Knowledge towards Cervical and Breast Cancers among Industrial Workers: Results from a Multisite Study in Northern Vietnam

 , , , and
, , , and 
Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Design
2.2. Measure and Instruments
2.2.1. Socioeconomic Characteristics
2.2.2. Knowledge of Breast Cancer and Cervical Cancer
2.2.3. Health Risk Behaviors
2.2.4. Health Seeking Behaviors
2.3. Statistical Analysis
2.4. Ethics Approval
3. Results
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
Appendix A

References
- World Health Organization. Breast Cancer; WHO: Geneva, Switzerland, 2018. [Google Scholar]
- Global Burden of Disease Cancer Collaboration; Fitzmaurice, C.; Dicker, D.; Pain, A.; Hamavid, H.; Moradi-Lakeh, M.; MacIntyre, M.F.; Allen, C.; Hansen, G.; Woodbrook, R.; et al. The Global Burden of Cancer 2013. JAMA Oncol. 2015, 1, 505–527. [Google Scholar] [CrossRef] [PubMed]
- Wadler, B.M.; Judge, C.M.; Prout, M.; Allen, J.D.; Geller, A.C. Improving Breast Cancer Control via the Use of Community Health Workers in South Africa: A Critical Review. J. Oncol. 2011, 2011. [Google Scholar] [CrossRef] [PubMed]
- Coleman, M.P.; Quaresma, M.; Berrino, F.; Lutz, J.M.; De Angelis, R.; Capocaccia, R.; Baili, P.; Rachet, B.; Gatta, G.; Hakulinen, T.; et al. Cancer survival in five continents: A worldwide population-based study (CONCORD). Lancet Oncol. 2008, 9, 730–756. [Google Scholar] [CrossRef]
- Bray, F.; Ferlay, J.; Soerjomataram, I.; Siegel, R.L.; Torre, L.A.; Jemal, A. Global cancer statistics 2018: GLOBOCAN estimates of incidence and mortality worldwide for 36 cancers in 185 countries. CA Cancer J. Clin. 2018, 68, 394–424. [Google Scholar] [CrossRef] [Green Version]
- World Health Organization. Cervical Cancer; WHO: Geneva, Switzerland, 2018. [Google Scholar]
- Jenkins, C.; Minh, L.N.; Anh, T.T.; Ngan, T.T.; Tuan, N.T.; Giang, K.B.; Hoat, L.N.; Lohfeld, L.; Donnelly, M.; Van Minh, H.; et al. Breast cancer services in Vietnam: A scoping review. Glob. Health Action 2018, 11, 1435344. [Google Scholar] [CrossRef]
- Global Health Data Exchange. Global Burden of Diseases; Institute for Health Metrics and Evaluation: Seattle, WA, USA, 2017. [Google Scholar]
- Ferlay, J.; Soerjomataram, I.; Dikshit, R.; Eser, S.; Mathers, C.; Rebelo, M.; Parkin, D.M.; Forman, D.; Bray, F. Cancer incidence and mortality worldwide: Sources, methods and major patterns in GLOBOCAN 2012. Int. J. Cancer 2015, 136, E359–E386. [Google Scholar] [CrossRef]
- Thi Nguyen, D.N.; Simms, K.; Vu Nguyen, H.Q.; Van Tran, T.; Nguyen, N.H.; LaMontagne, D.S.; Castle, P.; Canfell, K. The burden of cervical cancer in Vietnam: Synthesis of the evidence. Cancer Epidemiol. 2019, 59, 83–103. [Google Scholar] [CrossRef]
- Jia, Y.; Li, S.; Yang, R.; Zhou, H.; Xiang, Q.; Hu, T.; Zhang, Q.; Chen, Z.; Ma, D.; Feng, L. Knowledge about cervical cancer and barriers of screening program among women in Wufeng County, a high-incidence region of cervical cancer in China. PLoS ONE 2013, 8, e67005. [Google Scholar] [CrossRef]
- Shrestha, S.; Dhakal, P. Knowledge, Attitude and Practice Regarding Cervical Cancer Screening Among Women Attending a Teaching Hospital, Bharatpur, Chitwan. J. Fam. Reprod. Health 2017, 11, 18–23. [Google Scholar]
- Liu, L.Y.; Wang, Y.J.; Wang, F.; Yu, L.X.; Xiang, Y.J.; Zhou, F.; Li, L.; Zhang, Q.; Fu, Q.Y.; Ma, Z.B.; et al. Factors associated with insufficient awareness of breast cancer among women in Northern and Eastern China: A case-control study. BMJ Open 2018, 8, e018523. [Google Scholar] [CrossRef]
- Thapa, N.; Maharjan, M.; Petrini, M.A.; Shah, R.; Shah, S.; Maharjan, N.; Shrestha, N.; Cai, H. Knowledge, attitude, practice and barriers of cervical cancer screening among women living in mid-western rural, Nepal. J. Gynecol. Oncol. 2018, 29, e57. [Google Scholar] [CrossRef] [PubMed]
- The World Bank. The World Bank in Vietnam; The World Bank: Washington, DC, USA, 2018. [Google Scholar]
- International Labour Organization. Viet Nam: Serving Markets and Workers; International Labour Organization: Geneva, Switzerland, 2018. [Google Scholar]
- Chee, H.L.; Rashidah, S.; Shamsuddin, K.; Zainiyah, S.Y. Knowledge and practice of breast self examination and Pap smear screening among a group of electronics women workers. Med. J. Malays. 2003, 58, 320–329. [Google Scholar]
- Sung, T.I.; Chen, P.C.; Jyuhn-Hsiarn Lee, L.; Lin, Y.P.; Hsieh, G.Y.; Wang, J.D. Increased standardized incidence ratio of breast cancer in female electronics workers. BMC Public Health 2007, 7, 102. [Google Scholar] [CrossRef] [PubMed]
- Savitz, D.A.; Andrews, K.W.; Brinton, L.A. Occupation and cervical cancer. J. Occup. Environ. Med. 1995, 37, 357–361. [Google Scholar] [CrossRef] [PubMed]
- Alterman, T.; Burnett, C.; Peipins, L.; Lalich, N.; Halperin, W. Occupation and cervical cancer: An opportunity for prevention. J. Womens Health 1997, 6, 649–657. [Google Scholar] [CrossRef] [PubMed]
- Bradley, K.A.; DeBenedetti, A.F.; Volk, R.J.; Williams, E.C.; Frank, D.; Kivlahan, D.R. AUDIT-C as a brief screen for alcohol misuse in primary care. Alcohol. Clin. Exp. Res. 2007, 31, 1208–1217. [Google Scholar] [CrossRef] [PubMed]
- Ryan, P. Integrated theory of health behavior change: Background and intervention development. Clin. Nurse Spec. 2009, 23, 161–172. [Google Scholar] [CrossRef] [PubMed]
- Lorig, K.; Ritter, P.L.; Plant, K. A disease-specific self-help program compared with a generalized chronic disease self-help program for arthritis patients. Arthritis Care Research. 2005, 53, 950–957. [Google Scholar] [CrossRef]
- Gage, H.; Hampson, S.; Skinner, T.C.; Hart, J.; Storey, L.; Foxcroft, D.; Kimber, A.; Cradock, S.; McEvilly, E.A. Educational and psychosocial programmes for adolescents with diabetes: Approaches, outcomes and cost-effectiveness. Patient Educ. Couns. 2004, 53, 333–346. [Google Scholar] [CrossRef]
- Parsa, P.; Kandiah, M.; Mohd Zulkefli, N.A.; Rahman, H.A. Knowledge and behavior regarding breast cancer screening among female teachers in Selangor, Malaysia. Asian Pac. J. Cancer Prev. 2008, 9, 221–227. [Google Scholar]
- Ames, B.N.; Gold, L.S. The causes and prevention of cancer: The role of environment. Biotherapy 1998, 11, 205–220. [Google Scholar] [CrossRef] [PubMed]
- Brody, J.G.; Rudel, R.A. Environmental pollutants and breast cancer. Environ. Health Perspect. 2003, 111, 1007–1019. [Google Scholar] [CrossRef] [PubMed]
- Gupta, A.; Shridhar, K.; Dhillon, P.K. A review of breast cancer awareness among women in India: Cancer literate or awareness deficit? Eur. J. Cancer 2015, 51, 2058–2066. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Forbes, L.J.; Atkins, L.; Thurnham, A.; Layburn, J.; Haste, F.; Ramirez, A.J. Breast cancer awareness and barriers to symptomatic presentation among women from different ethnic groups in East London. Br. J. Cancer 2011, 105, 1474–1479. [Google Scholar] [CrossRef] [PubMed]
- Aydogan, U.; Doganer, Y.C.; Kilbas, Z.; Rohrer, J.E.; Sari, O.; Usterme, N.; Yuksel, S.; Akbulut, H.; Balkan, S.M.; Saglam, K.; et al. Predictors of knowledge level and awareness towards breast cancer among Turkish females. Asian Pac. J. Cancer Prev. 2015, 16, 275–282. [Google Scholar] [CrossRef] [PubMed]
- Kobeissi, L.; Samari, G.; Telesca, D.; Esfandiari, M.; Galal, O. The impact of breast cancer knowledge and attitudes on screening and early detection among an immigrant Iranian population in southern California. J. Relig. Health 2014, 53, 1759–1769. [Google Scholar] [CrossRef]
- Jenkins, C.; Ngan, T.T.; Ngoc, N.B.; Phuong, T.B.; Lohfeld, L.; Donnelly, M.; Van Minh, H.; Murray, L. Strengthening breast cancer services in Vietnam: A mixed-methods study. Glob. Health Res. Policy 2019, 4, 2. [Google Scholar] [CrossRef]
- Bruce, J.G.; Tucholka, J.L.; Steffens, N.M.; Neuman, H.B. Quality of online information to support patient decision-making in breast cancer surgery. J. Surg. Oncol. 2015, 112, 575–580. [Google Scholar] [CrossRef] [Green Version]
- Trieu, P.D.; Mello-Thoms, C.; Brennan, P.C. Female breast cancer in Vietnam: A comparison across Asian specific regions. Cancer Biol. Med. 2015, 12, 238–245. [Google Scholar] [CrossRef]
- Demment, M.M.; Peters, K.; Dykens, J.A.; Dozier, A.; Nawaz, H.; McIntosh, S.; Smith, J.S.; Sy, A.; Irwin, T.; Fogg, T.T.; et al. Developing the Evidence Base to Inform Best Practice: A Scoping Study of Breast and Cervical Cancer Reviews in Low- and Middle-Income Countries. PLoS ONE 2015, 10, e0134618. [Google Scholar] [CrossRef]
- Jenkins, C.N.; McPhee, S.J.; Bird, J.A.; Pham, G.Q.; Nguyen, B.H.; Nguyen, T.; Lai, K.Q.; Wong, C.; Davis, T.B. Effect of a media-led education campaign on breast and cervical cancer screening among Vietnamese-American women. Prev. Med. 1999, 28, 395–406. [Google Scholar] [CrossRef] [PubMed]
- Im, E.O.; Park, Y.S.; Lee, E.O.; Yun, S.N. Korean women’s attitudes toward breast cancer screening tests. Int. J. Nurs. Stud. 2004, 41, 583–589. [Google Scholar] [CrossRef] [PubMed]
- Sambanje, M.N.; Mafuvadze, B. Breast cancer knowledge and awareness among university students in Angola. Pan Afr. Med. J. 2012, 11, 70. [Google Scholar] [PubMed]
- Aweke, Y.H.; Ayanto, S.Y.; Ersado, T.L. Knowledge, attitude and practice for cervical cancer prevention and control among women of childbearing age in Hossana Town, Hadiya zone, Southern Ethiopia: Community-based cross-sectional study. PLoS ONE 2017, 12, e0181415. [Google Scholar] [CrossRef] [PubMed]
- Mitiku, I.; Tefera, F. Knowledge about Cervical Cancer and Associated Factors among 15–49 Year Old Women in Dessie Town, Northeast Ethiopia. PLoS ONE 2016, 11, e0163136. [Google Scholar] [CrossRef] [PubMed]
- Ali-Risasi, C.; Mulumba, P.; Verdonck, K.; Vanden Broeck, D.; Praet, M. Knowledge, attitude and practice about cancer of the uterine cervix among women living in Kinshasa, the Democratic Republic of Congo. BMC Womens Health 2014, 14, 30. [Google Scholar] [CrossRef]
- Touch, S.; Oh, J.K. Knowledge, attitudes, and practices toward cervical cancer prevention among women in Kampong Speu Province, Cambodia. BMC Cancer 2018, 18, 294. [Google Scholar] [CrossRef]
- Taylor, V.M.; Nguyen, T.T.; Jackson, J.C.; McPhee, S.J. Cervical cancer control research in Vietnamese American communities. Cancer Epidemiol. Biomark. Prev. 2008, 17, 2924–2930. [Google Scholar] [CrossRef]
- Paul, P.; LaMontagne, D.S.; Le, N.T. Knowledge of cervical cancer and HPV vaccine post- vaccination among mothers and daughters in Vietnam. Asian Pac. J. Cancer Prev. 2012, 13, 2587–2592. [Google Scholar] [CrossRef]
- Yi, J.K.; Lackey, S.C.; Zahn, M.P.; Castaneda, J.; Hwang, J.P. Human papillomavirus knowledge and awareness among Vietnamese mothers. J. Community Health 2013, 38, 1003–1009. [Google Scholar] [CrossRef]
- Darabi, F.; Yaseri, M.; Kaveh, M.H.; Khalajabadi Farahani, F.; Majlessi, F.; Shojaeizadeh, D. The effect of a theory of planned behavior-based educational intervention on sexual and reproductive health in iranian adolescent girls: A randomized controlled trial. J. Res. Health Sci. 2017, 17, e00400. [Google Scholar] [PubMed]

{kind=link}
| Characteristics | n | % |
|---|---|---|
| Gender | ||
| Male | 48 | 16.7 |
| Female | 239 | 83.3 |
| Education | ||
| Under High School | 25 | 8.7 |
| High School | 176 | 61.3 |
| Above High School | 86 | 30.0 |
| Marital Status | ||
| Single | 12 | 4.2 |
| Living with Spouse/Partner | 277 | 95.9 |
| Number of children | ||
| 0 | 12 | 4.4 |
| 1 | 44 | 16.0 |
| 2 | 177 | 64.1 |
| >2 | 43 | 15.6 |
| Nonimmigrant/Migrant | 137 | 48.9 |
| Mean SD | ||
| Age (Years) | 31.9 | 4.5 |
| Monthly Income (USD) | 273.6 | 96.5 |
| Years of Experience | 9.9 | 3.8 |
| Working Hours Per Day | 8.2 | 0.9 |
| Characteristics | Male | Female | Total | p-Value | |||
|---|---|---|---|---|---|---|---|
| n | % | n | % | n | % | ||
| Number of Sexual Partners within Last 12 Months | |||||||
| 0 | 5 | 11.6 | 33 | 17.7 | 38 | 16.6 | 0.57 † |
| 1 | 31 | 72.1 | 120 | 64.5 | 151 | 65.9 | |
| Did not remember | 7 | 16.3 | 33 | 17.7 | 40 | 17.5 | |
| Current Smoking Status | |||||||
| Never Smokers | 20 | 42.6 | 204 | 95.8 | 224 | 86.2 | <0.01 * |
| Former Smokers | 8 | 17.0 | 9 | 4.2 | 17 | 6.5 | |
| Current Smokers | 19 | 40.4 | 0 | 0.0 | 19 | 7.3 | |
| Current Drinking Status | |||||||
| Hazardous Drinking | 35 | 76.1 | 3 | 1.3 | 38 | 13.7 | <0.01 * |
| Binge Drinking | 34 | 73.9 | 3 | 1.3 | 37 | 13.4 | <0.01 * |
| Other Medical Characteristics | |||||||
| Having Acute or Chronic Conditions | 45 | 95.7 | 187 | 82.4 | 232 | 84.7 | 0.02 * |
| Having Medical Checkup in the Last 12 Months | 41 | 93.2 | 215 | 94.3 | 256 | 94.1 | 0.77 * |
| Using Reproductive Healthcare and Premarital Services in the Last 12 Months | 14 | 31.1 | 111 | 48.9 | 125 | 46.0 | 0.03 * |
| Health Information Sources | |||||||
| Friends/Relatives | 18 | 40.0 | 104 | 44.3 | 122 | 43.6 | 0.6 * |
| Poster/Banner | 6 | 13.3 | 15 | 6.4 | 21 | 7.5 | 0.11 * |
| Internet | 25 | 55.6 | 113 | 48.1 | 138 | 49.3 | 0.36 * |
| Mobile phone messages | 9 | 20.0 | 17 | 7.2 | 26 | 9.3 | <0.01 * |
| Radio, TV | 20 | 44.4 | 82 | 34.9 | 102 | 36.4 | 0.22 * |
| Speakers | 9 | 20.0 | 29 | 12.3 | 38 | 13.6 | 0.17 * |
| Magazines, newspaper | 19 | 42.2 | 87 | 37.0 | 106 | 37.9 | 0.5 * |
| Medical staffs | 26 | 57.8 | 114 | 48.5 | 140 | 50.0 | 0.26 * |
| Social media | 25 | 55.6 | 109 | 46.4 | 134 | 47.9 | 0.26 * |
| Other | 1 | 2.2 | 1 | 0.4 | 2 | 0.7 | 0.19 * |
| Characteristics | n | % |
|---|---|---|
| Causes of Breast Cancer | ||
| No Breastfeeding | 90 | 32.3 |
| Genetic | 70 | 25.1 |
| Pollution and Chemicals | 110 | 39.4 |
| Smoking | 81 | 29.0 |
| Mammary Gland Engorgement | 91 | 32.6 |
| Signs of Breast Cancer | ||
| Feeling Lumps in the Breast | 213 | 76.3 |
| Breast Enlarging or Breast Shape Changing | 128 | 45.9 |
| Swollen Lymph Nodes in Armpit | 103 | 36.9 |
| One of the Nipples is Dimpled or Rough | 70 | 25.1 |
| Breast Skin Thick, Wrinkled | 54 | 19.4 |
| Breast Skin Changing Color or Grainy Like Orange Peel | 53 | 19.0 |
| Pus Spills from the Nipple | 98 | 35.1 |
| Prevention Measures for Breast Cancer | ||
| Early Diagnosis of Breast Cancer | 226 | 81.3 |
| Breastfeeding | 125 | 45.0 |
| Healthy Diet | 114 | 41.0 |
| Exercise Regularly | 127 | 45.7 |
| No Drinking Alcohol | 88 | 31.7 |
| No Smoking | 99 | 35.6 |
| Mean | SD | |
| Total Score (Score Ranged from 0 to 18) | 6.9 | 5.1 |
| Characteristics | n | % |
|---|---|---|
| Sexually Transmitted Diseases Believed to Cause Cervical Cancer | ||
| Gonorrhea | 120 | 44.0 |
| Syphilis | 122 | 44.7 |
| Warts | 114 | 41.8 |
| Chlamydia infection | 114 | 41.8 |
| Assessed Factors as the Cause of Cervical Cancer | ||
| Genital Infections | 217 | 77.5 |
| Having A Lot of Sexual Partners | 140 | 50.0 |
| Early Sexual Initiation | 68 | 24.3 |
| Too Many Children | 36 | 12.9 |
| Smoking | 41 | 14.6 |
| Assessed Symptoms as Signs of Cervical Cancer | ||
| Vaginal Bleeding after Sex | 152 | 54.5 |
| Abnormal Bleeding between Menstrual Cycles | 102 | 36.6 |
| Vaginal Discharge | 120 | 43.0 |
| Pain when Having Sex | 114 | 40.9 |
| Pelvic Pain | 72 | 25.8 |
| Heavy Bleeding during Menstruation | 47 | 16.9 |
| Measures Believed to Prevent Cervical Cancer | ||
| Periodic Gynecological Examination, Gynecological Treatment | 218 | 77.6 |
| Vaccination | 131 | 46.6 |
| Not Having A Lot of Sexual Partners | 131 | 46.6 |
| Not Early Sexual Initiation | 83 | 29.5 |
| Cervical Cancer Cannot Be Prevented | 4 | 1.4 |
| Mean | SD | |
| Total Score (Score Ranged from 0 to 19) | 7.9 | 5.0 |
| Characteristics | Knowledge of Breast Cancer | Knowledge of Cervical Cancer | ||
|---|---|---|---|---|
| Coefficient | 95% CI | Coefficient | 95% CI | |
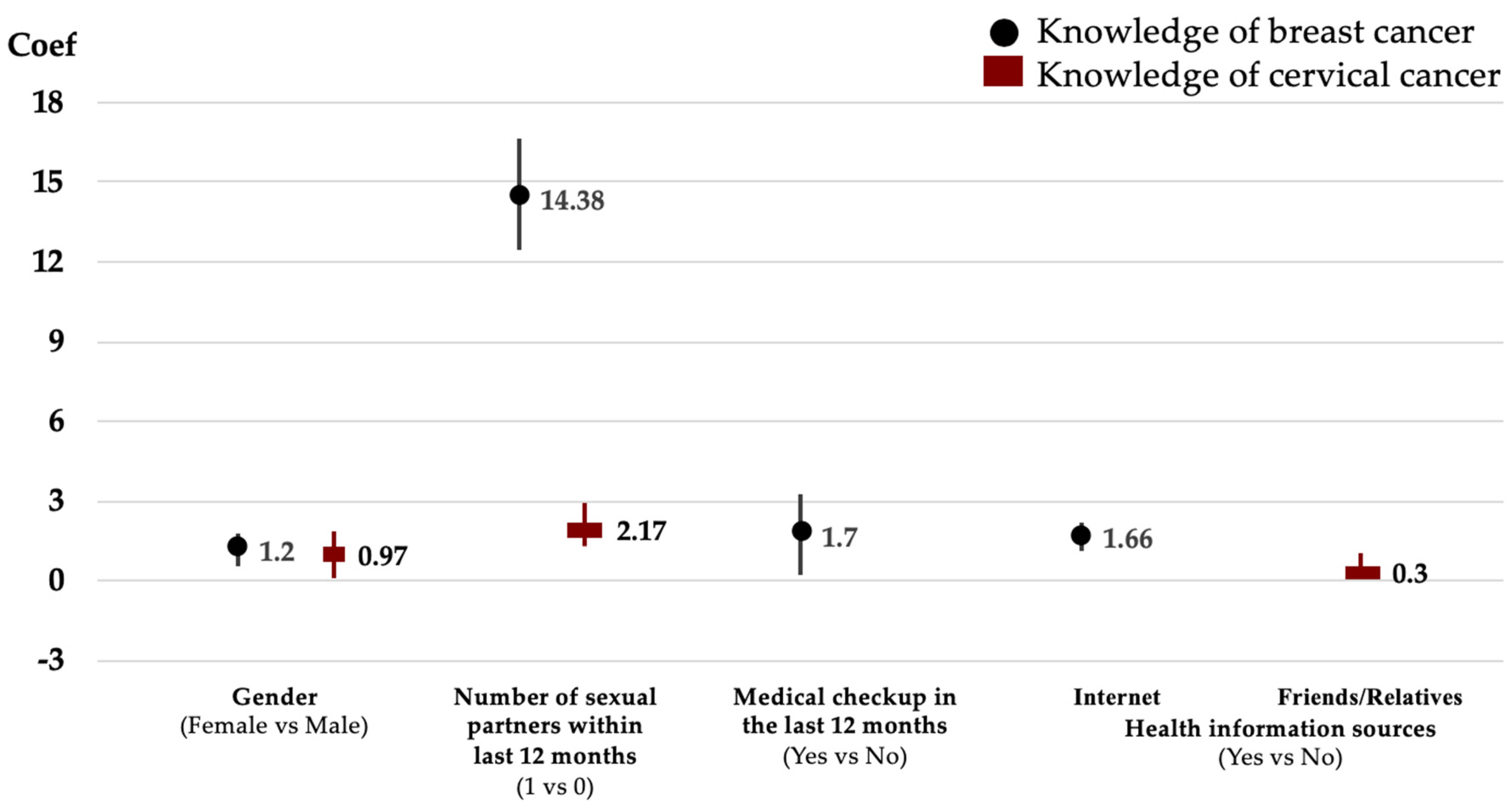
| Gender (Female vs. Male) | 1.20 ** | 0.73; 1.67 | 0.97 *** | 0.57; 1.37 |
| Education (vs. Under High School) | ||||
| High School | −0.26 | −0.68; 0.15 | −0.16 | −0.60; 0.27 |
| Above High School | −0.22 | −0.65; 0.21 | −0.04 | −0.47; 0.40 |
| Marital Status (vs. Single) | ||||
| Living with Spouse/Partner | −1.13 | −0.64; 0.42 | −0.14 | −1.54; 0.29 |
| Immigrant (No vs. Yes) | −0.19 | −0.44; 0.06 | −0.12 | −0.33; 0.09 |
| Age | 0.05 | −0.03; 0.04 | −0.03* | −0.06; 0.00 |
| Years of Experience | 0.02 | −0.01; 0.05 | 0.03** | 0.00; 0.06 |
| Number of Sexual Partners within Last 12 Months (1 vs. 0) | 14.38 *** | 12.42; 16.34 | 2.17 *** | 1.71; 2.55 |
| Current Smoking Status (vs. Never Smokers) | ||||
| Former Smokers | 0.56 *** | 0.13; 0.98 | 0.45 * | −0.00; 0.93 |
| Current Smokers | 0.53 * | −0.29; 1.36 | 0.33 | −0.17; 1.22 |
| Medical Checkup in the Last 12 Months (Yes vs. No) | 1.70 ** | 0.20; 3.24 | 0.05 | −0.76; 0.85 |
| Using Reproductive Healthcare and Premarital Services in the Last 12 Months (Yes vs. No) | 0.07 | −0.16; 0.30 | 0.02 | −0.18; 0.24 |
| Health Information Sources (Yes vs. No) | ||||
| Friends/Relatives | 0.07 | −0.19; 0.33 | 0.30 ** | 0.06; 0.55 |
| Posters/Banners | 0.36 * | −0.04; 0.70 | 0.10 | −0.30; 0.45 |
| Internet | 1.66 *** | 1.09; 2.22 | 0.12 | −0.03; 0.30 |
| Mobile Phone Messages | −0.25 | −2.59; 0.43 | −0.10 | −0.60; 0.47 |
| Radio, TV | −0.32 * | −0.64; 0.00 | −0.15 | −0.43; 0.12 |
| Speaker | 0.39 ** | 0.02; 0.74 | 0.10 | −0.30; 0.63 |
| Magazines, Newspaper | 0.33 ** | 0.01; 0.63 | 0.17 | −0.13; 0.33 |
| Medical Staffs | 0.70 | −1.23; 2.74 | 0.08 | −0.11; 0.33 |
| Social Media | 0.85 | −0.25; 1.98 | −0.02 | −0.18; 0.12 |
© 2019 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Tran, B.X.; Vo, T.; Dang, A.K.; Nguyen, Q.N.; Nguyen, C.T.; Hoang, C.L.; Do, K.N.; Latkin, C.A.; Ho, C.S.H.; Ho, R.C.M. Knowledge towards Cervical and Breast Cancers among Industrial Workers: Results from a Multisite Study in Northern Vietnam. Int. J. Environ. Res. Public Health 2019, 16, 4301. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph16214301
Tran BX, Vo T, Dang AK, Nguyen QN, Nguyen CT, Hoang CL, Do KN, Latkin CA, Ho CSH, Ho RCM. Knowledge towards Cervical and Breast Cancers among Industrial Workers: Results from a Multisite Study in Northern Vietnam. International Journal of Environmental Research and Public Health. 2019; 16(21):4301. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph16214301
Chicago/Turabian StyleTran, Bach Xuan, Tracy Vo, Anh Kim Dang, Quang Nhat Nguyen, Cuong Tat Nguyen, Chi Linh Hoang, Khanh Nam Do, Carl A. Latkin, Cyrus S. H. Ho, and Roger C. M. Ho. 2019. "Knowledge towards Cervical and Breast Cancers among Industrial Workers: Results from a Multisite Study in Northern Vietnam" International Journal of Environmental Research and Public Health 16, no. 21: 4301. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph16214301