Wetlands for Wellbeing: Piloting a Nature-Based Health Intervention for the Management of Anxiety and Depression

 ,
,
Abstract
:1. Introduction
2. Materials and Methods
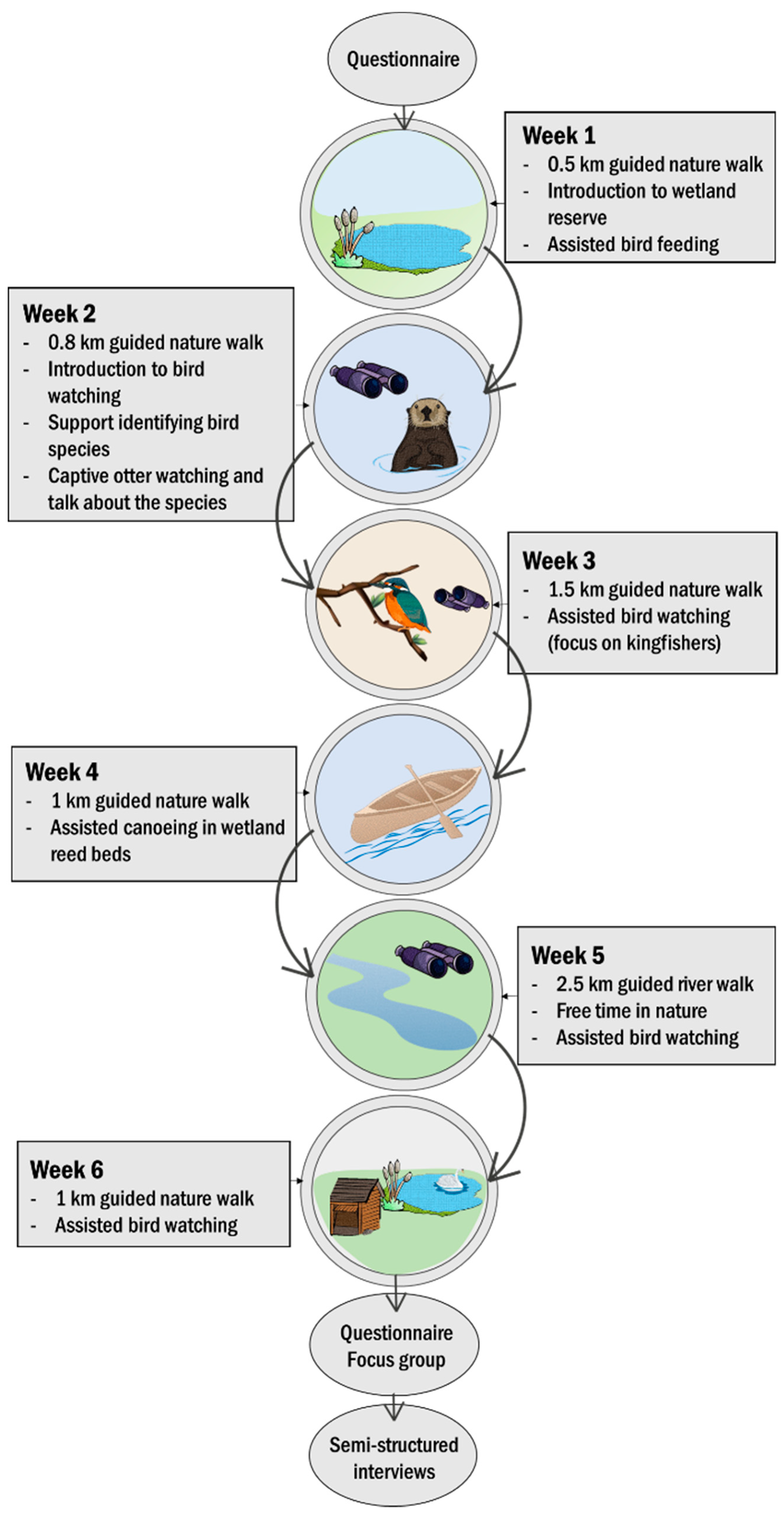
2.1. Wetland NBI Design
2.2. Participant Recruitment
2.3. Questionnaire
2.4. Focus Groups and Interviews
2.5. Statistical Analyses
3. Results
3.1. Participants
3.2. Wetland NBI Mental Health Outcomes
3.2.1. Reducing Symptoms of Anxiety and Depression
3.2.2. Contribution to Long-Term Symptom Management
3.3. Additional Associated Wetland NBI Outcomes
3.3.1. Reducing Social Isolation
3.3.2. Increasing Confidence to be in Nature
3.3.3. Improving Physical Health Management
3.4. The Role of the Natural Environment in Facilitating Wetland NBI Outcomes
3.5. The Role of the Wetland NBI Design in Delivering Outcomes
3.5.1. Provision of Transportation
3.5.2. Engagement of NBI Staff
3.5.3. Session Content
3.5.4. Group Dynamics
4. Discussion
4.1. Wetland NBI Outcomes
4.2. Explanatory Pathways Underpinning the Outcomes
4.3. Importance of NBI Design
4.4. Valuing the Impact of the Wetland NBI
4.5. Limitations of the Wetland NBI Pilot
5. Conclusions
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- World Health Organization. Motion for Your Mind: Physical Activity for Mental Health Promotion, Protection and Care. Available online: http://www.euro.who.int/__data/assets/pdf_file/0018/403182/WHO-Motion-for-your-mind-ENG.pdf?ua=1 (accessed on 14 October 2019).
- Foreman, K.J.; Marquez, N.; Dolgert, A.; Fukutaki, K.; Fullman, N.; McGaughey, M.; Pletcher, M.A.; Smith, A.E.; Tang, K.; Yuan, C.-W.; et al. Forecasting life expectancy, years of life lost, and all-cause and cause-specific mortality for 250 causes of death: Reference and alternative scenarios for 2016–40 for 195 countries and territories. Lancet 2018, 392, 2052–2090. [Google Scholar] [CrossRef]
- NHS England. The Five Year Forward View for Mental Health. Available online: https://www.england.nhs.uk/wp-content/uploads/2016/02/Mental-Health-Taskforce-FYFV-final.pdf (accessed on 14 October 2019).
- Bloom, D.E.; Cafiero, E.; Jané-Llopis, E.; Abrahams-Gessel, S.; Bloom, L.R.; Fathima, S.; Feigl, A.B.; Gaziano, T.; Hamandi, A.; Mowafi, M. The Global Economic Burden of Noncommunicable Diseases; World Economic Forum: Geneva, Switzerland, 2012. [Google Scholar]
- Roe, J.J.; Thompson, W.C.; Aspinall, A.P.; Brewer, J.M.; Duff, I.E.; Miller, D.; Mitchell, R.; Clow, A. Green space and stress: Evidence from cortisol measures in deprived urban communities. Int. J. Environ. Res. Public Health 2013, 10, 4086–4103. [Google Scholar] [CrossRef] [PubMed]
- Tyrväinen, L.; Ojala, A.; Korpela, K.; Lanki, T.; Tsunetsugu, Y.; Kagawa, T. The influence of urban green environments on stress relief measures: A field experiment. J. Environ. Psychol. 2014, 38, 1–9. [Google Scholar] [CrossRef]
- Olafsdottir, G.; Cloke, P.; Schulz, A.; van Dyck, Z.; Eysteinsson, T.; Thorleifsdottir, B.; Vögele, C. Health benefits of walking in nature: A randomized controlled study under conditions of real-life stress. Environ. Behav. 2018. [Google Scholar] [CrossRef]
- Hunter, M.R.; Gillespie, B.W.; Chen, S.Y.-P. Urban nature experiences reduce stress in the context of daily life based on salivary biomarkers. Front. Psychol. 2019, 10, 722. [Google Scholar] [CrossRef] [PubMed]
- Dadvand, P.; Nieuwenhuijsen, M.J.; Esnaola, M.; Forns, J.; Basagaña, X.; Alvarez-Pedrerol, M.; Rivas, I.; López-Vicente, M.; Pascual, M.D.C.; Su, J. Green spaces and cognitive development in primary schoolchildren. Proc. Natl. Acad. Sci. USA 2015, 112, 7937–7942. [Google Scholar] [CrossRef] [PubMed]
- Gidlow, C.J.; Jones, M.V.; Hurst, G.; Masterson, D.; Clark-Carter, D.; Tarvainen, M.P.; Smith, G.; Nieuwenhuijsen, M. Where to put your best foot forward: Psycho-physiological responses to walking in natural and urban environments. J. Environ. Psychol. 2016, 45, 22–29. [Google Scholar] [CrossRef]
- Barton, J.; Griffin, M.; Pretty, J. Exercise-, nature-and socially interactive-based initiatives improve mood and self-esteem in the clinical population. Perspect. Public Health 2012, 132, 89–96. [Google Scholar] [CrossRef] [PubMed]
- Gubbels, J.S.; Kremers, S.P.J.; Droomers, M.; Hoefnagels, C.; Stronks, K.; Hosman, C.; de Vries, S. The impact of greenery on physical activity and mental health of adolescent and adult residents of deprived neighborhoods: A longitudinal study. Health Place 2016, 40, 153–160. [Google Scholar] [CrossRef] [PubMed]
- Beyer, K.; Kaltenbach, A.; Szabo, A.; Bogar, S.; Nieto, F.; Malecki, K. Exposure to neighborhood green space and mental health: Evidence from the survey of the health of wisconsin. Int. J. Environ. Res. Public Health 2014, 11, 3453–3472. [Google Scholar] [CrossRef] [PubMed]
- Nutsford, D.; Pearson, A.L.; Kingham, S.; Reitsma, F. Residential exposure to visible blue space (but not green space) associated with lower psychological distress in a capital city. Health Place 2016, 39, 70–78. [Google Scholar] [CrossRef] [PubMed]
- Völker, S.; Kistemann, T. “I’m always entirely happy when I’m here!” urban blue enhancing human health and well-being in Cologne and Düsseldorf, Germany. Soc. Sci. Med. 2013, 91, 141–152. [Google Scholar] [CrossRef] [PubMed]
- White, M.; Smith, A.; Humphryes, K.; Pahl, S.; Snelling, D.; Depledge, M. Blue space: The importance of water for preference, affect, and restorativeness ratings of natural and built scenes. J. Environ. Psychol. 2010, 30, 482–493. [Google Scholar] [CrossRef]
- Grassini, S.; Revonsuo, A.; Castellotti, S.; Petrizzo, I.; Benedetti, V.; Koivisto, M. Processing of natural scenery is associated with lower attentional and cognitive load compared with urban ones. J. Environ. Psychol. 2019, 62, 1–11. [Google Scholar] [CrossRef]
- de Vries, S.; ten Have, M.; van Dorsselaer, S.; van Wezep, M.; Hermans, T.; de Graaf, R. Local availability of green and blue space and prevalence of common mental disorders in the Netherlands. BJPsych Open 2016, 2, 366–372. [Google Scholar] [CrossRef] [PubMed]
- Pedersen, E.; Weisner, S.E.B.; Johansson, M. Wetland areas’ direct contributions to residents’ well-being entitle them to high cultural ecosystem values. Sci. Total Environ. 2019, 646, 1315–1326. [Google Scholar] [CrossRef] [PubMed]
- Kaplan, S. The restorative benefits of nature: Toward an integrative framework. J. Environ. Psychol. 1995, 15, 169–182. [Google Scholar] [CrossRef]
- Reeves, J.P.; Knight, A.T.; Strong, E.A.; Heng, V.; Neale, C.; Cromie, R.; Vercammen, A. The application of wearable technology to quantify health and wellbeing co-benefits from urban wetlands. Front. Psychol. 2019, 10, 1840. [Google Scholar] [CrossRef] [PubMed]
- Mavoa, S.; Davern, M.; Breed, M.; Hahs, A. Higher levels of greenness and biodiversity associate with greater subjective wellbeing in adults living in Melbourne, Australia. Health Place 2019, 57, 321–329. [Google Scholar] [CrossRef] [PubMed]
- Aerts, R.; Honnay, O.; Van Nieuwenhuyse, A. Biodiversity and human health: Mechanisms and evidence of the positive health effects of diversity in nature and green spaces. Br. Med. Bull. 2018, 127, 5–22. [Google Scholar] [CrossRef] [PubMed]
- Carrus, G.; Scopelliti, M.; Lafortezza, R.; Colangelo, G.; Ferrini, F.; Salbitano, F.; Agrimi, M.; Portoghesi, L.; Semenzato, P.; Sanesi, G. Go greener, feel better? The positive effects of biodiversity on the well-being of individuals visiting urban and peri-urban green areas. Landsc. Urban Plan. 2015, 134, 221–228. [Google Scholar] [CrossRef]
- Dallimer, M.; Irvine, K.N.; Skinner, A.M.J.; Davies, Z.G.; Rouquette, J.R.; Maltby, L.L.; Warren, P.H.; Armsworth, P.R.; Gaston, K.J. Biodiversity and the feel-good factor: Understanding associations between self-reported human well-being and species richness. Bioscience 2012, 62, 47–55. [Google Scholar] [CrossRef]
- Lovell, R.; Depledge, M.; Maxwell, S. Health and the Natural Environment: A Review of Evidence, Policy, Practice and Opportunities for the Future. Available online: https://beyondgreenspace.files.wordpress.com/2018/09/health-and-the-natural-environment_full-report.pdf (accessed on 14 October 2019).
- Bragg, R.; Atkins, G. A Review of Nature-Based Interventions for Mental Health Care. Available online: http://publications.naturalengland.org.uk/publication/4513819616346112 (accessed on 14 October 2019).
- Shanahan, D.F.; Astell–Burt, T.; Barber, E.A.; Brymer, E.; Cox, D.T.C.; Dean, J.; Depledge, M.; Fuller, R.A.; Hartig, T.; Irvine, K.N. Nature–based interventions for improving health and wellbeing: The purpose, the people and the outcomes. Sports 2019, 7, 141. [Google Scholar] [CrossRef] [PubMed]
- Husk, K.; Blockley, K.; Lovell, R.; Bethel, A.; Lang, I.; Byng, R.; Garside, R. What Approaches to Social Prescribing Work, for Whom, and in What Circumstances? A Realist Review. Health Soc. Care Community 2019. Available online: https://0-onlinelibrary-wiley-com.brum.beds.ac.uk/doi/epdf/10.1111/hsc.12839 (accessed on 14 October 2019).
- Marselle, M.R.; Warber, S.L.; Irvine, K.N. Growing resilience through interaction with nature: Can group walks in nature buffer the effects of stressful life events on mental health? Int. J. Environ. Res. Public Health 2019, 16, 986. [Google Scholar] [CrossRef] [PubMed]
- Marselle, M.; Irvine, K.; Lorenzo-Arribas, A.; Warber, S. Moving beyond green: Exploring the relationship of environment type and indicators of perceived environmental quality on emotional well-being following group walks. Int. J. Environ. Res. Public Health 2015, 12, 106–130. [Google Scholar] [CrossRef] [PubMed]
- Korpela, K.M.; Stengård, E.; Jussila, P. Nature walks as a part of therapeutic intervention for depression. Ecopsychology 2016, 8, 8–15. [Google Scholar] [CrossRef]
- Iwata, Y.; Dhubháin, Á.N.; Brophy, J.; Roddy, D.; Burke, C.; Murphy, B. Benefits of group walking in forests for people with significant mental ill-health. Ecopsychology 2016, 8, 16–26. [Google Scholar] [CrossRef]
- Mumaw, L.M.; Maller, C.; Bekessy, S. Strengthening wellbeing in urban communities through wildlife gardening. Cities Environ. 2017, 10, 6. [Google Scholar]
- Park, S.-A.; Lee, A.-Y.; Park, H.-G.; Lee, W.-L. Benefits of gardening activities for cognitive function according to measurement of brain nerve growth factor levels. Int. J. Environ. Res. Public Health 2019, 16, 760. [Google Scholar] [CrossRef] [PubMed]
- De Kloet, E.R.; Joëls, M.; Holsboer, F. Stress and the brain: From adaptation to disease. Nat. Rev. Neurosci. 2005, 6, 463–475. [Google Scholar] [CrossRef] [PubMed]
- Tennant, R.; Hiller, L.; Fishwick, R.; Platt, S.; Joseph, S.; Weich, S.; Parkinson, J.; Secker, J.; Stewart-Brown, S. The Warwick-Edinburgh mental well-being scale (WEMWBS): Development and UK validation. Health Qual. Life Outcomes 2007, 5, 63. [Google Scholar] [CrossRef] [PubMed]
- Cohen, S.; Kamarck, T.; Mermelstein, R. A global measure of perceived stress. J. Health Soc. Behav. 1983, 24, 385–396. [Google Scholar] [CrossRef] [PubMed]
- Spitzer, R.L.; Kroenke, K.; Williams, J.B.W.; Löwe, B. A brief measure for assessing generalized anxiety disorder: The GAD-7. Arch. Intern. Med. 2006, 166, 1092–1097. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Watson, D.; Clark, L.A.; Tellegen, A. Development and validation of brief measures of positive and negative affect: The PANAS scales. J. Personal. Soc. Psychol. 1988, 54, 1063–1070. [Google Scholar] [CrossRef]
- R Core Team. R: A Language and Environment for Statistical Computing; R Core Team: Vienna, Austria, 2019; Available online: https://www.r-project.org/ (accessed on 14 October 2019).
- Hsieh, H.-F.; Shannon, S.E. Three approaches to qualitative content analysis. Qual. Health Res. 2005, 15, 1277–1288. [Google Scholar] [CrossRef] [PubMed]
- Edge, J. A pilot study addressing the effect of aromatherapy massage on mood, anxiety and relaxation in adult mental health. Complement. Ther. Nurs. Midwifery 2003, 9, 90–97. [Google Scholar] [CrossRef]
- Dayapoğlu, N.; Tan, M. Evaluation of the effect of progressive relaxation exercises on fatigue and sleep quality in patients with multiple sclerosis. J. Altern. Complement. Med. 2012, 18, 983–987. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Dimeo, F.C.; Thomas, F.; Raabe-Menssen, C.; Pröpper, F.; Mathias, M. Effect of aerobic exercise and relaxation training on fatigue and physical performance of cancer patients after surgery. A randomised controlled trial. Support. Care Cancer 2004, 12, 774–779. [Google Scholar] [CrossRef] [PubMed]
- Yu, D.S.F.; Lee, D.T.F.; Woo, J. Improving health-related quality of life of patients with chronic heart failure: Effects of relaxation therapy. J. Adv. Nurs. 2010, 66, 392–403. [Google Scholar] [CrossRef] [PubMed]
- Xu, J.; Roberts, R.E. The power of positive emotions: It’s a matter of life or death—subjective well-being and longevity over 28 years in a general population. Health Psychol. 2010, 29, 9–19. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Moskowitz, J.T.; Epel, E.S.; Acree, M. Positive affect uniquely predicts lower risk of mortality in people with diabetes. Health Psychol. 2008, 27, S73–S82. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Nylocks, K.M.; Rafaeli, E.; Bar-Kalifa, E.; Flynn, J.J.; Coifman, K.G. Testing the influence of negative and positive emotion on future health-promoting behaviors in a community sample. Motiv. Emot. 2019, 43, 285–298. [Google Scholar] [CrossRef]
- O’Brien, L. Engaging with and shaping nature: A nature-based intervention for those with mental mealth and behavioural problems at the Westonbirt Arboretum in England. Int. J. Environ. Res. Public Health 2018, 15, 2214. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Shanahan, D.F.; Lin, B.B.; Bush, R.; Gaston, K.J.; Dean, J.H.; Barber, E.; Fuller, R.A. Toward improved public health outcomes from urban nature. Am. J. Public Health 2015, 105, 470–477. [Google Scholar] [CrossRef] [PubMed]
- Frumkin, H. Beyond toxicity: Human health and the natural environment. Am. J. Prev. Med. 2001, 20, 234–240. [Google Scholar] [CrossRef]
- Irvine, K.N.; Warber, S.L. Greening healthcare: Practicing medicine as if the environment mattered. Altern. Ther. Health Med. 2002, 8, 76–83. [Google Scholar] [PubMed]
- Dierdre, D.; Sunil, B. Visitor attitudes and erosional impacts on the coast walk. Proc. Linn. Soc. N. S. W. 2012, 134, B113–B118. [Google Scholar]
- Bell, S.L.; Phoenix, C.; Lovell, R.; Wheeler, B.W. Seeking everyday wellbeing: The coast as a therapeutic landscape. Soc. Sci. Med. 2015, 142, 56–67. [Google Scholar] [CrossRef] [PubMed]
- White, M.P.; Alcock, I.; Wheeler, B.W.; Depledge, M.H. Coastal proximity, health and well-being: Results from a longitudinal panel survey. Health Place 2013, 23, 97–103. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ashbullby, K.J.; Pahl, S.; Webley, P.; White, M.P. The beach as a setting for families’ health promotion: A qualitative study with parents and children living in coastal regions in Southwest England. Health Place 2013, 23, 138–147. [Google Scholar] [CrossRef] [PubMed]
- Herzog, T.R.; Maguire, C.P.; Maguire, P.; Nebel, M.B. Assessing the restorative components of environments. J. Environ. Psychol. 2003, 23, 159–170. [Google Scholar] [CrossRef]
- Korpela, K.M.; Ylen, M.; Tyrvainen, L.; Silvennoinen, H. Favorite green, waterside and urban environments, restorative experiences and perceived health in Finland. Health Promot. Int. 2010, 25, 200–209. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Marselle, M.; Irvine, K.; Warber, S. Walking for well-being: Are group walks in certain types of natural environments better for well-being than group walks in urban environments? Int. J. Environ. Res. Public Health 2013, 10, 5603–5628. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Irvine, K.; Warber, S.; Devine-Wright, P.; Gaston, K. Understanding urban green space as a health resource: A qualitative comparison of visit motivation and derived effects among park users in Sheffield, UK. Int. J. Environ. Res. Public Health 2013, 10, 417–442. [Google Scholar] [CrossRef] [PubMed]
- Priest, P. The healing balm effect: Using a walking group to feel better. J. Health Psychol. 2007, 12, 36–52. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kaplan, R.; Kaplan, S. The Experience of Nature: A Psychological Perspective; Cambridge University Press: Cambridge, UK, 1989. [Google Scholar]
- Berman, M.G.; Jonides, J.; Kaplan, S. The cognitive benefits of interacting with nature. Psychol. Sci. 2008, 19, 1207–1212. [Google Scholar] [CrossRef] [PubMed]
- Kaplan, S.; Berman, M.G. Directed attention as a common resource for executive functioning and self-regulation. Perspect. Psychol. Sci. 2010, 5, 43–57. [Google Scholar] [CrossRef] [PubMed]
- James, W. Psychology: The Briefer Course; Holt: New York, NY, USA, 1892. [Google Scholar]
- South, J.; Giuntoli, G.; Kinsella, K. An Evaluation of the Walking for Wellness Project and the Befriender Role; London, UK, 2013. Available online: http://publications.naturalengland.org.uk/publication/4853061788893184 (accessed on 29 October 2019).
- Hartig, T.; Mitchell, R.; De Vries, S.; Frumkin, H. Nature and health. Annu. Rev. Public Health 2014, 35, 207–228. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ngom, R.; Gosselin, P.; Blais, C. Reduction of disparities in access to green spaces: Their geographic insertion and recreational functions matter. Appl. Geogr. 2016, 66, 35–51. [Google Scholar] [CrossRef]
- Schebella, M.F.; Weber, D.; Schultz, L.; Weinstein, P. The wellbeing benefits associated with perceived and measured biodiversity in Australian urban green spaces. Sustainability 2019, 11, 802. [Google Scholar] [CrossRef] [Green Version]
- Staats, H.; Hartig, T. Alone or with a friend: A social context for psychological restoration and environmental preferences. J. Environ. Psychol. 2004, 24, 199–211. [Google Scholar] [CrossRef]
- Heintzman, P. Nature-based recreation and spirituality: A complex relationship. Leis. Sci. 2009, 32, 72–89. [Google Scholar] [CrossRef]
- Mind. Feel better Outside, Feel Better Inside: Ecotherapy for Mental Wellbeing, Resilience and Recovery; London, UK, 2013. Available online: https://www.mind.org.uk/media/336359/Feel-better-outside-feel-better-inside-report.pdf (accessed on 29 October 2019).
- Fujiwara, D.; Campbell, R. Valuation Techniques for social Cost-Benefit Analysis: Stated Preference, Revealed Preference and Subjective Wellbeing Approaches; London, UK, 2011. Available online: https://assets.publishing.service.gov.uk/government/uploads/system/uploads/attachment_data/file/209107/greenbook_valuationtechniques.pdf (accessed on 29 October 2019).
- Fujiwara, D. A General Method for valuing Non-Market Goods Using Wellbeing Data: Three-Stage Wellbeing Valuation; CEP Discussion Papers (CEPDP1233). London, UK, 2013. Available online: http://eprints.lse.ac.uk/51577/ (accessed on 29 October 2019).
- Fujiwara, D.; Kudrna, L.; Dolan, P. Quantifying and Valuing the Wellbeing Impacts of Culture and Sport; London, UK, 2014. Available online: https://assets.publishing.service.gov.uk/government/uploads/system/uploads/attachment_data/file/304899/Quantifying_and_valuing_the_wellbeing_impacts_of_sport_and_culture.pdf (accessed on 29 October 2019).



{kind=link}
{kind=link}
| Sociodemographic Background | Wetland NBI | Community Mental Wellbeing Service | ||
|---|---|---|---|---|
| N | % | N | % | |
| Gender | n = 16 | n = 851 | ||
| Male | 8 | 50 | 406 | 48 |
| Female | 8 | 50 | 445 | 52 |
| Age | n = 16 | n = 851 | ||
| 18–29 | 3 | 19 | 190 | 22 |
| 30–49 | 5 | 31 | 341 | 40 |
| 50–64 | 3 | 19 | 300 | 35 |
| 65–84 | 5 | 31 | 20 | 3 |
| Ethnicity | n = 16 | n = 508 | ||
| White—British | 13 | 81 | 477 | 94 |
| White—Other | 3 | 19 | 17 | 3 |
| Any Black background | 0 | 0 | 6 | 1 |
| Any Asian background | 0 | 0 | 4 | 1 |
| Other ethnic background | 0 | 0 | 4 | 1 |
| Employment status | n = 16 | n = 209 | ||
| Currently unemployed | 10 | 63 | 163 | 78 |
| Retired | 5 | 31 | 13 | 6 |
| Student | 1 | 6 | 1 | 1 |
| Employed (Full-time) | 0 | 0 | 12 | 6 |
| Employed (Part-time) | 0 | 0 | 14 | 7 |
| Voluntary work | 0 | 0 | 5 | 2 |
| Home environment | n = 16 | Not asked of wider membership | ||
| Urban | 8 | 50 | ||
| Rural | 8 | 50 | ||
| Measure a | Pre-Intervention Mean (± SE) | Post-Intervention Mean (± SE) | z | p |
|---|---|---|---|---|
| WEMWBS | 37 (± 2.79) | 41 (± 4.31) | −2.60 | 0.009 |
| GAD-7 | 13.27 (± 1.54) | 10.28 (± 1.46) | −3.02 | 0.002 |
| PSS | 24.31 (± 2.54) | 22.35 (± 1.47) | −2.04 | 0.041 |
| PANAS (positive) | 26 (± 2.64) | 30.57 (± 3.08) | −2.49 | 0.012 |
| PANAS (negative) | 28.63 (± 2.99) | 27.71 (± 3.66) | −2.24 | 0.025 |
© 2019 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Maund, P.R.; Irvine, K.N.; Reeves, J.; Strong, E.; Cromie, R.; Dallimer, M.; Davies, Z.G. Wetlands for Wellbeing: Piloting a Nature-Based Health Intervention for the Management of Anxiety and Depression. Int. J. Environ. Res. Public Health 2019, 16, 4413. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph16224413
Maund PR, Irvine KN, Reeves J, Strong E, Cromie R, Dallimer M, Davies ZG. Wetlands for Wellbeing: Piloting a Nature-Based Health Intervention for the Management of Anxiety and Depression. International Journal of Environmental Research and Public Health. 2019; 16(22):4413. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph16224413
Chicago/Turabian StyleMaund, Phoebe R., Katherine N. Irvine, Jonathan Reeves, Emily Strong, Ruth Cromie, Martin Dallimer, and Zoe G. Davies. 2019. "Wetlands for Wellbeing: Piloting a Nature-Based Health Intervention for the Management of Anxiety and Depression" International Journal of Environmental Research and Public Health 16, no. 22: 4413. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph16224413