‘A Healthy CIT’: An Investigation into Student Health Metrics, Lifestyle Behaviours and the Predictors of Positive Mental Health in an Irish Higher Education Setting


Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Design
2.2. Questionnaire Instrument
2.3. Survey Implementation and Data Collection Procedure
2.4. Statistical Analysis
3. Results
3.1. Response Rate and Student Demographics
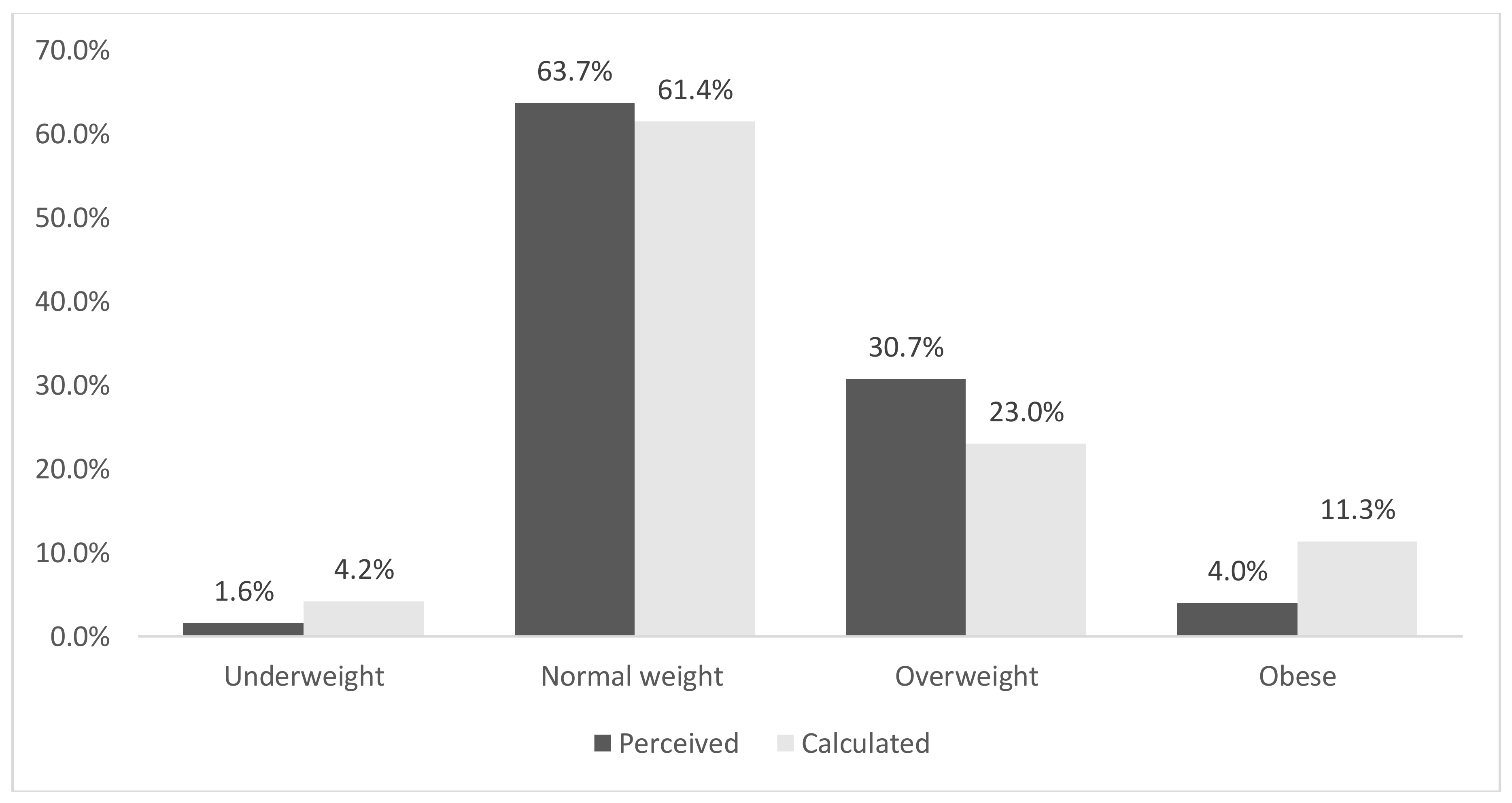
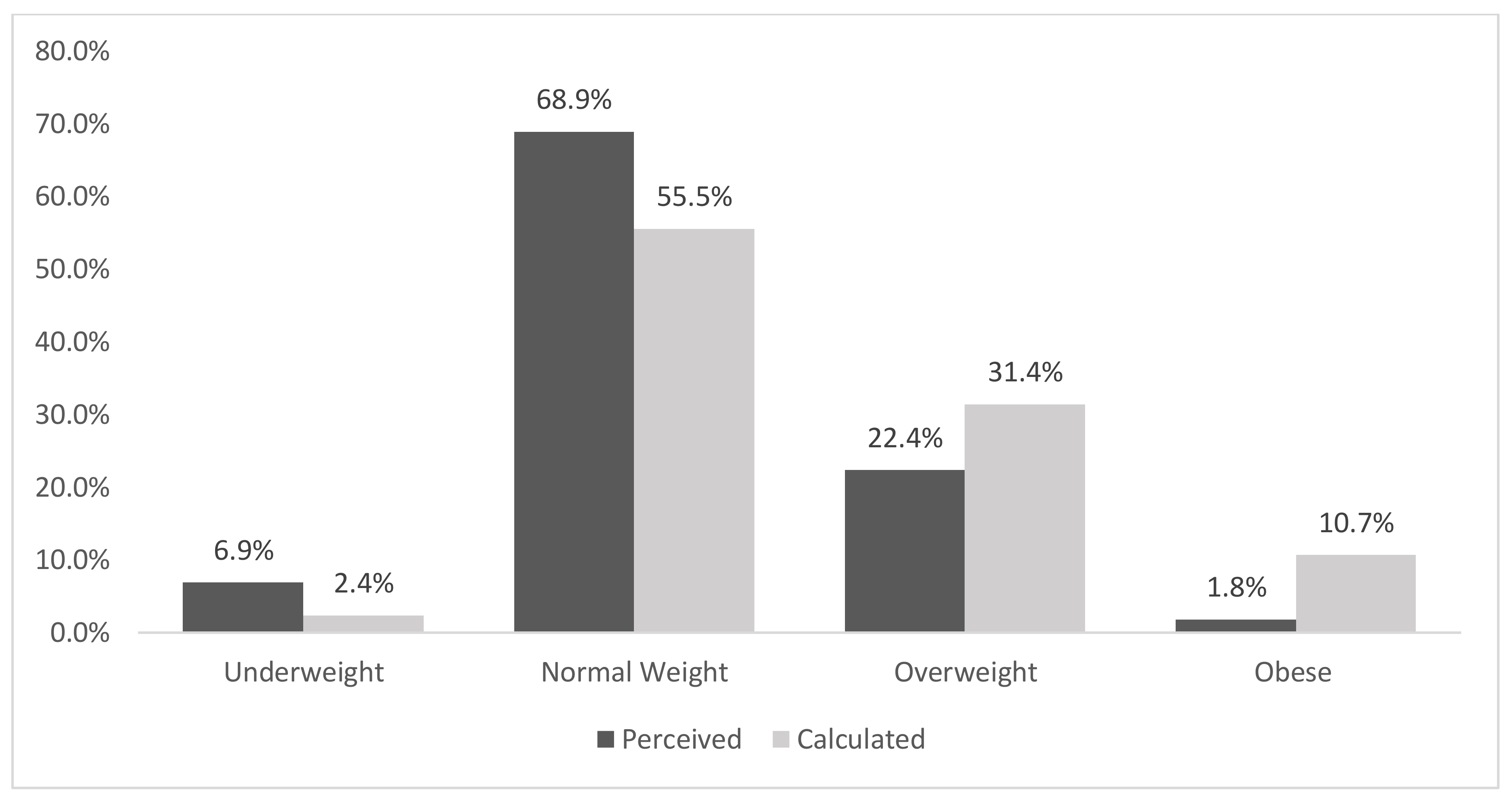
3.2. General Health and Body Mass Index [BMI]
3.3. Food Habits and Nutrition
3.4. Physical Activity and Sedentary Time
3.5. Alcohol
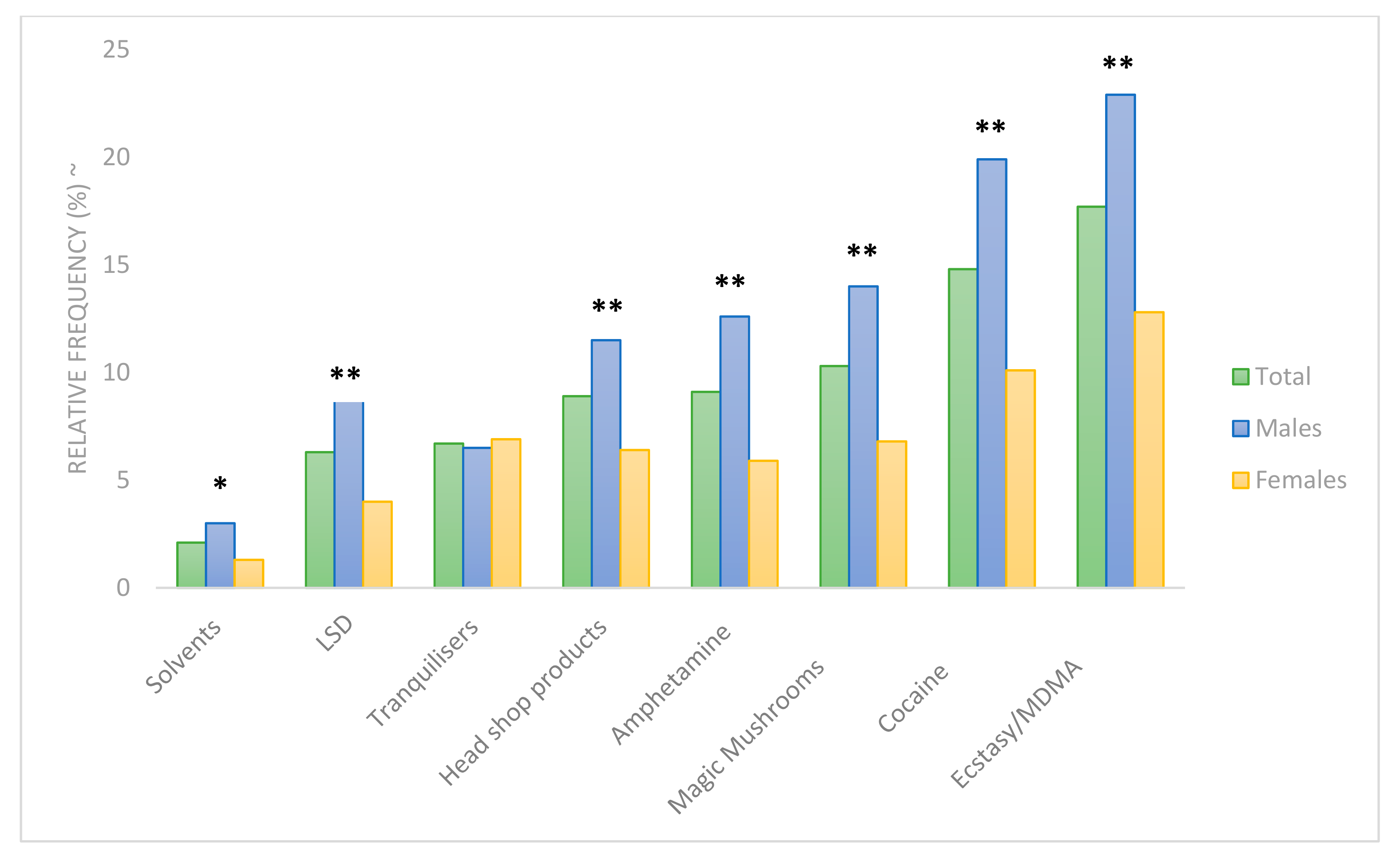
3.6. Tobacco Smoking and Illicit Substances
3.7. Sexual Health and Behaviours
3.8. Sleep
3.9. Mental Wellbeing
3.10. Social Media
3.11. Predictors of Energy and Vitality Index (EVI) Scores
4. Discussion
4.1. Strengths
4.2. Limitations
5. Conclusions
Author Contributions
Funding
Conflicts of Interest
References
- World Health Organisation (WHO). Global Status Report on Non Communicable Diseases 2014; WHO: Geneva, Switzerland, 2014. [Google Scholar]
- World Health Organisation (WHO). Non Communicable Diseases Country Profiles 2018; CC BY NC-SA 3.0 IGO; WHO: Geneva, Switzerland, 2018. [Google Scholar]
- Department of Health. Healthy Ireland. A Framework for Improved Health and Wellbeing. 2013–2025. Dublin. 2013. Available online: https://health.gov.ie/wp-content/uploads/2014/03/HealthyIrelandBrochureWA2.pdf (accessed on 9 September 2019).
- Wang, D.; Ou, C.Q.; Chen, M.Y.; Duan, N. Health-promoting lifestyles of university students in mainland China. BMC Public Health 2009, 9, 379. [Google Scholar] [CrossRef] [PubMed]
- Hunt, J.; Eisenberg, D. Mental health problems and help-seeking behavior among college students. J. Adolesc. Health 2010, 46, 3–10. [Google Scholar] [CrossRef]
- El Ansari, W.; Stock, C.; Snelgrove, S.; Hu, X.; Parke, S.; Davies, S.; John, J.; Adetunji, H.; Stoate, M.; Deeny, P.; et al. Feeling healthy? A survey of physical and psychological wellbeing of students from seven universities in the UK. Int. J. Environ. Res. Public Health 2011, 8, 1308–1323. [Google Scholar] [CrossRef] [PubMed]
- El Ansari, W.; Stock, C.; John, J.; Deeny, P.; Phillips, C.; Snelgrove, S.; Adetunji, H.; Hu, X.; Parke, S.; Stoate, M.; et al. Health promoting behaviours and lifestyle characteristics of students at seven universities in the UK. Cent. Eur. J. Public Health 2011, 19, 197–204. [Google Scholar] [CrossRef]
- Hoffman, D.J.; Policastro, P.; Quick, V.; Lee, S.K. Changes in body weight and fat mass of men and women in the first year of college: A study of the “freshman 15”. J. Am. Coll. Health 2006, 55, 41–45. [Google Scholar] [CrossRef]
- Vadeboncoeur, C.; Townsend, N.; Foster, C. A meta-analysis of weight gain in first year university students: Is freshman 15 a myth? BMC Obes. 2015, 2, 22. [Google Scholar] [CrossRef]
- De Vos, P.; Hanck, C.; Neisingh, M.; Prak, D.; Groen, H.; Faas, M.M. Weight gain in freshman college students and perceived health. Prev. Med. Rep. 2015, 2, 229–234. [Google Scholar] [CrossRef] [Green Version]
- Bodenlos, J.S.; Gengarelly, K.; Smith, R. Gender differences in freshmen weight gain. Eat. Behav. 2015, 19, 1–4. [Google Scholar] [CrossRef]
- Kelly, M.C.; Latner, J.D. Evaluating patterns of weight and body composition change among college women. Eat. Behav. 2015, 17, 157–162. [Google Scholar] [CrossRef]
- Finlayson, G.; Higgs, C.J.; Hill, A.; Hetherington, M. Susceptibility to weight gain. Eating behaviour traits and physical activity as predictors of weight gain during the first year of university. Appetite 2012, 58, 1091–1098. [Google Scholar] [CrossRef]
- Serlachius, A.; Hamer, M.; Wardle, J. Stress and weight change in university students in the United Kingdom. Physiol. Behav. 2007, 92, 548–553. [Google Scholar] [CrossRef] [PubMed]
- Gropper, S.S.; Simmons, K.P.; Connell, L.J.; Ulrich, P.V. Changes in body weight, composition, and shape: A 4-year study of college students. Appl. Physiol. Nutr. Metab. 2012, 37, 1118–1123. [Google Scholar] [CrossRef] [PubMed]
- Mikolajczyk, R.T.; Maxwell, A.E.; El Ansari, W.; Stock, C.; Petkeviciene, J.; Guillen-Grima, F. Relationship between perceived body weight and body mass index based on self- reported height and weight among university students: A cross-sectional study in seven European countries. BMC Public Health 2010, 10, 40. [Google Scholar] [CrossRef]
- Hilger, J.; Loerbroks, A.; Diehl, K. Eating behaviour of university students in Germany: Dietary intake, barriers to healthy eating and changes in eating behaviour since the time of matriculation. Appetite 2017, 109, 100–107. [Google Scholar] [CrossRef]
- Opoku-Acheampong, A.A.; Kidd, T.; Adhikari, K.; Muturi, N.; Kattelmann, K. Assessing physical activity, fruit, vegetable, and sugar-sweetened beverage intake patterns of college students in Kansas. J. Nutr. Educ. Behav. 2018, 50, 977–983. [Google Scholar] [CrossRef]
- Unusan, N. Linkage between stress and fruit and vegetable intake among university students: An empirical analysis on Turkish students. Nutr. Res. 2006, 26, 385–390. [Google Scholar] [CrossRef]
- Papadaki, A.; Hondros, G.; Scott, J.; Kapsokefalou, M. Eating habits of University students living at, or away from home in Greece. Appetite 2007, 49, 169–176. [Google Scholar] [CrossRef]
- Keller, S.; Maddock, J.E.; Hannöver, W.; Thyrian, J.R.; Basler, H.D. Multiple health risk behaviors in German first year university students. Prev. Med. 2008, 46, 189–195. [Google Scholar] [CrossRef]
- Morse, K.L.; Driskell, J.A. Observed sex differences in fast-food consumption and nutrition self-assessments and beliefs of college students. Nutr. Res. 2009, 29, 173–179. [Google Scholar] [CrossRef]
- Driskell, J.A.; Meckna, B.R.; Scales, N.E. Differences exist in the eating habits of university men and women at fast-food restaurants. Nutr. Res. 2006, 26, 524–530. [Google Scholar] [CrossRef]
- Hope, A.; Dring, C.; Dring, J. The Health of Irish Students: College Lifestyle and Attitudinal National (CLAN) Survey; Department of Health and Children: Dublin, Ireland, 2005. [Google Scholar]
- Nelson, M.C.; Lust, K.; Story, M.; Ehlinger, E. Credit card debt, stress and key health risk behaviors among college students. Am. J. Health Promot. 2008, 22, 400–406. [Google Scholar] [CrossRef] [PubMed]
- Diehl, K.; Hilger, J. Physical activity and the transition from school to university: A cross-sectional survey among university students in Germany. Sci. Sport 2016, 31, 223–226. [Google Scholar] [CrossRef]
- LaCaille, L.J.; Dauner, K.N.; Krambeer, R.J.; Pedersen, J. Psychosocial and environmental determinants of eating behaviors, physical activity, and weight change among college students: A qualitative analysis. J. Am. Coll. Health 2011, 59, 531–538. [Google Scholar] [CrossRef] [PubMed]
- Davoren, M.P.; Shiely, F.; Byrne, M.; Perry, I.J. Hazardous alcohol consumption among university students in Ireland: A cross-sectional study. BMJ Open 2015, 5, e006045. [Google Scholar] [CrossRef] [PubMed]
- Heather, N.; Partington, S.; Partington, E.; Longstaff, F.; Allsop, S.; Jankowski, M.; Wareham, H.; St Clair Gibson, A. Alcohol use disorders and hazardous drinking among undergraduates at English universities. Alcohol. Alcohol. 2011, 46, 270–277. [Google Scholar] [CrossRef]
- Bewick, B.M.; Mulhern, B.; Barkham, M.; Trusler, K.; Hill, A.J.; Stiles, W.B. Changes in undergraduate student alcohol consumption as they progress through university. BMC Public Health 2008, 8, 163. [Google Scholar] [CrossRef]
- Lannoy, S.; Billieux, J.; Poncin, M.; Maurage, P. Binging at the campus: Motivations and impulsivity influence binge drinking profiles in university students. Psychiatry Res. 2017, 250, 146–154. [Google Scholar] [CrossRef]
- Hallett, J.; Howat, P.M.; Maycock, B.R.; McManus, A.; Kypri, K.; Dhaliwal, S.S. Undergraduate student drinking and related harms at an Australian university: Web-based survey of a large random sample. BMC Public Health 2012, 12, 37. [Google Scholar] [CrossRef]
- Connor, J.; Gray, A.; Kypri, K. Drinking history, current drinking and problematic sexual experiences among university students. Aust. N. Z. J. Public Health 2010, 34, 487–494. [Google Scholar] [CrossRef]
- Kypri, K.; Langley, J.D.; McGee, R.; Saunders, J.B.; Williams, S. High prevalence persistent hazardous drinking among New Zealand tertiary students. Alcohol. Alcohol. 2002, 37, 457–464. [Google Scholar] [CrossRef]
- Zakletskaia, L.; Wilson, E.; Fleming, M.F. Alcohol Use in Students Seeking Primary Care Treatment at University Health Services. J. Am. Coll. Health 2010, 59, 217–223. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Maphisa, J.M.; Young, C. Risk of alcohol use disorder among South African university students: The role of drinking motives. Addict. Behav. 2018, 82, 44–49. [Google Scholar] [CrossRef] [PubMed]
- Quintela, O.; Bermejo, A.M.; Tabernero, M.J.; Strano-Rossi, S.; Chiarotti, M.; Lucas, A.C. Evaluation of cocaine, amphetamines and cannabis use in university students through hair analysis: Preliminary results. Forensic Sci. Int. 2000, 107, 273–279. [Google Scholar] [CrossRef]
- Bennett, T.; Holloway, K. Motives for illicit prescription drug use among university students: A systematic review and meta-analysis. Int. J. Drug Policy 2017, 44, 12–22. [Google Scholar] [CrossRef]
- Downing-Matibag, T.M.; Geisinger, B. Hooking up and sexual risk taking among college students: A health belief model perspective. Qual. Health Res. 2009, 19, 1196–1209. [Google Scholar] [CrossRef]
- Beiter, R.; Nash, R.; McCrady, M.; Rhoades, D.; Linscomb, M.; Clarahan, M.; Sammut, S. The prevalence and correlates of depression, anxiety, and stress in a sample of college students. J. Affect. Disord. 2015, 173, 90–96. [Google Scholar] [CrossRef]
- Becker, S.P.; Jarrett, M.A.; Luebbe, A.M.; Garner, A.A.; Burns, G.L.; Kofler, M.J. Sleep in a large, multi-university sample of college students: Sleep problem prevalence, sex differences, and mental health correlates. Sleep Health 2018, 4, 174–181. [Google Scholar] [CrossRef]
- Barone, T.L. “Sleep is on the back burner”: Working students and sleep. Soc. Sci. J. 2017, 54, 159–167. [Google Scholar] [CrossRef]
- Demirci, K.; Akgönül, M.; Akpinar, A. Relationship of smartphone use severity with sleep quality, depression, and anxiety in university students. J. Behav. Addict. 2015, 4, 85–92. [Google Scholar] [CrossRef] [Green Version]
- Orsal, O.; Orsal, O.; Unsal, A.; Ozalp, S.S. Evaluation of internet addiction and depression among university students. Procedia Soc. Behav. Sci. 2013, 82, 445–454. [Google Scholar] [CrossRef]
- Moreno, M.A.; Whitehill, J.M. Influence of social media on alcohol use in adolescents and young adults. Alcohol. Res. 2014, 36, 91. [Google Scholar] [PubMed]
- Moreno, M.A.; D’Angelo, J.; Whitehill, J. Social media and alcohol: Summary of research, intervention ideas and future study directions. Media Commun. 2016, 4, 50–59. [Google Scholar] [CrossRef]
- Dodd, L.J.; Al-Nakeeb, Y.; Nevill, A.; Forshaw, M.J. Lifestyle risk factors of students: A cluster analytical approach. Prev. Med. 2010, 51, 73–77. [Google Scholar] [CrossRef]
- Moreno-Gómez, C.; Romaguera-Bosch, D.; Tauler-Riera, P.; Bennasar-Veny, M.; Pericas-Beltran, J.; Martinez-Andreu, S.; Aguilo-Pons, A. Clustering of lifestyle factors in Spanish university students: The relationship between smoking, alcohol consumption, physical activity and diet quality. Public Health Nutr. 2012, 15, 2131–2139. [Google Scholar] [CrossRef]
- Varela-Mato, V.; Cancela, J.M.; Ayan, C.; Martin, V.; Molina, A. Lifestyle and health among Spanish university students: Differences by gender and academic discipline. Int. J. Environ. Res. Public Health 2012, 9, 2728–2741. [Google Scholar] [CrossRef]
- Okanagan Charter: An International Charter for Health Promoting Universities & Colleges. 2015. Available online: https://internationalhealthycampuses2015.sites.olt.ubc.ca/files/2016/01/Okanagan-Charter-January13v2.pdf (accessed on 12 September 2019).
- Bickerdike, A.; Dinneen, J.; O’Neill, C. ‘A Healthy CIT’: A case study outlining the initial development of a campus health promotion initiative in an Irish higher education setting. In Proceedings of the Smart Cities in Smart Regions Conference, Finland University of Applied Sciences, Lahti, Finland, 26–27 September 2018; Aarrevaara, E., Harjapää, A., Eds.; Lahti University of Applied Sciences: Lahti, Finland, 2018. [Google Scholar]
- Mac Neela, P.; Dring, C.; Van Lente, E.; Place, C.; Dring, J.; Mc Caffrey, J. Health and Wellbeing of NUI Galway Undergraduate Students: The Student Lifestyle Survey; NUIG Galway: Galway, Ireland, 2012. [Google Scholar]
- Mac Neela, P. Personal communication; NUI Galway: Galway, Ireland, 2015. [Google Scholar]
- Morgan, K.; McGee, H.; Watson, D.; Perry, I.; Barry, M.; Shelley, E.; Harrington, J.; Molcho, M.; Layte, R.; Tully, N.; et al. SLAN 2007: Survey of Lifestyle, Attitudes & Nutrition in Ireland: Main Report; Department of Health and Children: Dublin, Ireland, 2008. [Google Scholar]
- Body Mass Index-BMI. Available online: http://www.euro.who.int/en/health-topics/disease-prevention/nutrition/a-healthy-lifestyle/body-mass-index-bmi (accessed on 12 September 2019).
- Craig, C.L.; Marshall, A.L.; Sjöström, M.; Bauman, A.E.; Booth, M.L.; Ainsworth, B.E.; Pratt, M.; Ekelund, U.; Yngve, A.; Sallis, J.F.; et al. International physical activity questionnaire: 12-country reliability and validity. Med. Sci. Sports Exerc. 2003, 35, 1381–1395. [Google Scholar] [CrossRef]
- Department of Health & Children; Health Service Executive. The National Guidelines on Physical Activity for Ireland; Dept Health & Health Service Executive: Dublin, Ireland, 2009. [Google Scholar]
- Sport Ireland; IPSOS MRBI. Irish Sports Monitor 2015 Annual Report; Sport Ireland: Dublin, Ireland, 2015. [Google Scholar]
- Babor, T.F.; Higgins-Biddle, J.C.; Saunders, J.B.; Monteiro, M.G. The Alcohol Use Disorders Identification Test. Guidelines for Use in Primary Care; WHO: Geneva, Switzerland, 2001. [Google Scholar]
- Ware, J.; Snoww, K.K.; Kosinksi, M.A.; Gandek, B.G. SF-36 Health Survey: Manual and Interpretation Guide; Quality Metric, Inc.: Lincoln, RI, USA, 1993. [Google Scholar]
- Buysse, D.J.; Reynolds, C.F.; Monk, T.H.; Berman, S.R.; Kupfer, D.J. The Pittsburgh Sleep Quality Index: A new instrument for psychiatric practice and research. Psychiatry Res 1989, 28, 193–213. [Google Scholar] [CrossRef]
- Bickerdike, A.; Deasmhunaigh, C.; O’Flynn, S.; O’Tuathaigh, C. Learning strategies, study habits and social networking activity of undergraduate medical students. Int. J. Med. Educ. 2016, 7, 230–236. [Google Scholar] [CrossRef] [Green Version]
- Kunttu, K.; Pesonen, T. Student Health Survey 2012: A National Survey among Finnish University Students; Finnish Student Health Service: Helsinki, Finland, 2013. [Google Scholar]
- Key Facts and Figures for 2017/18. Available online: https://hea.ie/statistics/data_visualisations/infographics/ (accessed on 22 August 2019).
- Lee, R.L.; Loke, A.J. Health-promoting behaviors and psychosocial well-being of university students in Hong Kong. Public Health Nurs. 2005, 22, 209–220. [Google Scholar] [CrossRef]
- IPSOS MRBI; Dept of Health. Healthy Ireland Survey 2018 Summary of Findings; Stationery Office: Dublin, Ireland, 2018. Available online: https://health.gov.ie/wp-content/uploads/2018/10/Healthy-Ireland-Survey-2018.pdf (accessed on 12 September 2019).
- Vaez, M.; Laflamme, L. Health behaviors, self-rated health, and quality of life: A study among first-year Swedish university students. J. Am. Coll. Health 2003, 51, 156. [Google Scholar] [CrossRef]
- Wardle, J.; Haase, A.M.; Steptoe, A. Body image and weight control in young adults: International comparisons in university students from 22 countries. Int. J. Obes. 2006, 30, 644–651. [Google Scholar] [CrossRef] [PubMed]
- Di Angelantonio, E.; Bhupathiraju, S.N.; Wormser, D.; Gao, P.; Kaptoge, S.; Berrington de Gonzalez, A.; Cairns, B.J.; Huxley, R.; Jackson, ChL.; Joshy, G.; et al. Body-mass index and all-cause mortality: Individual-participant-data meta-analysis of 239 prospective studies in four continents. Lancet 2016, 388, 776–786. [Google Scholar] [CrossRef]
- Finer, N. Medical consequences of obesity. Medicine 2015, 43, 88–93. [Google Scholar] [CrossRef]
- McHugh, M.L. Interrater reliability: The kappa statistic. Biochem. Med. 2012, 22, 276–282. [Google Scholar] [CrossRef]
- Herman, K.M.; Hopman, W.M.; Rosenberg, M.W. Self-rated health and life satisfaction among Canadian adults: Associations of perceived weight status versus BMI. Qual. Life Res. 2013, 22, 2693–2705. [Google Scholar] [CrossRef] [PubMed]
- Inoue, M.; Toyokawa, S.; Miyoshi, Y.; Miyano, Y.; Suzuki, T.; Suyama, Y.; Inoue, K.; Kobayashi, Y. Degree of agreement between weight perception and body mass index of Japanese workers: MY Health Up Study. J. Occup. Health 2007, 49, 376–381. [Google Scholar] [CrossRef] [PubMed]
- Robinson, E. Overweight but unseen: A review of the underestimation of weight status and a visual normalization theory. Obes. Rev. 2017, 18, 1200–1209. [Google Scholar] [CrossRef]
- Healthy Food for Life. Available online: https://www.hse.ie/eng/about/who/healthwellbeing/our-priority-programmes/heal/food-pyramid-images/foodforlifefoodpyramidrationale2016.pdf (accessed on 12 September 2019).
- Chau, J.Y.; Grunseit, A.C.; Chey, T.; Stamatakis, E.; Brown, W.J.; Matthews, C.E.; Bauman, A.E.; van der Ploeg, H.P. Daily sitting time and all-cause mortality: A meta-analysis. PLoS ONE 2013, 8, e80000. [Google Scholar] [CrossRef]
- Reinert, D.F.; Allen, J.P. The alcohol use disorders identification test: An update of research findings. Alcohol. Clin. Exp. Res. 2007, 31, 185–199. [Google Scholar] [CrossRef]
- De Meneses-Gaya, C.; Zuardi, A.; Loureiro, S.R.; Crippa, J.A.S. Alcohol Use Disorders Identification Test (AUDIT): An updated systematic review of psychometric properties. Psychol. Neurosci. 2009, 2, 83–97. [Google Scholar] [CrossRef]
- Kokotailo, P.K.; Egan, J.; Gangnon, R.; Brown, D.; Mundt, M.; Fleming, M. Validity of the alcohol use disorders identification test in college students. Alcohol. Clin. Exp. Res. 2004, 28, 914–920. [Google Scholar] [CrossRef] [PubMed]
- Capron, D.W.; Schmidt, N.B. Positive drinking consequences among hazardous drinking college students. Addict. Behav. 2012, 37, 663–667. [Google Scholar] [CrossRef] [PubMed]
- IPSOS MRBI; Dept of Health. Healthy Ireland Survey 2016 Summary of Findings; Stationery Office: Dublin, Ireland, 2016. Available online: https://health.gov.ie/wp-content/uploads/2016/10/Healthy-Ireland-Survey-2016-Summary-Findings.pdf (accessed on 12 September 2019).
- Houghton, F.; Keane, N.; Murphy, N.; Houghton, S.; Dunne, C. Tertiary level students and the mental health index (MHI-5) in Ireland. Irish J. Appl. Soc. Stud. 2011, 10, 7. [Google Scholar] [CrossRef]
- Stallman, H.M. Psychological distress in university students: A comparison with general population data. Aust. Psychol. 2010, 45, 249–257. [Google Scholar] [CrossRef]
- Eskin, M.; Sun, J.M.; Abuidhail, J.; Yoshimasu, K.; Kujan, O.; Janghorbani, M.; Flood, C.; Carta, M.G.; Tran, U.S.; Mechri, A.; et al. Suicidal behavior and psychological distress in university students: A 12-nation study. Arch. Suicide Res. 2016, 20, 369–388. [Google Scholar] [CrossRef] [PubMed]
- Hayley, A.C.; Sivertsen, B.; Hysing, M.; Vedaa, Ø.; Øverland, S. Sleep difficulties and academic performance in Norwegian higher education students. Br. J. Educ. Psychol. 2017, 87, 722–737. [Google Scholar] [CrossRef]
- Önder, İ.; Beşoluk, Ş.; İskender, M.; Masal, E.; Demirhan, E. Circadian preferences, sleep quality and sleep patterns, personality, academic motivation and academic achievement of university students. Learn. Individ. Differ. 2014, 32, 184–192. [Google Scholar] [CrossRef]
- Flueckiger, L.; Roselind, L.; Meyer, A.H.; Mata, J. How health behaviors relate to academic performance via affect: An intensive longitudinal study. PLoS ONE 2014, 9, e0111080. [Google Scholar] [CrossRef]
- Ahrberg, K.; Dresler, M.; Niedermaier, S.; Steiger, A.; Genzel, L. The interaction between sleep quality and academic performance. J. Psychiatr. Res. 2012, 46, 1618–1622. [Google Scholar] [CrossRef]
- Abdulghani, H.M.; Alrowais, N.A.; Bin-Saad, N.S.; Al-Subaie, N.M.; Haji, A.M.; Alhaqwi, A.I. Sleep disorder among medical students: Relationship to their academic performance. Med. Teach. 2012, 34, 37–41. [Google Scholar] [CrossRef]
- Gilbert, S.P.; Weaver, C.C. Sleep quality and academic performance in university students: A wake-up call for college psychologists. J. Coll. Stud. Psychother. 2010, 24, 295–306. [Google Scholar] [CrossRef]
- Forquer, L.M.; Camden, A.E.; Gabriau, K.M.; Johnson, C.M. Sleep patterns of college students at a public university. J. Am. Coll. Health 2008, 56, 563–565. [Google Scholar] [CrossRef] [PubMed]
- Mongan, D.; Long, J. Overview of Alcohol Consumption, Alcohol-Related Harm and Alcohol Policy in Ireland; HRB Overview Series 10; HRB: Dublin, Ireland, 2016. [Google Scholar]
- Davoren, M.P.; Demant, J.; Shiely, F.; Perry, I.J. Alcohol consumption among university students in Ireland and the United Kingdom from 2002 to 2014: A systematic review. BMC Public Health 2016, 16, 173. [Google Scholar] [CrossRef] [PubMed]




{kind=link}
{kind=link}
{kind=link}
| Demographic Variable | Total | M | F | p-Value * | |||
|---|---|---|---|---|---|---|---|
| n | % | n | % | n | % | ||
| Sex | 2267 | 1094 | 48.3 | 1173 | 51.7 | ||
| Age | |||||||
| 18–20 years # | 806 | 35.6 | 357 | 32.7 | 449 | 38.4 | 0.003 |
| 21–23 years | 754 | 33.3 | 362 | 33.1 | 392 | 33.5 | |
| 24 years and older # | 703 | 31.1 | 374 | 34.2 | 329 | 28.1 | |
| Total | 2263 | 1093 | 1170 | ||||
| Mode of study | |||||||
| Undergraduate | 1891 | 90.2 | 907 | 89.4 | 984 | 91.0 | 0.22 |
| Postgraduate (Taught) | 133 | 6.3 | 66 | 6.5 | 67 | 6.2 | |
| Postgraduate (Research) | 72 | 3.4 | 42 | 4.1 | 30 | 2.8 | |
| Total | 2096 | 1015 | 1081 | ||||
| Registration status | |||||||
| Full-time | 1918 | 88.4 | 919 | 87.6 | 999 | 89.2 | 0.28 |
| Part-time or evening | 251 | 11.6 | 130 | 12.4 | 121 | 10.8 | |
| Total | 2169 | 1049 | 1120 | ||||
| Faculty ** | |||||||
| Business & Humanities # | 941 | 42.9 | 327 | 30.8 | 614 | 54.2 | <0.0005 |
| Engineering & Science # | 922 | 42.0 | 579 | 54.6 | 343 | 30.3 | |
| Crawford College of Art & Design # | 169 | 7.7 | 59 | 5.6 | 110 | 9.7 | |
| Cork School of Music # | 98 | 4.5 | 37 | 3.5 | 61 | 5.4 | |
| National Maritime College of Ireland # | 51 | 2.3 | 49 | 4.6 | 2 | 0.2 | |
| Other # | 13 | 0.6 | 10 | 0.9 | 3 | 0.3 | |
| Total | 2194 | 1061 | 1133 | ||||
| Year Group (undergraduates) | |||||||
| 1 | 642 | 32.6 | 298 | 31.7 | 344 | 33.5 | 0.49 |
| 2 | 510 | 25.9 | 256 | 27.2 | 254 | 24.7 | |
| 3 | 464 | 23.6 | 213 | 22.7 | 251 | 24.4 | |
| 4 | 338 | 17.2 | 165 | 17.6 | 173 | 16.8 | |
| Other | 13 | 0.7 | 8 | 0.9 | 5 | 0.5 | |
| Total | 1967 | 940 | 1027 | ||||
| Year Group (postgraduates) | |||||||
| 1 | 97 | 47.5 | 47 | 43.5 | 50 | 52.1 | 0.06 |
| 2 | 49 | 24.0 | 22 | 20.4 | 27 | 28.1 | |
| 3 | 20 | 9.8 | 11 | 10.2 | 9 | 9.4 | |
| 4 | 23 | 11.3 | 16 | 14.8 | 7 | 7.3 | |
| 5/6/Other # | 15 | 7.4 | 12 | 11.1 | 3 | 3.1 | |
| Total | 204 | 108 | 96 | ||||
| Nationality | |||||||
| Irish # | 1937 | 89.2 | 954 | 91.0 | 983 | 87.5 | |
| UK | 30 | 1.4 | 16 | 1.5 | 14 | 1.2 | 0.006 |
| Other European # | 141 | 6.5 | 48 | 4.6 | 93 | 8.3 | |
| Other | 64 | 2.9 | 30 | 2.9 | 34 | 3.0 | |
| Total | 2172 | 1048 | 1124 | ||||
| Academic Achievement (undergraduates only) | |||||||
| Less than 40% | 11 | 0.6 | 6 | 0.6 | 5 | 0.5 | 0.02 |
| 40–59% # | 464 | 23.9 | 253 | 27.2 | 211 | 20.9 | |
| 60–69% | 766 | 39.5 | 357 | 38.3 | 409 | 40.6 | |
| 70% or above | 491 | 25.3 | 226 | 24.3 | 265 | 26.3 | |
| Don’t Know # | 144 | 7.4 | 57 | 6.1 | 87 | 8.6 | |
| Declined to Provide this Information | 63 | 3.2 | 32 | 3.4 | 31 | 3.1 | |
| Total | 1940 | 931 | 1008 | ||||
| Physical Activity Variable | Total | M | F | p-Value * | |||
|---|---|---|---|---|---|---|---|
| n | % | n | % | n | % | ||
| Perceived Barriers | |||||||
| No time/workload/exams | 862 | 51.6 | 408 | 51.1 | 454 | 52.2 | <0.0005 |
| Already take enough exercise # | 208 | 12.5 | 122 | 15.3 | 86 | 9.9 | |
| Interested but not willing to spend time | 170 | 10.2 | 85 | 10.6 | 85 | 9.8 | |
| Injury/disability/medical # condition/pregnancy | 124 | 7.4 | 48 | 6.0 | 76 | 8.7 | |
| Not the sporty type | 93 | 5.6 | 36 | 4.5 | 57 | 6.6 | |
| No access to facilities # | 65 | 3.9 | 21 | 2.6 | 44 | 5.1 | |
| Not interested | 63 | 3.8 | 30 | 3.8 | 33 | 3.8 | |
| Exercising too much/overtraining # | 43 | 2.6 | 32 | 4.0 | 11 | 1.3 | |
| Other | 41 | 2.5 | 17 | 2.1 | 24 | 2.8 | |
| Total | 1669 | 799 | 870 | ||||
| Sitting time during average day at college (hours) | |||||||
| Less than 1 hour | 25 | 1.4 | 8 | 0.9 | 17 | 1.9 | 0.48 |
| 1–2 h | 56 | 3.2 | 26 | 3.1 | 30 | 3.4 | |
| 2–3 h | 163 | 9.4 | 76 | 9.0 | 87 | 9.8 | |
| 3–4 h | 351 | 20.2 | 180 | 21.3 | 171 | 19.3 | |
| 4–5 h | 475 | 27.4 | 227 | 26.8 | 248 | 28.0 | |
| More than 5 h | 664 | 38.3 | 330 | 39.0 | 334 | 37.7 | |
| Total | 1734 | 847 | 887 | ||||
| AUDIT Domain | Items | Cronbach’s α | Total | Males | Females | p-Value # | |||
|---|---|---|---|---|---|---|---|---|---|
| n * | Median | n | Median | n | Median | ||||
| Total AUDIT | 1–10 | 0.82 | 1329 | 7.0 | 651 | 8.0 | 678 | 7.0 | <0.0005 |
| Hazardous Alcohol Use | 1–3 | 0.66 | 1469 | 5.0 | 707 | 6.0 | 762 | 5.0 | <0.0005 |
| Dependence symptoms | 4–6 | 0.61 | 1430 | 0.0 | 694 | 0.0 | 736 | 0.0 | 0.57 |
| Harmful alcohol use | 7–10 | 0.68 | 1412 | 2.0 | 683 | 2.00 | 729 | 1.0 | 0.43 |
| ‘In What Way Do You Protect Yourself from a Sexually Transmitted Infection?’ (Yes) | Total (n = 1356)~ | Males (n = 659) | Females (n = 697) | p-Value * |
|---|---|---|---|---|
| I don’t protect myself at all | 6.2 | 6.8 | 5.6 | 0.41 |
| I protect myself by use of a condom | 61.6 | 68.3 | 55.2 | <0.0005 |
| I have intercourse with only one constant partner | 50.2 | 44.0 | 56.1 | <0.0005 |
| I expect my partner to have an STI test | 5.9 | 3.6 | 8.0 | 0.001 |
| Other | 1.4 | 0.8 | 2.0 | 0.08 |
| ‘Did You Drink Alcohol and/or Use Drugs before You Had Sexual Intercourse the Last Time?’ (Yes/No) | Total (n = 1331) | Males (n = 650) | Females (n = 681) | p-Value * |
| Yes | 31.6 | 34.8 | 28.5 | 0.02 |
| ‘Have You (or Your Partner) ever Used the Morning after Pill?’ (Yes/No) | Total (n = 1322) | Males (n = 629) | Females (n = 693) | p-Value * |
| Yes | 44.4 | 36.7 | 51.4 | <0.0005 |
| Psychological Stressor (‘Highly Stressed’) | Total | Males | Females | Md. MHI-5 Scores (‘Highly Stressed’ vs. other Categories) # | ||||
|---|---|---|---|---|---|---|---|---|
| (n) | % | (n) | % | (n) | % | |||
| Exams | 524 | 34.6 | 179 | 24.2 *** | 345 | 44.5 | 56.0 *** | 68.0 |
| College workload | 432 | 28.3 | 149 | 20.1 *** | 283 | 36.1 | 56.0 *** | 68.0 |
| Studies in general | 377 | 24.6 | 122 | 16.4 *** | 255 | 32.4 | 50.0 *** | 68.0 |
| Financial situation | 352 | 23.1 | 138 | 18.6 *** | 214 | 27.2 | 53.5 *** | 68.0 |
| Pressure outside of work/college | 290 | 19.4 | 93 | 12.8 *** | 197 | 25.7 | 52.0 *** | 68.0 |
| Competition at college | 160 | 10.7 | 52 | 7.1 *** | 108 | 14.0 | 48.0 *** | 64.0 |
| Living situation | 147 | 9.7 | 46 | 6.2 *** | 101 | 13.0 | 44.0 *** | 64.0 |
| Family situation | 141 | 9.3 | 45 | 6.1 *** | 96 | 12.3 | 44.0 *** | 64.0 |
| Relationships/sexuality | 98 | 6.5 | 38 | 5.2 | 60 | 7.7 | 40.0*** | 64.0 |
| Illness | 68 | 4.5 | 17 | 2.3 *** | 51 | 6.6 | 32.0 *** | 64.0 |
| Circle of friends | 55 | 3.6 | 18 | 2.5 * | 37 | 4.7 | 32.0 *** | 64.0 |
| Social Media | 33 | 2.2 | 9 | 1.2 * | 24 | 3.1 | 36.0 *** | 64.0 |
| Social Media Platform | Total (n = 1537) | Males (n = 751) | Females (n = 786) | p-Value |
|---|---|---|---|---|
| 93.0 | 90.3 | 95.7 | <0.0005 | |
| Snapchat | 69.2 | 64.2 | 74.0 | <0.0005 |
| 54.2 | 42.7 | 65.1 | <0.0005 | |
| 40.6 | 40.6 | 40.6 | 1.0 | |
| 27.4 | 29.2 | 25.7 | 0.14 | |
| No social media account | 3.6 | 5.5 | 1.9 | <0.0005 |
| Other | 2.7 | 2.5 | 2.9 | 0.75 |
| Predictor Variable | Standardised β | p-Value |
|---|---|---|
| Sex | −0.15 | <0.0005 |
| General health rating | 0.15 | <0.0005 |
| Daily total fruit and vegetable servings | 0.08 | <0.0005 |
| AUDIT-C scores | 0.05 | 0.04 |
| Mental health rating | 0.32 | <0.0005 |
| Recent sleep quality | 0.27 | <0.0005 |
| Social media 90 min or more on weekdays | −0.06 | 0.01 |
| Perception of being overweight/obese | −0.09 | <0.0005 |
| Adjusted R Squared of the Model | 0.370 | <0.0005 |
© 2019 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Bickerdike, A.; Dinneen, J.; O’Neill, C. ‘A Healthy CIT’: An Investigation into Student Health Metrics, Lifestyle Behaviours and the Predictors of Positive Mental Health in an Irish Higher Education Setting. Int. J. Environ. Res. Public Health 2019, 16, 4318. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph16224318
Bickerdike A, Dinneen J, O’Neill C. ‘A Healthy CIT’: An Investigation into Student Health Metrics, Lifestyle Behaviours and the Predictors of Positive Mental Health in an Irish Higher Education Setting. International Journal of Environmental Research and Public Health. 2019; 16(22):4318. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph16224318
Chicago/Turabian StyleBickerdike, Andrea, Joan Dinneen, and Cian O’Neill. 2019. "‘A Healthy CIT’: An Investigation into Student Health Metrics, Lifestyle Behaviours and the Predictors of Positive Mental Health in an Irish Higher Education Setting" International Journal of Environmental Research and Public Health 16, no. 22: 4318. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph16224318