Oral Health Status and Need for Oral Care in an Aging Population: A Systematic Review

 , ,
, ,  ,
,
Abstract
:1. Introduction
1.1. Rationale of the Systematic Review
1.2. Objectives
1.3. Clinical Question (PICO):
- P: A population of participants with diagnosis of dementia aged 60 years or older
- I: Analysis of the oral health status and of the association between periodontal disease and dementia
- C: Comparison between oral health of elderly with and without dementia
- O: Prevalence of oral disease (affecting hard and soft tissues) in elderly with dementia compared to those without dementia, to define their need of oral care. Role of tooth loss due to periodontal disease in the onset/progression of dementia.
2. Material and Methods
2.1. Protocol and Registration
2.2. Eligibility Criteria
- Participants must have been diagnosed with dementia
- Quantitative data about oral health problems
- Participants had to be available
- Participants had to be 60 years or older
- Cohort, case-control, cross-sectional studies, and clinical trial were considered
- Case report and reviews
- No quantitative data available
- Age of participants below 60 years
2.2.1. Search
2.2.2. Study Selection
2.2.3. Data Collection Process
2.2.4. Quality assessment
3. Results
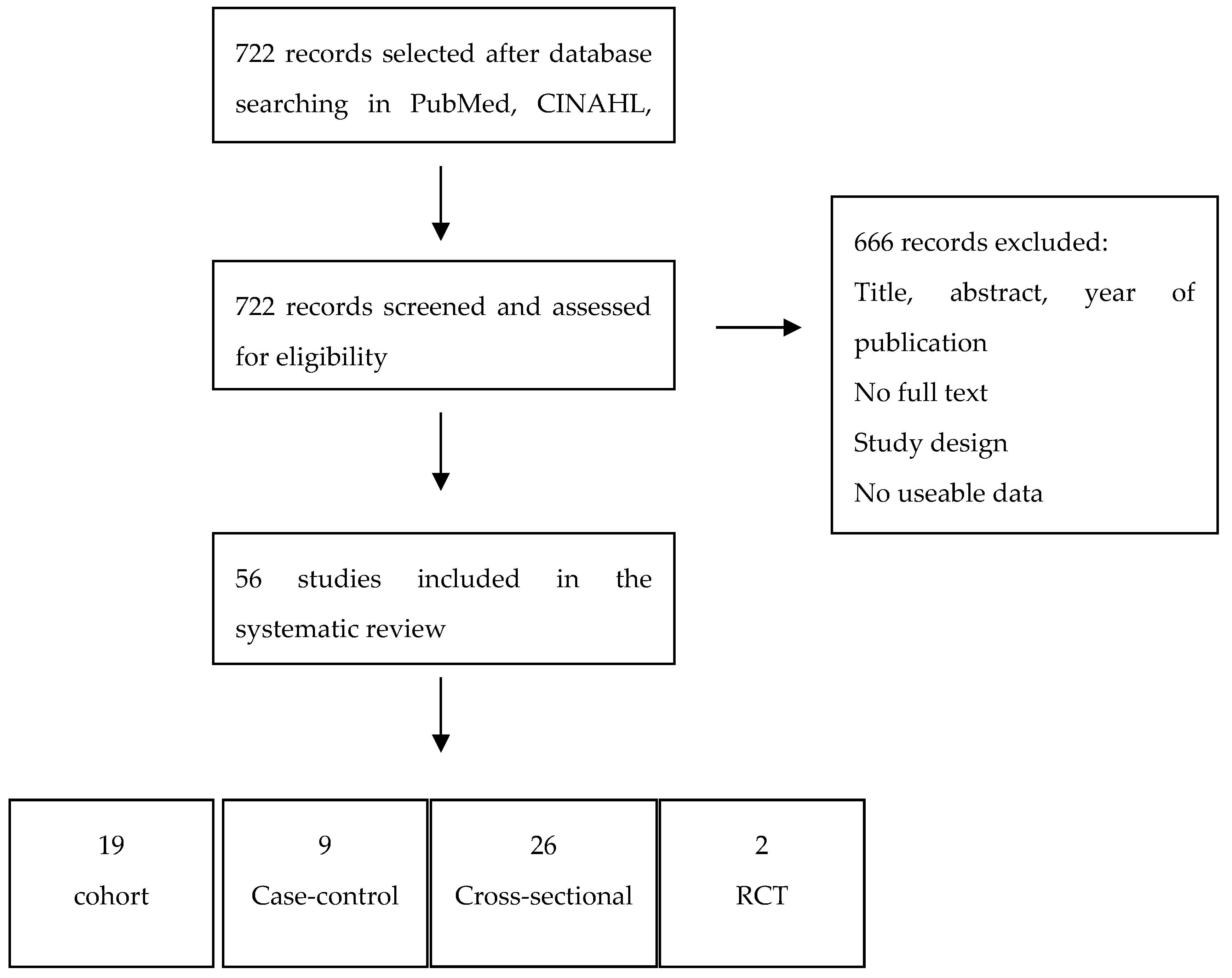
3.1. Study Selection and Characteristics
3.2. Results of Individual Studies
4. Discussion
Strengths and Limitations
5. Conclusions
Author Contributions
Funding
Conflicts of Interest
References
- National Institute on Aging; National Institutes of Health, U.S.; Department of Health and Human Services. Global Health and Aging; World Health Organisation: Geneva, Switzerland, 2011. [Google Scholar]
- Lopez, R.; Smith, P.C.; Göstemeyer, G.; Schwendicke, F. Ageing, dental caries and periodontal diseases. J. Clin. Periodontol. 2017, 44 (Suppl. 18), S145–S152. [Google Scholar] [CrossRef] [PubMed]
- Nangle, M.R.; Riches, J.; Grainger, S.A.; Manchery, N.; Sachdev, P.S.; Henry, J.D. Oral Health and Cognitive Function in Older Adults: A systematic Review. Gerodontology 2019, 65, 659–672. [Google Scholar] [CrossRef] [PubMed]
- Wu, B.; Fillenbaum, G.G.; Plassman, B.L.; Guo, L. Association Between Oral Health and Cognitive Status: A Systematic Review. J. Am. Geriatr. Soc. 2016, 64, 739–751. [Google Scholar] [CrossRef] [PubMed]
- Moritz, D.J.; Kasl, S.V.; Berkman, L.F. Cognitive Functioning and the Incidence of Limitations in Activities of Daily Living in an Elderly Community Sample. Am. J. Epidemiol. 1995, 141, 41–49. [Google Scholar] [CrossRef] [PubMed]
- Ship, J.A.; De Carli, C.; Friedland, R.P.; Baum, B.J. Diminished submandibular salivary flow in dementia of the Alzheimer type. J. Gerontol. 1990, 45, M61–M66. [Google Scholar] [CrossRef] [PubMed]
- Ship, J.A.; Pillemer, S.R.; Baum, B.J. Xerostomia and the geriatric patient. J. Am. Geriatr. Soc. 2002, 50, 535–543. [Google Scholar] [CrossRef] [PubMed]
- Silva, M.; Hopcraft, M.; Morgan, M. Dental caries in Victorian nursing homes. Aust. Dent. J. 2014, 59, 321–328. [Google Scholar] [CrossRef]
- Martande, S.S.; Pradeep, A.R.; Singh, S.P.; Kumari, M.; Suke, D.K.; Raju, A.P.; Naik, S.B.; Singh, P.; Guruprasad, C.N.; Chatterji, A. Periodontal Health Condition in Patients With Alzheimer’s Disease. Am. J. Alzheimers Dis. Other Demen. 2014, 29, 498–502. [Google Scholar] [CrossRef]
- Lee, Y.T.; Lee, H.C.; Hu, C.J.; Huang, L.K.; Chao, S.P.; Lin, C.P.; Su, E.C.; Lee, Y.C.; Chen, C.C. Periodontitis as a Modifiable Risk Factor for Dementia: A Nationwide Population-Based Cohort Study. Am. Geriatr. Soc. 2017, 65, 301–305. [Google Scholar] [CrossRef]
- Ewan, V.; Staines, K. Diagnosis and management of oral mucosal lesions in older people: A review. Rev. Clin. Gerontol. 2008, 18, 115–128. [Google Scholar] [CrossRef]
- De Vries, M.W.; Visscher, C.; Delwel, S.; van der Steen, J.T.; Pieper, M.J.C.; Scherder, E.J.A.; Achterberg, W.P.; Lobbezoo, F. Orofacial Pain during Mastication in People with Dementia: Reliability Testing of the Orofacial Pain Scale for Non-Verbal Individuals. Behav. Neurol. 2016, 2016, 3123402. [Google Scholar] [CrossRef] [PubMed]
- Chalmers, J.M.; Carter, K.D.; Spencer, A.J. Oral diseases and conditions in community-living older adults with and without dementia. Spec. Care Dent. 2003, 23, 7–17. [Google Scholar] [CrossRef] [PubMed]
- Gil-Montoya, J.A.; Sanchez-Lara, I.; Carnero-Pardo, C.; Fornieles-Rubio, F.; Montes, J.; Barrios, R.; Gonzalez-Moles, M.A.; Bravo, M. Oral Hygiene in the Elderly with Different Degrees of Cognitive Impairment and Dementia. J. Am. Geriatr. Soc. 2017, 65, 642–647. [Google Scholar] [CrossRef]
- Cerutti-Kopplin, D.; Feine, J.; Padilha, D.M.; de Souza, R.F.; Ahmadi, M.; Rompré, P.; Booij, L.; Emami, E. Tooth Loss Increases the Risk of Diminished Cognitive Function: A Systematic Review and Meta-analysis. JDR Clin. Trans. Res. 2016, 1, 10–19. [Google Scholar] [CrossRef] [PubMed]
- Noble, J.M.; Scarmeas, N.; Papapanou, P.N. Poor Oral Health as a Chronic, Potentially, Modifiable Dementia Risk Factor: Review of Literature. Curr. Neurol. Neurosci. Rep. 2013, 13, 384. [Google Scholar] [CrossRef] [PubMed]
- Liberati, A.; Altman, D.G.; Tetzlaff, J.; Mulrow, C.; Gøtzsche, P.C.; Ioannidis, J.P.; Clarke, M.; Devereaux, P.J.; Kleijnen, J.; Moher, D. The PRISMA statement for reporting systematic reviews and meta-analyses of studies that evaluate health care interventions: Explanation and elaboration. J. Clin. Epidemiol. 2009, 62, e1–e34. [Google Scholar] [CrossRef] [PubMed]
- Wells, G.A.; Shea, B.; O’Connell, D.; Petersen, J.; Welch, V.; Losos, M.; Tugwell, P. The Newcastle-Ottawa Scale (NOS) for Assessing the Quality of Nonrandomized Studies in Meta-Analyses; Department of Epidemiology and Community Medicine, University of Ottawa, Canada: Ottawa, ON, Canada, 2012. [Google Scholar]
- Hoeksema, A.R.; Peters, L.L.; Raghoebar, G.M.; Meijer, H.J.A.; Vissink, A.; Visser, A. Oral health status and need for oral care of care-dependent indwelling elderly: From admission to death. Clin. Oral Investig. 2017, 21, 2189–2196. [Google Scholar] [CrossRef] [PubMed]
- Luo, J.; Wu, B.; Zhao, Q.; Guo, Q.; Meng, H.; Yu, L.; Zheng, L.; Hong, Z.; Ding, D. Association between tooth loss and cognitive function among 3063 Chinese older adults: A community-based study. PLoS ONE 2015, 10, e0120986. [Google Scholar] [CrossRef]
- Chalmers, J.M.; Carter, K.D.; Spencer, A.J. Caries incidence and increments in community-living older adults with and without dementia. Gerodontology 2002, 19, 80–94. [Google Scholar] [CrossRef]
- Chalmers, J.M.; Carter, K.; Spencer, A. Oral health of Adelaide nursing home residents: Longitudinal study. Aust. J. Ageing 2004. [Google Scholar] [CrossRef]
- Chen, X.; Shuman, S.K.; Hodges, J.S.; Gatewood, L.C.; Xu, J. Patterns of tooth loss in older adults with and without dementia: A retrospective study based on a Minnesota cohort. J. Am. Geriatr. Soc. 2010, 58, 2300–2307. [Google Scholar] [CrossRef] [PubMed]
- De Souza Rolim, T.; Fabri, G.M.; Nitrini, R.; Anghinah, R.; Teixeira, M.J.; de Siqueira, J.T.; Cestari, J.A.; de Siqueira, S.R. Oral infections and orofacial pain in Alzheimer’s disease: A case-control study. J. Alzheimers Dis. 2014, 38, 823–829. [Google Scholar] [CrossRef] [PubMed]
- Dintica, C.S.; Rizzuto, D.; Marseglia, A.; Kalpouzos, G.; Welmer, A.K.; Wårdh, I.; Bäckman, L.; Xu, W. Tooth loss is associated with accelerated cognitive decline and volumetric brain differences: A population-based study. Neurobiol. Aging 2018, 67, 23–30. [Google Scholar] [CrossRef] [PubMed]
- Ellefsen, B.; Holm-Pedersen, P.; Morse, D.E.; Schroll, M.; Andersen, B.B.; Waldemar, G. Assessing caries increments in elderly patients with and without dementia: A one-year follow-up study. J. Am. Dent. Assoc. 2009, 140, 1392–1400. [Google Scholar] [CrossRef]
- Hatipoglu, M.G.; Kabay, S.C.; Güven, G. The clinical evaluation of the oral status in Alzheimer-type dementia patients. Gerodontology 2011, 28, 302–306. [Google Scholar] [CrossRef]
- Hoben, M.; Poss, J.W.; Norton, P.G.; Estabrooks, C.A. Oral/dental items in the resident assessment instrument–minimum data set 2.0 lack validity: Results of a retrospective, longitudinal validation study. Popul. Health Metr. 2016, 14, 36. [Google Scholar] [CrossRef]
- Jones, J.A.; Lavallee, N.; Alman, J.; Sinclair, C.; Garcia, R.I. Caries incidence in patients with dementia. Gerodontology 1993, 10, 76–82. [Google Scholar] [CrossRef]
- Kato, H.; Takahashi, Y.; Iseki, C.; Igari, R.; Sato, H.; Sato, H.; Koyama, S.; Tobita, M.; Kawanami, T.; Iino, M.; et al. Tooth Loss-associated Cognitive Impairment in the Elderly: A Community-based Study in Japan. Intern. Med. 2019, 58, 1411–1416. [Google Scholar] [CrossRef]
- Ide, M.; Harris, M.; Stevens, A.; Sussams, R.; Hopkins, V.; Culliford, D.; Fuller, J.; Ibbett, P.; Raybould, R.; Thomas, R.; et al. Periodontitis and cognitive decline in Alzheimer’s disease. PLoS ONE 2016, 11, e0151081. [Google Scholar] [CrossRef]
- Ship, J.A.; Puckett, S.A. Longitudinal study on oral health in subjects with Alzheimer’s disease. J. Am. Geriatr. Soc. 1994, 42, 57–63. [Google Scholar] [CrossRef]
- Sumi, Y.; Ozawa, N.; Michiwaki, Y.; Washimi, Y.; Toba, K. Oral conditions and oral management approaches in mild dementia patients. Nihon Ronen Igakkai Zasshi 2012, 49, 90–98. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Takeuchi, K.; Ohara, T.; Furuta, M.; Takeshita, T.; Shibata, Y.; Hata, J.; Yoshida, D.; Yamashita, Y.; Ninomiya, T. Tooth Loss and Risk of Dementia in the Community: The Hisayama Study. J. Am. Geriatr. Soc. 2017, 65, e95–e100. [Google Scholar] [CrossRef] [PubMed]
- Yoo, J.J.; Yoon, J.H.; Kang, M.J.; Kim, M.; Oh, N. The effect of missing teeth on dementia in older people: A nationwide population-based cohort study in South Korea. BMC Oral Health 2019, 19, 61. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Zenthöfer, A.; Schröder, J.; Cabrera, T.; Rammelsberg, P.; Hassel, A.J. Comparison of oral health among older people with and without dementia. Community Dent. Health 2014, 31, 27–31. [Google Scholar]
- Zenthöfer, A.; Cabrera, T.; Rammelsberg, P.; Hassel, A.J. Improving oral health of institutionalized older people with diagnosed dementia. Aging Ment. Health 2016, 20, 303–308. [Google Scholar] [CrossRef]
- Chu, C.H.; Ng, A.; Chau, A.M.; Lo, E.C. Oral health status of elderly Chinese with dementia in Hong Kong. Oral Health Prev. Dent. 2015, 13, 51–57. [Google Scholar] [CrossRef]
- Rolim Tde, S.; Fabri, G.M.; Nitrini, R.; Anghinah, R.; Teixeira, M.J.; Siqueira, J.T.; Cesari, J.A.; Siqueira, S.R. Evaluation of patients with Alzheimer’s disease before and after dental treatment. Arq. Neuropsiquiatr. 2014, 72, 919–924. [Google Scholar] [CrossRef] [Green Version]
- Kossioni, A.E.; Kossionis, G.E.; Polychronopoulou, A. Oral health status of elderly hospitalised psychiatric patient. Gerodontology 2012, 29, 272–283. [Google Scholar] [CrossRef]
- Leal, S.C.; Bittar, J.; Portugal, A.; Falcão, D.P.; Faber, J.; Zanotta, P. Medication in elderly people: Its influence on salivary pattern, signs and symptoms of dry mouth. Gerodontology 2010, 27, 129–133. [Google Scholar] [CrossRef]
- Nordenram, G.; Ryd-Kjellen, E.; Johansson, G.; Nordstrom, G.; Winblad, B. Alzheimer’s disease, oral function and nutritional status. Gerodontology 1996, 13, 9–16. [Google Scholar] [CrossRef]
- Warren, J.J.; Chalmers, J.M.; Levy, S.M.; Blanco, V.L.; Ettinger, R.L. Oral health of persons with and without dementia attending a geriatric clinic. Spec. Care Dent. 1997, 17, 47–53. [Google Scholar] [CrossRef] [PubMed]
- Zenthöfer, A.; Baumgart, D.; Cabrera, T.; Rammelsberg, P.; Schröder, J.; Corcodel, N.; Hassel, A.J. Poor dental hygiene and periodontal health in nursing home residents with dementia: An observational study. Odontology 2017, 105, 208–213. [Google Scholar] [CrossRef] [PubMed]
- Adam, H.; Preston, A.J. The oral health of individuals with dementia in nursing homes. Gerodontology 2006, 23, 99–105. [Google Scholar] [CrossRef] [PubMed]
- Bomfim, F.M.S.; Chiari, B.M.; Roque, F.P. Fatores associados a sinais sugestivos de disfagia orofaríngea em idosas institucionalizadas. CoDAS 2013, 25, 154–163. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Chalmers, J.M.; Hodge, C.; Fuss, J.M.; Spencer, A.J.; Carter, K.D. The prevalence and experience of oral diseases in Adelaide nursing home residents. Aust. Dent. J. 2002, 47, 123–130. [Google Scholar] [CrossRef] [Green Version]
- Chapman, P.J.; Shaw, R.M. Normative dental treatment needs of Alzheimer patients. Aust. Dent. J. 1991, 36, 141–144. [Google Scholar] [CrossRef]
- Chen, X.; Clark, J.J.; Naorungroj, S. Oral health in older adults with dementia living in different environments: A propensity analysis. Spec. Care Dent. 2013, 33, 239–247. [Google Scholar] [CrossRef]
- Chen, X.; Clark, J.J.; Naorungroj, S. Oral health in nursing home residents with different cognitive statuses. Gerodontology 2013, 30, 49–60. [Google Scholar] [CrossRef]
- Chen, X.; Clark, J.J.; Chen, H.; Naorungroj, S. Cognitive impairment, oral self-care function and dental caries severity in community-dwelling older adults. Gerodontology 2015, 32, 53–61. [Google Scholar] [CrossRef] [Green Version]
- Cohen-Mansfield, J.; Lipson, S. The underdetection of pain of dental etiology in persons with dementia. Am. J. Alzheimers Dis. Other Demen. 2002, 17, 249–253. [Google Scholar] [CrossRef]
- Delwel, S.; Scherder, E.J.A.; de Baat, C.; Binnekade, T.T.; van der Wouden, J.C.; Hertogh, C.M.P.M.; Maier, A.B.; Perez, R.S.G.M.; Lobbezoo, F. Orofacial pain and its potential oral causes in older people with mild cognitive impairment or dementia. J. Oral Rhabilit. 2019, 46, 23–32. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ellefsen, B.; Holm-Pedersen, P.; Morse, D.E.; Schroll, M.; Andersen, B.B.; Waldemar, G. Caries prevalence in older persons with and without dementia. J. Am. Geriatr. Soc. 2008, 56, 59–67. [Google Scholar] [CrossRef] [PubMed]
- Ellefsen, B.S.; Morse, D.E.; Waldemar, G.; Holm-Pedersen, P. Indicators for root caries in Danish persons with recently diagnosed Alzheimer’s disease. Gerodontology 2012, 29, 194–202. [Google Scholar] [CrossRef] [PubMed]
- Elsig, F.; Schimmel, M.; Duvernay, E.; Giannelli, S.V.; Graf, C.E.; Carlier, S.; Herrmann, F.R.; Michel, J.P.; Gold, G.; Zekry, D.; et al. Tooth loss, chewing efficiency and cognitive impairment in geriatric patients. Gerodontology 2015, 32, 149–156. [Google Scholar] [CrossRef]
- Eshkoor, S.A.; Hamid, T.A.; Nudin, S.S.; Mun, C.Y. Association between dentures and the rate of falls in dementia. Med. Devices 2014, 7, 225–230. [Google Scholar] [CrossRef] [Green Version]
- Gil-Montoya, J.A.; Barrios, R.; Sánchez-Lara, I.; Carnero-Pardo, C.; Fornieles-Rubio, F.; Montes, J.; Gonzalez-Moles, M.A.; Bravo, M. Prevalence of drug-induced xerostomia in older adults with cognitive impairment or dementia: An observational study. Drugs Aging 2016, 33, 611–618. [Google Scholar] [CrossRef]
- Kossioni, A.E.; Kossionis, G.E.; Polychronopoulou, A. Self-reported oral complaints in older mentally ill patient. Geriatr. Gerontol. Int. 2013, 13, 358–364. [Google Scholar] [CrossRef]
- Furuta, M.; Komiya-Nonaka, M.; Akifusa, S.; Shimazaki, Y.; Adachi, M.; Kinoshita, T.; Kikutani, T.; Yamashita, Y. Interrelationship of oral health status, swallowing function, nutritional status, and cognitive ability with activities of daily living in Japanese elderly people receiving home care services due to physical disabilities. Community Dent. Oral Epidemiol. 2013, 41, 173–181. [Google Scholar] [CrossRef]
- Hopcraft, M.S.; Morgan, M.V.; Satur, J.G.; Wright, F.A.C. Edentulism and dental caries in Victorian nursing homes. Gerodontology 2012, 29, e512–e519. [Google Scholar] [CrossRef]
- Lee, K.H.; Wu, B.; Plassman, B.L. Cognitive function and oral health-related quality of life in older adults. J. Am. Geriatr. Soc. 2013, 61, 1602–1607. [Google Scholar] [CrossRef] [Green Version]
- Minakuchi, S.; Takaoka, S.; Shimoyama, K.; Uematsu, H. Factors affecting denture use in some institutionalized elderly people. Spec. Care Dent. 2006, 26, 101–105. [Google Scholar] [CrossRef] [PubMed]
- Philip, P.; Rogers, C.; Kruger, E.; Tennant, M. Oral hygiene care status of elderly with dementia and in residential aged care facilities. Gerodontology 2012, 29, e306–e311. [Google Scholar] [CrossRef] [PubMed]
- Ribeiro, G.R.; Costa, J.L.; Ambrosano, G.M.; Garcia, R.C. Oral health of the elderly with Alzheimer’s diseas. Oral Surg. Oral Med. Oral Pathol. Oral Radiol. 2012, 114, 338–343. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Srisilapanan, P.; Jai-Ua, C. Oral health status of dementia patients in Chiang Mai Neurological Hospital. J. Med. Assoc. Thai 2013, 96, 351–357. [Google Scholar]
- Syrjälä, A.-M.H.; Ylöstalo, P.; Ruoppi, P.; Komulainen, K.; Hartikainen, S.; Sulkava, R.; Knuuttila, M. Dementia and oral health among subjects aged 75 years or older. Gerodontology 2012, 29, 36–42. [Google Scholar] [CrossRef]
- Tiisanoja, A.; Syrjala, A.M.; Tertsonen, M.; Komulainen, K.; Pesonen, P.; Knuuttila, M.; Hartikainen, S.; Ylostalo, P. Oral disease and inflammatory burden and Alzheimer’s disease among subjects aged 75 years or older. Spec. Care Dent. 2019, 39, 158–165. [Google Scholar] [CrossRef]
- Fjeld, K.G.; Mowe, M.; Eide, H.; Willumsen, T. Effect of electric toothbrush on residents’ oral hygiene: A randomized clinical trial in nursing homes. Eur. J. Oral Sci. 2014, 122, 142–148. [Google Scholar] [CrossRef]
- American Psychiatric Association. Diagnostic and Statistical Manual of Mental Disorders, 4th ed.; Text. Revision DSM-IV-TR; American Psychiatric Association: Arlington, VA, USA, 2000. [Google Scholar]
- World Health Organization. ICD-10 International Statistical Classification of Diseases and Related Health Problems; WHO: Geneva, Switzerland, 2008. [Google Scholar]
- McKhann, G.M.; Knopman, D.S.; Chertkow, H.; Hyman, B.T.; Jack, C.R., Jr.; Kawas, C.H.; Klunk, W.E.; Koroshetz, W.J.; Manly, J.J.; Mayeux, R.; et al. The diagnosis of dementia due to Alzheimer’s disease: Recommendations from the National Institute on Aging-Alzheimer’s association workgroups on diagnostic guidelines for Alzheimer’s disease. Alzheimers Dement. 2011, 7, 263–269. [Google Scholar] [CrossRef] [Green Version]
- Folstein, M.F.; Folstein, S.E.; McHugh, P.R. Mini-mental state. J. Psychiatr. Res. 1975, 12, 189–198. [Google Scholar] [CrossRef]
- Morris, J.C. The clinical dementia rating (CDR): Current version and scoring rules. Neurology 1993, 43, 2412–2414. [Google Scholar] [CrossRef]
- Delwel, S.; Binnekade, T.T.; Perez, R.S.; Hertogh, C.M.; Scherder, E.J.; Lobbezzoo, F. Oral health and Orofacial pain in older people with dementia: A systematic review with focus on dental hard tissues. Clin. Oral Investig. 2017, 21, 17–32. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Weijenberg, R.A.F.; Delwel, S.; Ho, B.V.; van der Maarel-Wierink, C.D.; Lobbezoo, F. Mind your teeth-The relationship between mastication and cognition. Gerodontology 2019, 36, 2–7. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Delwel, S.; Scherder, E.J.A.; Perez, R.S.G.M.; Hertogh, C.M.P.M.; Maier, A.B.; Lobbezoo, F. Oral function of older people with mild cognitive impairment or dementia. J. Oral Rehabilit. 2018, 45, 990–997. [Google Scholar] [CrossRef] [PubMed]
- Jablonski, R.A.; Therrien, B.; Mahoney, E.K.; Kolanowski, A.; Gabello, M.; Brock, A. An intervention to reduce care-resistant behavior in persons with dementia during oral hygiene: A pilot study. Spec. Care Dent. 2011, 31, 77–87. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Willumsen, T.; Karlsen, L.; Naess, R.; Bjørntvedt, S. Are the barriers to good oral hygiene in nursing homes within the nurses or the patients? Gerodontology 2012, 29, e748–e755. [Google Scholar] [CrossRef] [PubMed]
- Delwel, S.; Binnekade, T.T.; Perez Roberto, S.G.; Hertogh, C.M.P.M.; Scherder, E.J.A.; Lobbezzoo, F. Oral hygiene and oral health in older people with dementia: A comprehensive review with focus on oral soft tissues. Clin. Oral Investig. 2018, 22, 93–108. [Google Scholar] [CrossRef] [PubMed] [Green Version]


{kind=link}
| Cohort Studies | Representativeness of Exposed Cohort | Selection of Non Exposed Cohort | Ascertainment of Exposure | Demonstration Outcome Not Present at Start of Study | Comparability | Outcome | Total |
|---|---|---|---|---|---|---|---|
| Chalmers et al. 2002 [21] | + | − | − | − | ++ | ++− | 5 |
| Chalmers et al. 2003 [13] | + | − | − | + | ++ | +++ | 7 |
| Chalmers et al. 2004 [22] | + | − | − | − | −− | ++− | 3 |
| Chen et al. 2010 [23] | + | + | + | − | −− | +++ | 5 |
| De Souza Rolim et al. 2014 [24] | + | − | + | − | −− | +−− | 3 |
| Dintica et al. 2018 [25] | + | − | + | + | ++ | +++ | 8 |
| Ellefsen et al. 2009 [26] | + | + | + | − | ++ | ++− | 7 |
| Hatipoglu et al. 2011 [27] | − | − | − | + | −− | ++ | 3 |
| Hoben et al. 2016 [28] | + | − | + | − | +− | ++ | 5 |
| Jones et al. 1993 [29] | + | − | − | + | ++ | ++− | 6 |
| Kato et al. 2019 [30] | + | − | + | + | +− | −++ | 6 |
| Ide et al. 2016 [31] | − | − | + | + | +− | +++ | 6 |
| Lee et al. 2017 [10] | + | + | + | − | ++ | +++ | 8 |
| Ship and Puckett 1994 [32] | + | + | + | − | +− | ++− | 6 |
| Sumi et al. 2012 [33] | + | − | + | − | −− | ++ | 4 |
| Takeuchi et al. 2017 [34] | + | − | + | − | ++ | +++ | 7 |
| Yoo et al. 2019 [35] | + | − | + | + | ++ | ++− | 7 |
| Zenthofer et al. 2014 [36] | − | − | + | + | −− | +++ | 5 |
| Zenthofer et al. 2016 [37] | + | + | + | + | ++ | +++ | 5 |
| Case-Control Studies | Definition of Cases | Representativeness of Cases | Selection of Controls | Definition of Controls | Comparability | Exposure | Total |
|---|---|---|---|---|---|---|---|
| Chu et al. 2015 [38] | − | + | − | + | ++ | +−− | 5 |
| De Souza Rolim et al. 2014 [39] | + | + | + | + | ++ | ++− | 8 |
| Gil–Montoya et al. 2017 [14] | + | + | − | + | ++ | −++ | 7 |
| Hoeksema et al. 2016 [19] | + | + | − | + | −− | −++ | 5 |
| Kossioni et al. 2012 [40] | + | + | − | − | ++ | ++− | 6 |
| Leal et al. 2010 [41] | − | + | − | + | −− | −++ | 4 |
| Nordenram et al. 1996 [42] | + | + | + | + | ++ | ++− | 8 |
| Warren et al. 1997 [43] | + | + | − | − | ++ | +++ | 7 |
| Zenthofer et al. 2017 [44] | + | + | + | − | ++ | −−+ | 6 |
| Cross-Sectional Studies | Representativeness of the Sample | Sample Size | Non-Respondents | Ascertainment of the Exposure | Comparability | Outcome | Total |
|---|---|---|---|---|---|---|---|
| Adam et al. 2006 [45] | − | + | + | − | −−- | +− | 3 |
| Bomfin et al. 2013 [46] | − | − | + | − | −− | − | 1 |
| Chalmers et al. 2002 [47] | − | + | + | − | −− | ++ | 4 |
| Chapman et al. 1991 [48] | − | + | − | − | −− | +−− | 2 |
| Chen et al. 2013 [49] | + | + | + | + | −− | ++− | 6 |
| Chen et al. 2013-2015 [50,51] | + | + | + | + | −− | −+ | 5 |
| Cohen-Mansfield 2002 [52] | − | − | − | − | −− | +−− | 1 |
| Delwel et al. 2019 [53] | + | + | + | + | ++ | +++ | 9 |
| Ellefsen et al. 2008-2012 [54,55] | + | + | + | − | ++ | ++− | 7 |
| Elsig et. Al. 2015 [56] | + | + | + | − | −− | ++− | 5 |
| Eshkoor et al. 2014 [57] | − | + | − | − | −− | −−− | 1 |
| Gil-Montoya et al. 2016 [58] | + | + | + | + | −− | ++ | 6 |
| Kossioni et al. 2013 [59] | + | − | + | −− | ++ | −+− | 5 |
| Furuta et al. 2013 [60] | − | + | − | − | ++ | ++− | 5 |
| Hopcraft et al. 2012 [61] | − | + | + | − | −− | ++− | 4 |
| Lee et al. 2013 [62] | + | − | − | + | +− | ++ | 5 |
| Luo et al. 2015 [20] | + | + | + | + | −+ | −++ | 7 |
| Minakuchi et al. 2006 [63] | + | + | − | + | +− | ++− | 6 |
| Philip et al. 2012 [64] | − | − | − | + | −− | ++− | 3 |
| Ribeiro et al. 2012 [65] | + | + | − | −− | ++− | 5 | |
| Srilapanan et al. 2013 [66] | − | + | − | − | −− | +−− | 2 |
| Syrjala et al. 2012 [67] | + | + | + | + | ++ | ++− | 8 |
| Tiisanoja et al. 2018 [68] | − | + | − | + | + | ++ | 5 |
| Randomized Clinical Trial | Definition | Representativeness of Cases | Selection of Controls | Definition of Controls | Comparability | Exposure | Total |
|---|---|---|---|---|---|---|---|
| Fjeld et al. 2014 [69] | + | − | + | + | +++ | 6 | |
| Zenthofer et al. 2016 [44] | + | + | − | − | ++ | +−− | 5 |
| Study | Design | Dementia Group | Mean Age | Control Group | Mean Age | Dementia and Oral Health Measure |
|---|---|---|---|---|---|---|
| Adam et al. 2006 [45] | Cross-sectional | 81 | 80.8 | 54 | 85.5 | Abbreviated Mental Test. Orofacial pain, dentures, edentulousness, DMFT, Debris Index |
| Bonfim et al. 2013 [46] | Cross-sectional | ? | ? | ? | ? | MMSE, chart, ADL. Number of present teeth, dentures |
| Chalmers et al. 2002 [21] | Cohort | 116 | 91: <79 years 25: 80+ years | 116 | 91: <79 years 25: 80+ years | MMSE. Number of present teeth, DMFT, root caries, Plaque Index |
| Chalmers et al. 2002 [47] | Cross-sectional | 224 | 83.2 | 0 | - | MMSE. Number of present teeth, DMFT, dentures, dental habits, coronal and root caries, retained roots |
| Chalmers et al. 2003 [13] | Cohort | 103 | 82: <79 years 21:80+ years | 113 | 88:<79 years 25:80+ years | MMSE. Number of present teeth, DMFT, coronal and root caries, Plaque Index |
| Chalmers et al. 2004 [22] | Cohort | 224 | 83.2 | 0 | - | MMSE. Orofacial pain, number of present teeth, DMFT, dental habits, number of coronal and root caries, retained roots |
| Chapman et al. 1991 [48] | Cross-sectional | 85 | 74.9 | 0 | - | Dementia measure not described. Number of present teeth, dentures, DMFT, Presence of deposits |
| Chen et al. 2010 [23] | Cohort | 119 | 81.5 | 372 | 73.8 | Chart. Present of calculus, plaque and gingival bleeding |
| Chen et al. 2013 [49] | Cross-sectional | Community: 51 Assisted living: 18 NHR: 501 | 79.3 | 0 | - | Chart, ICD-9. Number of present teeth, decay or retained roots, presence of calculus, plaque and gingival bleeding, need for oral care |
| Chen et al. 2013 [50] | Cross-sectional | 501 | 82.6 | 199 | 76.1 | Chart. Presence of calculus, plaque and gingival bleeding |
| Chen et al. 2015 [51] | Cross-sectional | 46 | 79.3 | 138 | 71.6 | Chart. Need for oral care |
| Chu et al. 2015 [38] | Case-control | 59 | 79.8 | 59 | 79.8 | Chart. DMFT, Community Periodontal Index, Salivary flow |
| Cohen-Mansfield 2002 [52] | Cross-sectional | 21 | 88.0 | 0 | - | MMSE, MDS-COGS. Number of broken or fractured teeth, caries, retained roots, dentures, presence of gingivitis and periodontal disease |
| De Souza Rolim et al. 2014 [24] | Case-control | 29 | 75.2 | 30 | 61.2 | NINCDS-ADRDA for AD, MMSE. Orofacial pain, DMFT, Gingival Bleeding Index, probing pocket depth, CAL, Plaque Index |
| De Souza Rolim et al. 2014 [39] | Case-control | 29 | 75.2 | 0 | - | NINCDS-ADRDA for AD, MMS Orofacial pain, DMFT, Gingival Bleeding Index, probing pocket depth, CAL, Plaque Index |
| Delwel et al. 2019 [53] | Cross-sectional | Dementia:303 MCI: 45 | - | - | MMS. Presence of orofacial pain using the OPS-NVI and self-reported pain, number of missing or restored teeth, coronal and root caries, retained roots, DPSI, Plaque Index of Silness and Loë, oral hygiene, oral mucosal lesions | |
| Ellefsen et al. 2008 [54] | Cross-sectional | AD:61 OD:26 | 82.8 81.5 | 19 | 79.8 | ICD-10. Coronal caries, root caries |
| Ellefsen et al. 2009 [26] | Cohort | AD:49 OD:15 | 83.6 81.3 | 13 | 79.9 | ICD-10. Number of present teeth, DMFT, CCI, NCI, ADJCI |
| Ellefsen et al. 2012 [55] | Cross-sectional | 61 | 82.8 | 0 | - | Number of present teeth, DMFT, coronal caries, root caries |
| Elsig et al. 2013 [56] | Cross-sectional | 29 | 82.5 | 22 | 81.9 | NPT, MMSE, CERAD, CDR. Number of present teeth, presence of visible dental plaque |
| Eshkoor et al. 2014 [57] | Cross-sectional | 1210 | 71.0 | 0 | - | MMSE. Presence of teeth or dentures |
| Fjeld et al. 2014 [69] | RCT | 159 | 85.5 | 43 | 88.5 | Evaluated by physician. Number of present teeth, Simplified Oral Hygiene Index, mouth dryness |
| Furuta et al. 2013 [60] | Cross-sectional | 204 | - | 82 | - | CDR. Number of present teeth, dentures |
| Gil-Montoya et al. 2016 [58] | Cross-sectional | MiD:73 MoD:66 SeD:36 | 76.4 77.6 80.4 | 156 | 77.4 | NINCDS-ADRDA. Drug-induced xerostomia |
| Gil-Montoya et al. 2017 [14] | Case-control | 133 | 80.0 | 324 | 79.8 | DSM-IVR, NINCDS-ADRDA. Plaque Index, Bleeding Index |
| Hatipoglu et al. 2011 [27] | Prospective-cohort | 31 | 67.6 | 47 | 65.3 | MMSE. Dentures, DMFT, oral hygiene status, mucosal pathology |
| Hoben et al. 2016 [28] | cohort | 1606 | 85.0 | 1105 | 83.4 | Chart. Presence of debris, of inflamed, swollen or bleeding gums, oral care by staff |
| Hoeksema et al. 2016 [19] | Case-control | 479 | 84.0 | 246 | 81.1 | MMSE. Visual plaque according to the score of Mombelli |
| Hopcraft et al. 2012 [61] | Cross-sectional | 510 | ? | 0 | - | Chart. Number of present teeth, DMFT, coronal caries, retained roots |
| Ide et al. 2016 [31] | Cohort | 59 | 77.6 | 0 | - | NINCDS-ADRDA. Presence of visible plaque, bleeding on probing, pocket depth, presence of moderate and severe periodontal disease (CDC/AAP criteria) |
| Jones et al. 1993 [29] | Cohort | 23 | 67.4 | 46 | 66.1 | Longitudinal study of dementia. Present Teeth, CCI, RCI |
| Kossioni et al. 2012 [40] | Case-control | 27 | 76.5 | 84 | - | DSM-IV. Number of present teeth, DMFT, presence of plaque or calculus, mucosal pathology |
| Kossioni et al. 2013 [59] | Cross-sectional | 23 | 76.3 | 0 | - | Mentally ill, including dementia. Mucosal complaints |
| Leal et al. 2010 [41] | Case-control | 20 | 69.6 | 20 | 68.3 | NPT, CDR, MMSE. Mucosal pathology, salivary flow |
| Lee et al. 2013 [62] | Cross-sectional | 19 | 83.9 | 169 | 77.4 | MCI, MiD, DSM-IV. Missing teeth, coronal and root caries, periodontal pocket depth, Plaque Index |
| Luo et al. 2015 [20] | Cross-sectional | 120 | 80.9 | 2389 | 70.0 | DSM-IV. Missing teeth |
| Minakuchi et al. 2006 [63] | Cross-sectional | 155 | 50 | COD by MHLW JP. Number of present teeth, dentures | ||
| Nordenram et al. 1996 [42] | Case-control | 40 | 87.0 | 40 | 87.0 | DSM-III-R, MMSE. Number of present teeth, dentures |
| Philip et al. 2012 [64] | Cross-sectional | 84 | 85.7 | 102 | 84.3 | Chart, ADLOH. DMFT, retained roots, degree of gingival inflammation, Plaque Index |
| Ribeiro et al. 2012 [65] | Cross-sectional | 30 | 79.1 | 30 | 67.8 | ICD-10, DSM-IV, MMSE, CDR. Number of present teeth, dentures, DMFT, Oral Health Index |
| Ship et al. 1994 [32] | Cohort | 21 | 64.0 | 21 | 65.0 | NINCDS-ADRDA, CT, MRI, PET, PT. Number of present teeth, DMFT, Change in gingival status, periodontal pocket depth, salivary flow |
| Srilapanan et al. 2013 [66] | Cross-sectional | 69 | 75.5 | 0 | - | Chart, MMSE. Dental Habits, number of present teeth, dentures, DMFT, caries, Community Periodontal Index, need for oral care |
| Sumi et al. 2012 [33] | Cohort | 10 | 77.7 | 0 | - | NINCD-ADRDA, MMSE. Number of present teeth, DMFT, Gingival Index, Plaque Index |
| Syrjala et al. 2012 [67] | Cross-sectional | 49 | 84.8 | 278 | 81.4 | DSM-III-R, DSM-IV, McKeith. Number of present teeth, dentures, number of teeth with periodontal pockets > 4 mm, presence of poor oral hygiene |
| Warren et al. 1997 [43] | Case-control | 45 | 81.6 | 133 | 80.3 | MMSE, chart, NT, scans. Number of present teeth, dental habits, coronal and root caries, dentures, modification of Gingival Index, modification of Debris Index, xerostomia, mucosal pathology |
| Zenthöfer et al. 2014 [36] | Cohort | 57 | 83.1 | 36 | 82.6 | MMSE, chart. Decayed and missing teeth, periodontitis, Gingival Bleeding Index, CPITN, Dental Hygiene Index, Plaque Control Record |
| Zenthöfer et al. 2016 [37] | Cohort | 33 | 81.7 | 60 | 83.4 | MMSE, chart. Missing teeth, Gingival Bleeding Index, CPITN, Plaque Control Record, mucosa pathology |
| Zenthöfer et al. 2016 [44] | RCT | 136 | 84.6 | 83 | 80.7 | MMSE. Gingival Bleeding Index, CPITN |
| Zenthöfer et al. 2017 [44] | Case-control | 136 | 84.6 | 83 | 80.7 | MMSE. Gingival Bleeding Index, CPITN |
| Study | Design | Dementia or Periodontal Disease Group | Mean Age | Control Group | Mean Age | Dementia and Oral Periodontal Disease Measure: |
|---|---|---|---|---|---|---|
| Dintica et al. 2018 [25] | Cohort | Free D: 2715 | - | - | Dementia incidence: DSM-IV, MMSE. | |
| Ide et al. 2016 [31] | Cohort | Mid to Mod: 60 30 men 30 women | 77.7 | - | - | Presence or absence of periodontal disease following CDC/AAP |
| Kato et al. 2019 [30] | Cohort | 210 Men: 103 Women: 107 | 78.1 +− 4.9 | - | - | Cochran-Armitage trend test Mann-Whitney U test Kruskal-Wallis test Spearman’s rank correlation test Student’s t-test |
| Lee et al. 2017 [10] | Cohort | PD: 3028 (54% male) | 72.4 | No PD: 3028 (54% male) | 72.4 | Dementia incidence: ICD-9-CM codes 523.3–5 |
| Takeuchi et al. 2017 [34] | Cohort | PD: 1566 (691 men and 875 women) | - | - | - | Dementia incidence: DSM-III, MMSE, HDS-R. |
| Tiisanoja et al. 2018 [68] | Cross-sectional | IG: 170 | 80.9 AD: 82.2 OD: 82.5 | - | - | DSM-IV, McKeith et al. MMSE. Structured oral examination examining number of teeth with periodontal pocket depth of 4 mm or more |
| Yoo et al. 2019 [35] | Cohort | TE: 104,903 | - | NE: 104,903 | - | Dementia incidence: Disease codes and definition codes associated with dementia |
| Study | Number of Present Teeth No Dementia | Number of Present Teeth Dementia | p Value: Dementia vs. No Dementia |
|---|---|---|---|
| Bomfin et al. 2013 [46] | 2.0 | 3.0 | - |
| Chalmers et al. 2002, 2003 [13,21,47] | 17.2 | 18.0 | >0.05 |
| Chapman et al. 1991 [48] | - | 12.8 | - |
| Chen et al. 2010 [23] | - | 18.2 community living 19.3 assisted living | - |
| Delwel et al. 2019 [53] | - | Dementia:18.0 MCI: 22.0 | 0.058 |
| Ellefsen et al. 2009 [26] | 20.2 | 17.3 AD 16.1 OD | ≤ 0.001 |
| Ellefsen et al. 2012 [55] | - | 16.5 | - |
| Elsig et al. 2013 [56] | 6.5 | 4.9 | 0.533 |
| Fjeld et al. 2013 [69] | 20.1 | 20.0 | - |
| Hopcraft et al. 2012 [61] | 14.6 | 0.7 | >0.05 |
| Jones et al. 1993 [29] | 18.2 | 17.9 | 0.90 |
| Kossioni et al. 2012 [40] | - | 4.4 | - |
| Ribeiro et al. 2012 [65] | Median 13.5 (0.0-28-0) | Median 1.0 (o.o-22-0) | 0.0004 |
| Srisilapanan et al. 2013 [66] | - | 19.5 | - |
| Sumi et al. 2012 [33] | - | 12.7 | - |
| Syrjala et al. 2012 [67] | 15.0 | 10.9 AD 7.8 VaD 1.7 OD | - |
| Warren et al. 1997 [43] | 13.0 | 10.0 AD 13.0 OD | p > 0.05 |
| Study | Coronal Caries No Dementia | Coronal Caries Dementia | Root caries no Dementia | Root Caries Dementia | Retained Roots no Dementia | Retained Root Dementia |
|---|---|---|---|---|---|---|
| Chalmers et al. 2002–2003 [13,47] | 0.0 * | * 0 ** 5 | 0.3 | 0.8 | Decayed: 0.0 * Sound: 0.1 | Decayed: 0.3 * Sound: 0.1 |
| De Souza Rolim et al. 2014 [24,39] | 3.4% | 6.8% | - | - | 10.2% | 6.8% |
| Delwel et al. 2019 [53] | - | 27.0% | - | 19.0% | - | 18.1% |
| Ellefsen et al. 2008–2012 [54,55] | 1.0 * | 2.9 * | 1.7 * | 4.9 * AD 2.3 * OD | 0.0 | AD 10.0 * OD 0.5 * |
| Jones et al. 1993 [29] | 0.8 | 1.4 | 0.4 | 1.8 | - | - |
| Lee et al. 2013 [62] | 0.8 | 1.0 | 0.5 * | 1.8 * | - | - |
| Philip et al. 2012 [64] | - | - | - | - | 1.2 | 1.8 |
| Warren et al. 1997 [43] | 0.4 | AD 0.1 OD 0.4 | 0.8 | AD O.6 OD 0.6 | - | - |
| Study | DMFT No Dementia | DMFT Dementia |
|---|---|---|
| Adam et al. 2006 [45] | Decayed 1.1 Missing 28.2 Filled 0.7 | Decayed 0.80 Missing 27.3 Filled 0.90 |
| Chalmers et al. 2002 [21,47] | Decayed 0.0–0.4 Missing – Filled 24.7–25.7 | Decayed 0.5–1.6 * Missing – Filled 22.1-23.9 |
| Chalmers et al. 2003 [13] | Decayed 0.0–0.1 Missing - Filled - | Decayed 0.3–1.3 * Missing - Filled - |
| Chapman et al. 1991 [48] | Decayed - Missing - Filled - | Decayed 1.4 Missing 17.8 Filled 6.4 DMFT 25.6 |
| Chen et al. 2013 [49,50] | Decayed - Missing - Filled - | Decayed 5.5 (C), 5.3 (A), 6.0 (NHR) Missing - Filled 10.4 (C), 10.9 (A), 8.7 (NHR) |
| Chu et al. 2015 [38] | Decayed 0.8 Missing 18.3 Filled 2.4 DMFT 21.5 | Decayed 1.2 Missing 18.9 Filled 2.5 DMFT 22.3 |
| De Souza Rolim et al. 2014 [24,39] | Decayed - Missing - Filled - | Decayed - Missing - Filled – DMFT 27.2 Range 11–32 |
| Hatipoglu et al. 2011 [27] | Decayed Missing Filled DMFT 19.7 | Decayed Missing Filled DMFT 24.2 |
| Hopcraft et al. 2012 [61] | Decayed 2.9 Missing 17.4 Filled 4.8 DMFT 25.0 | Decayed 2.4 Missing 17.9 Filled 4.8 DMFT 25.0 |
| Kossioni et al. 2012 [40] | Decayed - Missing - Filled - | Decayed 1.8 Missing - Filled 0.9 |
| Lee et al. 2013 [62] | Decayed CC+RC Missing 12.7 Filled - | Decayed CC+RC Missing 10.2 Filled - |
| Luo et al. 2015 [20] | Decayed - Missing 9.3 Filled - | Decayed - Missing 18.7 ** Filled - |
| Philip et al. 2012 [64] | Decayed 2.9 Missing 18.0 Filled 5.0 DMFT 26.1 | Decayed 3.0 Missing 17.4 Filled 5.3 DMFT 25.9 |
| Ribeiro et al. 2012 [65] | Decayed Missing Filled DMFT 25.5 * | Decayed Missing Filled DMFT 28.0 * |
| Srisilapanan et al. 2013 [66] | Decayed - Missing - Filled - | Decayed 1.5 Missing 12.6 Filled 0.8 DMFT 14.9 |
| Zenthöfer et al. 2014 [36] | Decayed 0.7 Missing 19.9 Filled - | Decayed 0.6 Missing 20.8 Filled - |
| Zenthöfer et al. 2016 [37] | Decayed - Missing 20.5 Filled - | Decayed - Missing 20.5 Filled - |
| Study | Outcome Measure | Gingival Health No Dementia | Gingival Health Dementia |
|---|---|---|---|
| Chen et al. 2010 [23] | Calculus/plaque/gingival bleeding | No: 1.2% M to M: 85.5% High: 13.3% | No: 0.9% M to M: 67.9% High: 31.3% |
| Chen et al. 2013 [49] | Calculus/plaque/gingival bleeding | - | C: 0% No, 65.8% Small, 34.2 High A: 8.3% No, 66.7% Small, 25.0% High NHR: 59.2% No, 59.2% Small, 40.5% High |
| Chen et al. 2013 [50] | Calculus/plaque/gingival bleeding | No:0.0% M to M: 73.8% ** High: 26.2% | No: 0.3% M to M: 59.2% High:40.4% |
| Chu et al. 2015 [38] | Community Periodontal Index, pockets ≥ 3 mm | 74.0% | 78.0% |
| Cohen-Mansfield et al. 2002 [52] | Periodontal disease Gingivitis | - | 44.4% 38.9% |
| De Souza Rolim et al. 2014 [24] | Probing pocket depth (mm) Gingivitis MoD-SeV periodontitis Periodontal infection Gingival Bleeding Index | - 10.0%-10.0% 6.7% 26.7% - | 1.6 mm 31.0% 6.9%–20.7% 58.6 ** 46.0% |
| De Souza Rolim et al. 2014 [39] | Probing pocket depth (mm) Gingivitis MoD-SeV periodontitis Periodontal infection Gingival Bleeding Index | - 10.0%–10.0% 6.7% 26.7% - | 1.6 mm 31.0% 6.9%–20.7% 58.6 ** 46.0% |
| Delwel et al. 2019 [53] | Silness and Loë Plaque Index DPSI Probing pocket depth (mm) Mobility grade | 2.0 3- (IQR = 2.4) ≥4 mm in 73.8% participants Grade 2 in18.8% Grade 3 in 5.8% | |
| Gil-Montoya et al. 2016 [58] | Bleeding Index | 50.6 | 67.5 *** |
| Hoben et al. 2016 [28] | Inflamed, swollen or bleeding gums | 1.2% | 0.8% |
| Hopcraft et al. 2012 [61] | Periodontal pocket depth 4 mm, periodontal pocket depth > 6 mm | 35.0% | 36.0% |
| Ide et al. 2016 [31] | Probing depth > 3 mm Bleeding on probing Periodontitis according to CDC/AAP criteria: MoD-SeV | 6.7% 13.6% 37.3 25.4%–1.9% | |
| Lee et al. 2013 [62] | Periodontal pocket depth | 1.5 mm | 1.4 mm |
| Philip et al. 2012 [64] | Gingival inflammation: Minimal: Light: Moderate: | 22.5% 36.3% 32.5% 6.8% | 13.0% 21.0% 56.5% 13.0% |
| Sumi et al. 2012 [33] | Gingival Index Loe-Silness | - | 1.2 |
| Srisilapanan et al. 2013 [66] | Community Periodontal Index, highest score: Normal Bleeding Calculus Pocket depth 4–5 mm Pocket depth ≥ 6 mm | - - - - - | 9.4% 1.9% 34.0% 30.2% 24.5% |
| Syrjala et al. 2012 [67] | Number of teeth with periodontal pockets | 2.8 AD 2.8 VaD 1.7 OD | |
| Warren et al. 1997 [43] | Modified version of Gingival Index by Silness and Loe | 0.7 | 1.1 AD 1.2 0.9 OD |
| Zenthöfer et al. 2014 [36] | Periodontitis Gingival Bleeding Index Community periodontal index of treatment needs | 73.9% 40.9% 2.8 | 100% *** 43.8% 3.4 *** |
| Zenthöfer et al. 2016 [37] | Gingival Bleeding Index Community periodontal index of treatment needs | 38.1% 3.1 | 52.1% * 3.3 |
| Zenthöfer et al. 2016 [44] | Community periodontal index of treatment needs | 2.7 | 3.1 *** |
| Zenthöfer et al. 2017 [44] | Gingival Bleeding Index Community periodontal index of treatment needs | 48.8% 2.7 | 53.8% 3.1 *** |
| Study | Dentures no Dementia | Dentures Dementia | Edentulousness No Dementia | Edentulousness Dementia |
|---|---|---|---|---|
| Adam et al. 2006 [45] | / | / | 70.0% | 63.0% |
| Bomfim et al. 2013 [46] | 20.0% | 20.0% | 46.7% | 40.0% |
| Chalmers et al. 2003 [13] | 27.6-30.1% | 20.7-23.3% | / | / |
| Chapman et al. 1991 [48] | - | 59.0% | - | 64.7% |
| Chen et al. 2013 [49] | - | 48.0% C 38.9% A 47.1% NHR | / | / |
| Chu et al. 2015 [38] | 14.0% | 17.0% | / | / |
| De Souza Rolim et al. 2014 [24] | 43.3% | 25.8% | 43.3% | 32.3% |
| Elsig et al. 2013 [56] | / | / | 54.6% | 62.1% |
| Eshkoor et al. 2014 [57] | 81.8% | 86.2% | / | / |
| Hatipoglu et al. 2011 [27] | 57.0% Max 55.0% Mand | 97.0% Max 100.0% Mand | / | / |
| Kossioni et al. 2012 [40] | - | 62.9% | ||
| Nordenram et al. 1996 [42] | 17.0% | 7.0% Mod 5.0% Sed | 43.0% | 36.0% MoD 45.0% SeD |
| Ship et al. 1994 [32] | 43.0% | 40.0-67.0% | / | / |
| Srisilapapanan et al. 2013 [66] | - | 40.6% | - | 11.6% |
| Syrjala et al. 2012 [67] | 73.7% | 75.5% AD 68.6% VaD 72.2% OD | 44.6% | 63.3% AD 68.8% VaD 72.7% OD |
| Warren et al. 1997 [43] | / | / | 31.6% | 40.0% AD 32.0% OD |
| Study | Orofacial Pain No Dementia | Orofacial Pain Dementia |
|---|---|---|
| Adam et al. 2006 [45] | 18.5% | 7.4% |
| Chalmers et al. 2003 [13] | 11.2–11.5% | 18.4–19.0% |
| Cohen-Mansfield et al. 2002 [52] | - | 60.0% |
| De Souza Rolim et al. 2014 [24] | 6.7% | 20.7% |
| Delwel et al. 2019 [53] | - | Dementia: 27.4% MCI: 20.5% |
| Kossioni et al. 2012 [40] | - | 21.7% |
| Study | Follow-Up Period | Association between Tooth Loss/Periodontal Disease and Dementia |
|---|---|---|
| Dintica et al. 2018 [25] | 9 years | Annual mean change in MMSE by tooth loss: −0.94 to −0.37 * |
| Ide et al. 2016 [31] | 6 months | Mean change in MMSE by the presence of periodontal disease: −3.6 to −0.03 −3.6 to 0.04 *** |
| Kato et al. 2019 [30] | 4 years | Cochran-Armitage trend test Mann-Whitney U test Kruskal-Wallis test Spearman’s rank correlation test Student’s t-test |
| Lee et al. 2017 [10] | Index date: date of the first periodontal disease diagnosis. Patients were followed until dementia diagnosis, death, withdrawal from the NHI or December 31, 2012 | Hazard ratio of having dementia in persons with periodontal disease → HR: 1.02–1.32 1.01–1.32 ** |
| Takeuchi et al. 2017 [34] | 5 years | Hazard ratio of having dementia in persons with 10-19 remaining teeth → HR: 1.45–3.03 1.06–2.46 *** |
| Tiisanoja et al. 2018 [68] | Risk of having AD in persons with pocket depth ≥ 4 mm → RR: 1.54 | |
| Yoo et al. 2019 [35] | 7 year | Odds Ratio of having dementia in persons with 7–12 teeth lost → OR: 1.272 |
© 2019 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Lauritano, D.; Moreo, G.; Della Vella, F.; Di Stasio, D.; Carinci, F.; Lucchese, A.; Petruzzi, M. Oral Health Status and Need for Oral Care in an Aging Population: A Systematic Review. Int. J. Environ. Res. Public Health 2019, 16, 4558. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph16224558
Lauritano D, Moreo G, Della Vella F, Di Stasio D, Carinci F, Lucchese A, Petruzzi M. Oral Health Status and Need for Oral Care in an Aging Population: A Systematic Review. International Journal of Environmental Research and Public Health. 2019; 16(22):4558. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph16224558
Chicago/Turabian StyleLauritano, Dorina, Giulia Moreo, Fedora Della Vella, Dario Di Stasio, Francesco Carinci, Alberta Lucchese, and Massimo Petruzzi. 2019. "Oral Health Status and Need for Oral Care in an Aging Population: A Systematic Review" International Journal of Environmental Research and Public Health 16, no. 22: 4558. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph16224558