Spatiotemporal Distribution of Tuberculosis during Urbanization in the New Urban Area of Nanchang City, China, 2010–2018


Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Area
2.2. Data Collection
2.3. Data Analysis
3. Results
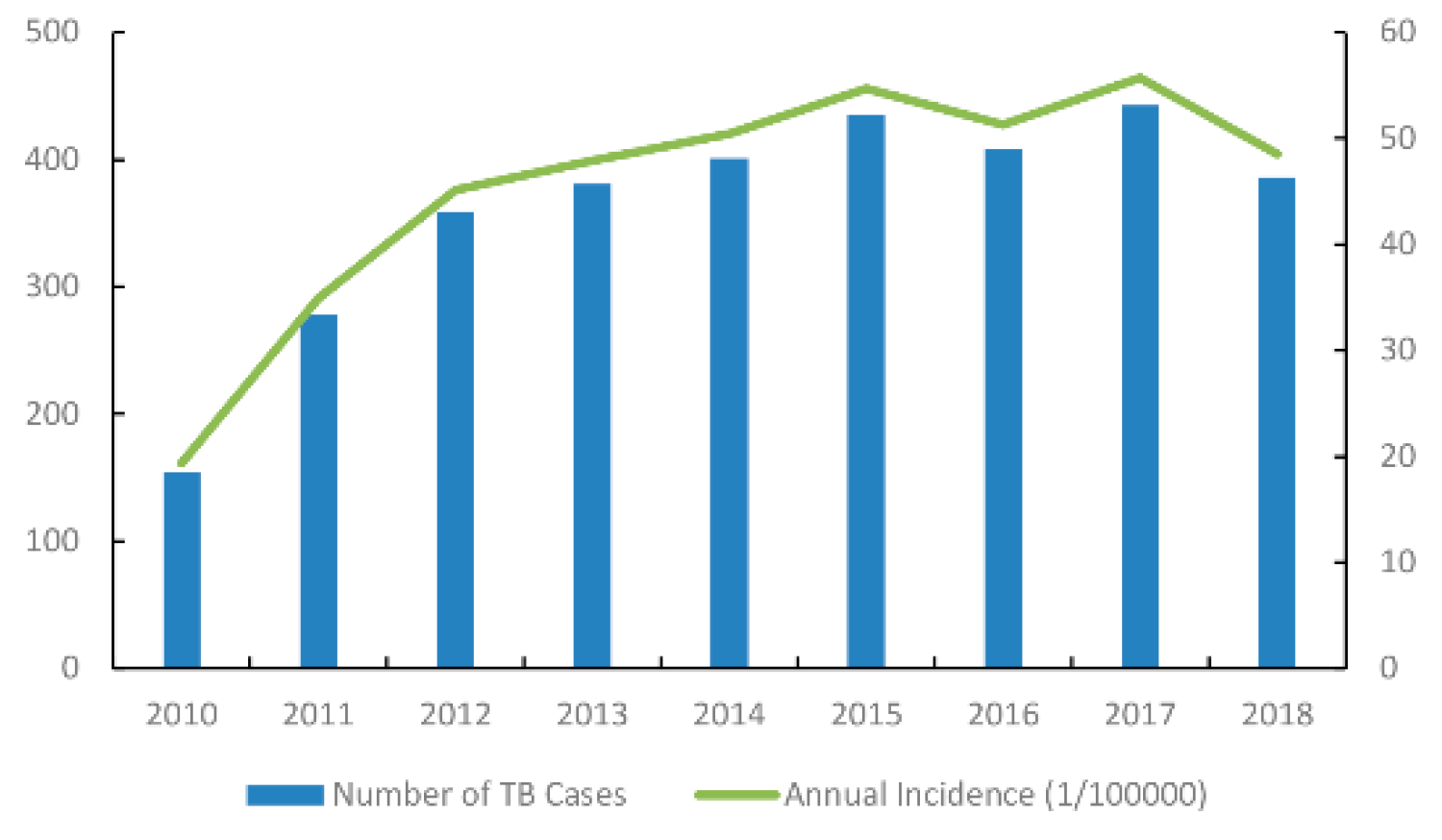
3.1. Descriptive Statistics
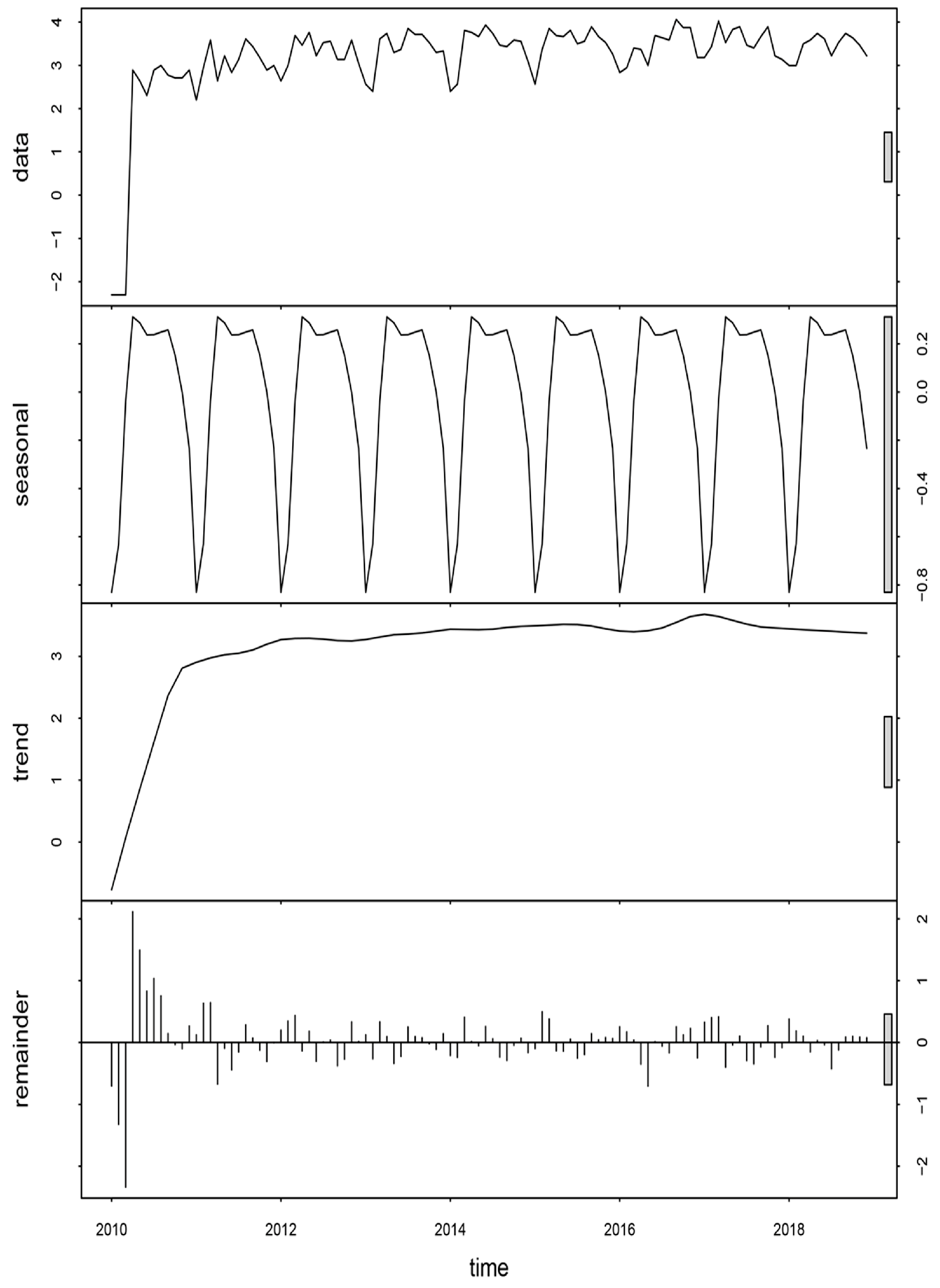
3.2. Seasonal Decomposition Analyses
3.3. Spatiotemporal Analysis
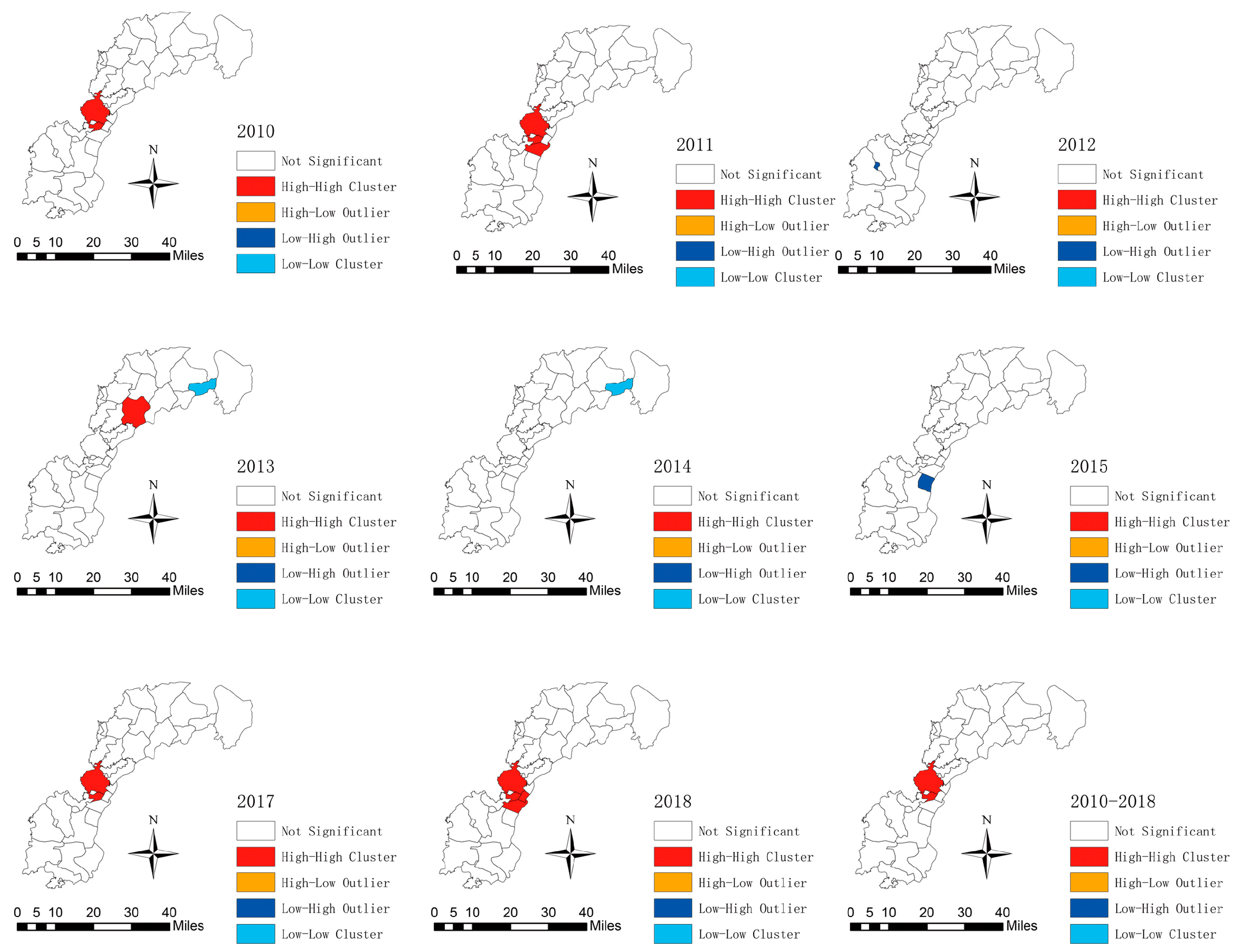
3.3.1. Spatial Autocorrelation Analysis
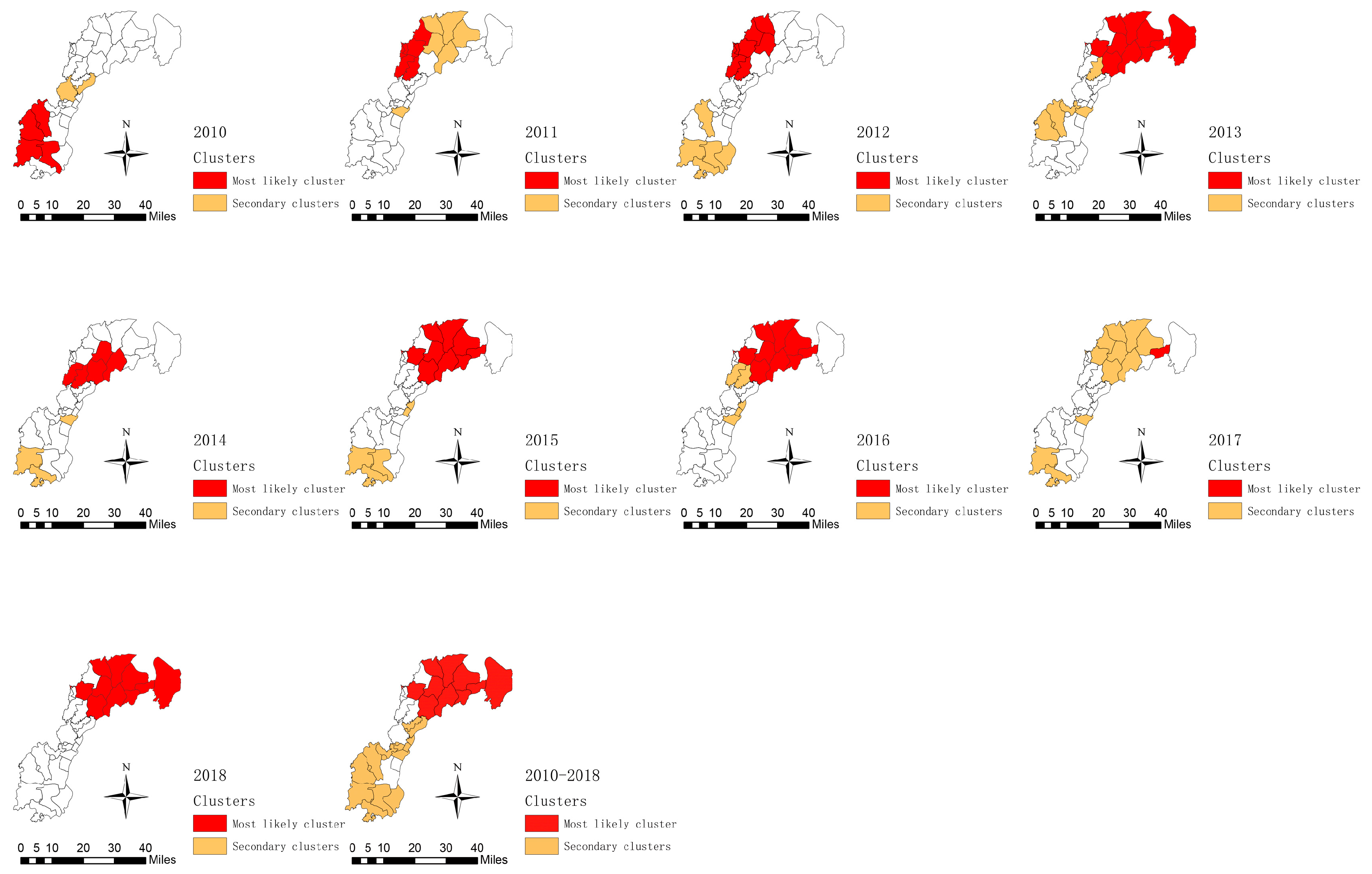
3.3.2. Spatiotemporal Cluster Analysis
4. Discussion
5. Conclusions
Availability of Data and Materials
Ethics Statement
Author Contributions
Acknowledgments
Conflicts of Interest
References
- Tuite, A.R.; Guthrie, J.L.; Alexander, D.C.; Whelan, M.S.; Lee, B.; Lam, K.; Ma, J.; Fisman, D.N.; Jamieson, F.B. Epidemiological evaluation of spatiotemporal and genotypic clustering of Mycobacterium tuberculosis in Ontario, Canada. Int. J. Tuberc. Lung Dis. 2013, 17, 1322–1327. [Google Scholar] [CrossRef] [PubMed]
- Espindola, A.L.; Varughese, M.; Laskowski, M.; Shoukat, A.; Heffernan, J.M.; Moghadas, S.M. Strategies for halting the rise of multidrug resistant TB epidemics: Assessing the effect of early case detection and isolation. Int. Health 2017, 9, 80–90. [Google Scholar] [CrossRef] [PubMed]
- Glaziou, P.; Floyd, K.; Raviglione, M.C. Global Epidemiology of Tuberculosis. Semin. Respir. Crit. Care Med. 2018, 39, 271–285. [Google Scholar] [CrossRef] [PubMed]
- The National Overview of Notifiable Infectious Disease in 2018. Chinese Ministry of Health. Available online: http://www.nhc.gov.cn/jkj/s3578/201904/050427ff32704a5db64f4ae1f6d57c6c.shtml (accessed on 11 September 2019).
- Shi, Q.N.; Ma, J.Q. Big data analysis of tuberculosis dynamic surveillance in China. Chin. J. Health Inf. Manag. 2017, 14, 643–648. [Google Scholar]
- Michishita, R. Monitoring two decades of urbanization in the Poyang Lake area, China through spectral unmixing. Remote Sens. Environ. 2012, 117, 3–18. [Google Scholar] [CrossRef]
- Wang, T.; Xue, F.; Chen, Y.; Ma, Y.; Liu, Y. The spatial epidemiology of tuberculosis in Linyi City, China, 2005–2010. BMC Public Health 2012, 12, 885. [Google Scholar] [CrossRef]
- Shochat, E.; Warren, P.S.; Faeth, S.H.; McIntyre, N.E.; Hope, D. From patterns to emerging processes in mechanistic urban ecology. Trends Ecol. Evol. 2006, 21, 186–191. [Google Scholar] [CrossRef]
- Jia, Z.W.; Jia, X.W.; Liu, Y.X.; Dye, C.; Chen, F.; Chen, C.S.; Zhang, W.Y.; Li, X.W.; Cao, W.C.; Liu, H.L. Spatial analysis of tuberculosis cases in migrants and permanent residents, Beijing, 2000–2006. Emerg. Infect. Dis. 2008, 14, 1413–1419. [Google Scholar] [CrossRef]
- Wong, D.F.K.; Li, C.Y.; Song, H.X. Rural migrant workers in urban China: Living a marginalised life. Int. J. Soc. Welf. 2007, 16, 32–40. [Google Scholar] [CrossRef]
- Prasad, A.; Ross, A.; Rosenberg, P.; Dye, C. A world of cities and the end of TB. Trans. R. Soc. Trop. Med. Hyg. 2016, 110, 151–152. [Google Scholar] [CrossRef] [Green Version]
- Yue, Y.; Sun, J.; Liu, X.; Ren, D.; Liu, Q.; Xiao, X.; Lu, L. Spatial analysis of dengue fever and exploration of its environmental and socio-economic risk factors using ordinary least squares: A case study in five districts of Guangzhou City, China, 2014. Int. J. Infect. Dis. 2018, 75, 39–48. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Zhang, W.Y.; Wang, L.Y.; Liu, Y.X.; Yin, W.W.; Hu, W.B.; Magalhaes, R.J.; Ding, F.; Sun, H.L.; Zhou, H.; Li, S.L.; et al. Spatiotemporal transmission dynamics of hemorrhagic fever with renal syndrome in China, 2005–2012. PLoS Negl. Trop. Dis. 2014, 8, e3344. [Google Scholar] [CrossRef] [PubMed]
- Liu, M.Y.; Li, Q.H.; Zhang, Y.J.; Ma, Y.; Liu, Y.; Feng, W.; Hou, C.B.; Amsalu, E.; Li, X.; Wang, W.; et al. Spatial and temporal clustering analysis of tuberculosis in the mainland of China at the prefecture level, 2005–2015. Infect. Dis. Poverty 2018, 7, 106. [Google Scholar] [CrossRef] [PubMed]
- Sun, J.; Lu, L.; Wu, H.; Yang, J.; Liu, K.; Liu, Q. Spatiotemporal patterns of severe fever with thrombocytopenia syndrome in China, 2011–2016. Ticks Tick-Borne Dis. 2018, 9, 927–933. [Google Scholar] [CrossRef]
- Wang, L.Y.; Zhang, W.Y.; Ding, F.; Hu, W.B.; Magalhaes, R.J.S.; Sun, H.L.; Li, Y.X.; Zou, W.; Wang, Y.; Liu, Q.Y.; et al. Spatiotemporal patterns of Japanese encephalitis in China, 2002–2010. PLoS Negl. Trop. Dis. 2013, 7, e2285. [Google Scholar] [CrossRef]
- Zhang, Y.; Liu, Q.Y.; Luan, R.S.; Liu, X.B.; Zhou, G.C.; Jiang, J.Y.; Li, H.S.; Li, Z.F. Spatial-temporal analysis of malaria and the effect of environmental factors on its incidence in Yongcheng, China, 2006–2010. BMC Public Health 2012, 12, 544. [Google Scholar] [CrossRef]
- Rao, H.X.; Zhang, X.; Zhao, L.; Yu, J.; Ren, W.; Zhang, X.L.; Ma, Y.C.; Shi, Y.; Ma, B.Z.; Wang, X.; et al. Spatial transmission and meteorological determinants of tuberculosis incidence in Qinghai Province, China: A spatial clustering panel analysis. Infect. Dis. Poverty 2016, 5, 45. [Google Scholar] [CrossRef]
- Rao, H.; Shi, X.; Zhang, X. Using the Kulldorff’s scan statistical analysis to detect spatio-temporal clusters of tuberculosis in Qinghai Province, China, 2009–2016. BMC Infect. Dis. 2017, 17, 578. [Google Scholar] [CrossRef]
- He, X.; Cao, M.; Mahapatra, T.; Du, X.; Mahapatra, S.; Li, Q.; Feng, L.; Tang, S.; Zhao, Z.; Liu, J.; et al. Burden of tuberculosis in Xinjiang between 2011 and 2015: A surveillance data-based study. PLoS ONE 2017, 12, e0187592. [Google Scholar] [CrossRef]
- The Government of Honggutan New District. Nanchang, China. Available online: http://hgt.nc.gov.cn/mlhgt/index.jhtml (accessed on 11 September 2019).
- The Xinjian County People’s Government. Nanchang, China. Available online: http://www.xinjian.gov.cn/Category_109/Index.aspx (accessed on 11 September 2019).
- Resource and Environment Data Cloud Platform. Institute of Geographic Sciences and Natural Resources Research. Available online: http://www.resdc.cn/ (accessed on 1 September 2019).
- The R Project for Statistical Computing. Auckland, New Zealand. Available online: https://www.r-project.org/. (accessed on 1 September 2019).
- Software for the Spatial, Temporal, and Space-Time Scan Statistics. Harvard Medical School and Harvard Pilgrim Health Care Institute. Available online: https://www.satscan.org/ (accessed on 1 September 2019).
- Acharya, B.K.; Cao, C.; Lakes, T.; Chen, W.; Naeem, S. Spatiotemporal analysis of dengue fever in Nepal from 2010 to 2014. BMC Public Health 2016, 16, 849. [Google Scholar] [CrossRef]
- Tang, X.; Geater, A.; McNeil, E.; Deng, Q.; Dong, A.; Zhong, G. Spatial, temporal and spatio-temporal clusters of measles incidence at the county level in Guangxi, China during 2004–2014: Flexibly shaped scan statistics. BMC Infect. Dis. 2017, 17, 243. [Google Scholar] [CrossRef] [PubMed]
- Kulldorff, M.; Song, C.; Gregorio, D.; Samociuk, H.; DeChello, L. Cancer map patterns: Are they random or not? Am. J. Prev. Med. 2006, 30, S37–S49. [Google Scholar] [CrossRef] [PubMed]
- Ribeiro, F.K.; Pan, W.; Bertolde, A.; Vinhas, S.A.; Peres, R.L.; Riley, L.; Palaci, M.; Maciel, E.L. Genotypic and Spatial Analysis of Mycobacterium tuberculosis Transmission in a High-Incidence Urban Setting. Clin. Infect. Dis. 2015, 61, 758–766. [Google Scholar] [CrossRef] [PubMed]
- Gong, P.; Liang, S.; Carlton, E.J.; Jiang, Q.; Wu, J.; Wang, L.; Remais, J.V. Urbanisation and health in China. Lancet 2012, 379, 843–852. [Google Scholar] [CrossRef]
- Xie, C.; Xu, L.; Wang, X.; Xiong, Z.; Song, L. Epidemiological characteristics and spatial-temporal clustering analysis on pulmonary tuberculosis in Changsha from 2013 to 2016. Zhong Nan Da Xue Xue Bao Yi Xue Ban 2018, 43, 898–903. [Google Scholar] [CrossRef]
- Li, X.; Yang, Q.; Feng, B.; Xin, H.; Zhang, M.; Deng, Q.; Deng, G.; Shan, W.; Yue, J.; Zhang, H.; et al. Tuberculosis infection in rural labor migrants in Shenzhen, China: Emerging challenge to tuberculosis control during urbanization. Sci. Rep. 2017, 7, 4457. [Google Scholar] [CrossRef]
- Wu, B.; Yu, Y.; Xie, W.; Liu, Y.; Zhang, Y.; Hu, D.; Li, Y. Epidemiology of tuberculosis in Chongqing, China: A secular trend from 1992 to 2015. Sci. Rep. 2017, 7, 7832. [Google Scholar] [CrossRef]
- Wei, X.; Zou, G.; Yin, J.; Walley, J.; Yang, H.; Kliner, M.; Mei, J. Providing financial incentives to rural-to-urban tuberculosis migrants in Shanghai: An intervention study. Infect. Dis. Poverty 2012, 1, 9. [Google Scholar] [CrossRef]
- Kodmon, C.; Zucs, P.; van der Werf, M.J. Migration-related tuberculosis: Epidemiology and characteristics of tuberculosis cases originating outside the European Union and European Economic Area, 2007 to 2013. Eurosurveillance 2016, 21. [Google Scholar] [CrossRef]
- Davies, P.D. The effects of poverty and ageing on the increase in tuberculosis. Monaldi Arch. Chest Dis. 1999, 54, 168–171. [Google Scholar]
- Noppert, G.A.; Clarke, P. The Modern Profile of Tuberculosis: Developing the TB Social Survey to understand contemporary social patterns in tuberculosis. Public Health Nurs. 2018, 35, 48–55. [Google Scholar] [CrossRef] [PubMed]
- Top, R.; Boshuizen, H.; Dekkers, A.; Altes, H.K. Similar seasonal peak in clustered and unique extra-pulmonary tuberculosis notifications: Winter crowding hypothesis ruled out? Int. J. Tuberc. Lung Dis. 2013, 17, 1466–1471. [Google Scholar] [CrossRef] [PubMed]
- Ma, M.J.; Yang, Y.; Wang, H.B.; Zhu, Y.F.; Fang, L.Q.; An, X.P.; Wan, K.L.; Whalen, C.C.; Yang, X.X.; Lauzardo, M.; et al. Transmissibility of tuberculosis among school contacts: An outbreak investigation in a boarding middle school, China. Infect. Genet. Evol. 2015, 32, 148–155. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Fang, Y.; Zhang, L.; Tu, C.; Ye, D.; Fontaine, R.; Ma, H.; Hao, J.; Fu, L.; Ying, X.; Chen, Q.; et al. Outbreak of pulmonary tuberculosis in a Chinese high school, 2009–2010. J. Epidemiol. 2013, 23, 307–312. [Google Scholar] [CrossRef]
- Chen, W.; Xia, Y.; Li, X.; Zhou, L.; Li, C.; Wan, K.; Cheng, S. A tuberculosis outbreak among senior high school students in China in 2011. J. Int. Med. Res. 2012, 40, 1830–1839. [Google Scholar] [CrossRef]
- Wang, J.F.; Xu, C.D. Geodectecter: Principle and procpective. Acta Geogr. Sin. 2017, 27, 116–134. [Google Scholar]
- Liu, Y.; Rao, K.; Wu, J.; Gakidou, E. China’s health system performance. Lancet 2008, 372, 1914–1923. [Google Scholar] [CrossRef]
- Alirol, E.; Getaz, L.; Stoll, B.; Chappuis, F.; Loutan, L. Urbanisation and infectious diseases in a globalised world. Lancet 2011, 11, 131–141. [Google Scholar] [CrossRef]







{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Variable | 2010 | 2011 | 2012 | 2013 | 2014 | 2015 | 2016 | 2017 | 2018 | Total |
|---|---|---|---|---|---|---|---|---|---|---|
| Gender | ||||||||||
| Male | 122(79.2) | 197(70.9) | 268(74.7) | 295(77.4) | 288(71.8) | 322(74.0) | 288(70.6) | 318(71.8) | 277(71.8) | 2375(73.2) |
| Female | 32(20.8) | 81(29.1) | 91(25.3) | 86(22.6) | 113(28.2) | 113(26.0) | 120(29.4) | 125(28.2) | 109(28.2) | 870(26.8) |
| Age group | ||||||||||
| 0–20 | 23(14.9) | 23(8.3) | 27(7.5) | 29(7.6) | 26(6.5) | 38(8.7) | 36(8.8) | 31(7.0) | 32(8.3) | 265(8.2) |
| 20–40 | 59(38.3) | 88(31.7) | 72(20.1) | 82(21.5) | 98(24.4) | 86(19.8) | 87(21.3) | 104(23.5) | 98(25.4) | 774(23.9) |
| 40–60 | 28(18.2) | 74(26.6) | 122(34.0) | 109(28.6) | 117(29.2) | 138(31.7) | 107(26.2) | 119(26.9) | 82(21.2) | 896(27.6) |
| >60 | 44(28.6) | 93(33.5) | 138(38.4) | 161(42.3) | 160(39.9) | 173(39.8) | 178(43.6) | 189(42.7) | 174(45.1) | 1310(40.4) |
| Occupation | ||||||||||
| Farmers | 48(31.2) | 133(47.8) | 229(63.8) | 244(64.0) | 268(66.8) | 260(59.8) | 237(58.1) | 238(53.7) | 181(46.9) | 1838(56.6) |
| Students | 38(24.7) | 35(12.6) | 28(7.8) | 30(7.9) | 36(9.0) | 40(9.2) | 44(10.8) | 39(8.8) | 42(10.9) | 332(10.2) |
| Unemployed | 11(7.1) | 22(7.9) | 24(6.7) | 33(8.7) | 24(6.0) | 38(8.7) | 30(7.4) | 56(12.6) | 55(14.2) | 293(9.0) |
| Retired | 13(8.4) | 21(7.6) | 19(5.3) | 27(7.1) | 23(5.7) | 24(5.5) | 26(6.4) | 23(5.2) | 24(6.2) | 200(6.2) |
| Criminals | 12(7.8) | 0(0.0) | 0(0.0) | 1(0.3) | 1(0.2) | 9(2.1) | 22(5.4) | 29(6.5) | 23(6.0) | 85(2.6) |
| Workers | 12(7.8) | 14(5.0) | 6(1.7) | 2(0.5) | 6(1.5) | 7(1.6) | 10(2.5) | 6(1.4) | 3(0.8) | 66(2.0) |
| Others | 29(18.8) | 50(18.0) | 42(11.7) | 31(8.1) | 18(4.5) | 16(3.7) | 22(5.4) | 20(4.5) | 27(7.0) | 255(7.9) |
| Unknown | 3(1.9) | 3(1.1) | 11(3.1) | 13(3.4) | 25(6.2) | 41(9.4) | 17(4.2) | 32(7.2) | 31(8.0) | 176(5.4) |
| Diagnosis | ||||||||||
| Sputum smear-positive (SS+) TB | 27(17.5) | 122(43.9) | 232(64.6) | 235(61.7) | 251(62.6) | 261(60.0) | 245(60.0) | 241(54.4) | 175(45.3) | 1789(55.1) |
| Sputum smear-negative(SS-)TB | 101(65.5) | 114(41.0) | 44(12.3) | 45(11.8) | 69(17.2) | 82(18.9) | 79(19.4) | 99(22.3) | 118(30.6) | 751(23.1) |
| Sputum smear not done | 5(3.2) | 1(0.4) | 0(0.0) | 2(0.5) | 2(0.5) | 2(0.5) | 6(1.6) | 20(4.5) | 16(4.1) | 54(1.7) |
| Tuberculosis Type | ||||||||||
| Tuberculosis pleurisy cases | 15(9.7) | 21(7.6) | 28(7.8) | 30(7.9) | 22(5.5) | 26(6.0) | 22(5.4) | 33(7.4) | 16(4.1) | 213(6.6) |
| Other diseases | 6(3.9) | 20(7.2) | 55(15.3) | 69(18.1) | 56(14.0) | 64(14.7) | 56(13.7) | 46(10.4) | 53(13.7) | 425(13.1) |
| Clusters | Longitude (E) | Latitude (N) | Radius (km) | Time Frame | Population | No. Counties | Annual Cases/100,000 | Observed/Expected | LLR | RR |
|---|---|---|---|---|---|---|---|---|---|---|
| 1 | 116.37 | 28.95 | 43.74 | 3/1/2015–10/31/2017 | 185,214 | 10 | 66.3 | 2.45 | 106.02 | 2.61 |
| 2 | 115.84 | 28.67 | 0 | 6/1/2011–9/30/2013 | 183,246 | 1 | 6.8 | 0.25 | 47.85 | 0.24 |
| 3 | 115.86 | 28.77 | 0.74 | 8/1/2011–2/28/2014 | 831,09 | 2 | 2.3 | 0.086 | 41.24 | 0.085 |
| 4 | 115.88 | 28.72 | 3.04 | 1/1/2010–8/31/2012 | 148,000 | 2 | 8.1 | 0.3 | 37.12 | 0.29 |
| 5 | 115.68 | 28.39 | 14.57 | 2/1/2015–9/30/2017 | 166,248 | 4 | 49.4 | 1.83 | 34.5 | 1.89 |
| 6 | 115.81 | 28.68 | 0 | 6/1/2015–12/31/2017 | 21,862 | 1 | 90.2 | 3.33 | 25.89 | 3.37 |
| 7 | 115.83 | 28.7 | 2.43 | 1/1/2010–5/31/2010 | 144,047 | 2 | 0 | 0 | 16.15 | 0 |
| 8 | 115.66 | 28.58 | 4.02 | 9/1/2016–11/30/2018 | 81,779 | 3 | 51.1 | 1.89 | 15.88 | 1.92 |
| 9 | 115.81 | 28.62 | 5.03 | 1/1/2010–7/31/2012 | 76,100 | 2 | 9.7 | 0.36 | 14.8 | 0.35 |
© 2019 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Yang, S.; Gao, Y.; Luo, W.; Liu, L.; Lei, Y.; Zhang, X. Spatiotemporal Distribution of Tuberculosis during Urbanization in the New Urban Area of Nanchang City, China, 2010–2018. Int. J. Environ. Res. Public Health 2019, 16, 4395. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph16224395
Yang S, Gao Y, Luo W, Liu L, Lei Y, Zhang X. Spatiotemporal Distribution of Tuberculosis during Urbanization in the New Urban Area of Nanchang City, China, 2010–2018. International Journal of Environmental Research and Public Health. 2019; 16(22):4395. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph16224395
Chicago/Turabian StyleYang, Shu, Yuan Gao, Wei Luo, Longfu Liu, Yuanhua Lei, and Xiaoling Zhang. 2019. "Spatiotemporal Distribution of Tuberculosis during Urbanization in the New Urban Area of Nanchang City, China, 2010–2018" International Journal of Environmental Research and Public Health 16, no. 22: 4395. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph16224395