; 1.6 | ** F | 3; 1.8 | 12; 1.1 | NS | 0 | 15; 1.2 | N/A |
| No | 586; 98.2 | 638; 99.4 | 389; 99.8 | 835; 98.4 | 165; 98.2 | 1059; 98.9 | 25 | 1199; 98.8 | |||||
| Somnolence | Yes | 54; 9.0 | 54; 8.4 | NS | 18; 4,6 | 90; 10.6 | ** | 13; 7.7 | 95; 8.9 | NS | 2; 8.0 | 106; 8.7 | NS |
| No | 543; 91.0 | 588; 91.6 | 372; 95.4 | 759; 89.4 | 155; 92.3 | 976; 91.1 | 23; 92.0 | 1108; 91.3 | |||||
| Anxiety | Yes | 48; 8.0 | 64; 10.0 | NS | 25; 6.4 | 87; 10.2 | ** | 16; 9.5 | 96; 9.0 | NS | 2; 8.0 | 110; 9.0 | NS |
| No | 549; 92.0 | 578; 90.0 | 365; 93.6 | 762; 89.8 | 152; 90.5 | 975; 91.0 | 23; 92.0 | 1104; 91.0 | |||||
| Parental Opinion N = (1220) | AEFI (Adverse Event Following Immunization) | |||
|---|---|---|---|---|
| Yes | No | p | ||
| N = 394 | N = 826 | |||
| a. Vaccinations are a very important method for the prevention of infectious diseases | Yes | 360 | 771 | NS |
| No | 34 | 55 | ||
| b. The evidence of vaccinations’ efficacy is insufficient | Yes | 97 | 238 | NS |
| No | 297 | 588 | ||
| c. Vaccinations did not provide long-term immunity | Yes | 119 | 196 | ** |
| No | 275 | 630 | ||
| d. Being sick with an infectious disease results in better immunity than vaccination | Yes | 66 | 120 | NS |
| No | 328 | 706 | ||
| e. The realization of vaccination is indicative of parents’ concern for children’s health | Yes | 337 | 726 | NS |
| No | 57 | 100 | ||
| f. The current vaccination strategy is reasonable | Yes | 223 | 604 | *** |
| No | 171 | 222 | ||
| g. Vaccination should not be performed too early | Yes | 101 | 123 | *** |
| No | 293 | 703 | ||
| h. The number of vaccinations is too high and should be reduced | Yes | 100 | 111 | *** |
| No | 294 | 715 | ||
| i. The vaccination costs outweigh the benefits | Yes | 66 | 121 | NS |
| No | 328 | 795 | ||
| j. Education in this subject is sufficient | Yes | 72 | 173 | NS |
| No | 322 | 653 | ||
| k. Information on the unwanted post-vaccination reactions is sufficient | Yes | 97 | 238 | NS |
| No | 297 | 588 | ||
| Parameter | Odds Ratio Estimates | |||
|---|---|---|---|---|
| Point Estimates | Adjusted OR (95% CI) | p Value | ||
| Number of vaccines (n) | quantitative variable | 1.026 | 1.01–1.04 | <0.001 |
| Education level | lower vs. higher | 0.723 | 0.56–0.93 | 0.01 |
| Vaccination are safe | yes vs. no | 0.554 | 0.42–0.73 | <0.001 |
| Current vaccination strategy is reasonable | yes vs. no | 0.640 | 0.48–0.84 | 0.001 |
| The number of vaccines is too high and should be decreased | yes vs. no | 1.648 | 1.18–2.88 | 0.002 |
© 2019 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Barański, K.; Gajda, M.; Braczkowska, B.; Kowalska, M. Parental Declaration of Adverse Event Following Immunization in a Cross-Sectional Study in Poland. Int. J. Environ. Res. Public Health 2019, 16, 4038. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph16204038
Barański K, Gajda M, Braczkowska B, Kowalska M. Parental Declaration of Adverse Event Following Immunization in a Cross-Sectional Study in Poland. International Journal of Environmental Research and Public Health. 2019; 16(20):4038. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph16204038
Chicago/Turabian StyleBarański, Kamil, Maksymilian Gajda, Bogumiła Braczkowska, and Małgorzata Kowalska. 2019. "Parental Declaration of Adverse Event Following Immunization in a Cross-Sectional Study in Poland" International Journal of Environmental Research and Public Health 16, no. 20: 4038. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph16204038