Relationship among Activities of Daily Living, Nutritional Status, and 90 Day Readmission in Elderly Patients with Heart Failure

 ,
,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Design and Subjects
2.2. Investigation
2.3. Assessment of ADL
2.4. Assessment of Nutritional Status
2.5. Assessment of Initiation of Walking Exercise
2.6. Assessment of Follow-up
2.7. Statistical Analysis
3. Results
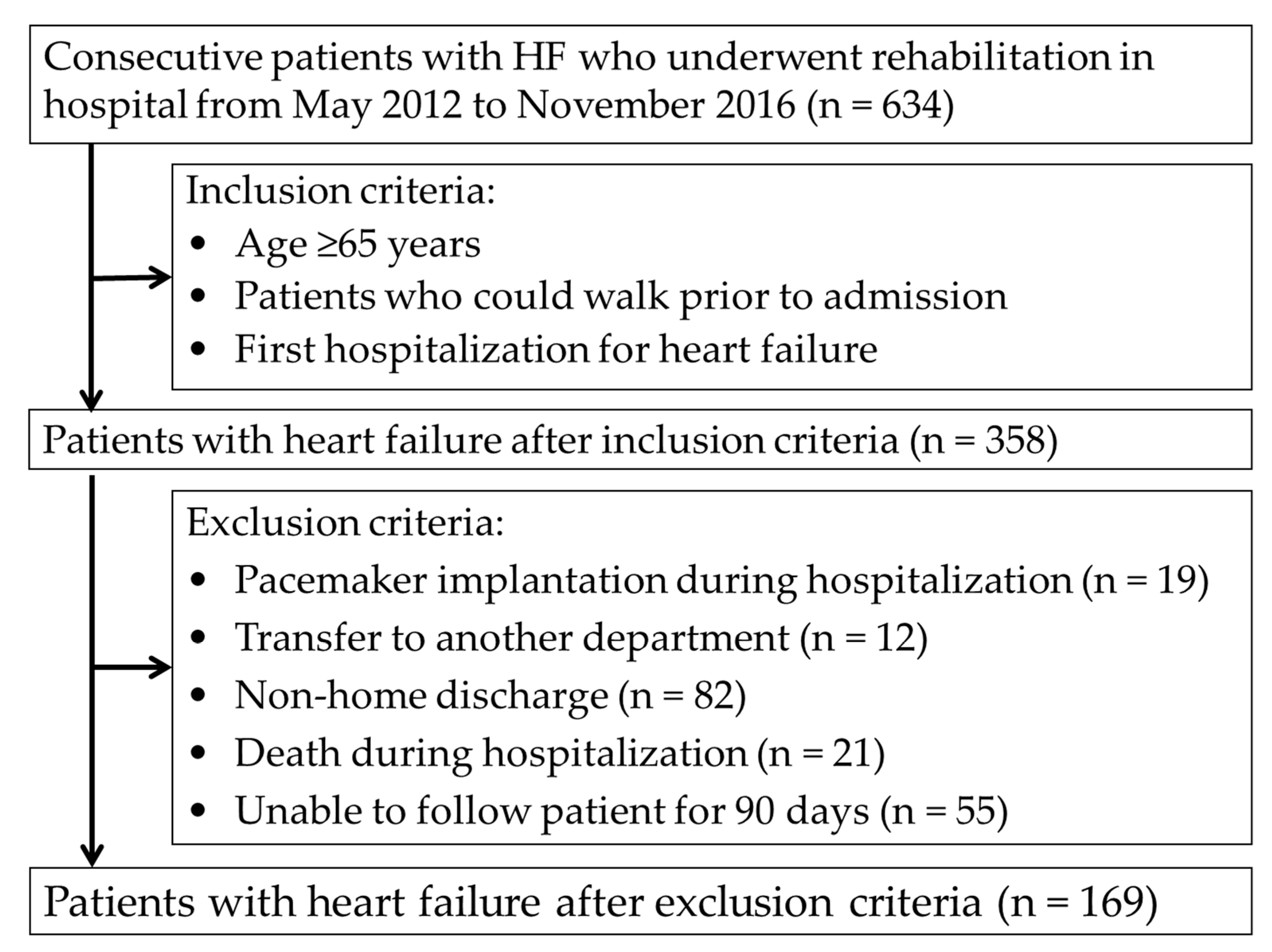
3.1. Patient Flow
3.2. Patient Characteristics
3.3. Hospital Readmission
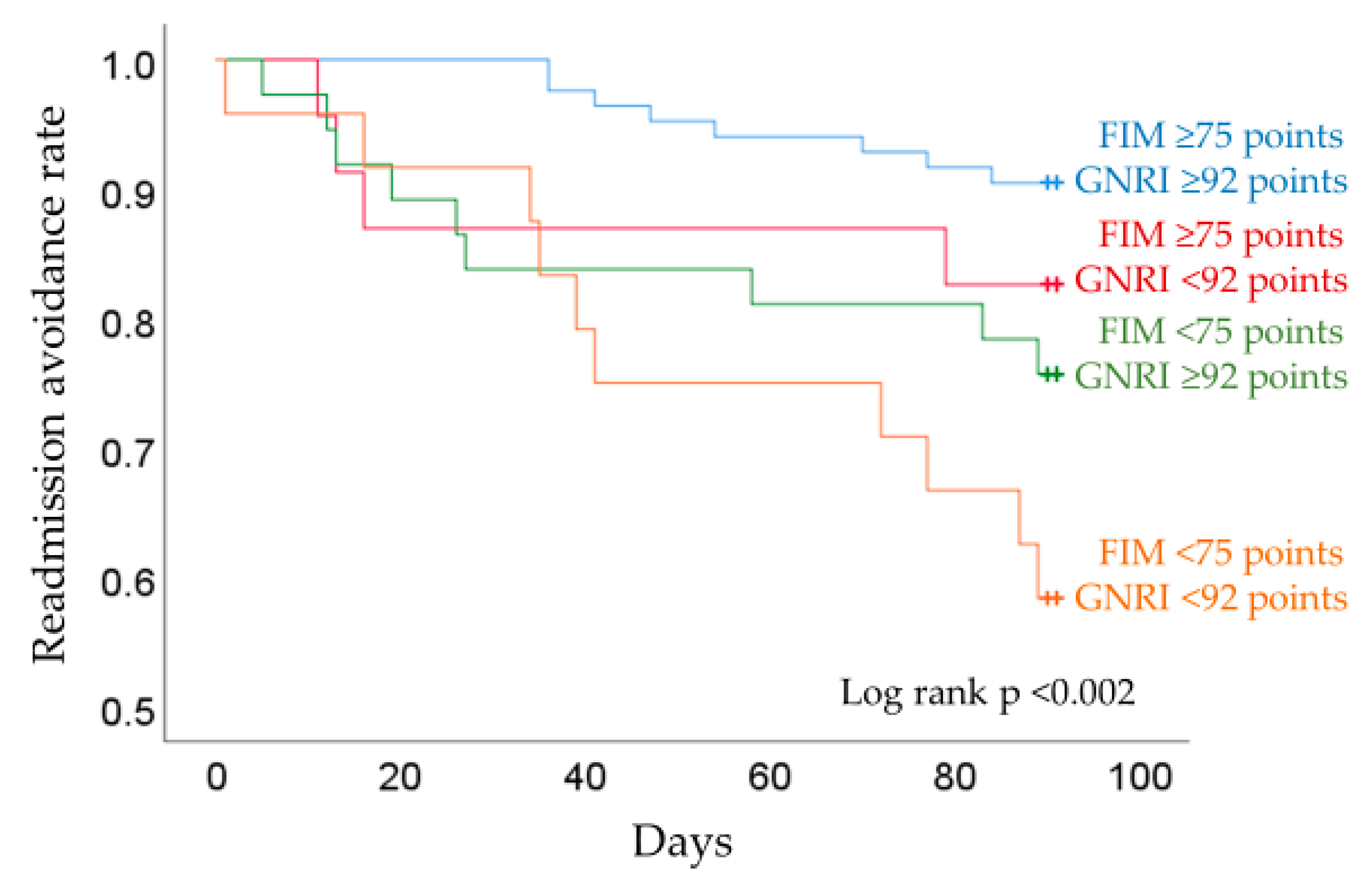
3.4. Readmission Rates by Motor FIM and GNRI
4. Discussion
4.1. Characteristics of Readmission Group of Elderly HF Patients
4.2. Motor ADL and GNRI as Factors of Hospital Readmission
4.3. Relation Between ADL, GNRI and the Rate of Readmission
4.4. Strengths and Limitations of this Investigation
5. Conclusions
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- Kannel, W.B.; Belanger, A.J. Epidemiology of heart failure. Am. Heart J. 1991, 121, 951–957. [Google Scholar] [CrossRef]
- Roger, V.L.; Go, A.S.; Lloyd-Jones, D.M.; Adams, R.J.; Berry, J.D.; Brown, T.M.; Carnethon, M.R.; Dai, S.; de Simone, G.; Ford, E.S.; et al. Heart Disease and Stroke Statistics-2011 Update: A report from the American Heart Association. Circulation 2011, 123, 18–209. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Yasuda, S.; Nakao, K.; Nishimura, K.; Miyamoto, Y.; Sumita, Y.; Shishido, T.; Anzai, T.; Tsutsui, H.; Ito, H.; Komuro, I.; et al. The current status of cardiovascular medicine in Japan-Analysis of a large number of health records from a nationwide claim-based database, JROAD-DPC. Circ. J. 2016, 80, 2327–2335. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ponikowski, P.; Voors, A.A.; Anker, S.D.; Bueno, H.; Cleland, J.G.F.; Coats, A.J.S.; Falk, V.; González-Juanatey, J.R.; Harjola, V.P.; Jankowska, E.A.; et al. 2016 ESC Guidelines for the diagnosis and treatment of acute and chronic heart failure: The Task Force for the diagnosis and treatment of acute and chronic heart failure of the European Society of Cardiology (ESC) Developed with the special contribution of the Heart Failure Association (HFA) of the ESC. Eur. Heart J. 2016, 37, 2129–2200. [Google Scholar] [PubMed]
- Hamaguchi, S.; Kinugawa, S.; Goto, D.; Tsuchihashi-Makaya, M.; Yokota, T.; Yamada, S.; Yokoshiki, H.; Takeshita, A.; Tsutsui, H. Predictors of long-term adverse outcomes in elderly patients over 80 years hospitalized with heart failure.-A report from the Japanese Cardiac Registry of Heart Failure in Cardiology (JCARE-CARD)-. Circ. J. 2011, 75, 2403–2410. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Sakata, Y.; Shimokawa, H. Epidemiology of heart failure in Asia. Circ. J. 2013, 77, 2209–2217. [Google Scholar] [CrossRef] [Green Version]
- Saito, M.; Negishi, K.; Marwick, T.H. Meta-analysis of risks for short-term readmission in patients with heart failure. Am. J. Cardiol. 2016, 117, 626–632. [Google Scholar] [CrossRef]
- Tsuchihashi-Makaya, M.; Hamaguchi, S.; Kinugawa, S.; Yokota, T.; Goto, D.; Yokoshiki, H.; Kato, N.; Takeshita, A.; Tsutsui, H. Characteristics and outcomes of hospitalized patients with heart failure and reduced vs preserved ejection fraction. Report from the Japanese Cardiac Registry of Heart Failure in Cardiology (JCARE-CARD). Circ. J. 2009, 73, 1893–1900. [Google Scholar] [CrossRef] [Green Version]
- Dunlay, S.M.; Redfield, M.M.; Weston, S.A.; Therneau, T.M.; Hall Long, K.; Shah, N.D.; Roger, V.L. Hospitalizations after heart failure diagnosis a community perspective. J. Am. Coll. Cardiol. 2009, 54, 1695–1702. [Google Scholar] [CrossRef] [Green Version]
- Dharmarajan, K.; Hsieh, A.F.; Lin, Z.; Bueno, H.; Ross, J.S.; Horwitz, L.; Barreto-Filho, J.A.; Kim, N.; Suter, L.G.; Bernheim, S.M.; et al. Hospital readmission performance and patterns of readmission: Retrospective cohort study of Medicare admissions. BMJ 2013, 347, f6571. [Google Scholar] [CrossRef] [Green Version]
- Ottenbacher, K.J.; Hsu, Y.; Granger, C.V.; Fiedler, R.C. The reliability of the Functional Independence Measure: A quantitative review. Arch. Phys. Med. Rehabil. 1996, 77, 1226–1232. [Google Scholar] [CrossRef]
- Dunlay, S.M.; Manemann, S.M.; Chamberlain, A.M.; Cheville, A.L.; Jiang, R.; Weston, S.A.; Roger, V.L. Activities of daily living and outcomes in heart failure. Circ. Heart Fail. 2015, 8, 261–267. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Tsutsui, H.; Tsuchihashi-Makaya, M.; Kinugawa, S.; Goto, D.; Takeshita, A. Clinical characteristics and outcome of hospitalized patients with heart failure in Japan. Circ. J. 2006, 70, 1617–1623. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Agra Bermejo, R.M.; González Ferreiro, R.; Varela Román, A.; Gómez Otero, I.; Kreidieh, O.; Conde Sabarís, P.; Rodríguez-Mañero, M.; Moure González, M.; Seoane Blanco, A.; Virgós Lamela, A.; et al. Nutritional status is related to heart failure severity and hospital readmissions in acute heart failure. Int. J. Cardiol. 2017, 230, 108–114. [Google Scholar] [CrossRef] [PubMed]
- Kinugasa, Y.; Kato, M.; Sugihara, S.; Hirai, M.; Yamada, K.; Yanagihara, K.; Yamamoto, K. Geriatric nutritional risk index predicts functional dependency and mortality in patients with heart failure with preserved ejection fraction. Circ. J. 2013, 77, 705–711. [Google Scholar] [CrossRef] [Green Version]
- Aziz, E.F.; Javed, F.; Pratap, B.; Musat, D.; Nader, A.; Pulimi, S.; Alivar, C.L.; Herzog, E.; Kukin, M.L. Malnutrition as assessed by nutritional risk index is associated with worse outcome in patients admitted with acute decompensated heart failure: An ACAP-HF data analysis. Heart Int. 2011, 6, e2. [Google Scholar] [CrossRef]
- Granger, C.V.; Cotter, A.C.; Hamilton, B.B.; Fiedler, R.C. Functional assessment scales: A study of persons after stroke. Arch. Phys. Med. Rehabil. 1993, 74, 133–138. [Google Scholar]
- Scattolin, F.A.; Diogo, M.J.; Colombo, R.C. Correlation between instruments for measuring health-related quality of life and functional independence in elderly with heart failure. Cad. Saude Publica 2007, 23, 2705–2715. [Google Scholar] [CrossRef] [Green Version]
- Bouillanne, O.; Morineau, G.; Dupont, C.; Coulombel, I.; Vincent, J.P.; Nicolis, I.; Benazeth, S.; Cynober, L.; Aussel, C. Geriatric Nutritional Risk Index: A new index for evaluating at-risk elderly medical patients. Am. J. Clin. Nutr. 2005, 82, 777–783. [Google Scholar] [CrossRef] [Green Version]
- Narumi, T.; Arimoto, T.; Funayama, A.; Kadowaki, S.; Otaki, Y.; Nishiyama, S.; Takahashi, H.; Shishido, T.; Miyashita, T.; Miyamoto, T.; et al. Prognostic importance of objective nutritional indexes in patients with chronic heart failure. J. Cardiol. 2013, 62, 307–313. [Google Scholar] [CrossRef] [Green Version]
- Yamada, K.; Furuya, R.; Takita, T.; Maruyama, Y.; Yamaguchi, Y.; Ohkawa, S.; Kumagai, H. Simplified nutritional screening tools for patients on maintenance hemodialysis. Am. J. Clin. Nutr. 2008, 87, 106–113. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Japanese Circulation Society Joint Working Group. Guidelines for rehabilitation in patients with cardiovascular disease 2012. Circ. J. 2014, 78, 2022–2093. [Google Scholar]
- Kitamura, M.; Izawa, K.P.; Taniue, H.; Mimura, Y.; Imamura, K.; Nagashima, H.; Brubaker, P.H. Relationship between activities of daily living and readmission within 90 days in hospitalized elderly patients with heart failure. BioMed Res. Int. 2017, 2017, e7420738. [Google Scholar] [CrossRef] [PubMed]
- Muzzarelli, S.; Leibundgut, G.; Maeder, M.T.; Rickli, H.; Handschin, R.; Gutmann, M.; Jeker, U.; Buser, P.; Pfisterer, M.; Brunner-La Rocca, H.P. Predictors of early readmission or death in elderly patients with heart failure. Am. Heart J. 2010, 160, 308–314. [Google Scholar] [CrossRef] [PubMed]
- Massari, F.; Scicchitano, P.; Iacoviello, M.; Passantino, A.; Guida, P.; Sanasi, M.; Piscopo, A.; Romito, R.; Valle, R.; Caldarola, P.; et al. Multiparametric approach to congestion for predicting long-term survival in heart failure. J. Cardiol. 2019, 19. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Massari, F.; Scicchitano, P.; Ciccone, M.M.; Caldarola, P.; Aspromonte, N.; Iacoviello, M.; Barro, S.; Pantano, I.; Valle, R. Bioimpedance vector analysis predicts hospital length of stay in acute heart failure. Nutrition 2019, 61, 56–60. [Google Scholar] [CrossRef] [PubMed]
- Aizawa, H.; Imai, S.; Fushimi, K. Factors associated with 30-day readmission of patients with heart failure from a Japanese administrative database. BMC Cardiovasc. Disord. 2015, 15, 134. [Google Scholar] [CrossRef] [Green Version]
- Zapatero, A.; Barba, R.; Gonzalez, N.; Losa, J.E.; Plaza, S.; Canora, J.; Marco, J. Influence of obesity and malnutrition on acute heart failure. Rev. Esp. Cardiol. (Engl. Ed.) 2012, 65, 421–426. [Google Scholar] [CrossRef]
- Galloway, R.V.; Karmarkar, A.M.; Graham, J.E.; Tan, A.; Raji, M.; Granger, C.V.; Ottenbacher, K.J. Hospital readmission following discharge from inpatient rehabilitation for older adults with debility. Phys. Ther. 2016, 96, 241–251. [Google Scholar] [CrossRef] [Green Version]
- Conner, D.; Barnes, C.; Harrison-Felix, C.; Reznickova, N. Rehabilitation outcomes in a population of nonagenarians and younger seniors with hip fracture, heart failure, or cerebral vascular accident. Arch. Phys. Med. Rehabil. 2010, 91, 1505–1510. [Google Scholar] [CrossRef]
- Krumholz, H.M. Post-hospital syndrome-an acquired, transient condition of generalized risk. N. Engl. J. Med. 2013, 368, 100–102. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Rodríguez-Pascual, C.; Paredes-Galán, E.; Ferrero-Martínez, A.I.; Gonzalez-Guerrero, J.L.; Hornillos-Calvo, M.; Menendez-Colino, R.; Torres-Torres, I.; Vilches-Moraga, A.; Galán, M.C.; Suarez-Garcia, F.; et al. The frailty syndrome is associated with adverse health outcomes in very old patients with stable heart failure: A prospective study in six Spanish hospitals. Int. J. Cardiol. 2017, 236, 296–303. [Google Scholar] [CrossRef] [PubMed]
- Minamisawa, M.; Miura, T.; Motoki, H.; Ueki, Y.; Nishimura, H.; Shimizu, K.; Shoin, W.; Harada, M.; Mochidome, T.; Senda, K.; et al. Geriatric Nutritional Risk Index Predicts Cardiovascular Events in Patients at Risk for Heart Failure. Circ. J. 2018, 82, 1614–1622. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Nakayama, H.; Koyama, S.; Kuragaichi, T.; Shiba, M.; Fujiwara, H.; Takatsu, Y.; Sato, Y. Prognostic value of rising serum albumin during hospitalization in patients with acute heart failure. Am. J. Cardiol. 2016, 117, 1305–1309. [Google Scholar] [CrossRef] [PubMed]
- Ueda, T.; Kawakami, R.; Horii, M.; Sugawara, Y.; Matsumoto, T.; Okada, S.; Nishida, T.; Soeda, T.; Okayama, S.; Somekawa, S.; et al. Noncardiovascular death, especially infection, is a significant cause of death in elderly patients with acutely decompensated heart failure. J. Card. Fail. 2014, 20, 174–180. [Google Scholar] [CrossRef] [PubMed]
- Kitamura, M.; Izawa, K.P.; Yaekura, M.; Mimura, Y.; Nagashima, H.; Oka, K. Differences in nutritional status and activities of daily living and mobility in elderly hospitalized patients with heart failure. ESC Heart Fail. 2019, 6, 344–350. [Google Scholar] [CrossRef]
- Houston, D.K.; Nicklas, B.J.; Ding, J.; Harris, T.B.; Tylavsky, F.A.; Newman, A.B.; Lee, J.S.; Sahyoun, N.R.; Visser, M.; Kritchevsky, S.B. Dietary protein intake is associated with lean mass change in older, community-dwelling adults: The Health, Aging, and Body Composition (Health ABC) Study. Am. J. Clin. Nutr. 2008, 87, 150–155. [Google Scholar] [CrossRef] [Green Version]
- Trobec, K.; von Haehling, S.; Anker, S.D.; Lainscak, M. Growth hormone, insulin-like growth factor 1, and insulin signaling-a pharmacological target in body wasting and cachexia. J. Cachexia Sarcopenia Muscle 2011, 2, 191–200. [Google Scholar] [CrossRef] [Green Version]
- Freeman, L.M.; Roubenoff, R. The nutrition implications of cardiac cachexia. Nutr. Rev. 1994, 52, 340–347. [Google Scholar] [CrossRef]
- Wakabayashi, H.; Sakuma, K. Rehabilitation nutrition for sarcopenia with disability: A combination of both rehabilitation and nutrition care management. J. Cachexia Sarcopenia Muscle 2014, 5, 269–277. [Google Scholar] [CrossRef]
- Htun, N.C.; Ishikawa-Takata, K.; Kuroda, A.; Tanaka, T.; Kikutani, T.; Obuchi, S.P.; Hirano, H.; Iijima, K. Screening for malnutrition in community dwelling older Japanese: Preliminary development and evaluation of the Japanese Nutritional Risk Screening Tool (NRST). J. Nutr. Health Aging 2016, 20, 114–120. [Google Scholar] [CrossRef] [PubMed]
- Kono, Y.; Izawa, H.; Aoyagi, Y.; Ishikawa, A.; Sugiura, T.; Mori, E.; Yanohara, R.; Ishiguro, T.; Yamada, R.; Okumura, S.; et al. Predictive impact of early mobilization on rehospitalization for elderly Japanese heart failure patients. Heart Vessel. 2019, 26. [Google Scholar] [CrossRef] [PubMed]
- Davidson, P.M.; Cockburn, J.; Newton, P.J.; Webster, J.K.; Betihavas, V.; Howes, L.; Owensby, D.O. Can a heart failure-specific cardiac rehabilitation program decrease hospitalizations and improve outcomes in high-risk patients? Eur. J. Cardiovasc. Prev. Rehabil. 2010, 17, 393–402. [Google Scholar] [CrossRef] [PubMed]
- Bonilla-Palomas, J.L.; Gámez-López, A.L.; Castillo-Domínguez, J.C.; Moreno-Conde, M.; López-Ibáñez, M.C.; Alhambra-Expósito, R.; Ramiro-Ortega, E.; Anguita-Sánchez, M.P.; Villar-Ráez, A. Nutritional intervention in malnourished hospitalized patients with heart failure. Arch. Med. Res. 2016, 47, 535–540. [Google Scholar] [CrossRef] [PubMed]



{kind=link}
{kind=link}
| Clinical Characteristics | Readmission n = 31 | Non-Readmission n = 138 | F or χ2 Value | p Value |
|---|---|---|---|---|
| Age, years | 83.4 ± 5.4 | 80.7 ± 7.1 | 1.9 a | 0.051 |
| Male Sex, % | 58.1 | 51.4 | 0.4 | 0.51 |
| BMI, kg/m2 | 21.3 ± 3.4 | 22.7 ± 3.3 | 0.1 | 0.03 |
| Clinical parameters | ||||
| LVEF, % | 49.1 ± 14.0 | 46.1 ± 16.3 | 2.7 a | 0.36 |
| BNP, pg/mL | 774.3 ± 428.7 | 929.6 ± 967.4 | 5.3 a | 0.17 |
| NYHA class I/II, % | 0/13/42/45 | 2/13/45/40 | 0.9 | 0.83 |
| Creatinine level, mg/dL | 1.8 ± 1.5 | 1.3 ± 1.2 | 6.3 a | 0.14 |
| eGFR, mL/min/1.73 m2 | 41.4 ± 22.8 | 47.8 ± 21.3 | 0.2 a | 0.14 |
| Hemoglobin level, g/dL | 10.6 ± 2.6 | 11.6 ± 2.5 | 0.0 a | 0.047 |
| Albumin level at discharge, g/dL | 3.6 ± 0.5 | 3.7 ± 0.4 | 0.1 a | 0.17 |
| GNRI | 94.1 ± 9.7 | 98.6 ± 9.5 | 0.0 a | 0.02 |
| Comorbidity, % | ||||
| Hypertension | 83.9 | 87.0 | 0.2 | 0.65 |
| Diabetes | 25.8 | 37.7 | 1.6 | 0.21 |
| Ischemic heart disease | 48.4 | 44.2 | 0.2 | 0.67 |
| Valvular disease | 38.7 | 29.7 | 1.0 | 0.33 |
| Atrial fibrillation | 30.0 | 14.6 | 1.3 | 0.25 |
| Orthopedic Conditions | 29.0 | 39.1 | 1.1 | 0.29 |
| Neurological disease | 12.9 | 23.2 | 1.6 | 0.21 |
| Respiratory disease | 29.0 | 21.0 | 0.9 | 0.33 |
| Medication | ||||
| Catecholamine | 12.9 | 10.1 | 0.2 | 0.65 |
| Diuretic | 93.5 | 92.8 | 0.02 | 0.88 |
| ACEI/ARB | 51.6 | 40.6 | 1.3 | 0.26 |
| β-blockers | 54.8 | 55.1 | <0.01 | 0.98 |
| Rehabilitation progress | ||||
| Motor FIM score at discharge | 71.2 ± 10.8 | 77.1 ± 10.9 | 0.1 a | 0.007 |
| Cognitive FIM score at discharge | 31.4 ± 4.8 | 31.2 ± 5.4 | 0.7 a | 0.87 |
| Initiation of walking exercise, days | 6.2 ± 6.3 | 4.9 ± 4.7 | 2.2 a | 0.20 |
| Length of hospital stay, days | 20.1 ± 11.8 | 17.9 ± 9.0 | 2.7 a | 0.24 |
| Variables | Univariate Analysis | Multivariate Analysis | ||||
|---|---|---|---|---|---|---|
| Cox Proportional Hazard Ratio | 95% CI | p Value | Cox Proportional Hazard Ratio | 95% CI | p Value | |
| BMI, kg/m2 | 0.88 | 0.79–0.99 | 0.03 | |||
| Hemoglobin level, g/dL | 0.88 | 0.78–1.002 | 0.054 | |||
| GNRI | 0.96 | 0.92–0.99 | 0.02 | 0.96 | 0.93–0.998 | 0.048 |
| Motor FIM score at discharge | 0.96 | 0.94–0.99 | 0.01 | 0.97 | 0.94–0.999 | 0.03 |
© 2019 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Kitamura, M.; Izawa, K.P.; Yaekura, M.; Mimura, Y.; Ikeda, Y.; Nagashima, H.; Brubaker, P.H. Relationship among Activities of Daily Living, Nutritional Status, and 90 Day Readmission in Elderly Patients with Heart Failure. Int. J. Environ. Res. Public Health 2019, 16, 5068. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph16245068
Kitamura M, Izawa KP, Yaekura M, Mimura Y, Ikeda Y, Nagashima H, Brubaker PH. Relationship among Activities of Daily Living, Nutritional Status, and 90 Day Readmission in Elderly Patients with Heart Failure. International Journal of Environmental Research and Public Health. 2019; 16(24):5068. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph16245068
Chicago/Turabian StyleKitamura, Masahiro, Kazuhiro P. Izawa, Masakazu Yaekura, Yumi Mimura, Yuichi Ikeda, Hitomi Nagashima, and Peter H. Brubaker. 2019. "Relationship among Activities of Daily Living, Nutritional Status, and 90 Day Readmission in Elderly Patients with Heart Failure" International Journal of Environmental Research and Public Health 16, no. 24: 5068. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph16245068