Progreso en Salud: Findings from Two Adapted Social Network HIV Risk Reduction Interventions for Latina Seasonal Workers


Abstract
:1. Introduction
2. Materials and Methods
2.1. The Adapted VOICES Intervention
2.2. The HEALTHY Intervention
2.3. Assessments
2.4. Measures
2.5. Data Analysis
3. Results
3.1. Cognitive Factors
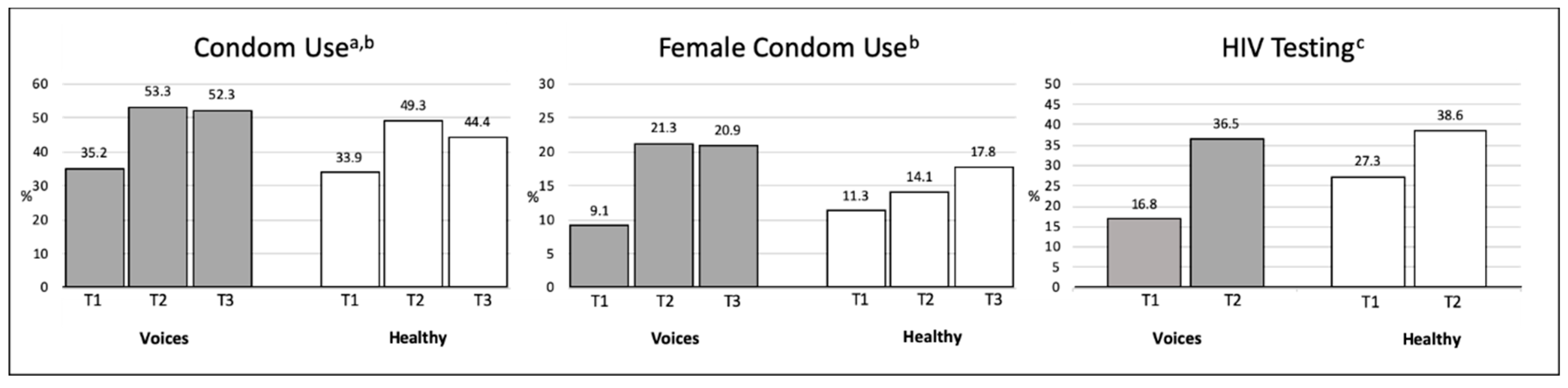
3.2. Behavioral Factors
3.3. Communication Factors
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- Centers for Disease Control and Prevention. CDC Fact Sheet: HIV among Latinos; Centers for Disease Control and Prevention: Atlanta, GA, USA, 2015.
- Centers for Disease Control and Prevention. HIV and Hispanics/Latinos. Available online: https://www.cdc.gov/hiv/group/racialethnic/hispaniclatinos/index.html (accessed on 6 December 2018).
- Centers for Disease Control and Prevention. HIV among Latinos: A Snapshot; Centers for Disease Control and Prevention: Atlanta, GA, USA, 2017.
- Henao-Martinez, A.; Castillo-Mancilla, J. The Hispanic HIV epidemic. Curr. Infect. Dis. Rep. 2013, 15, 46–51. [Google Scholar] [CrossRef] [PubMed]
- Shriver, M. The Shriver Report: A Woman’s Nation Pushes Back from the Brink; Macmillan: New York, NY, USA, 2014. [Google Scholar]
- Snyder, T.; de Brey, C.; Dillow, S. Digest of Education Statistics 2014 NCES 2016-006; National Center for Education Statistics: Washington, DC, USA, 2016.
- Kanamori, M.; De La Rosa, M.; Diez, S.; Weissman, J.; Trepka, M.J.; Sneij, A.; Schmidt, P.; Rojas, P. A brief report: Lessons learned and preliminary findings of Progreso en Salud, an HIV risk reduction intervention for Latina seasonal farmworkers. Int. J. Environ. Res. Public Health 2016, 14, 32. [Google Scholar] [CrossRef] [PubMed]
- McCullagh, M.C.; Sanon, M.-A.; Foley, J.G. Cultural health practices of migrant seasonal farmworkers. J. Cult. Divers. 2015, 22, 64. [Google Scholar] [PubMed]
- National Center for Farmworker Health. Farmworker Fact. Sheet; National Center for Farmworker Health: Buda, TX, USA, 2017.
- National Center for Farmworker Health. HIV/AIDS Agricultural Worker Factsheet; National Center for Farmworker Health: Buda, TX, USA, 2017.
- Centers for Disease Control and Prevention. HIV Surveillance Report: Diagnoses of HIV Infection in the United States and Dependent Areas. 2017. Available online: https://www.cdc.gov/hiv/pdf/library/reports/surveillance/cdc-hiv-surveillance-report-2017-vol-29.pdf (accessed on 1 April 2019).
- Florida Department of Health; Bureau of Communicable Diseases; HIV/AIDS Section. Epidemiological Profile for Area 11, Miami-Dade County. 2018. Available online: http://miamidade.floridahealth.gov/programs-and-services/infectious-disease-services/hiv-aids-services/_documents/10-26-18-update-HIV-Surveillance/_documents/FS-2017-MIAMI-DADE.pdf (accessed on 1 April 2019).
- Florida Department of Health Miami-Dade County. HIV/AIDS Surveillance Electronic HIV/AIDS Reporting System [e-HARS]. In Frozen database on June 2016 ed. 2016. Available online: http://miamidade.floridahealth.gov/programs-and-services/infectious-disease-services/hiv-aids-services/_documents/1-6-17-hiv-aids-surveillance-monthly-report/_documents/hiv-surveillance-monthly-report-2016-11.pdf (accessed on 1 April 2019).
- Cianelli, R.; Villegas, N. Social Determinants of Health for HIV among Hispanic Women; SAGE Publications Sage CA: Los Angeles, CA, USA, 2016. [Google Scholar]
- Acevedo, V. Cultural competence in a group intervention designed for Latino patients living with HIV/AIDS. Health Soc. Work 2008, 33, 111–120. [Google Scholar] [CrossRef]
- Ghosh, D.; Krishnan, A.; Gibson, B.; Brown, S.-E.; Latkin, C.A.; Altice, F.L. Social network strategies to address HIV prevention and treatment continuum of care among at-risk and HIV-infected substance users: A systematic scoping review. AIDS Behav. 2017, 21, 1183–1207. [Google Scholar] [CrossRef]
- Schulz, K.F.; Altman, D.G.; Moher, D. CONSORT 2010 statement: Updated guidelines for reporting parallel group randomised trials. BMC Med. 2010, 8, 18. [Google Scholar] [CrossRef]
- Añez, L.M.; Paris, M., Jr.; Bedregal, L.E.; Davidson, L.; Grilo, C.M. Application of cultural constructs in the care of first generation Latino clients in a community mental health setting. J. Psychiatr. Pract. 2005, 11, 221–230. [Google Scholar] [CrossRef]
- Comas-Diaz, L. Latino healing: The integration of ethnic psychology into psychotherapy. Psychother. Theory Res. Pract. Train. 2006, 43, 436. [Google Scholar] [CrossRef]
- Damschroder, L.J.; Lowery, J.C. Evaluation of a large-scale weight management program using the consolidated framework for implementation research (CFIR). Implement. Sci. 2013, 8, 51. [Google Scholar] [CrossRef]
- Peterson-Iyer, K. Culturally Competent Care for Latino Patients: Introduction; Markulla Center for Applied Ethics: Santa Clara, CA, USA, 2008; Volume 5, p. 2011. [Google Scholar]
- Heckathorn, D.D. Comment: Snowball versus respondent-driven sampling. Sociol. Methodol. 2011, 41, 355–366. [Google Scholar] [CrossRef]
- Farquhar, S.; de Jesus Gonzalez, C.; Hall, J.; Samples, J.; Ventura, S.; Sanchez, V.; Shadbeh, N. Recruiting and retaining indigenous farmworker participants. J. Immigr. Minor. Health 2014, 16, 1011–1015. [Google Scholar] [CrossRef] [PubMed]
- Ajzen, I.; Fishbein, M. Understanding Attitudes and Predicting Social Behaviour; Pearson: London, UK, 1980. [Google Scholar]
- Neumann, M.S.; O’Donnell, L.; San Doval, A.; Schillinger, J.; Blank, S.; Ortiz-Rios, E.; Garcia, T.; O’Donnell, C.R. Effectiveness of the VOICES/VOCES sexually transmitted disease/human immunodeficiency virus prevention intervention when administered by health department staff: Does it work in the “real world”? Sex. Transm. Dis. 2011, 38, 133–139. [Google Scholar] [CrossRef]
- Fisher, H.H.; Patel-Larson, A.; Green, K.; Shapatava, E.; Uhl, G.; Kalayil, E.; Moore, A.; Williams, W.; Chen, B. Evaluation of an HIV prevention intervention for African Americans and Hispanics: Findings from the VOICES/VOCES Community-based Organization Behavioral Outcomes Project. AIDS Behav. 2011, 15, 1691. [Google Scholar] [CrossRef] [PubMed]
- Hamdallah, M.; Vargo, S.; Herrera, J. The VOICES/VOCES success story: Effective strategies for training, technical assistance and community-based organization implementation. AIDS Educ. Prev. 2006, 18, 171–183. [Google Scholar] [CrossRef]
- O’Donnell, L.N.; Doval, A.S.; Duran, R.; O’Donnell, C. Video-based sexually transmitted disease patient education: Its impact on condom acquisition. Am. J. Public Health 1995, 85, 817–822. [Google Scholar] [CrossRef] [PubMed]
- O’Donnell, L.; Stueve, A.; Joseph, H.A.; Flores, S. Adapting the VOICES HIV behavioral intervention for Latino men who have sex with men. AIDS Behav. 2014, 18, 767–775. [Google Scholar] [CrossRef]
- Stallworth, J.M.; Andía, J.F.; Burgess, R.; Alvarez, M.E.; Collins, C. Diffusion of effective behavioral interventions and Hispanic/Latino populations. AIDS Educ. Prev. 2009, 21 (Suppl. B), 152–163. [Google Scholar] [CrossRef]
- Kanamori, M.; De La Rosa, M.; Diez, S.L.; Weissman, J.; Trepka, M.J.; Sneij, A.; Schmidt, P.; Rojas, P. Progreso en Salud, An HIV risk reduction intervention for Latina seasonal farmworkers: Preliminary findings. In Annals of Behavioral Medicine; Springer: Berlin/Heidelberg, Germany, 2017; pp. S2604–S2605. [Google Scholar]
- Bryan, A.D.; Aiken, L.S.; West, S.G. Increasing condom use: Evaluation of a theory-based intervention to prevent sexually transmitted diseases in young women. Health Psychol. 1996, 15, 371. [Google Scholar] [CrossRef]
- Zeger, S.L.; Liang, K.-Y.; Albert, P.S. Models for longitudinal data: A generalized estimating equation approach. Biometrics 1988, 1049–1060. [Google Scholar] [CrossRef]
- Hubbard, A.E.; Ahern, J.; Fleischer, N.L.; Van der Laan, M.; Satariano, S.A.; Jewell, N.; Bruckner, T.; Satariano, W.A. To GEE or not to GEE: Comparing population average and mixed models for estimating the associations between neighborhood risk factors and health. Epidemiology 2010, 21, 467–474. [Google Scholar] [CrossRef]
- Wang, K.; Brown, K.; Shen, S.Y.; Tucker, J. Social network-based interventions to promote condom use: A systematic review. AIDS Behav. 2011, 15, 1298–1308. [Google Scholar] [CrossRef] [PubMed]
- Dunning, T.; Freedman, D. Modeling selection effects. In The Sage Handbook of Social Science Methodology; Outhwaite, W., Turner, S.P., Eds.; Sage: London, UK, 2007. [Google Scholar]
- Christakis, N.A.; Fowler, J.H. Connected: The Surprising Power of Our Social Networks and How They Shape Our Lives—How Your Friends’ Friends’ Friends Affect Everything You Feel, Think, and Do; Back Bay Books: New York, NY, USA, 2011. [Google Scholar]
- Fowler, J.H.; Christakis, N.A. Cooperative behavior cascades in human social networks. Proc. Natl. Acad. Sci. USA 2010, 107, 5334–5338. [Google Scholar] [CrossRef] [PubMed]
- Valente, T.; Ritt-Olson, A.; Stacy, A.; Unger, J.; Okamoto, J.; Sussman, S. Peer acceleration: Effects of a social network tailored substance abuse prevention program among high-risk adolescents. Addiction 2007, 102, 1804–1815. [Google Scholar] [CrossRef] [PubMed]
- Rand, D.; Arbesman, S.; Christakis, N. Dynamic social networks promote cooperation in experiments with humans. Proc. Natl. Acad. Sci. USA 2011, 108, 19193–19198. [Google Scholar] [CrossRef] [PubMed]
- Banerjee, A.; Chandrasekhar, A.G.; Duflo, E.; Jackson, M.O. The diffusion of microfinance. Science 2013, 341, 1236498. [Google Scholar] [CrossRef]
- Merzel, C.; D’Afflitti, J. Reconsidering community-based health promotion: Promise, performance, and potential. Am. J. Public Health 2003, 93, 557–574. [Google Scholar] [CrossRef]
- Stephens, A.J.; Tchetgen, E.J.T.; De Gruttola, V. Augmented GEE for improving efficiency and validity of estimation in cluster randomized trials by leveraging cluster-and individual-level covariates. Stat. Med. 2012, 31, 915. [Google Scholar] [CrossRef]
- Panageas, K.S.; Schrag, D.; Russell Localio, A.; Venkatraman, E.; Begg, C.B. Properties of analysis methods that account for clustering in volume–outcome studies when the primary predictor is cluster size. Stat. Med. 2007, 26, 2017–2035. [Google Scholar] [CrossRef]
- Hussey, M.A.; Hughes, J.P. Design and analysis of stepped wedge cluster randomized trials. Contemp. Clin. Trials 2007, 28, 182–191. [Google Scholar] [CrossRef]
- Food and Drug Administration. Truvada Approved to Reduce the Risk of Sexually Transmitted HIV in People Who Are Not Infected with the Virus. 2012. Available online: https://www.fda.gov/media/83604/download (accessed on 1 April 2019).
- Thigpen, M.C.; Kebaabetswe, P.M.; Paxton, L.A.; Smith, D.K.; Rose, C.E.; Segolodi, T.M.; Henderson, F.L.; Pathak, S.R.; Soud, F.A.; Chillag, K.L. Antiretroviral preexposure prophylaxis for heterosexual HIV transmission in Botswana. N. Engl. J. Med. 2012, 367, 423–434. [Google Scholar] [CrossRef]
- Baeten, J.M.; Donnell, D.; Ndase, P.; Mugo, N.R.; Campbell, J.D.; Wangisi, J.; Tappero, J.W.; Bukusi, E.A.; Cohen, C.R.; Katabira, E. Antiretroviral prophylaxis for HIV prevention in heterosexual men and women. N. Engl. J. Med. 2012, 367, 399–410. [Google Scholar] [CrossRef] [PubMed]
- Grant, R.M.; Lama, J.R.; Anderson, P.L.; McMahan, V.; Liu, A.Y.; Vargas, L.; Goicochea, P.; Casapía, M.; Guanira-Carranza, J.V.; Ramirez-Cardich, M.E. Preexposure chemoprophylaxis for HIV prevention in men who have sex with men. N. Engl. J. Med. 2010, 363, 2587–2599. [Google Scholar] [CrossRef] [PubMed]
- Anderson, P.L.; Glidden, D.V.; Liu, A.; Buchbinder, S.; Lama, J.R.; Guanira, J.V.; McMahan, V.; Bushman, L.R.; Casapía, M.; Montoya-Herrera, O. Emtricitabine-tenofovir concentrations and pre-exposure prophylaxis efficacy in men who have sex with men. Sci. Transl. Med. 2012, 4. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Aaron, E.; Blum, C.; Seidman, D.; Hoyt, M.J.; Simone, J.; Sullivan, M.; Smith, D.K. Optimizing delivery of HIV preexposure prophylaxis for women in the United States. AIDS Patient Care STDs 2018, 32, 16–23. [Google Scholar] [CrossRef] [Green Version]
- Walters, S.M.; Rivera, A.V.; Starbuck, L.; Reilly, K.H.; Boldon, N.; Anderson, B.J.; Braunstein, S. Differences in awareness of pre-exposure prophylaxis and post-exposure prophylaxis among groups at-risk for HIV in New York State: New York City and Long Island, NY, 2011–2013. JAIDS J. Acquir. Immune Defic. Syndr. 2017, 75, S383–S391. [Google Scholar] [CrossRef]
- Eaton, L.A.; Matthews, D.D.; Driffin, D.D.; Bukowski, L.; Wilson, P.A.; Stall, R.D.; Team, P.S. A multi-US city assessment of awareness and uptake of pre-exposure prophylaxis (PrEP) for HIV prevention among Black men and transgender women who have sex with men. Prev. Sci. 2017, 18, 505–516. [Google Scholar] [CrossRef]
- Flash, C.A.; Dale, S.K.; Krakower, D.S. Pre-exposure prophylaxis for HIV prevention in women: Current perspectives. Int. J. Women’s Health 2017, 9, 391. [Google Scholar] [CrossRef] [Green Version]


{kind=link}
| VOICES | HEALTHY | ||||
|---|---|---|---|---|---|
| Characteristics | n | % | n | % | p Value |
| Total | 127 | 100 | 131 | 100 | |
| Mean age in years (standard deviation) | 34.8 | (9.9) | 34.5 | (10.3) | 0.834 |
| Highest level of Education | |||||
| None | 8 | 6.3 | 7 | 5.3 | 0.226 |
| From 1st to 8th grade | 54 | 42.5 | 38 | 29.0 | |
| 9th to 11th grade | 19 | 15.0 | 23 | 17.6 | |
| High school graduate or equivalent degree | 18 | 14.2 | 20 | 15.3 | |
| Post high school education | 18 | 14.2 | 21 | 16.0 | |
| Some Bachelor-level college education | 10 | 16.8 | 22 | 16.8 | |
| Marital Status | |||||
| Single | 22 | 17.3 | 29 | 22.1 | 0.472 |
| Legally married | 50 | 39.4 | 49 | 37.4 | |
| Cohabitating | 48 | 37.8 | 41 | 31.3 | |
| Separated/divorced | 6 | 4.8 | 12 | 9.1 | |
| Widow | 1 | 0.8 | 0 | 0.0 | |
| Country of Birth | |||||
| Non US-born | 105 | 82.7 | 108 | 82.4 | 0.960 |
| US-born | 22 | 17.3 | 23 | 17.6 | |
| Mean total income from the past 6 months, US dollars (standard deviation) | 5506 | (508) | 5611 | (492) | 0.122 |
| Has health insurance | |||||
| Yes | 27 | 21.3 | 32 | 24.4 | 0.324 |
| No | 100 | 78.7 | 99 | 75.6 | |
| Trajectories | b | SE | 95% CI | Effect Size (d) |
|---|---|---|---|---|
| Cognitive Factors | ||||
| HIV Knowledge | 0.09 | |||
| 6-months follow-up | 2.35 *** | 0.39 | 1.59–3.11 | |
| 12-months follow-up | 2.45 *** | 0.41 | 1.65–3.26 | |
| VOICES vs. HEALTHY | −1.22 *** | 0.33 | −1.86–0.57 | |
| Condom use self-efficacy | 0.02 | |||
| 6-months follow-up | 0.84 * | 0.38 | 0.10–1.59 | |
| 12-months follow-up | 0.84 * | 0.37 | 0.13–1.56 | |
| VOICES vs. HEALTHY | −0.6 * | 0.31 | −1.29–0.08 | |
| Adequate knowledge of condom use | 0.08 | |||
| 6-months follow-up | 1.11 * | 0.45 | 0.23–1.99 | |
| 12-months follow-up | 2.74 *** | 0.41 | 1.94–3.55 | |
| VOICES vs. HEALTHY | −0.59 | 0.36 | −1.29–0.10 | |
| Behavioral Factors | ||||
| Condom use | ||||
| 6-months follow-up | 0.41 ** | 0.14 | 0.14–0.69 | 0.01 |
| 12-months follow-up | 0.37 ** | 0.12 | 0.13–0.62 | |
| VOICES vs. HEALTHY | 0.08 | 0.22 | −0.35–0.52 | |
| Female condom use | ||||
| 6-months follow-up | 0.62 * | 0.30 | 0.05–1.20 | 0.01 |
| 12-months follow-up | 0.75 ** | 0.29 | 0.19–1.32 | |
| VOICES vs. HEALTHY | 0.13 | 0.24 | −1.16–0.71 | |
| HIV testing | 0.03 | |||
| Changes from before intervention (baseline) to during intervention (6-months and 12-months follow-up) | 0.77 *** | 0.21 | 0.37–1.18 | |
| VOICES vs. HEALTHY | −0.34 | 0.21 | −0.75–0.07 | |
| Communication Factors | ||||
| Talk with friends about HIV prevention | 0.07 | |||
| 6-months follow-up | 1.11 *** | 0.25 | 0.63–1.59 | |
| 12-months follow-up | 1.51 *** | 0.26 | 1.01–2.02 | |
| Intervention VOICES | 0.40 | 0.21 | −0.01–0.81 | |
| Intention to negotiate safe sex with male partner | ||||
| 6-months follow-up | 0.15 * | 0.07 | 0.01–0.29 | 0.01 |
| 12-months follow-up | 0.05 | 0.07 | −0.09–0.20 | |
| VOICES vs. HEALTHY | 0.05 | 0.06 | −0.07–0.16 | |
© 2019 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Kanamori, M.; De La Rosa, M.; Shrader, C.-H.; Munayco, C.; Doblecki-Lewis, S.; Prado, G.; Safren, S.; Trepka, M.J.; Fujimoto, K. Progreso en Salud: Findings from Two Adapted Social Network HIV Risk Reduction Interventions for Latina Seasonal Workers. Int. J. Environ. Res. Public Health 2019, 16, 4530. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph16224530
Kanamori M, De La Rosa M, Shrader C-H, Munayco C, Doblecki-Lewis S, Prado G, Safren S, Trepka MJ, Fujimoto K. Progreso en Salud: Findings from Two Adapted Social Network HIV Risk Reduction Interventions for Latina Seasonal Workers. International Journal of Environmental Research and Public Health. 2019; 16(22):4530. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph16224530
Chicago/Turabian StyleKanamori, Mariano, Mario De La Rosa, Cho-Hee Shrader, Cesar Munayco, Susanne Doblecki-Lewis, Guillermo Prado, Steven Safren, Mary Jo Trepka, and Kayo Fujimoto. 2019. "Progreso en Salud: Findings from Two Adapted Social Network HIV Risk Reduction Interventions for Latina Seasonal Workers" International Journal of Environmental Research and Public Health 16, no. 22: 4530. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph16224530