Understanding the Experience and Needs of School Counsellors When Working with Young People Who Engage in Self-Harm


Abstract
:1. Introduction
2. Methods
2.1. Study Design
2.2. Participants
2.3. Procedure
2.4. Analysis
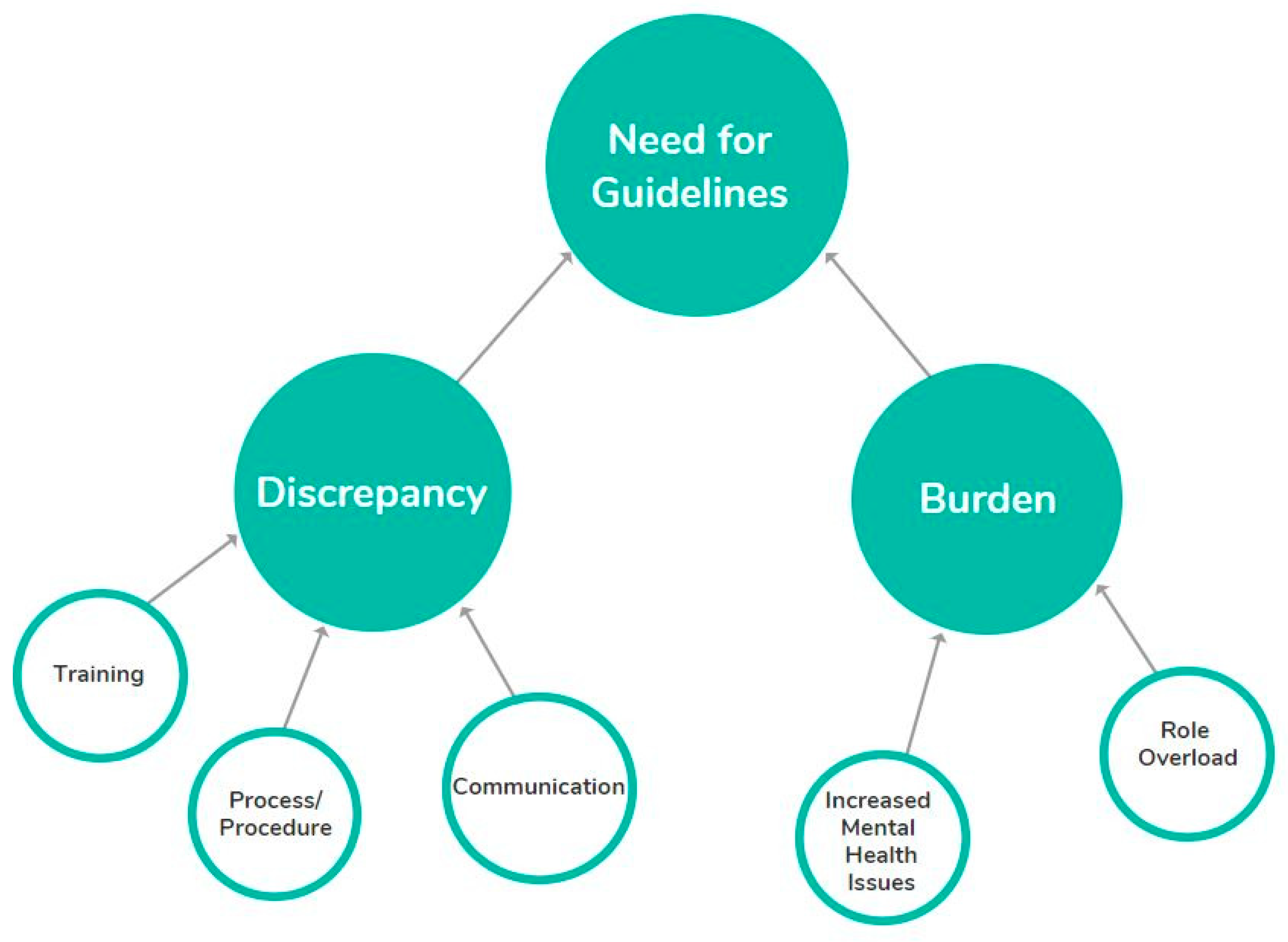
3. Results
3.1. Theme 1: Burden
3.1.1. Subtheme 1: Increased Mental Health Issues
“I’d say more suicide ideation and less self-harm at the moment anyway”[Interview 5]
“I think definitely that self-harm has become more prevalent perhaps”[Interview 18]
“And I do think that the level of anxiety and depression is really, um, increased because of societal pressure…”[Interview 13]
“there will be a group of ten kids talking about some, something on social media about kids cutting themselves and how you do it”[Interview 26]
“It’s just connections on their phone or whatever but no real friends”[Interview 21]
3.1.2. Subtheme 2: Role Overload
“There’s too many people coming through the door”[Interview 11]
“Our biggest gripe here is that we’re understaffed”[Interview 5]
“Someone improves and they’re okay, and then you have another 10 referrals waiting”[Interview 32]
“I got a text message when I was out doing something else. Just like I’ve cut myself and I’ve taken a whole lot of pills”[Interview 3]
“…well, sorry you don’t even get in my door unless there’s something much more specific going on”[Interview 13]
3.2. Theme 2: Discrepancy—Differences in the Way That Self-Harm is Managed
3.2.1. Subtheme 1: Training
“I don’t remember anything on self-harm”[Interview 6]
“…not a single mention of it in 2 years training as a guidance counsellor”[Interview 14]
“…none to very little, I can’t even remember. I would say it was none”[Interview 20]
“I wouldn’t say we got any specific training in self-harm…. A lot of my training has come through external training from my [previous job]”[Interview 31]
“I guess I just really relied on supervision and talking about it”[Interview 3]
“…so, I watched her and I picked up what she said and what she did”[Interview 20]
“There have been a couple of really good workshop seminar days on suicide risk assessment and that’s been very good, but then also I’ve just kind of done my own thing”[Interview 20]
“I can go to a really good supervisor you know, but I know it’s all private and state schools are all challenged by budgets”[Interview 26]
“We do a presentation in the staff room to all staff around high risk and uh issues of depression and also suicidality or the possibility of suicidality”[Interview 22]
“Meet with all the new stuff at the start of every year and explain what we do here and the services we have”[Interview 20]
“we do keep a running roll of people that have been referred to us or we suspect are at risk of serious self-harm…and we gauge the risk level at low, medium, or high depending on who they are, whether they’re had a connection with someone who has taken their life, or if they have self-harmed in the past. Or their personal circumstances at home.”[Interview 31]
“I think parents just have no idea, they just have no idea…It’s all, it’s either we don’t want to think about this or we’re going to take complete control of it”[Interview 10]
“If you actually allow skills around parenting….to communicate that to the children to self-regulate”[Interview 22]
“I had a [ethnicity] parent last term, you know your child is suicidal, she tried to commit suicide last year mum says oh I just don’t believe”[Interview 14]
“I don’t have capacity to work with the parents as well, yeah. So that’s, part of, a rock and a hard place with that at the moment. Seeing that yes, they need to be part of the conversation, don’t know how to do that well”[Interview 10]
3.2.2. Subtheme 2 Process/Procedure
“The deputy principal is somehow supposed to assess risk of which they’re not trained to assess”[Interview 19]
“So, every young person gets exactly the same questions I think that’s really important. Can I say while this is being recorded it would be so good if nationwide everybody did the same assessment”[Interview 20]
“I make a distinction in my own head, with the client, between self-harm and suicide risk”[Interview 23]
“I might use a tool maybe an anxiety scale or a depression scale”[Interview 26]
“The questionnaire then identifies a group of high-risk students, medium risk, low risk”[Interview 12]
“…like, yeah, level of safety is an issue like in terms of whether confidentiality gets broken or not”[Interview 26]
“So, there have been times when I will not disclose that to a family member if they’re over 16”[Interview 15]
“So, my confidentiality is really high unless it’s immediate, imminent risk…Uh… having said that, seeing year seven and eight’s … I’m just like actually you’re so young that I’m going to have to have a conversation with them around actually we need your parents involved in this”[Interview 10]
“We would be a little less willing to sit on disclosure around self-harm, though we do make a distinction between self-harm disclosure and suicidality”[Interview 22]
“Confidentiality breaching that has to happen at times inevitably puts your relationship is at risk. Our relationship stays more protected if the nurse does the informing of family as an accompli without negotiating with the student”[Interview 12]
“The kids get the confidentiality speech, so do the staff if they come in”[Interview 23]
“If they’ve got a plan for suicide always refer on, if they don’t have a plan still might refer on depending on history and self-harm, but there is not always a need to refer. But in both cases always call home”[Interview 20]
“We do a referral, um… sometimes it’s very difficult, um, to get it to stick because, um, the students have an ongoing relationship with us”[Interview 5]
“We’ve got a referral form that the teachers use, so they have to fill that in and email that to me”[Interview 20]
“…cutting that needs addressing, you need to get the nurses involved and the nurses and you work collaboratively and if [student] presented to you and the trust’s there, you’re the lead so I’ve created the lead caregiver… a lead caregiver which is defined in this stage by relationship to child”[Interview 1]
“But many of the nurses that come newer to our departments will engage in counselling. And where I sit, I think it’s very unhelpful….it needs to be done by a counsellor who has the skill …”[Interview 12]
“Students had to have self-harm incidences or scratches or whatever covered…but I just read that isn’t the recommended process and procedures”[Interview 18]
“If someone has presented that has been harming. The focus is on what that harm is and how serious it is. Our nurse is usually very good at drawing information out and being compassionate when she is dealing with that, in the moment, the counsellors deal with the aftermath, if you like, after the initial situation.”[Interview 31]
“And students are not shocked by that because we talk about suicidal thoughts very openly at the beginning of their life at the school, they all get this workshop on suicidal thought”[Interview 12]
3.2.3. Subtheme 3 Communication
“Collegiality between the nurses and the other counsellor is absolutely essential”[Interview 22]
“We (pastoral care) then try to consult with our nursing team…they don’t want to participate in our approach”[Interview 12]
“I set up a bit of a formulaic email, which is good, just to alert to the Dean”[Interview 23]
“Grounds-staff emailed me about three weeks ago and says oh there’s this boy…”[Interview 4]
“Teachers had noticed things but hadn’t feed it back to us”[Interview 11]
“We started an online referral form this year for staff. Um and that has just short circuited all those passing corridor conversations”[Interview 10]
“Yeah, trust us, we’re the professionals, we’re the trained psychologists… um… and we’ve made an assessment and this person isn’t at risk. Whereas we’re the ones that have had lots and lots of in depth conversations with them”[Interview 5]
“If we’re not informed of the plan, we can’t help them… um… also vice versa”[Interview 6]
“I feel like that work is paying off and there is a widening and there is a more collaborative approach”[Interview 19]
“They’re much slower to pick up. But it’s changed, I mean one time I could say really great things…and then other times…there will be a move of staff and then they’ve changed practices and procedures”[Interview 21]
“Our school policy says…they’ve been self-harming and they’ve just cut themselves…and their family are called and asked to come and take them home”[Interview 13]
“I will hold something before I take it to senior management because they’ll always be “let’s call whānau” and sometimes that actually makes a situation bigger… I don’t think there needs to be immediate family involvement[Interview 11]
“We do make a distinction between self-harm disclosure and suicidality disclosure…we wouldn’t necessarily disclose to parents about self-harm”[Interview 22]
3.3. Theme 3: Need for Guidelines
3.3.1. Subtheme 1: Positive Views about the Need for Guidelines
“Situations are not clear cut and guidelines are really helpful to go back and have something that you’re concretely measuring up against to help you work your way through to best practice”[Interview 13]
“Young people need to know that wherever they go they’re going to get the same care… And the same questioning and the same assessment and that bothers me that they don’t at this stage.”[Interview 20]
“Young people need to know that wherever they go they’re going to get the same care… And the same questioning and the same assessment and that bothers me that they don’t at this stage.” [Interview 20] “That’s where a guideline would come in like as a checkbox like have you thought of this, this, this, this, this. We can actually work your way through because it can be quite an intense thing depending on the time, depending on the situation”[Interview 3]
“We realized that that wasn’t really any process for how to deal with it at our school. So, I went online to see what I could track down…the ones for managing traumatic events for schools are like the encyclopedia Britannica. You know it’s too long, too complicated…you’ve got to have it simple so you can use it”[Interview 32]
3.3.2. Subtheme 2: Lack Utilization of Guidelines
“I know about our schools’ ones, I don’t know about, um, beyond our school”[Interview 13]
“I eventually got that training through the Ministry of Health uh Education whereby they had that little wee book”[Interview 22]
“I feel the NZAC, my professional body, if I wish to, I’ll go to them for and they will point me in the right direction”[Interview 23]
There isn’t like a formal process written down anywhere”[Interview 5]
“One of the areas that suffered is that there aren’t protocols here….”[Interview 1]
3.3.3. Subtheme 3: Need Flexibility
“I think really it’s about having the student at the center of it really and I sometimes think that that gets a bit lost when it comes to procedures and policies”[Interview 18]
“I always feel that it is a case-by-case, I really feel that. So, I don’t know how I would go with protocols but they are as you say they guidelines”[Interview 14]
“[guidelines] would be really useful because then it becomes a bottom line and then the school can adjust to their school needs”[Interview 26]
4. Discussion
4.1. How This Relates to Other Studies/Previous Literature
4.2. Limitations
4.3. Implications for Research and Practice
5. Conclusions
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- Hawton, K.; Hall, S.; Simkin, S.; Bale, L.; Bond, A.; Codd, S.; Stewart, A. Deliberate self-harm in adolescents: A study of characteristics and trends in Oxford, 1990–2000. J. Child. Psychol. Psychiatry 2003, 44, 1191–1198. [Google Scholar] [CrossRef]
- Mercado, M.C.; Holland, K.; Leemis, R.W.; Stone, D.M.; Wang, J. Trends in emergency department visits for nonfatal self-inflicted injuries among youth aged 10 to 24 years in the United States, 2001–2015. JAMA 2017, 318, 1931–1933. [Google Scholar] [CrossRef]
- Cavanagh, J.T.O.; Carson, A.J.; Sharpe, M.; Lawrie, S.M. Psychological autopsy studies of suicide: A systematic review. Psychol. Med. 2003, 33, 395–405. [Google Scholar] [CrossRef] [PubMed]
- Suominen, K.; Isometsa, E.; Suokas, J.; Haukka, J.; Achte, K.; Lonnqvist, J. Completed suicide after a suicide attempt: A 37-year follow-up study. Am. J. Psychiatry 2004, 161, 562–563. [Google Scholar] [CrossRef] [PubMed]
- Robinson, J. Repeated self-harm in young people: A review. Australas. Psychiatry 2016, 25, 105–107. [Google Scholar] [CrossRef] [PubMed]
- Robinson, J.; McCutcheon, L.; Browne, V.; Witt, K. Looking the Other Way: Young People and Self-Harm; Orygen, The National Centre of Excellence in Youth Mental Health: Melbourne, Australia, 2016. [Google Scholar]
- Mars, B.; Heron, J.; Crane, C.; Hawton, K.; Lewis, G.; Macleod, J.; Tilling, K.; Gunnell, D. Clinical and social outcomes of adolescent self harm: Population based birth cohort study. BMJ 2014, 349, g5954. [Google Scholar] [CrossRef]
- Martin, G.; Swannell, S.V.; Hazell, P.L.; Harrison, J.E.; Taylor, A.W. Self-injury in Australia: A community survey. Med J. Aust. 2010, 193, 506–510. [Google Scholar] [CrossRef] [PubMed]
- Fleming, T.M.; Clark, T.; Denny, S.; Bullen, P.; Crengle, S.; Peiris-John, R.; Robinson, E.; Rossen, F.V.; Sheridan, J.; Lucassen, M. Stability and change in the mental health of New Zealand secondary school students 2007–2012: Results from the national adolescent health surveys. Aust. New Zealand J. Psychiatry 2014, 48, 472–480. [Google Scholar] [CrossRef]
- UNICEF Office of Research. Building the Future: Children and the Sustainable Development Goals in Rich Countries, Innocenti Report Card 14; UNICEF Office of Research—Innocenti: Florence, Italy, 2017. [Google Scholar]
- Clark, T.; Fleming, T.; Bullen, P.; Denny, S.; Crengle, S.; Dyson, B.; Fortune, S.; Lucassen, M.; Peiris-John, R.; Robinson, E.M. Youth’12 Overview: The Health and Wellbeing of New Zealand Secondary School Students in 2012; University of Auckland, Faculty of Medical and Health Sciences: Auckland, New Zealand, 2013. [Google Scholar]
- Garish, J.A.; Wilson, M. Prevalence, correlates, and prospective predictors of non-suicidal self-injury among New Zealand adolescents: Cross-sectional and longitudinal survey data. Child Adolesc. Psychiatry Ment. Health 2015, 9, 28. [Google Scholar] [CrossRef]
- Robinson, J.; Too, L.S.; Pirkis, J.; Spittal, M. Spatial suicide clusters in Australia between 2010 and 2012: A comparison of cluster and non-cluster among young people and adults. BMC Psychiatry 2016, 16, 417. [Google Scholar] [CrossRef]
- Chan, S.; Denny, S.; Fleming, T.; Fortune, S.; Peiris-John, R.; Dyson, B. Exposure to suicide behaviour and individual risk of self-harm: Findings from a nationally representative New Zealand high school survey. Aust. New Zealand J. Psychiatry 2017, 52, 349–356. [Google Scholar] [CrossRef] [PubMed]
- Robinson, J.; Pan Yuen, H.; Martin, C.; Hughes, A.; Baksheev, G.N.; Dodd, S.; Bapat, S.; Schwass, W.; McGorry, P.; Yung, A.R. Does screening high school students for psychological distress, deliberate self-harm or suicidal ideation cause distress and is it acceptable? An Australian based study. Crisis J. Crisis Interv. Suicide Prev. 2011, 32, 254–263. [Google Scholar] [CrossRef] [PubMed]
- Robinson, J.; Hetrick, S.; Cox, G.; Bendall, S.; Yuen, H.P.; Yung, A.; Pirkis, J. Can an internet-based intervention reduce suicidal ideation, depression and hopelessness among secondary school students: Results from a pilot study. Early Interv. Psychiatry 2016, 10, 28–35. [Google Scholar] [CrossRef] [PubMed]
- Kong, L.; Sareen, J.; Katz, L.Y. School-Based Suicide Prevention Programs. In International Handbook of Suicide Prevention, 2nd ed.; O’Connor, R., Pirkis, J., Eds.; John Wiley & Sons, Ltd.: Chichester, UK, 2016; pp. 725–742. [Google Scholar]
- Fortune, S.; Sinclair, J.; Hawton, K. Adolescents’ views on preventing self-harm. Soc. Psychiatry Psychiatr. Epidemiol. 2008, 42, 96–104. [Google Scholar] [CrossRef] [PubMed]
- Jarvi, S.; Jackson, B.; Swenson, L.; Crawford, H. The Impact of Social Contagion on Non-Suicidal Self-Injury: A Review of the Literature. Arch. Suicide Res. 2013, 17, 1–19. [Google Scholar] [CrossRef]
- Evans, R.; Hurrell, C. The role of schools in children and young people’s self-harm and suicide: Systematic review and meta-ethnography of qualitative research. BMC Public Health 2016, 16, 401. [Google Scholar] [CrossRef]
- Michelmore, L.; Hindley, P. Help-Seeking for Suicidal Thoughts and Self-Harm in Young People: A Systematic Review. Suicide Life Threat. Behav. 2012, 42, 507–524. [Google Scholar] [CrossRef]
- Ystgaard, M.; Arensman, E.; Hawton, K.; Madge, N.; van Heeringen, K.; Hewitt, A.; De Wilde, E.J.; De Leo, D.; Fekete, S. Deliberate self-harm in adolescents: Comparison between those who receive help following self-harm and those who do not. J. Adolesc. 2009, 32, 875–891. [Google Scholar] [CrossRef]
- Robinson, J.; Gook, S.; Yuen, H.P.; Hughes, A.; Dodd, S.; Bapat, S.; Schwass, W.; McGorry, P.; Yung, A. Depression education and identification in schools: An Australian based study. Sch. Ment. Health 2010, 2, 13–22. [Google Scholar] [CrossRef]
- Denny, S.; Grant, S.; Galbreath, R.; Clark, T.C.; Fleming, T.; Bullen, P.; Dyson, B.; Crengle, S.; Fortune, S.; Peiris-John, R.; et al. Health Services in New Zealand Secondary Schools and the Associated Health Outcomes for Students; University of Auckland: Auckland, New Zealand, 2014. [Google Scholar]
- Pascall, M.J.; Bersamin, M. School-Based Health Centers, Depression, and Suicide Risk Among Adolescents. Am. J. Prev. Med. 2018, 54, 44–50. [Google Scholar] [CrossRef]
- Robinson, J.; Calear, A.L.; Bailey, E. Suicide prevention in educational settings: A review. Australas. Psychiatry 2018, 26, 132–140. [Google Scholar] [CrossRef] [PubMed]
- Robinson, J.; Bailey, E.; Witt, K.; Stefanec, N.; Milner, A.; Currier, D.; Pirkis, J.; Condron, P.; Hetrick, S. What works in youth suicide prevention? A systematic review and meta-analysis. In Proceedings of the 2018 IASP Asia Pacific Meeting, Bay of Islands, New Zealand, 2–5 May 2018. [Google Scholar]
- Kidger, J.; Gunnell, D.; Biddle, L.; Campbell, R.; Donovan, J. Part and parcel of teaching? Secondary school staff’s views on supporting student emotional health and well-being. Br. Educ. Res. J. 2009, 36, 919–935. [Google Scholar] [CrossRef]
- O’Dea, B.; King, C.; Subotic-Kerry, M.; O’Moore, K.; Christensen, H. School Counselors’ Perspectives of a Web-Based Stepped Care Mental Health Service for Schools: Cross-Sectional Online Survey. JMIR Ment. Health 2017, 4, e55. [Google Scholar] [CrossRef] [PubMed]
- Berger, E.; Hasking, P.; Reupert, A. Developing a Policy to Address Nonsuicidal Self-Injury in Schools. J. School Health 2015, 85, 629–647. [Google Scholar] [CrossRef]
- De Riggi, M.E.; Moumne, S.; Heath, N.L.; Lewis, S.P. Non-Suicidal Self-Injury in Our Schools: A Review and Research-Informed Guidelines for School Mental Health Professionals. Can. J. School Psychol. 2017, 32, 122–143. [Google Scholar] [CrossRef]
- Hasking, P.A.; Heath, N.L.; Kaess, M.; Lewis, S.P.; Plener, P.L.; Walsh, B.W.; Whitlock, J.; Wilson, M.S. Position paper for guiding response to non-suicidal self-injury in schools. Sch. Psychol. Int. 2016, 37, 644–663. [Google Scholar] [CrossRef]
- Thomas, D.R. A general inductive approach for analyzing qualitative evaluation data. Am. J. Eval. 2006, 27, 237–246. [Google Scholar] [CrossRef]
- Crowe, M.; Inder, M.; Porter, R. Conducting qualitative research in mental health: Thematic and content analyses. Aust. New Zealand J. Psychiatry 2015, 49, 616–623. [Google Scholar] [CrossRef]
- Guest, G.; Bunce, A.; Johnson, L. How many interviews are enough? An experiment with data saturation and variability. Field Methods 2006, 18, 59–82. [Google Scholar] [CrossRef]
- Braun, V.; Clarke, V. Using thematic analysis in psychology. Qual. Res. Psychol. 2006, 3, 77–101. [Google Scholar] [CrossRef]
- Burnard, P.; Gill, P.; Stewart, K.; Treasure, E.; Chadwick, B. Analysing and presenting qualitative data. Br. Dent. J. 2008, 204, 429. [Google Scholar] [CrossRef] [PubMed]
- Koch, T. Establishing rigour in qualitative research: The decision trail. J. Adv. Nurs. 2006, 53, 91–100. [Google Scholar] [CrossRef] [PubMed]


{kind=link}
| Interview | Decile | School Type | Location | Ethnicity (Participant) | Profession | School Population |
|---|---|---|---|---|---|---|
| 1 | 9 | State | Central Auckland | NZ European/Pākehā | School Guidance Counsellor | 2000+ |
| 2 | 9 | State | Central Auckland | Asian | School Guidance Counsellor | 2000+ |
| 3 | 9 | State | Central Auckland | NZ European/Pākehā | School Guidance Counsellor | 2000+ |
| 4 | 9 | State | Central Auckland | Samoan | School Guidance Counsellor | 2000+ |
| 5 | 10 | State | North Auckland | NZ European/Pākehā | School Guidance Counsellor | 1500–1999 |
| 6 | 10 | State | North Auckland | NZ European/Pākehā | School Guidance Counsellor | 1500–1999 |
| 7 | 7 | State | Central Auckland | NZ European/Pākehā | School Guidance Counsellor | 2000+ |
| 8 | 7 | State | Central Auckland | NZ European/Pākehā | School Guidance Counsellor | 2000+ |
| 9 | 7 | State | Central Auckland | NZ European/Pākehā | School Guidance Counsellor | 2000+ |
| 10 | 9 | State integrated | North Auckland | NZ European/Pākehā | School Guidance Counsellor | 2000+ |
| 11 | 8 | State | Central Auckland | NZ European/Pākehā | School Guidance Counsellor | 1000–1499 |
| 12 | 4 | State | Central Auckland | Dutch | School Guidance Counsellor | 1500–1999 |
| 13 | 4 | State | Central Auckland | NZ European/Pākehā | School Guidance Counsellor | 1500–1999 |
| 14 | 2 | State integrated | Central Auckland | NZ European/Pākehā | School Guidance Counsellor | Less than 500 |
| 15 | 4 | Private | Central Auckland | NZ European/Pākehā | School Guidance Counsellor | 500–999 |
| 17 | 4 | Private | Central Auckland | NZ European/Pākehā | Chaplain | 500–999 |
| 18 | 10 | Private | Central Auckland | NZ European/Pākehā | School Guidance Counsellor | 1000–1499 |
| 19 | 4 | State | East Auckland | NZ European/Pākehā | School Guidance Counsellor | 1000–1499 |
| 20 | 3 | State | Central Auckland | NZ European/Pākehā | School Guidance Counsellor | 1000–1499 |
| 21 | 3 | State | Central Auckland | NZ European/Pākehā | Social Worker | 1000–1499 |
| 22 | 10 | Private | North Auckland | NZ European/Pākehā | School Guidance Counsellor | 1500–1999 |
| 23 | 1 | State integrated | South Auckland | NZ European/Pākehā | School Guidance Counsellor | 500–999 |
| 26 | 10 | Private | South Auckland | NZ European/Pākehā | School Guidance Counsellor | 1000–1499 |
| 30 | 8 | State | West Auckland | NZ European/Pākehā | School Guidance Counsellor | 1000–1499 |
| 31 | 5 | State | Northland | English | School Guidance Counsellor | 1000–1499 |
| 32 | 5 | State | Northland | NZ European/Pākehā | School Guidance Counsellor | 1000–1499 |
| Need for Guidelines | |
| Positive views about the need for guidelines | Encourages best practice |
| Provides support in stressful situations | |
| Provides a rationale for school policy | |
| Lack utilization of guidelines | Believed guidelines did not exist/not accessible/not relevant to New Zealand context |
| Relied on informal policies | |
| Need flexibility | Understand individual context |
| Burden—Excessive Workload and Responsibility | |
| Increased Mental Health Issues | Increased prevalence of suicidal ideation, self-harm, anxiety, depression |
| Increase in potential drivers of mental health issues, including self-harm | |
| Role Overload | Change in role responsibility |
| Lack of resourcing | |
| Discrepancy—Differences in the Way That Self-Harm is Managed between Schools | |
| Training | Lack of training on self-harm/suicidal ideation during degree |
| Relied on professional development, mentoring, colleagues, supervision | |
| Educating wider staff members | |
| Educating parents | |
| Process/Procedure | Risk assessment |
| Confidentiality | |
| Referral | |
| Management strategies | |
| Preventative/proactive interventions | |
| Communication | Internal—between pastoral care staff and other school staff |
| External—between pastoral care staff and external agencies | |
| External—between school guidance counsellors and whānau | |
© 2019 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Te Maro, B.; Cuthbert, S.; Sofo, M.; Tasker, K.; Bowden, L.; Donkin, L.; Hetrick, S.E. Understanding the Experience and Needs of School Counsellors When Working with Young People Who Engage in Self-Harm. Int. J. Environ. Res. Public Health 2019, 16, 4844. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph16234844
Te Maro B, Cuthbert S, Sofo M, Tasker K, Bowden L, Donkin L, Hetrick SE. Understanding the Experience and Needs of School Counsellors When Working with Young People Who Engage in Self-Harm. International Journal of Environmental Research and Public Health. 2019; 16(23):4844. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph16234844
Chicago/Turabian StyleTe Maro, Ben, Sasha Cuthbert, Mia Sofo, Kahn Tasker, Linda Bowden, Liesje Donkin, and Sarah E. Hetrick. 2019. "Understanding the Experience and Needs of School Counsellors When Working with Young People Who Engage in Self-Harm" International Journal of Environmental Research and Public Health 16, no. 23: 4844. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph16234844