A Methodological Approach for Implementing an Integrated Multimorbidity Care Model: Results from the Pre-Implementation Stage of Joint Action CHRODIS-PLUS


 ,
,  , ,
, ,  , , , , and
, , , , and
Abstract
:1. Introduction
1.1. The Challenge of Multimorbidity
1.2. The Integrated Multimorbidity Care Model
1.3. Pilot Implementation of the Integrated Multimorbidity Care Model: Joint Action CHRODIS-PLUS
1.4. Aims and Objectives
2. Methods
2.1. Survey to Assess Characteristics of the Pilot Sites
2.2. Patient Risk Stratification Strategies
2.3. Implementation Strategy
2.3.1. Implementation Strategy Step 1: Scope Analysis
2.3.2. Implementation Strategy Step 2: SWOT Analysis
2.3.3. Implementation Strategy Steps 3 and 4: Development and Improvement of Methodology and Final Development of Action Plans
3. Results
3.1. Components in the Planned Interventions
3.2. Description of Pilot Sites
3.3. Key Performance Indicators
4. Discussion
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- Melis, R.; Marengoni, A.; Angleman, S.; Fratiglioni, L. Incidence and predictors of multimorbidity in the elderly: A population-based longitudinal study. PLoS ONE 2014, 9, e103120. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hopman, P.; Schellevis, F.G.; Rijken, M. Health-related needs of people with multiple chronic diseases: Differences and underlying factors. Qual. Life Res. 2016, 25, 651–660. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Onder, G.; Cesari, M.; Maggio, M.; Palmer, K. Defining a care pathway for patients with multimorbidity or frailty. Eur. J. Intern. Med. 2017, 38, 1–2. [Google Scholar] [CrossRef] [PubMed]
- Smith, S.M.; Soubhi, H.; Fortin, M.; Hudon, C.; O’Dowd, T. Managing patients with multimorbidity: Systematic review of interventions in primary care and community settings. BMJ 2012, 345, e5205. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Marengoni, A.; Angleman, S.; Melis, R.; Mangialasche, F.; Karp, A.; Garmen, A.; Meinow, B.; Fratiglioni, L. Aging with multimorbidity: A systematic review of the literature. Ageing Res. Rev. 2011, 10, 430–439. [Google Scholar] [CrossRef] [PubMed]
- Palmer, K.; Marengoni, A.; Forjaz, M.J.; Jureviciene, E.; Laatikainen, T.; Mammarella, F.; Muth, C.; Navickas, R.; Prados-Torres, A.; Rijken, M.; et al. Multimorbidity care model: Recommendations from the consensus meeting of the Joint Action on Chronic Diseases and Promoting Healthy Ageing across the Life Cycle (JA-CHRODIS). Health Policy 2018, 122, 4–11. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Available online: http://chrodis.eu/wp-content/uploads/2017/11/ja-chrodis-multimorbidity-care-model-wp6-rokas-navickas.pdf (accessed on 3 December 2019).
- Wagner, E.H. Chronic disease management: What will it take to improve care for chronic illness? Eff. Clin. Pract. 1998, 1, 2–4. [Google Scholar] [PubMed]
- Wagner, E.H.; Davis, C.; Schaefer, J.; Von Korff, M.; Austin, B. A survey of leading chronic disease management programs: Are they consistent with the literature? Manag. Care Q. 1999, 7, 56–66. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hopman, P.; De Bruin, S.R.; Forjaz, M.J.; Rodriguez-Blazquez, C.; Tonnara, G.; Lemmens, L.C.; Onder, G.; Baan, C.A.; Rijken, M. Effectiveness of comprehensive care programs for patients with multiple chronic conditions or frailty: A systematic literature review. Health Policy 2016, 120, 818–832. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Available online: http://www.chrodis.eu (accessed on 3 December 2019).
- Onder, G.; Palmer, K.; Navickas, R.; Jurevičienė, E.; Mammarella, F.; Strandzheva, M.; Mannucci, P.; Pecorelli, S.; Marengoni, A. Time to face the challenge of multimorbidity. A European perspective from the joint action on chronic diseases and promoting healthy ageing across the life cycle (JA-CHRODIS). Eur. J. Intern. Med. 2015, 26, 157–159. [Google Scholar] [CrossRef] [PubMed]
- Alonso-Morán, E.; Nuño-Solinis, R.; Onder, G.; Tonnara, G. Multimorbidity in risk stratification tools to predict negative outcomes in adult population. Eur. J. Intern. Med. 2015, 26, 182–189. [Google Scholar] [CrossRef] [PubMed]
- Marengoni, A.; Vetrano, D.L.; Calderón-Larrañaga, A.; Onder, G. Multimorbidity and patient-centred care in the 3D trial. Lancet 2019, 393, 127–128. [Google Scholar] [CrossRef] [Green Version]
- Institute for Healthcare Improvement: The Breakthrough Series: IHI’s Collaborative Model for Achieving Breakthrough Improvement [Internet]. Available online: http://www.ihi.org:80/resources/Pages/IHIWhitePapers/TheBreakthroughSeriesIHIsCollaborativeModelforAchievingBreakthroughImprovement.aspx (accessed on 3 December 2019).
- Available online: https://www.opimec.org (accessed on 3 December 2019).
- Prados-Torres, A.; del Cura-González, I.; Prados-Torres, D.; López-Rodríguez, J.A.; Leiva-Fernández, F.; Calderón-Larrañaga, A.; López-Verde, F.; Gimeno-Feliu, L.A.; Escortell-Mayor, E.; Pico-Soler, V.; et al. Effectiveness of an intervention for improving drug prescription in primary care patients with multimorbidity and polypharmacy: Study protocol of a cluster randomized clinical trial (Multi-PAP project). Implement. Sci. 2017, 12, 54. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Bonomi, A.E.; Wagner, E.H.; Glasgow, R.E.; Von Korff, M. Assessment of Chronic Illness Care (ACIC): A practical tool to measure quality improvement. Health. Serv. Res. 2002, 37, 791–820. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Glasgow, R.E.; Wagner, E.H.; Schaefer, J.; Mahoney, L.D.; Reid, R.J.; Greene, S.M. Development and validation of the Patient Assessment of Chronic Illness Care (PACIC). Med. Care 2005, 43, 436–444. [Google Scholar] [CrossRef] [PubMed]
- Smith, S.M.; Wallace, E.; O’Dowd, T.; Fortin, M. Interventions for improving outcomes in patients with multimorbidity in primary care and community settings. Cochrane Database Syst. Rev. 2016, 3, CD006560. [Google Scholar] [CrossRef]
- Salisbury, C.; Man, M.S.; Bower, P.; Guthrie, B.; Chaplin, K.; Gaunt, D.M.; Brookes, S.; Fitzpatrick, B.; Gardner, C.; Hollinghurst, S.; et al. Management of multimorbidity using a patient-centred care model: A pragmatic cluster-randomised trial of the 3D approach. Lancet 2018, 392, 41–50. [Google Scholar] [CrossRef]


{kind=link}
| Participants |
|---|
|
|
|
|
|
| Action Plan Steps |
|---|
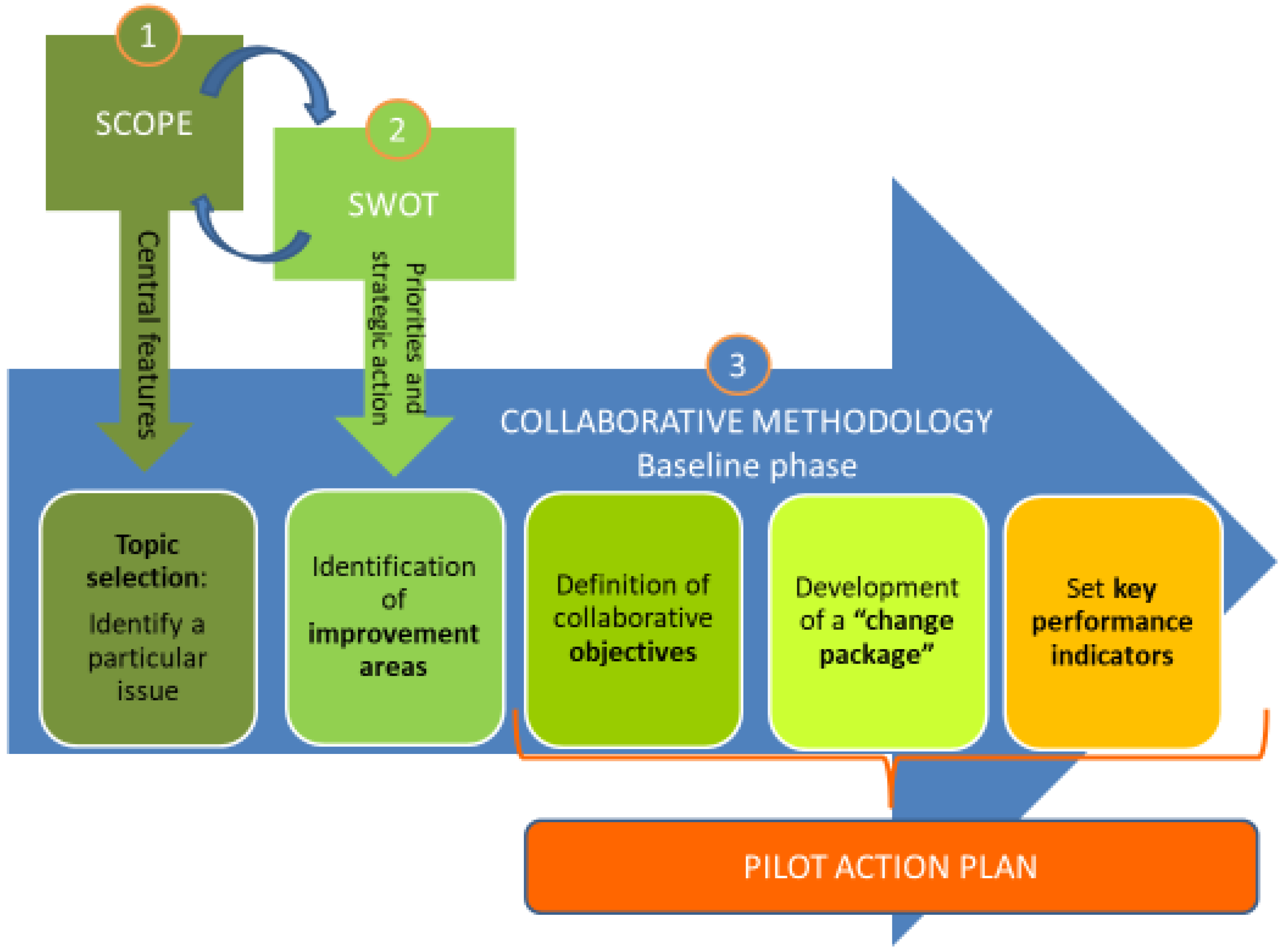
| 1. Identify the specific issues to work on The central features or elements of the intervention to work were already selected during the definition of the scope. These included components of the Integrated Multimorbidity Care Model [6]. |
| 2. Detect improvement areas Based on the strengths, weaknesses, opportunities, threats (SWOT) analysis, the working groups identified specific areas for improvement. |
| 3. Define specific objectives According to the improvement areas detected, the working groups developed achievable and realistic objectives. |
| 4. Develop the Change Package Based on the improvement areas and the associated objectives, concrete activities were described in a “change package”, which is a set of changes that lead to improvement and successful implementation of Integrated Multimorbidity Care Model during the implementation phase. Each objective defined in the previous step requires at least one activity. |
| 5. Set key performance indicators Key performance indicators were defined to ensure that the expected impact of the interventions can be accurately measured. Depending on the site, the indicators could either be intermediate health-related outcome measures, process indicators, or both. The targets had to be achievable and measurable. Existing data was chosen to measure progress. |
| Andalusian Health System | Aragon Health System | UCSC-Rome | VULSK | Kauno Klinikos | |
|---|---|---|---|---|---|
| Country | Spain | Spain | Italy | Lithuania | Lithuania |
| Patients | Complex chronic patients with multimorbidity (patients with chronic severe health problems, multimorbidity and polypharmacy) | Patients with multimorbidity (3+ diseases) and polypharmacy (5+ drugs) or complex | Adults with dementia or Down syndrome and multimorbidity | Patients with multimorbidity (2+ diseases) | Patients with multimorbidity (2+ diseases) |
| Age | No age limit | ≥65 years | ≥65 years Alzheimer Disease patients ≥18 years Down Syndrome patients | 45–70 | 45–70 |
| Target number of patients | All complex chronic patients with individualized care plans initiated from December 2018 to February 2019 all over the region | 200 | 200 | 200 | 200 |
| General aim | Assess the systematized application of individualized care plans to complex chronic patients | Training of healthcare professionals in multimorbidity + integrated care measures | Improve case coordination, and provide patients with a reference care provider (+Technocare) | To improve the quality of life, decrease the number of potentially avoidable hospitalizations/readmissions and improve quality of multimorbid patient care | To improve the quality of life, decrease the number of potentially avoidable hospitalizations/readmissions and improve quality of multimorbid patient care |
| Setting | Primary care centers in the region | 13 primary care health centers +1 hospital of reference | Outpatient clinic | Different primary care health centers (1 public, 1 private) | Different primary care health centers (1 urban, 1 rural) |
| Implementation | All of the five pilot sites include a six-month run-in period (patient recruitment), followed by a 12-month implementation period | ||||
| Andalusian Health System 1 | Aragon Health System | UCSC-Rome | VULSK | Kauno Klinikos | |
|---|---|---|---|---|---|
| Delivery of the care model system | |||||
| Regular comprehensive assessment of patients | Yes | Yes | Yes | Yes | |
| Multidisciplinary, coordinated team | Yes | Yes | Yes | Yes | |
| Professional appointed as coordinator of the individualized care plan (“case manager”) | Yes | Yes | Yes | Yes | |
| Individualized care plans | Yes | Yes | Yes | Yes | |
| Decision support | |||||
| Implementation of evidence-based practice | Yes | Yes | |||
| Training members of the multidisciplinary team | Yes | Yes | Yes | ||
| Developing a consultation system to consult professional experts | Yes | Yes | Yes | ||
| Self-management support | |||||
| Training of care providers to self-management support | Yes | ||||
| Providing options for patients and families to improve their self-management | Yes | Yes | Yes | ||
| Shared decision making (care provider and patients) | Yes | Yes | Yes | Yes | |
| Information systems and technology | |||||
| Electronic patient records and computerized clinical charts | Yes | Yes | |||
| Exchange of information between care providers and sectors by clinical information systems | Yes | Yes | |||
| Uniform coding of patients’ health problems where possible | Yes | ||||
| Patient-operated technology allowing patients to send information to their care providers | Yes | ||||
| Social and community resources | |||||
| Supporting access to community- and social- resources | Yes | ||||
| Involvement of social network (informal), including friends, patient associations, family, neighbors | Yes | Yes | |||
| Andalusian Health System | Aragon Health System | UCSC-Rome | Kauno Klinikos and VULSK |
|---|---|---|---|
| PROCESS INDICATORS Number of health districts participating in the pilot Drawing up and delivering the ndividualized care plans Number of primary care units involved Number of visits of complex chronic patients with individualized care plans to primary healthcare centers in 12 months Number of health care professional team meetings related to individualized care plans in 12 months Quality of performed individualized care plans | PROCESS INDICATORS Existence of a document describing the functions/role of the case manager Percentage of patients included in the program with case manager identified Number of primary care teams included in the program Implementation of a chronic care unit at the hospital Identification of personnel of reference at hospital’s chronic care unit Number of health professionals who accept to do/start/finish the training course Improvement of knowledge and skills in multimorbidity after the training course Existence of a module of information shared among professionals in the electronic health records Percentage of response to inter-consultations in less than 96 h Availability of direct and specific communication channels between chronic patients and their case managers Social support/needs assessment Identification and mapping of community assets | PROCESS INDICATORS A survey will be administered in the outpatient context at the start of the quality improvement intervention and 10 months after the rollout process Reduction of unnecessary referrals Percentage of dropouts (number of missing appointments by patients with AD and DS/number of fixed appointments for patients with AD and DS) calculated as an index for poor coordination of care Average number of Technocare contacts recorded in 12 months Percentage of extra Technocare contacts for Lazio region Percentage of Technocare dropouts (percentage of patients with AD and DS who disattend the fixed Technocare appointment/number of patients with AD and DS who fixed Technocare appointment) Percentage of rescheduled techno visits (percentage of rescheduled visits for patients with AD and DS/number of patients with AD and DS who fixed Technocare appointment Number of patients with AD and DS that participate in the group meeting | PROCESS INDICATORS Existence of a guidelines that describes the role of case manager % of patients with individualized care plan based on a comprehensive assessment Number of visits to primary care team in 12 months per patient Number of consultations in 12 months |
| IMMEDIATE HEALTH-RELATED OUTCOMES ACIC and PACIC+ Inpatient episodes of complex chronic patients with individualized care plans in 12 months Outpatient visits of complex chronic patients with individualized care plans in 12 months Emergency episodes of complex chronic patients with individualized care plans in 12 months Rate of unplanned hospitalization potentially preventable achieved in 12 months | IMMEDIATE HEALTH-RELATED OUTCOMES ACIC Number of admissions to the emergency room in 12 months Number of hospitalizations in 12 months Number of hospitalizations at chronic care unit/total hospitalizations Satisfaction of the training course by health professionals and self-perceived applicability in clinical practice Percentage of inter-consultations Percentage of patients with individualized care plan based on a comprehensive assessment Prevalence of polymedicated and hyper-polymedicated patients | IMMEDIATE HEALTH-RELATED OUTCOMES ACIC and PACIC+ Reduction of accessibility in Emergency Department and subsequent hospitalizations | IMMEDIATE HEALTH-RELATED OUTCOMES ACIC and PACIC+ Number of unplanned visits in 12 months Number and duration of hospitalizations, admissions to emergency room, and avoidable hospitalizations in 12 months Number of incompatible drugs combination (drug interaction rate) -EQ-5D questionnaire is a standardized instrument developed by the EuroQol Group as a measure of health-related quality of life -The EQ VAS records the patient’s self-rated health on a vertical visual analogue scale |
© 2019 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Palmer, K.; Carfì, A.; Angioletti, C.; Di Paola, A.; Navickas, R.; Dambrauskas, L.; Jureviciene, E.; João Forjaz, M.; Rodriguez-Blazquez, C.; Prados-Torres, A.; et al. A Methodological Approach for Implementing an Integrated Multimorbidity Care Model: Results from the Pre-Implementation Stage of Joint Action CHRODIS-PLUS. Int. J. Environ. Res. Public Health 2019, 16, 5044. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph16245044
Palmer K, Carfì A, Angioletti C, Di Paola A, Navickas R, Dambrauskas L, Jureviciene E, João Forjaz M, Rodriguez-Blazquez C, Prados-Torres A, et al. A Methodological Approach for Implementing an Integrated Multimorbidity Care Model: Results from the Pre-Implementation Stage of Joint Action CHRODIS-PLUS. International Journal of Environmental Research and Public Health. 2019; 16(24):5044. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph16245044
Chicago/Turabian StylePalmer, Katie, Angelo Carfì, Carmen Angioletti, Antonella Di Paola, Rokas Navickas, Laimis Dambrauskas, Elena Jureviciene, Maria João Forjaz, Carmen Rodriguez-Blazquez, Alexandra Prados-Torres, and et al. 2019. "A Methodological Approach for Implementing an Integrated Multimorbidity Care Model: Results from the Pre-Implementation Stage of Joint Action CHRODIS-PLUS" International Journal of Environmental Research and Public Health 16, no. 24: 5044. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph16245044