Effect of a Pedometer-Based, 24-Week Walking Intervention on Depression and Acculturative Stress among Migrant Women Workers


Abstract
:1. Introduction
2. Materials and Methods
2.1. Participants
2.2. Walking Adherence
2.3. Depression
2.4. Acculturative Stress
2.5. Intervention
2.5.1. Standard Treatment
2.5.2. Enhanced Treatment
2.6. Data Collection
2.7. Statistical Analyses
3. Results
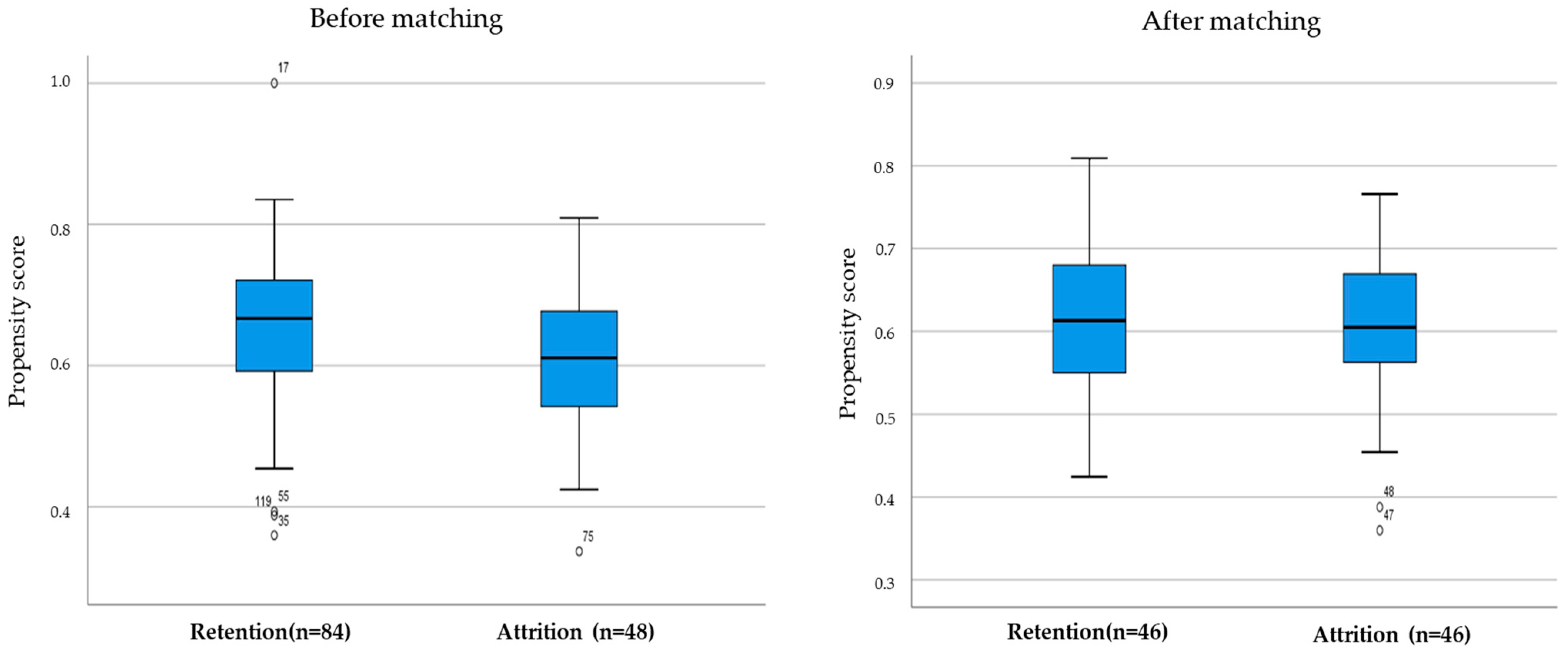
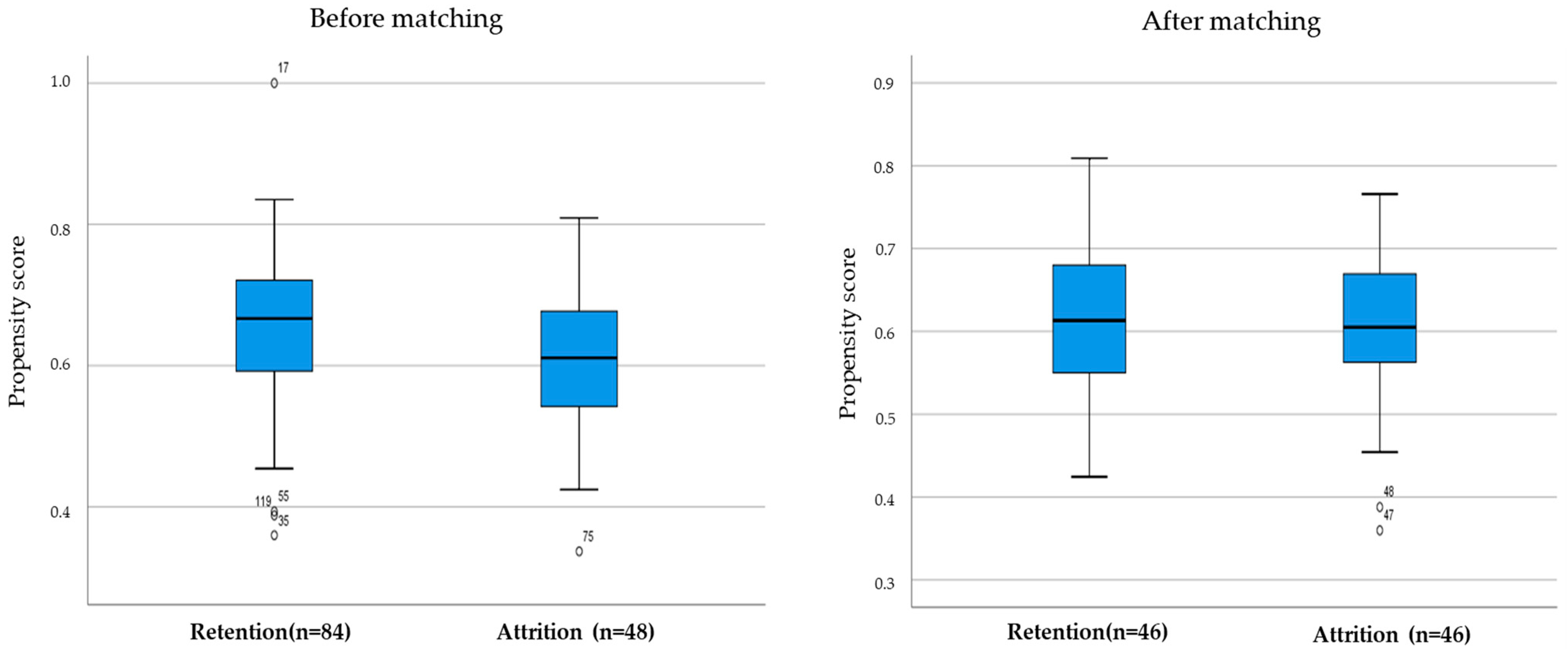
3.1. Participants’ Characteristics and Prospensity Scores Matching
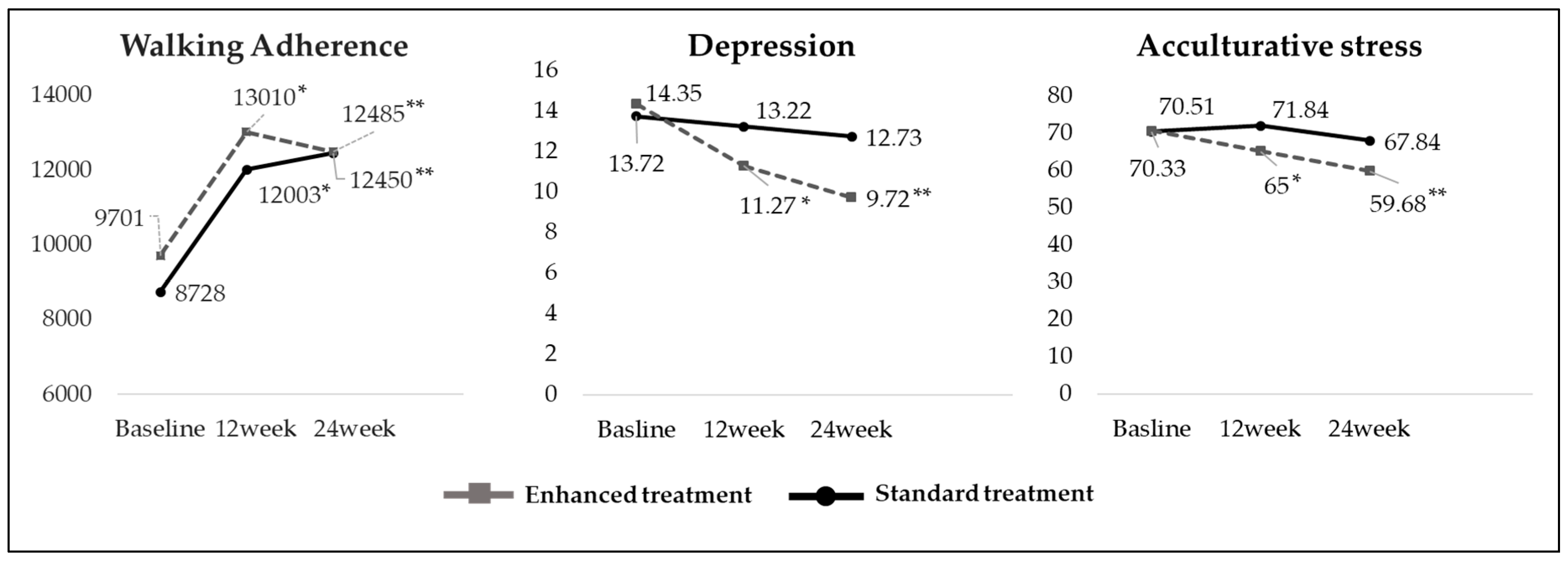
3.2. Walking Adherence, Depression, and Acculturative Stress
3.3. Changes in Depression and Acculturative Stress
4. Discussion
5. Conclusions
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- World Health Organization. Depression and Other Common Mental Disorders. Available online: https://apps.who.int/iris/bitstream/handle/10665/254610/WHO-MSD-MER-2017.2-eng.pdf?sequence=1 (accessed on 8 October 2019).
- World Health Organization. Depression. Available online: https://www.who.int/news-room/fac.sheets/detail/depression (accessed on 10 October 2019).
- Foo, S.; Tam, W.; Ho, C.; Tran, B.; Nguyen, L.; McIntyre, R.; Ho, R. Prevalence of depression among migrants: A systematic review and meta-analysis. Int. J. Environ. Res. Public Health 2018, 15, 1986. [Google Scholar] [CrossRef] [PubMed]
- Bas-Sarmiento, P.; Saucedo-Moreno, M.; Fernández-Gutiérrez, M.; Poza-Méndez, M. Mental health in immigrants versus native population: A systematic review of the literature. Arch. Psychiatr. Nurs. 2017, 31, 111–121. [Google Scholar] [CrossRef] [PubMed]
- Salami, B.; Salma, J.; Hegadoren, K. Access and utilization of mental health services for immigrants and refugees: Perspectives of immigrant service providers. Int. J. Ment. Health Nurs. 2019, 28, 152–161. [Google Scholar] [CrossRef] [PubMed]
- Statistics Korea. Korea Immigration Service Statistics. Available online: http://kosis.kr/statisticsList/statisticsListIndex.do?menuId=M_01_01&vwcd=MT_ZTITLE&parmTabId=M_01_01#SelectStatsBoxDiv (accessed on 20 May 2019).
- Lee, H.; Chae, D.; Cho, S.; Kim, J.; Yoo, R. Influence of a community-based stretching intervention on the health outcomes among Korean-Chinese female migrant workers in South Korea: A randomized prospective trial. Jpn. J. Nurs. Sci. 2017, 14, 277–287. [Google Scholar] [CrossRef] [PubMed]
- Lee, C.; Choi, S. Employment Situations of Chinese of Korean Ethnicity by Residential Status in South Korea; No. 2014-09; IOM Migration Research and Training Centre: Goyang-si, Gyeonggi-do, Korea, 2014. [Google Scholar]
- Lee, H.; Ahn, H.; Miller, A.; Park, C.; Kim, S. Acculturative stress, work-related psychosocial factors and depression in Korean-Chinese migrant workers in Korea. J. Occup. Health 2012, 54, 206–214. [Google Scholar] [CrossRef] [PubMed]
- Abedi, P.; Nikkhah, P.; Najar, S. Effect of pedometer-based walking on depression, anxiety and insomnia among postmenopausal women. Climacteric 2015, 18, 841–845. [Google Scholar] [CrossRef] [PubMed]
- Yuenyongchaiwat, K. Effects of 10,000 steps a day on physical and mental health in overweight participants in a community setting: A preliminary study. Braz. J. Phys. Ther. 2016, 20, 367–373. [Google Scholar] [CrossRef] [PubMed]
- Delavari, M.; Sønderlund, A.; Mellor, D.; Mohebbi, M.; Swinburn, B. Migration, acculturation and environment: Determinants of obesity among Iranian migrants in Australia. Int. J. Environ. Res. Public Health 2015, 12, 1083–1098. [Google Scholar] [CrossRef] [PubMed]
- Hovey, J.D. Acculturative stress, depression, and suicidal ideation in Mexican immigrants. Cult. Divers. Ethn. Minor Psychol. 2000, 6, 134–151. [Google Scholar] [CrossRef] [PubMed]
- Gidengil, E.; Stolle, D. The role of social networks in immigrant women’s political incorporation. Int. Migr. Rev. 2009, 43, 727–763. [Google Scholar] [CrossRef]
- Juarbe, T.; Turok, X.P.; Pérez-Stable, E.J. Perceived benefits and barriers to physical activity among older Latina women. West. J. Nurs. Res. 2002, 24, 868–886. [Google Scholar] [CrossRef] [PubMed]
- Shaghaghi, A.; Bhopal, R.; Sheikh, A. Approaches to recruiting ‘hard-to-reach’ populations into re-search: A review of the literature. Health Promot. Perspect. 2011, 1, 86–94. [Google Scholar] [PubMed]
- Cho, S.; Lee, H.; Kim, J.H.; Lee, M.; Lee, Y.M. Culturally adaptive walking intervention for Korean-Chinese female migrant workers. Res. Theor. Nurs. Pract. 2017, 31, 179–196. [Google Scholar] [CrossRef] [PubMed]
- Thomas, S.; Reading, J.; Shephard, R.J. Revision of the physical activity readiness questionnaire (PAR-Q). Can. J. Sport. Sci. 1992, 17, 338–345. [Google Scholar] [PubMed]
- Lee, H.; Cho, S.; Wilbur, J.; Kim, J.; Park, C.-G.; Lee, Y.-M.; Lee, H. Effects of culturally adaptive walking intervention on cardiovascular disease risks for middle-aged Korean-Chinese female migrant workers. Arch. Environ. Occup. Health 2017, 72, 317–327. [Google Scholar] [CrossRef] [PubMed]
- Cupples, M.; Dean, A.; Tully, M.A.; Taggart, M.; McCorkell, G.; O’Neill, S.; Coates, V. Using pedometer step-count goals to promote physical activity in cardiac rehabilitation: A feasibility study of a controlled trial. Int. J. Phys. Med. Rehabil. 2013, 1, 157. [Google Scholar]
- Wilbur, J.; Zenk, S.; Wang, E.; Oh, A.; McDevitt, J.; Block, D.; McNeil, S.; Ju, S. Neighborhood characteristics, adherence to walking, and depressive symptoms in midlife African American women. J. Women Health 2009, 18, 1201–1210. [Google Scholar] [CrossRef] [PubMed]
- Radloff, L. The CES-D scale: A self-report depression scale for research in the general population. Appl. Psychol. Meas. 1977, 1, 385–401. [Google Scholar] [CrossRef]
- Chon, K.; Lee, M. Development of Korean Version of CES-D: A Preliminary Study. Korean Psychol. Assoc. 1992, 1, 437–445. [Google Scholar]
- Sandhu, D.; Asrabadi, B. Development of an acculturative stress scale for international students: Preliminary findings. Psychol. Rep. 1994, 75, 435–448. [Google Scholar] [CrossRef] [PubMed]
- Yang, O.; Kim, Y. A study on the effects of depression among foreign wives through marriage migration. Ment. Health Soc. Work 2007, 26, 79–110. [Google Scholar]
- Bartholomew, L.K.; Parcel, G.S.; Kok, G. Intervention Mapping: A process for designing theory and evidence-based health education programs. Health Educ. Behav. 1998, 25, 545–563. [Google Scholar] [CrossRef] [PubMed]
- Thompson, W.R.; Gordon, N.F.; Pescatello, L.S. ACSM’s Guidelines for Exercise testing and Prescription, 6th ed.; Lippincott: Philadelphia, PA, USA, 2000. [Google Scholar]
- Tudor-Locke, C.; Bassett, D. How many steps/day are enough? Sports Med. 2004, 34, 1–8. [Google Scholar] [CrossRef] [PubMed]
- Tudor-Locke, C.; Schuna, J.M., Jr. Steps to preventing type 2 diabetes: Exercise, walk more, or sit less? Front. Endocrinol. 2012, 3, 142. [Google Scholar] [CrossRef] [PubMed]
- Gilson, N.D.; Puig-Ribera, A.; McKenna, J.; Brown, W.J.; Burton, N.W.; Cooke, C.B. Do walking strategies to increase physical activity reduce reported sitting in workplaces: A randomized control trial. Int. J. Behav. Nutr. Phys. Act. 2009, 6, 43. [Google Scholar] [CrossRef] [PubMed]
- Butler, C.E.; Clark, B.R.; Burlis, T.L.; Castillo, J.C.; Racette, S.B. Physical activity for campus employees: A university worksite wellness program. J. Phys. Act. Health 2015, 12, 470. [Google Scholar] [CrossRef] [PubMed]
- Berger, V. The reverse propensity score to detect selection bias and correct for baseline imbalances. Stat. Med. 2005, 24, 2777–2787. [Google Scholar] [CrossRef] [PubMed]
- Torres, E.R.; Sampselle, C.M.; Neighbors, H.W.; Ronis, D.L.; Gretebeck, K.A. Depressive symptoms and walking in African-Americans. Public Health Nurs. 2015, 32, 381–387. [Google Scholar] [CrossRef] [PubMed]
- Gawande, R.; To, M.N.; Pine, E.; Griswold, T.; Creedon, T.B.; Brunel, A.; Lozada, A.; Loucks, E.B.; Schuman-Olivier, Z. Mindfulness training enhances self-regulation and facilitates health behavior change for primary care patients: A randomized controlled trial. J. Gen. Intern. Med. 2019, 34, 293–302. [Google Scholar] [CrossRef] [PubMed]
- Kim, Y.; O’Sullivan, D.; Shin, S. Can 24 weeks strength training reduce feelings of depression and increase neurotransmitter in elderly females? Exp. Gerontol. 2019, 115, 62–68. [Google Scholar] [CrossRef] [PubMed]
- Dwyer, T.; Ponsonby, A.L.; Ukoumunne, O.C.; Pezic, A.; Venn, A.; Dunstan, D.; Barr, E.; Blair, S.; Cochrane, J.; Zimmet, P.; et al. Association of change in daily step count over five years with insulin sensitivity and adiposity: Population based cohort study. BMJ 2011, 342, 7249. [Google Scholar] [CrossRef] [PubMed]
- Kaleth, A.; Slaven, J.; Ang, D. Does increasing steps per day predict improvement in physical function and pain interference in adults with fibromyalgia? Arthrit. Care Res. 2014, 66, 1887–1894. [Google Scholar] [CrossRef] [PubMed]
- Rosano, A.; Dauvrin, M.; Buttigieg, S.C.; Ronda, E.; Tafforeau, J.; Dias, S. Migrant’s access to preventive health services in five EU countries. BMC Health Serv. Res. 2017, 17, 588. [Google Scholar] [CrossRef] [PubMed]
- Wieland, M.L.; Weis, J.A.; Yawn, B.P.; Sullivan, S.M.; Millington, K.L.; Smith, C.M.; Bertram, S.; Nigon, J.A.; Sia, I.G. Perceptions of tuberculosis among immigrants and refugees at an adult education center: A community-based participatory research approach. J. Immigr. Minor Health 2012, 14, 14–22. [Google Scholar] [CrossRef] [PubMed]
- Martinez, I.L.; Carter-Pokras, O. Assessing health concerns and barriers in a heterogeneous Latino community. J. Health Care Poor Underserved 2006, 17, 899–909. [Google Scholar] [CrossRef] [PubMed]
- Goodman, J.; Blum, T. Assessing the non-random sampling effects of subject attrition in longitudinal research. J. Manag. 1996, 22, 627–652. [Google Scholar] [CrossRef]
- Huang, L.; Lv, J.; Chen, N.; Liu, Y. Recruitment of older adults into randomized controlled trials: Issues and lessons learned from two community-based exercise interventions in Shanghai. J. Sports Health Sci. 2016, 5, 308–314. [Google Scholar] [CrossRef] [PubMed]
- Bravata, D.M.; Smith-Spangler, C.; Sundaram, V.; Gienger, A.L.; Lin, N.; Lewis, R.; Stave, C.D.; Olkin, I.; Sirard, J.R.J.J. Using pedometers to increase physical activity and improve health: A systematic review. JAMA 2007, 298, 2296–2304. [Google Scholar] [CrossRef] [PubMed]
- Eom, S.O.; Lee, I.J.J. The Effect of Health Coaching Programs on Self-Efficacy, Health Behaviors, and Quality of Life in Hypertensive People Living in Poverty. J. Korean Acad. Nurs. 2017, 47, 380–391. [Google Scholar] [CrossRef] [PubMed]


{kind=link}
{kind=link}
| Variable | Total | ST Group (n = 69) | ET Group (n = 63) | |||
|---|---|---|---|---|---|---|
| n (%)/M(SD) | n (%)/ M(SD) | n (%)/ M(SD) | x2 | t | p | |
| Age | 54.60 (5.09) | 56.20 (5.46) | 56.62 (4.69) | 0.47 | 0.639 | |
| Duration of stay (months) | 102.90 (68.08) | 81.41 (49.18) | 126.44 (77.86) | 4.01 | <0.001 | |
| Duration of current job (months) | 57.44 (49.46) | 54.06 (40.40) | 61.08 (57.80) | 0.81 | 0.419 | |
| Working time(h/day) | 12.45 (4.03) | 11.71 (3.17) | 13.24 (4.69) | 2.20 | 0.030 | |
| Income (USD/month) | 1322.13 (269.36) | 1312.54 (147.87) | 1332.64 (359.31) | 0.43 | 0.670 | |
| Education | ||||||
| ≥High school | 81 (61.8) | 40 (58.0) | 41 (65.1) | 0.702 | 0.402 | |
| Type of job | ||||||
| Housekeeper | 106 (80.3) | 58 (84.1) | 48 (76.2) | 1.443 | 0.486 | |
| Waitress | 13 (9.8) | 5 (7.2) | 8 (12.7) | |||
| Others | 13 (9.8) | 6 (8.7) | 7 (11.1) | |||
| Chronic disease | ||||||
| None | 63 (47.7) | 32 (46.4) | 31 (49.2) | 0.106 | 0.745 | |
| Walking(steps/day) | 9,193 (3212) | 8,728 (2,977) | 9,701 (3,875) | 1.65 | 0.102 | |
| Depression | 13.02 ( 8.68 ) | 13.72 (7.12) | 14.35 (10.17) | 0.41 | 0.681 | |
| Acculturative stress | 70.42 (21.37) | 70.33 (19.10) | 70.51 (23.77) | 0.05 | 0.963 |
| Outcome | B | SE | t | p |
|---|---|---|---|---|
| Depression | ||||
| Steps/day (per 1000 steps) | −0.308 | 0.121 | −2.545 | 0.012 |
| ET (reference: ST) | 0.701 | 1.551 | 0.452 | 0.652 |
| Week 12 (reference: Baseline) | 0.493 | 1.087 | 0.453 | 0.651 |
| Week 24 (reference: Baseline) | −0.124 | 1.041 | −0.119 | 0.906 |
| ET*Week 12 | −3.149 | 1.444 | −2.180 | 0.031 |
| ET*Week 24 | −3.104 | 1.380 | −2.249 | 0.027 |
| Acculturative stress | ||||
| Steps/day (per 1000 steps) | −0.748 | 0.330 | −2.266 | 0.024 |
| ET (reference: ST) | −1.255 | 3.894 | −0.322 | 0.748 |
| Week 12 (reference: Baseline) | 4.119 | 3.132 | 1.315 | 0.190 |
| Week 24 (reference: Baseline) | 1.661 | 2.728 | 0.609 | 0.543 |
| ET*Week 12 | −8.679 | 4.202 | −2.066 | 0.040 |
| ET*Week 24 | −7.178 | 3.612 | −1.987 | 0.049 |
© 2019 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Kim, Y.; Lee, Y.-M.; Cho, M.; Lee, H. Effect of a Pedometer-Based, 24-Week Walking Intervention on Depression and Acculturative Stress among Migrant Women Workers. Int. J. Environ. Res. Public Health 2019, 16, 4385. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph16224385
Kim Y, Lee Y-M, Cho M, Lee H. Effect of a Pedometer-Based, 24-Week Walking Intervention on Depression and Acculturative Stress among Migrant Women Workers. International Journal of Environmental Research and Public Health. 2019; 16(22):4385. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph16224385
Chicago/Turabian StyleKim, Youlim, Young-Me Lee, Mikyeong Cho, and Hyeonkyeong Lee. 2019. "Effect of a Pedometer-Based, 24-Week Walking Intervention on Depression and Acculturative Stress among Migrant Women Workers" International Journal of Environmental Research and Public Health 16, no. 22: 4385. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph16224385