Association between Basal Metabolic Rate and Handgrip Strength in Older Koreans


Abstract
:1. Introduction
2. Materials and Methods
2.1. Survey Overview and Study Population
2.2. Data Collection
2.3. Definition of Comorbidity Number
2.4. Definitions of BMR
2.5. Definitions of Fat Mass
2.6. Statistical Analysis
2.7. Ethics Statement
3. Results
3.1. Clinical Characteristics of the Participants
3.2. Association between BMR and Studied Variables
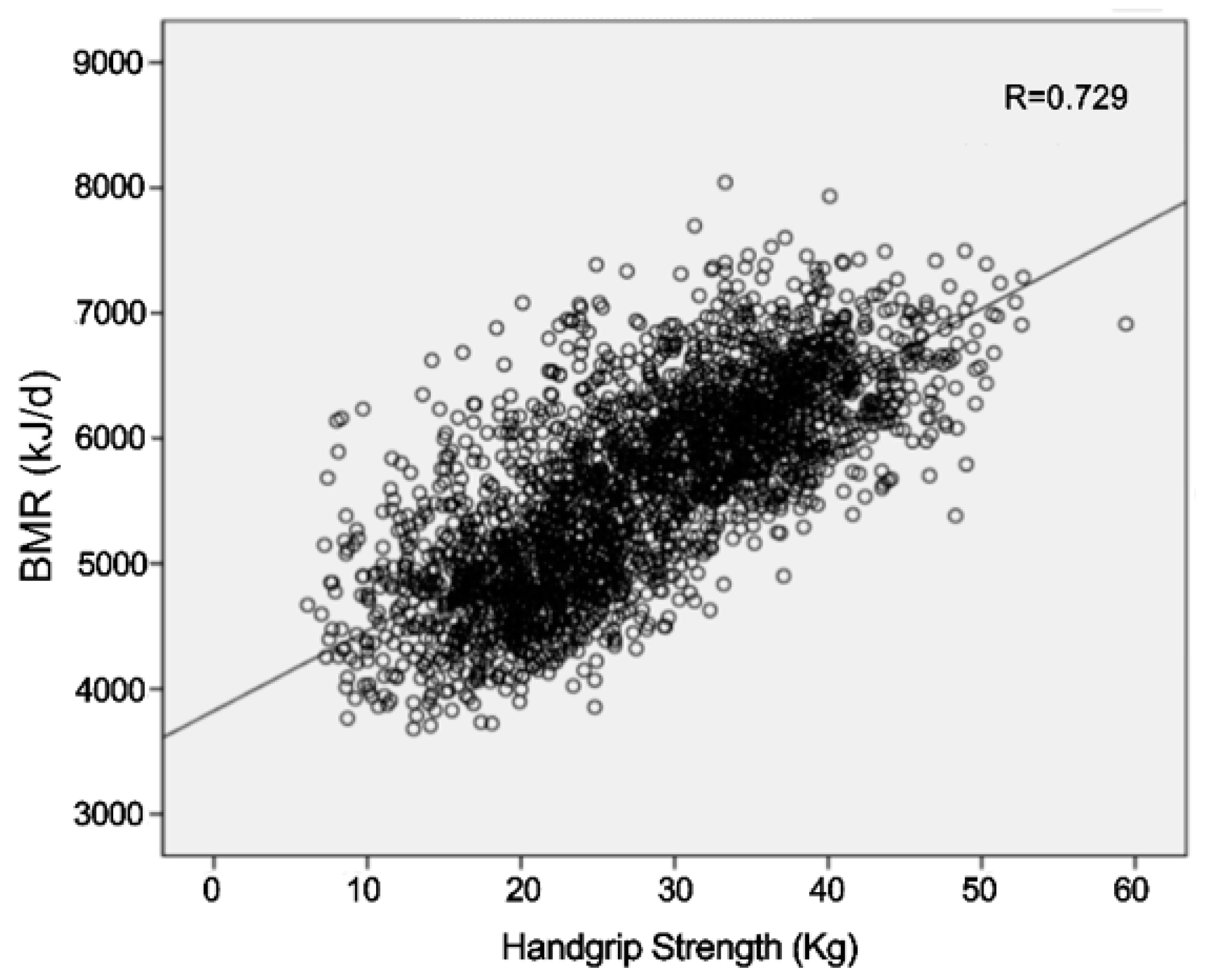
3.3. Association between BMR and HGS
4. Discussion
5. Conclusions
Author Contributions
Funding
Conflicts of Interest
References
- Sabounchi, N.S.; Rahmandad, H.; Ammerman, A. Best-fitting prediction equations for basal metabolic rate: Informing obesity interventions in diverse populations. Int. J. Obes. 2013, 37, 1364. [Google Scholar] [CrossRef] [PubMed]
- Aversa, Z.; Costelli, P.; Muscaritoli, M. Cancer-induced muscle wasting: Latest findings inprevention and treatment. Ther. Adv. Med. Oncol. 2017, 9, 369–382. [Google Scholar] [CrossRef] [PubMed]
- Zhang, K.; Sun, M.; Werner, P.; Kovera, A.; Albu, J.; Pi-Sunyer, F.; Boozer, C. Sleeping metabolic rate in relation to body mass index and body composition. Int. J. Obes. 2002, 26, 376. [Google Scholar] [CrossRef] [PubMed]
- Speakman, J.R.; Selman, C. Physical activity and resting metabolic rate. Proc. Nutr. Soc. 2003, 62, 621–634. [Google Scholar] [CrossRef] [PubMed]
- Visser, M.; Deeg, D.J.; Lips, P.; Harris, T.B.; Bouter, L.M. Skeletal muscle mass and muscle strength in relation to lower-extremity performance in older men and women. J. Am. Geriatr. Soc. 2000, 48, 381–386. [Google Scholar] [CrossRef] [PubMed]
- Newman, A.B.; Kupelian, V.; Visser, M.; Simonsick, E.M.; Goodpaster, B.H.; Kritchevsky, S.B.; Tylavsky, F.A.; Rubin, S.M.; Harris, T.B. Strength, but not muscle mass, is associated with mortality in the health, aging and body composition study cohort. J. Gerontol. A Biol. Sci. Med. Sci. 2006, 61, 72–77. [Google Scholar] [CrossRef] [PubMed]
- Visser, M.; Goodpaster, B.H.; Kritchevsky, S.B.; Newman, A.B.; Nevitt, M.; Rubin, S.M.; Simonsick, E.M.; Harris, T.B. Muscle mass, muscle strength, and muscle fat infiltration as predictors of incident mobility limitations in well-functioning older persons. J. Gerontol. A Biol. Sci. Med. Sci. 2005, 60, 324–333. [Google Scholar] [CrossRef]
- Soysal, P.; Bulut, E.A.; Yavuz, I.; Isik, A.T. Decreased basal metabolic rate can be an objective marker for sarcopenia and frailty in older males. J. Am. Med. Dir. Assoc. 2019, 20, 58–63. [Google Scholar] [CrossRef]
- Janssen, I.; Ross, R. Linking age-related changes in skeletal muscle mass and composition with metabolism and disease. J. Nutr Health Aging 2005, 9, 408. [Google Scholar]
- Tzankoff, S.; Norris, A. Effect of muscle mass decrease on age-related BMR changes. J. Appl. Physiol. 1977, 43, 1001–1006. [Google Scholar] [CrossRef]
- Clark, B.C.; Manini, T.M. Sarcopenia =/= dynapenia. J. Gerontol. A Biol. Sci. Med. Sci. 2008, 63, 829–834. [Google Scholar] [CrossRef] [PubMed]
- Stavres, J.; Zeigler, M.P.; Pasternostro Bayles, M. Six weeks of moderate functional resistance training increases basal metabolic rate in sedentary adult women. Int. J. Exerc. Sci. 2018, 11, 32–41. [Google Scholar]
- Clark, B.C.; Manini, T.M. What is dynapenia? Nutrition 2012, 28, 495–503. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Stark, T.; Walker, B.; Phillips, J.K.; Fejer, R.; Beck, R. Hand-held dynamometry correlation with the gold standard isokinetic dynamometry: A systematic review. PM&R 2011, 3, 472–479. [Google Scholar]
- Rantanen, T.; Guralnik, J.M.; Foley, D.; Masaki, K.; Leveille, S.; Curb, J.D.; White, L. Midlife hand grip strength as a predictor of old age disability. JAMA 1999, 281, 558–560. [Google Scholar] [CrossRef] [PubMed]
- Korea Centers for Disease Control & Prevention. Available online: http://knhanes.cdc.go.kr (accessed on 8 November 2019).
- Son, D.H.; Yoo, J.W.; Cho, M.R.; Lee, Y.J. Relationship between handgrip strength and pulmonary function in apparently healthy older women. J. Am. Geriatr Soc. 2018, 66, 1367–1371. [Google Scholar] [CrossRef]
- Klein, L. 5-Evaluation of the hand and upper extremity, Fundamentals of Hand therapy, 2nd ed.; Elsevier: Scottsdale, AZ, USA, 2014; pp. 67–86. [Google Scholar]
- Roberts, H.C.; Denison, H.J.; Martin, H.J.; Patel, H.P.; Syddall, H.; Cooper, C.; Sayer, A.A. A review of the measurement of grip strength in clinical and epidemiological studies: Towards a standardised approach. Age Ageing 2011, 40, 423–429. [Google Scholar] [CrossRef]
- Yoo, J.-I.; Choi, H.; Ha, Y.-C. Mean hand grip strength and cut-off value for sarcopenia in Korean adults using KNHANES VI. J. Korean Med. Sci. 2017, 32, 868–872. [Google Scholar] [CrossRef]
- Jo, Y.S.; Choi, S.M.; Lee, J.; Park, Y.S.; Lee, S.-M.; Yim, J.-J.; Yoo, C.-G.; Kim, Y.W.; Han, S.K.; Lee, C.-H. The relationship between chronic obstructive pulmonary disease and comorbidities: A cross-sectional study using data from KNHANES 2010–2012. Respir. Med. 2015, 109, 96–104. [Google Scholar] [CrossRef]
- Camps, S.G.; Wang, N.X.; Tan, W.S.K.; Henry, C.J. Estimation of basal metabolic rate in Chinese: Are the current prediction equations applicable? Nutr. J. 2015, 15, 79. [Google Scholar] [CrossRef]
- Bogardus, C.; Lillioja, S.; Ravussin, E.; Abbott, W.; Zawadzki, J.K.; Young, A.; Knowler, W.C.; Jacobowitz, R.; Moll, P.P. Familial dependence of the resting metabolic rate. NEJM 1986, 315, 96–100. [Google Scholar] [CrossRef] [PubMed]
- Woolcott, O.O.; Bergman, R.N. Relative fat mass (RFM) as a new estimator of whole-body fat percentage—A cross-sectional study in American adult individuals. Sci. Rep. 2018, 8. [Google Scholar] [CrossRef] [PubMed]
- Paek, J.K.; Kim, J.; Kim, K.; Lee, S.Y. Usefulness of relative fat mass in estimating body adiposity in Korean adult population. Endocr. J. 2019. [Google Scholar] [CrossRef] [PubMed]
- Beyer, S.E.; Sanghvi, M.M.; Aung, N.; Hosking, A.; Cooper, J.A.; Paiva, J.M.; Lee, A.M.; Fung, K.; Lukaschuk, E.; Carapella, V. Prospective association between handgrip strength and cardiac structure and function in UK adults. PLoS ONE 2018, 13, e0193124. [Google Scholar] [CrossRef] [PubMed]
- Piaggi, P.; Thearle, M.S.; Bogardus, C.; Krakoff, J. Lower energy expenditure predicts long-term increases in weight and fat mass. J. Clin. Endocrinol. Metab. 2013, 98, E703–E707. [Google Scholar] [CrossRef]
- Roubenoff, R.; Hughes, V.A. Sarcopenia: Current concepts. J. Gerontol. A Biol. Sci. Med. Sci. 2000, 55, 716–724. [Google Scholar] [CrossRef]
- Kim, S.H.; Shin, M.J.; Shin, Y.B.; Kim, K.U. Sarcopenia associated with chronic obstructive pulmonary disease. J. Bone Metab. 2019, 26, 65–74. [Google Scholar] [CrossRef]
- Pisciottano, M.V.C.; Pinto, S.S.; Szejnfeld, V.L.; Castro, C.H. The relationship between lean mass, muscle strength and physical ability in independent healthy elderly women from the community. J. Nutr. Health Aging 2014, 18, 554–558. [Google Scholar] [CrossRef]
- Papadakis, M.A.; Grady, D.; Black, D.; Tierney, M.J.; Gooding, G.A.; Schambelan, M.; Grunfeld, C. Growth hormone replacement in healthy older men improves body composition but not functional ability. Ann. Intern. Med. 1996, 124, 708–716. [Google Scholar] [CrossRef]
- Pratley, R.; Nicklas, B.; Rubin, M.; Miller, J.; Smith, A.; Smith, M.; Hurley, B.; Goldberg, A. Strength training increases resting metabolic rate and norepinephrine levels in healthy 50-to 65-yr-old men. J. Appl. Physiol. 1994, 76, 133–137. [Google Scholar] [CrossRef]
- Perry, C.G.; Lally, J.; Holloway, G.P.; Heigenhauser, G.J.; Bonen, A.; Spriet, L.L. Repeated transient mRNA bursts precede increases in transcriptional and mitochondrial proteins during training in human skeletal muscle. J. Physiol. 2010, 588, 4795–4810. [Google Scholar] [CrossRef] [PubMed]
- Breitenbach, M.; Rinnerthaler, M.; Hartl, J.; Stincone, A.; Vowinckel, J.; Breitenbach-Koller, H.; Ralser, M. Mitochondria in ageing: There is metabolism beyond the ROS. FEMS Yeast Res. 2014, 14, 198–212. [Google Scholar] [CrossRef] [PubMed]
- Frontera, W.R.; Meredith, C.N.; O’Reilly, K.P.; Evans, W.J. Strength training and determinants of VO2max in older men. J. Appl. Physiol. 1990, 68, 329–333. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Xiao, C.M.; Kang, Y.; Zhuang, Y.C. Effects of elastic resistance band exercise on postural balance, estrogen, bone metabolism index, and muscle strength of perimenopausal period women. J. Am. Geriatr. Soc. 2016, 64, 1368–1370. [Google Scholar] [CrossRef] [PubMed]
- Jorgensen, J.O.; Vahl, N.; Dall, R.; Christiansen, J.S. Resting metabolic rate in healthy adults: Relation to growth hormone status and leptin levels. Metabolism 1998, 47, 1134–1139. [Google Scholar] [CrossRef]
- Ferrannini, E. The theoretical bases of indirect calorimetry: A review. Metabolism 1988, 37, 287–301. [Google Scholar] [CrossRef]



{kind=link}
{kind=link}
| Variable | Men (n = 1416) | Women (n = 1096) | p-Value * |
|---|---|---|---|
| Age (years) | 72.1 ± 0.09 | 73.5 ± 0.1 | <0.001 |
| BMI (kg/m2) | 23.6 ± 0.06 | 24.1 ± 0.07 | <0.001 |
| Relative fat mass | 25.3 ± 0.07 | 39.4 ± 0.09 | <0.001 |
| Smoking (%) | 1050 (74.2) | 62 (5.7) | <0.001 |
| Drinking (%) | 432 (30.5) | 53 (4.8) | <0.001 |
| Aerobic physical activity (%) | 578 (45.2) | 276 (29.7) | <0.001 |
| Resistance exercise (%) | 306 (21.6) | 68 (6.2) | <0.001 |
| Household income (%) | <0.001 | ||
| Quartile 1 (lowest) | 562 (40.1) | 567 (52.2) | |
| Quartile 2 | 435 (31.0) | 288 (26.50 | |
| Quartile 3 | 231 (16.5) | 136 (12.5) | |
| Quartile 4 (highest) | 174 (12.4) | 96 (8.8) | |
| Education level (%) | <0.001 | ||
| ≤Elementary school | 508 (39.8) | 703 (74.9) | |
| Middle school | 229 (17.9) | 105 (11.2) | |
| High school | 329 (25.8) | 84 (9.0) | |
| ≥University | 210 (16.5) | 46 (4.9) | |
| Basal metabolic rate (kJ/day) | 6173.8 ± 8.6 | 4875 ± 10.0 | <0.001 |
| Handgrip strength (kg) | 33.6 ± 0.1 | 20.2 ± 0.1 | <0.001 |
| Comorbidity number | 1.3 ± 0.02 | 1.3 ± 0.03 | 0.452 |
| Men Handgrip Strength (kg) | Women Handgrip Strength (kg) | |||||||||
|---|---|---|---|---|---|---|---|---|---|---|
| Variable | Q1 (~29.1) | Q2 (29.2–33.9) | Q3 (34.0–38.1) | Q4 (38.2–59.4) | p-Value for Trend * | Q1 (~16.8) | Q2 (16.9–20.5) | Q3 (20.6–23.8) | Q4 (23.9–37.1) | p-Value for Trend * |
| Unweighted N | 356 | 348 | 358 | 354 | 272 | 276 | 276 | 272 | ||
| Age (years) | 75.3 ± 0.2 | 73.2 ± 0.2 | 71.0 ± 0.2 | 69.4 ± 0.1 | <0.001 | 76.7 ± 0.2 | 73.9 ± 0.2 | 72.4 ± 0.2 | 7.07 ± 0.2 | <0.001 |
| BMI (kg/m2) | 22.8 ± 0.1 | 23.2 ± 0.09 | 23.7 ± 0.1 | 24.7 ± 0.1 | <0.001 | 23.4 ± 0.2 | 24.1 ± 0.2 | 24.2 ± 0.1 | 24.6 ± 0.1 | <0.001 |
| Relative fat mass | 25.0 ± 0.1 | 25.0 ± 0.1 | 25.4 ± 0.1 | 25.7 ± 0.1 | <0.001 | 39.6 ± 0.2 | 39.9 ± 0.2 | 39.1 ± 0.1 | 39.1 ± 0.1 | 0.007 |
| Smoking (%) | 253 (71.0) | 255 (72.4) | 269 (72.4) | 273 (77.6) | 0.022 | 21 (10.0) | 18 (6.5) | 10 (5.1) | 13 (4.6) | <0.001 |
| Drinking (%) | 93 (24.4) | 109 (30.60 | 114 (34.0) | 116 (33.0) | <0.001 | 8 (3.8) | 10 (3.6) | 15 (6.3) | 20 (7.0) | <0.001 |
| Aerobic physical activity (%) | 105 (34.4) | 131 (44.1) | 165 (49.5) | 177 (52.7) | <0.001 | 38 (13.2) | 68 (27.0) | 83 (31.0) | 87 (36.3) | <0.001 |
| Resistance exercise (%) | 40 (10.4) | 52 (16.5) | 100 (27.6) | 114 (33.0) | <0.001 | 4 (1.2) | 14 (4.8) | 27 (11.0) | 23 (7.6) | <0.001 |
| Household income (%) | <0.001 | <0.001 | ||||||||
| Quartile 1 (lowest) | 197 (54.8) | 149 (43.1) | 124 (34.5) | 92 (25.8) | 89 (35.6) | 68 (27.0) | 68 (23.8) | 52 (20.9) | ||
| Quartile 2 | 88 (24.5) | 109 (26.0) | 116 (25.8) | 122 (28.7) | 71 (25.0) | 72 (24.5) | 66 (23.0) | 72 (26.5) | ||
| Quartile 3 | 47 (13.7) | 47 (13.0) | 60 (18.3) | 77 (23.6) | 49 (15.7) | 62 (21.4) | 69 (25.0) | 74 (27.5) | ||
| Quartile 4 (highest) | 22 (7.0) | 36 (10.8) | 56 (17.3) | 60 (15.3) | 61 (23.8) | 70 (27.2) | 73 (28.3) | 71 (26.3) | ||
| Education level (%) | <0.001 | <0.001 | ||||||||
| ≤Elementary school | 170 (55.5) | 140 (47.8) | 108 (30.7) | 90 (28.3) | 182 (90.6) | 189 (78.4) | 170 (66.8) | 162 (68.3) | ||
| Middle school | 48 (16.7) | 56 (16.8) | 54 (15.7) | 71 (20.1) | 13 (4.8) | 20 (8.1) | 29 (12.3) | 43 (17.4) | ||
| High school | 59 (19.1) | 62 (17.7) | 106 (33.9) | 102 (32.8) | 8 (3.5) | 15 (6.0) | 35 (13.2) | 26 (9.9) | ||
| ≥University | 24 (8.7) | 56 (17.7) | 62 (19.7) | 68 (18.8) | 2 (1.1) | 16 (7.4) | 18 (7.7) | 10 (4.4) | ||
| Comorbidity number | 1.2 ± 0.05 | 1.4 ± 0.05 | 1.3 ± 0.05 | 1.2 ± 0.04 | 0.091 | 1.2 ± 0.07 | 1.4 ± 0.06 | 1.4 ± 0.05 | 1.2 ± 0.02 | 0.001 |
| Variable | Univariate | Multivariate (Enter) | Multivariate (Stepwise) | |||
|---|---|---|---|---|---|---|
| BMR | BMR | BMR | ||||
| r or Mean ± SD | p-Value | B (SE) | p-Value | B (SE) | p-Value | |
| Age | −0.255 | <0.001 | −1.6 (1.4) | |||
| BMI | 0.883 | <0.001 | 166.0 (4.0) | <0.001 | 165.8 (4.0) | <0.001 |
| RFM | 0.679 | <0.001 | −21.6 (3.0) | <0.001 | −21.6 (2.9) | <0.001 |
| HGS | 0.396 | <0.001 | 10.9 (1.0) | <0.001 | 11.5 (0.9) | <0.001 |
| Smoking | 0.353 | |||||
| No | 6152.9 ± 492.4 | Ref (0) | ||||
| Yes | 6181.0 ± 498.4 | 25.5 (14.2) | 0.078 | 28.1 (14.1) | 0.047 | |
| Drinking | 0.959 | |||||
| No | 6174.2 ± 504.7 | Ref (0) | ||||
| Yes | 6172.7 ± 479.0 | 12.9 (12.8) | 0.309 | |||
| Aerobic physical activity | 0.124 | |||||
| No | 6167.2 ± 506.8 | Ref (0) | ||||
| Yes | 6209.9 ± 475.9 | −17.4 (12.0) | 0.182 | |||
| Resistance exercise | <0.001 | |||||
| No | 6138.7 ± 495.4 | Ref (0) | ||||
| Yes | 6300.8 ± 481.8 | −12.4 (14.2) | 0.382 | |||
| Household income | <0.001 | |||||
| Quartile 1 (lowest) | 6099.9 ± 499.7 | Ref (0) | ||||
| Quartile 2 | 6156.6 ± 490.1 | −37.1 (14.6) | 0.011 | −34.9 (12.6) | 0.006 | |
| Quartile 3 | 6297.6 ± 474.0 | −7.4 (17.9) | 0.681 | |||
| Quartile 4 (highest) | 6298.4 ± 488.2 | 13.6 (20.7) | 0.509 | |||
| Education level | <0.001 | |||||
| ≤Elementary school | 6103.1 ± 492.2 | Ref (0) | ||||
| Middle school | 6149.6 ± 503.6 | 29.4 (16.9) | 0.082 | |||
| High school | 6241.5 ± 479.1 | 51.3 (15.4) | 0.001 | 39.4 (13.9) | 0.005 | |
| ≥University | 6325.5 ± 472.1 | 87.2 (19.1) | <0.001 | 75.1 (16.6) | <0.001 | |
| Comorbidity number | 0.125 | <0.001 | 10.1 (4.9) | 0.039 | 10.3 (4.9) | 0.035 |
| Variable | Univariate | Multivariate (Enter) | Multivariate (Stepwise) | |||
|---|---|---|---|---|---|---|
| BMR | BMR | BMR | ||||
| r or Mean ± SD | p-Value | B (SE) | p-Value | B (SE) | p-Value | |
| Age | −0.226 | <0.001 | −7.0 (1.5) | <0.001 | −8.0 (1.4) | <0.001 |
| BMI | 0.867 | <0.001 | 128.6 (3.3) | <0.001 | 129.4 (3.3) | <0.001 |
| RFM | 0.594 | <0.001 | −14.5 (2.7) | <0.001 | −15.7 (2.7) | <0.001 |
| HGS | 0.333 | <0.001 | 11.8 (1.4) | <0.001 | 12.2 (1.4) | <0.001 |
| Smoking | 0.449 | |||||
| No | 4878.0 ± 451.8 | Ref (0) | ||||
| Yes | 4832.9 ± 520.0 | −11.7 (29.3) | 0.689 | |||
| Drinking | 0.501 | |||||
| No | 4873.4 ± 452.0 | Ref (0) | ||||
| Yes | 4916.5 ± 527.7 | −3.3 (27.8) | 0.905 | |||
| Aerobic physical activity | 0.739 | |||||
| No | 4884.2 ± 458.7 | Ref (0) | ||||
| Yes | 4873.5 ± 414.7 | 0.6 (14.3) | 0.969 | |||
| Resistance exercise | 0.137 | |||||
| No | 4870.2 ± 459.5 | Ref (0) | ||||
| Yes | 4955.0 ± 389.2 | 18.1 (25.0) | 0.47 | |||
| Household income | 0.088 | |||||
| Quartile 1 (lowest) | 4849.3 ± 469.6 | Ref (0) | ||||
| Quartile 2 | 4878.1 ± 438.9 | 14.0 (15.5) | 0.369 | |||
| Quartile 3 | 4929.6 ± 416.9 | 33.3 (20.6) | 0.106 | |||
| Quartile 4 (highest) | 4952.9 ± 477.8 | 27.6 (23.3) | 0.236 | |||
| Education level | 0.158 | |||||
| ≤Elementary school | 4860.0 ± 452.2 | Ref (0) | ||||
| Middle school | 4952.2 ± 398.9 | 33.7 (21.0) | 0.109 | |||
| High school | 4893.9 ± 423.1 | 22.6 (23.8) | 0.344 | |||
| ≥University | 4943.9 ± 440.9 | 94.2 (30.6) | 0.002 | 94.9 (29.6) | 0.001 | |
| Comorbidity number | 17.2 (5.5) | 0.002 | 18.3 (5.4) | 0.001 | ||
| Model | Male Handgrip Quartile (kg) | ||||
| Q1 (~29.1) | Q2 (29.2~33.9) | Q3 (34.0~38.1) | Q4 (38.2~59.4) | p-Value for Trend | |
| Unadjusted | 5947.5 ± 13.1 | 6090.7 ± 12.5 | 6220.5 ± 16.1 | 6443.5 ± 16.9 | <0.001 |
| Model 1 * | 6077.9 ± 7.9 | 6152.8 ± 6.6 | 6199.4 ± 7.1 | 6280.0 ± 8.4 | <0.001 |
| Model 2 † | 6127.2 ± 13.4 | 6190.0 ± 12.3 | 6233.1 ± 12.9 | 6309.2 ± 13.8 | <0.001 |
| Model | Female Handgrip Quartile (kg) | ||||
| Q1 (~16.8) | Q2 (16.9~20.5) | Q3 (20.6~23.8) | Q4 (23.9~37.1) | p-Value for Trend | |
| Unadjusted | 4683.0 ± 20.3 | 4810.8 ± 21.2 | 4924.9 ± 18.5 | 5072.0 ± 12.1 | <0.001 |
| Model 1 * | 4797.2 ± 8.2 | 4811.2 ± 10.8 | 4895.3 ± 8.7 | 4975.5 ± 6.7 | <0.001 |
| Model 2 † | 4859.9 ± 15.4 | 4848.3 ± 17.8 | 4916.4 ± 13.0 | 5005.1 ± 14.7 | <0.001 |
© 2019 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Oh, S.-K.; Son, D.-H.; Kwon, Y.-J.; Lee, H.S.; Lee, J.-W. Association between Basal Metabolic Rate and Handgrip Strength in Older Koreans. Int. J. Environ. Res. Public Health 2019, 16, 4377. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph16224377
Oh S-K, Son D-H, Kwon Y-J, Lee HS, Lee J-W. Association between Basal Metabolic Rate and Handgrip Strength in Older Koreans. International Journal of Environmental Research and Public Health. 2019; 16(22):4377. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph16224377
Chicago/Turabian StyleOh, Sung-Kwan, Da-Hye Son, Yu-Jin Kwon, Hye Sun Lee, and Ji-Won Lee. 2019. "Association between Basal Metabolic Rate and Handgrip Strength in Older Koreans" International Journal of Environmental Research and Public Health 16, no. 22: 4377. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph16224377