Prevalence of Falls on Mount Fuji and Associated with Risk Factors: A Questionnaire Survey Study


Abstract
:1. Introduction
2. Materials and Methods
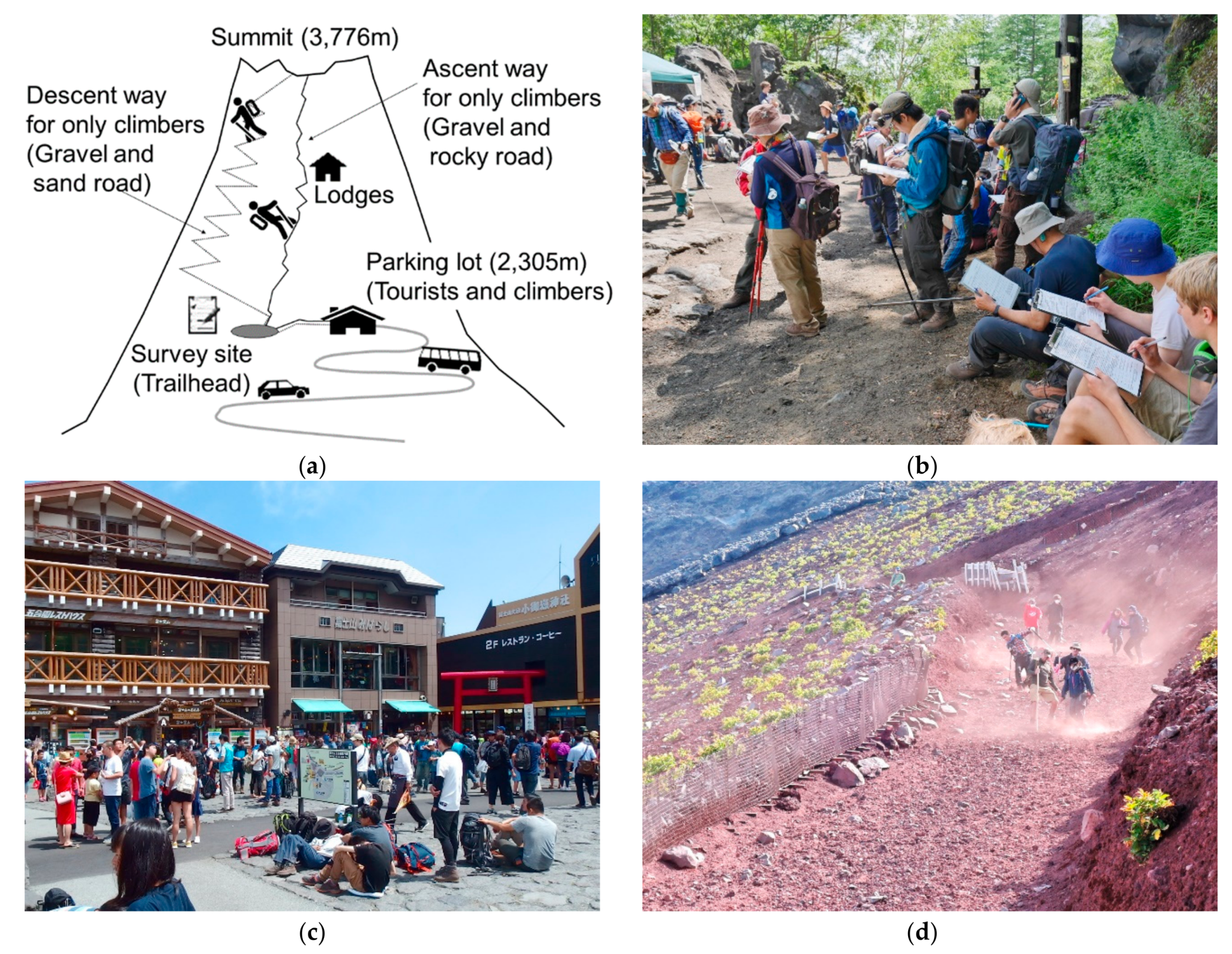
2.1. Survey Site
2.2. Participants
2.3. Questionnaire
2.4. Weather Information
2.5. Statistics
3. Results
4. Discussion
4.1. Effect of Sex on Falls
4.2. Effect of Prior Climbing Experience on Mount Fuji on the Incidence of Falls
4.3. Effects of Other Potential Factors on Falls
4.4. Methodological Considerations
5. Conclusions
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- Bärtsch, P.; Swenson, E.R. Acute high-altitude illnesses. N. Engl. J. Med. 2013, 369, 1666–1667. [Google Scholar] [CrossRef] [PubMed]
- Gao, C.; Abeysekera, J. A systems perspective of slip and fall accidents on icy and snowy surfaces. Ergonomics 2004, 47, 573–598. [Google Scholar] [CrossRef] [PubMed]
- Yang, F.; Munoz, J.; Han, L.Z.; Yang, F. Effects of vibration training in reducing risk of slip-related falls among young adults with obesity. J. Biomech. 2017, 57, 87–93. [Google Scholar] [CrossRef] [PubMed]
- Schwameder, H.; Roithner, R.; Müller, E.; Niessen, W.; Raschner, C. Knee joint forces during downhill walking with hiking poles. J. Sports Sci. 1999, 17, 969–978. [Google Scholar] [CrossRef] [PubMed]
- McIntosh, S.E.; Brillhart, A.; Dow, J.; Grissom, C.K. Search and rescue activity on Denali, 1990 to 2008. Wilderness Environ. Med. 2010, 21, 103–108. [Google Scholar] [CrossRef]
- Faulhaber, M.; Pocecco, E.; Niedermeier, M.; Ruedl, G.; Walter, D.; Sterr, R.; Ebner, H.; Schobersberger, W.; Burtscher, M. Fall-related accidents among hikers in the Austrian Alps: A 9-year retrospective study. BMJ Open Sport Exerc. Med. 2017, 3, e000304. [Google Scholar] [CrossRef]
- Yamamoto, K.; Saito, I.; Hongo, T.; Ogasawara, A. The structuring of problems in Mt. Fuji climbing using users consciousness structure analysis. Landsc. Res. Jpn. 2004, 67, 689–692. [Google Scholar] [CrossRef]
- Horiuchi, M.; Endo, J.; Akatsuka, S.; Uno, T.; Jones, T.E. Prevalence of acute mountain sickness on Mount Fuji: A pilot study. J. Travel Med. 2016, 23. [Google Scholar] [CrossRef] [Green Version]
- Howatson, G.; Hough, P.; Pattison, J.; Hill, J.A.; Blagrove, R.; Glaister, M.; Thompson, K.G. Trekking poles reduce exercise-induced muscle injury during mountain walking. Med. Sci. Sports Exerc. 2011, 43, 140–145. [Google Scholar] [CrossRef]
- Jones, T.E.; Yamamoto, K.; Hayashi, U.; Jones, N.R. Summer climbing incidents occurring on Fujisan’s north face from 1989 to 2008. Wilderness Environ. Med. 2014, 25, 378–383. [Google Scholar] [CrossRef]
- Horiuchi, M.; Uno, T.; Endo, J.; Handa, Y.; Hasegawa, T. Impact of Sleeping Altitude on Symptoms of Acute Mountain Sickness on Mt. Fuji. High Alt. Med. Biol. 2018, 19, 193–200. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Sasaki, T.; Matsumoto, S. Actual conditions of work, fatigue and sleep in non-employed, home-based female information technology workers with preschool children. Ind. Health 2005, 43, 142–150. [Google Scholar] [CrossRef] [PubMed]
- Hashimoto, K.; Murakami, M. Reliability and validity of the reversed Mood Check List-short form 2 (MCL-S.2) measuring the positive mood state following exercise. J. Health Sci. 2011, 33, 21–26. [Google Scholar] [CrossRef]
- Roach, R.C.; Hackett, P.H.; Oelz, O.; Bärtsch, P.; Luks, A.M.; Maclnnis, M.J.; Baillie, J.K.; Lake Louise AMS Score Consensus Committee. The 2018 Lake Louise Acute Mountain Sickness Score. High Alt. Med. Biol. 2018, 19, 4–6. [Google Scholar] [CrossRef] [PubMed]
- Zuur, A.F.; Ieno, E.N.; Smith, G.M. Linear regression. In Analysing Ecological Data; Zuur, A.F., Ieno, E.N., Smith, G.M., Eds.; Springer: New York, NY, USA, 2007; pp. 49–77. [Google Scholar]
- Zuur, A.F.; Ieno, E.N.; Smith, G.M. Monitoring for change: Using generalized least squares, non-metric multidimensional scaling, and Mantel test on western Montana grasslands. In Analysing Ecological Data; Zuur, A.F., Ieno, E.N., Smith, G.M., Eds.; Springer: New York, NY, USA, 2007; pp. 463–484. [Google Scholar]
- Zuur, A.F.; Ieno, E.N.; Walker, N.J.; Saveliev, A.A.; Smith, G.M. Required pre-knowledge: A linear regression and additive modelling example. In Mixed Effects Models and Extensions in Ecology with R; New Zuur, A.F., Ieno, E.N., Walker, N.J., Saveliev, A.A., Smith, G.M., Eds.; Springer: New York, NY, USA, 2009; pp. 531–552. [Google Scholar]
- R Core Team. A Language and Environment for Statistical Computing; R Foundation for Statistical Computing: Vienna, Austria, 2015. [Google Scholar]
- Ericksen, H.; Gribble, P.A. Sex differences, hormone fluctuations, ankle stability, and dynamic postural control. J. Athl. Train. 2012, 47, 143–148. [Google Scholar] [CrossRef]
- Fredsted, A.; Clausen, T.; Overgaard, K. Effects of step exercise on muscle damage and muscle Ca2+ content in men and women. J. Strength Cond. Res. 2008, 22, 1136–1146. [Google Scholar] [CrossRef]
- Yamamoto, K. A study of attributes of climbers and anxiety and risk recognized by them at Mt. Fuji. Landsc. Res. Jpn. 2010, 73, 485–488. [Google Scholar] [CrossRef]
- Nédélec, M.; Halson, S.; Abaidia, A.E.; Ahmaidi, S.; Dupont, G. Stress, Sleep and Recovery in Elite Soccer: A Critical Review of the Literature. Sports Med. 2015, 45, 1387–1400. [Google Scholar] [CrossRef]
- Lew, F.L.; Qu, X. Effects of mental fatigue on biomechanics of slips. Ergonomics 2014, 57, 1927–1932. [Google Scholar] [CrossRef]
- Kamińska, M.S.; Brodowski, J.; Karakiewicz, B. Fall risk factors in community-dwelling elderly depending on their physical function, cognitive status and symptoms of depression. Int. J. Environ. Res. Public Health 2015, 12, 3406–3416. [Google Scholar] [CrossRef]
- Lord, S.R.; Clark, R.D.; Webster, I.W. Visual acuity and contrast sensitivity in relation to falls in an elderly population. Age Ageing 1991, 20, 175–181. [Google Scholar] [CrossRef] [PubMed]
- Lord, S.R.; Ward, J.A.; Williams, P.; Anstey, K.J. Physiological factors associated with falls in older community-dwelling women. J. Am. Geriatr. Soc. 1994, 42, 1110–1117. [Google Scholar] [CrossRef] [PubMed]
- Basnyat, B.; Subedi, D.; Sleggs, J.; Lemaster, J.; Bhasyal, G.; Aryal, B.; Subedi, N. Disoriented and ataxic pilgrims: An epidemiological study of acute mountain sickness and high-altitude cerebral edema at a sacred lake at 4300 m in the Nepal Himalayas. Wilderness Environ. Med. 2000, 11, 89–93. [Google Scholar] [CrossRef]
- Mairer, K.; Wille, M.; Burtscher, M. The prevalence of and risk factors for acute mountain sickness in the Eastern and Western Alps. High Alt. Med. Biol. 2010, 11, 343–348. [Google Scholar] [CrossRef] [PubMed]
- Hackett, P.H.; Rennie, D.; Levine, H.D. The incidence, importance, and prophylaxis of acute mountain sickness. Lancet 1976, 2, 1149–1155. [Google Scholar] [CrossRef]
- Maggiorini, M.; Bühler, B.; Walter, M.; Oelz, O. Prevalence of acute mountain sickness in the Swiss Alps. BMJ 1990, 301, 853–855. [Google Scholar] [CrossRef] [PubMed]
- Vardy, J.; Vardy, J.; Judge, K. Can knowledge protect against acute mountain sickness? J. Public Health 2005, 27, 366–370. [Google Scholar] [CrossRef]
- Vardy, J.; Vardy, J.; Judge, K. Acute mountain sickness and ascent rates in trekkers above 2500 m in the Nepali Himalaya. Aviat. Space Environ. Med. 2006, 77, 742–744. [Google Scholar]
- Mairer, K.; Wille, M.; Bucher, T.; Burtscher, M. Prevalence of acute mountain sickness in the Eastern Alps. High Alt. Med. Biol. 2009, 10, 239–245. [Google Scholar] [CrossRef]
- Podsakoff, P.M.; MacKenzie, S.B.; Lee, J.Y.; Podsakoff, N.P. Common method biases in behavioral research: A critical review of the literature and recommended remedies. J. Appl. Psychol. 2003, 88, 879–903. [Google Scholar] [CrossRef]
- Koepp, G.A.; Snedden, B.J.; Levine, J.A. Workplace slip, trip and fall injuries and obesity. Ergonomics 2015, 58, 674–679. [Google Scholar] [CrossRef] [PubMed]
- Larsson, A.; Berggård, G.; Rosander, P.; Gard, G. Gait Speed with Anti-Slip Devices on Icy Pedestrian Crossings Relate to Perceived Fall-Risk and Balance. Int. J. Environ. Res. Public Health 2019, 16, 2451. [Google Scholar] [CrossRef] [PubMed]
- Cikajlo, I.; Matjacic, Z. The influence of boot stiffness on gait kinematics and kinetics during stance phase. Ergonomics 2007, 50, 2171–2182. [Google Scholar] [CrossRef] [PubMed]
- Lockhart, T.E.; Smith, J.L.; Woldstad, J.C. Effects of aging on the biomechanics of slips and falls. Hum. Factors 2005, 47, 708–729. [Google Scholar] [CrossRef]
- Liu, J.; Lockhart, T.; Kim, S. Reaction moment at the L5/S1 joint during simulated forward slipping with a handheld load. Int. J. Occup. Saf. Ergon. 2014, 20, 429–436. [Google Scholar] [CrossRef]
- She, S.; Tian, Y.; Lu, L.; Eimontaite, I.; Xie, T.; Sun, Y. An Exploration of Hiking Risk Perception: Dimensions and Antecedent Factors. Int. J. Environ. Res. Public Health 2019, 16, 1986. [Google Scholar] [CrossRef]


{kind=link}
| Please respond to the following questions with respect to falls and their situations | |||||||
| Did you fall in this mountain climbing? | 1. Yes (ground contact with any portions of the body) 2. No | ||||||
| First fall situation | Slope | a. Ascent | b. Descent | c. Unknown | d. Other | ||
| Cause | 1. Stagger | 2. Stumble | 3. Slip | 4. Caught pole | 5. Other | ||
| Injury | 1. None | 2. Knee pain | 3. Ankle sprain | 4. Scratch | 5. Other | ||
| Second fall situation | Slope | a. Ascent | b. Descent | c. Unknown | d. Other | ||
| Cause | 1. Stagger | 2. Stumble | 3. Slip | 4. Caught pole | 5. Other | ||
| Injury | 1. None | 2. Knee pain | 3. Ankle sprain | 4. Scratch | 5. Other | ||
| Situation of three or more falls | Times | ______ times | |||||
| Slope and times | a. Ascent ______ times | b. Descent ______ times | |||||
| Cause | 1. Stagger | 2. Stumble | 3. Slip | 4. Caught pole | 5. Other | ||
| Injury | 1. None | 2. Knee pain | 3. Ankle sprain | 4. Scratch | 5. Other | ||
| Please respond to following questions (parameters of #1 to #7 in the main text). | |||||||
| Age | ______ years old | ||||||
| Sex | 1. Male | 2. Female | |||||
| Prior climbing experience on Mount Fuji | 1. First time | 2. More than once | |||||
| Climbing experience on other mountains | 1. Less than two years | 2. More than two years | |||||
| Staying | 1. Overnight stay lodgers | 2. Single day climbers | |||||
| Guide | 1. With tour guide | 2. Without tour guide | |||||
| Summit success | 1. Reached | 2. Failed | |||||
| Please tell me about your symptoms of acute mountain sickness a recalling the worst condition. Please mark only one appropriate answer with a circle (parameters #8 in the main text). | |||||||
| Headache | 0. No headache | 1. Mild headache | |||||
| 2. Moderate headache | 3. Severe incapacitating headache | ||||||
| Gastrointestinal symptoms | 0. No gastrointestinal symptoms | 1. Poor appetite or nausea | |||||
| 2. Moderate nausea or vomiting | 3. Severe incapacitating nausea or vomiting | ||||||
| Fatigue and/or weakness | 0. No tired or weakness | 1. Mild fatigue/weakness | |||||
| 2.Moderate fatigue/weakness | 3. Severe incapacitating fatigue/weakness | ||||||
| Dizziness/lightheadedness | 0. No dizzy | 1. Mild dizziness | |||||
| 2. Moderate dizziness | 3. Severe incapacitating dizziness | ||||||
| Please indicate how fatigued you feel with a mark ( / ) on the line below (parameters #9 and #10 in the main text; visual analogue scale). | |||||||
| Whole body |  | ||||||
| Lower body |  | ||||||
| Please tell me about your current feelings. Please mark only one appropriate answer with a circle (parameter #11 in the main text). | |||||||
| Extremely unlikely | Moderately unlikely | Slightly unlikely | Neither | Slightly likely | Moderately likely | Extremely likely | |
| 1 I am lively | 1 | 2 | 3 | 4 | 5 | 6 | 7 |
| 2 I am relaxed | 1 | 2 | 3 | 4 | 5 | 6 | 7 |
| 3 I feel anxious | 1 | 2 | 3 | 4 | 5 | 6 | 7 |
| 4 I feel brisk | 1 | 2 | 3 | 4 | 5 | 6 | 7 |
| 5 I am comfortable | 1 | 2 | 3 | 4 | 5 | 6 | 7 |
| 6 I am bothered | 1 | 2 | 3 | 4 | 5 | 6 | 7 |
| 7 I am perky | 1 | 2 | 3 | 4 | 5 | 6 | 7 |
| 8 I feel calm | 1 | 2 | 3 | 4 | 5 | 6 | 7 |
| 9 I am regretful | 1 | 2 | 3 | 4 | 5 | 6 | 7 |
| 10 I feel refreshed | 1 | 2 | 3 | 4 | 5 | 6 | 7 |
| 11 I feel rested | 1 | 2 | 3 | 4 | 5 | 6 | 7 |
| 12 I am worried | 1 | 2 | 3 | 4 | 5 | 6 | 7 |
| Please tell me about your current conditions. Please mark only one appropriate answer with a circle (parameter #12 in the main text). | |||||||
| Disagree completely | Agree scarcely | Agree slightly | Agree considerably | Agree strongly | |||
| 1 I feel heavy in the head | 1 | 2 | 3 | 4 | 5 | ||
| 2 I feel nervous | 1 | 2 | 3 | 4 | 5 | ||
| 3 I feel my eyes are dry | 1 | 2 | 3 | 4 | 5 | ||
| 4 I feel ill | 1 | 2 | 3 | 4 | 5 | ||
| 5 I feel restless | 1 | 2 | 3 | 4 | 5 | ||
| 6 I feel a headache | 1 | 2 | 3 | 4 | 5 | ||
| 7 I feel a pain in the eyes | 1 | 2 | 3 | 4 | 5 | ||
| 8 I feel stiff in the neck and shoulders | 1 | 2 | 3 | 4 | 5 | ||
| 9 I feel the brain hot or muddled | 1 | 2 | 3 | 4 | 5 | ||
| 10 I feel like yawning | 1 | 2 | 3 | 4 | 5 | ||
| 11 I feel a pain in the hands or fingers | 1 | 2 | 3 | 4 | 5 | ||
| 12 I feel dizzy | 1 | 2 | 3 | 4 | 5 | ||
| 13 I feel drowsy | 1 | 2 | 3 | 4 | 5 | ||
| 14 I feel a lack of desire to do something | 1 | 2 | 3 | 4 | 5 | ||
| 15 I feel anxious | 1 | 2 | 3 | 4 | 5 | ||
| 16 I feel my eyes are blurry | 1 | 2 | 3 | 4 | 5 | ||
| 17 I feel tired in the whole body | 1 | 2 | 3 | 4 | 5 | ||
| 18 I feel depressed | 1 | 2 | 3 | 4 | 5 | ||
| 19 I feel dullness in the arms | 1 | 2 | 3 | 4 | 5 | ||
| 20 I feel difficulty in thinking | 1 | 2 | 3 | 4 | 5 | ||
| 21 I feel a desire to lie down | 1 | 2 | 3 | 4 | 5 | ||
| 22 I feel eyestrain | 1 | 2 | 3 | 4 | 5 | ||
| 23 I feel a lower back pain | 1 | 2 | 3 | 4 | 5 | ||
| 24 I feel my eyes are blinking | 1 | 2 | 3 | 4 | 5 | ||
| 25 I feel tired in the legs | 1 | 2 | 3 | 4 | 5 | ||
| Independent Variables | No Fall | Fall |
|---|---|---|
| Age | 37 ± 14 | 36 ± 15 |
| Sex | ||
| Male | 260 (75%) | 85 (25%) |
| Female | 129 (61%) | 82 (39%) |
| Climbing experience on Mount Fuji | ||
| More than once | 142 (77%) | 42 (23%) |
| First | 247 (66%) | 125 (34%) |
| Climbing experience on other mountains | ||
| More than two years | 163 (74%) | 57 (26%) |
| Less than two years | 226 (67%) | 110 (33%) |
| Stay | ||
| Single day climbers | 36 (62%) | 22 (38%) |
| Overnight stay lodgers | 353 (71%) | 145 (29%) |
| Tour guide | ||
| Without tour guide | 249 (71%) | 102 (29%) |
| With tour guide | 140 (68%) | 65 (32%) |
| Summit success | ||
| Failed | 64 (72%) | 25 (28%) |
| Reached | 325 (70%) | 142 (30%) |
| AMS | ||
| No AMS | 298 (71%) | 119 (29%) |
| AMS | 91 (65%) | 48 (35%) |
| Fatigue measured by a visual analogue scale | ||
| Whole body | 67 ± 26 | 71 ± 26 |
| Lower body | 63 ± 27 | 66 ± 26 |
| Mood change following acute physical activities (−3–3) | ||
| Pleasant emotions | 1.0 ± 1.4 | 0.8 ± 1.4 |
| Anxiety | −2.0 ± 1.1 | −1.9 ± 1.1 |
| Relaxed | 1.0 ± 1.3 | 0.7 ± 1.3 |
| Subjective feelings (1–5) | ||
| Sleepiness | 2.7 ± 1.0 | 2.7 ± 1.0 |
| Emotional stability | 1.4 ± 0.6 | 1.4 ± 0.5 |
| Uneasiness | 1.7 ± 0.7 | 1.7 ± 0.7 |
| Dullness | 2.4 ± 0.9 | 2.6 ± 0.9 |
| Eyestrain | 1.8 ± 0.9 | 1.9 ± 0.9 |
| Independent Variables | Partial Regression Coefficient | 95% CI | p Values | |
|---|---|---|---|---|
| Lower | Upper | |||
| Sex | ||||
| Female | 0.528 | 0.134 | 0.922 | 0.009 |
| Climbing experience on Mount Fuji | ||||
| First | 0.548 | 0.122 | 0.974 | 0.012 |
| Staying | ||||
| Overnight stay lodgers | −0.615 | −1.215 | −0.014 | 0.045 |
| Subjective feeling of relaxation | −0.212 | −0.373 | −0.052 | 0.010 |
| Sleepiness | −0.303 | −0.586 | −0.021 | 0.035 |
| Emotional stability | −0.462 | −0.883 | −0.041 | 0.032 |
| Dullness | 0.240 | −0.057 | 0.536 | 0.113 |
| Eyestrain | 0.313 | 0.039 | 0.586 | 0.025 |
© 2019 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Uno, T.; Fujino, M.; Ohwaki, A.; Horiuchi, M. Prevalence of Falls on Mount Fuji and Associated with Risk Factors: A Questionnaire Survey Study. Int. J. Environ. Res. Public Health 2019, 16, 4234. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph16214234
Uno T, Fujino M, Ohwaki A, Horiuchi M. Prevalence of Falls on Mount Fuji and Associated with Risk Factors: A Questionnaire Survey Study. International Journal of Environmental Research and Public Health. 2019; 16(21):4234. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph16214234
Chicago/Turabian StyleUno, Tadashi, Masaya Fujino, Atsushi Ohwaki, and Masahiro Horiuchi. 2019. "Prevalence of Falls on Mount Fuji and Associated with Risk Factors: A Questionnaire Survey Study" International Journal of Environmental Research and Public Health 16, no. 21: 4234. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph16214234