Reliability of a Virtual Prosthodontic Project Realized through a 2D and 3D Photographic Acquisition: An Experimental Study on the Accuracy of Different Digital Systems


 , , , and
, , , and 
Abstract
:1. Introduction
2. Materials and Methods
2.1. Patient Selection
- Patients requesting restorative treatments.
- Patients with systemic pathologies;
- Patients with oral pathologies, periodontal or articular disease.
2.2. Clinical and Laboratory (CAD) Procedures
2.3. Outcome
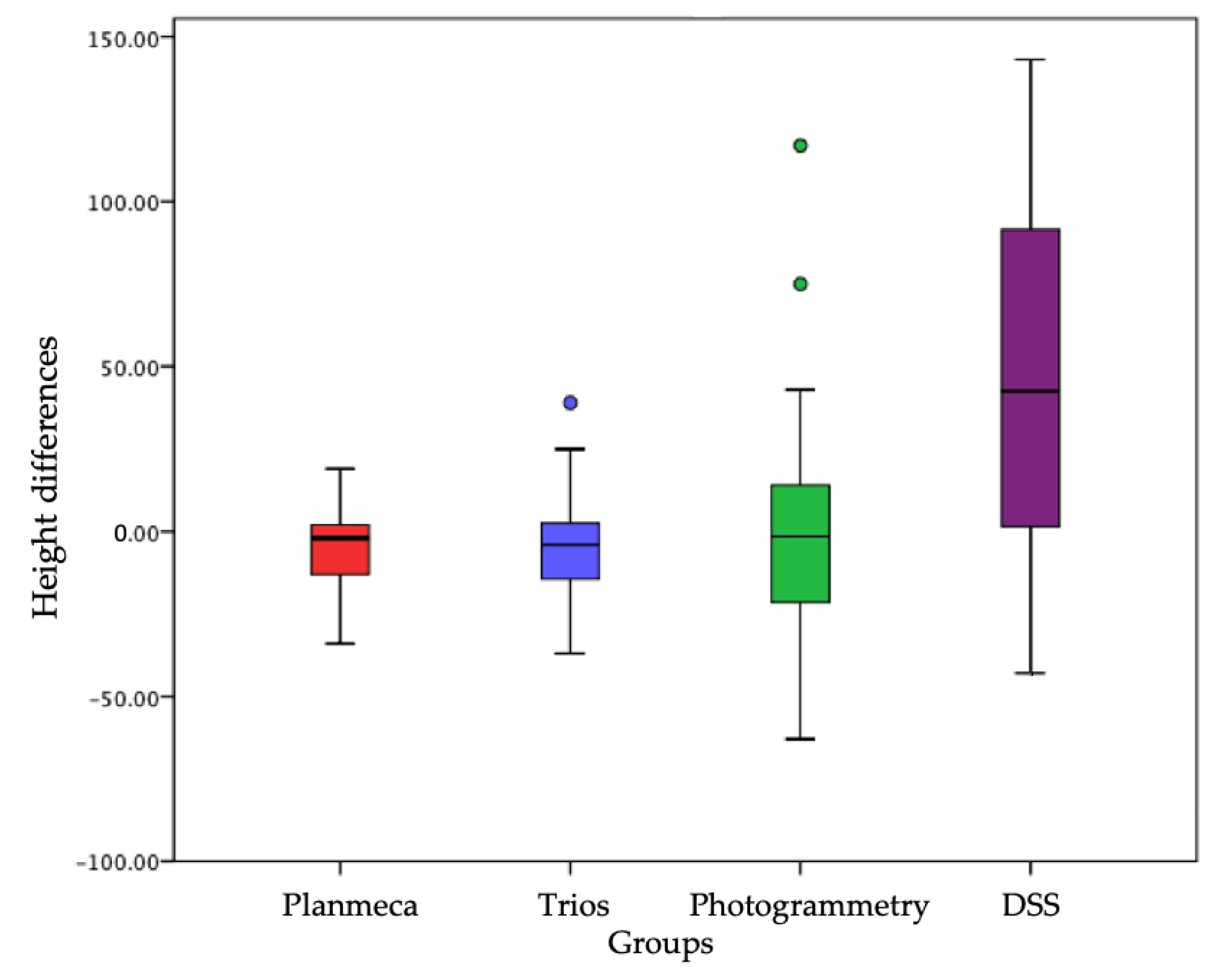
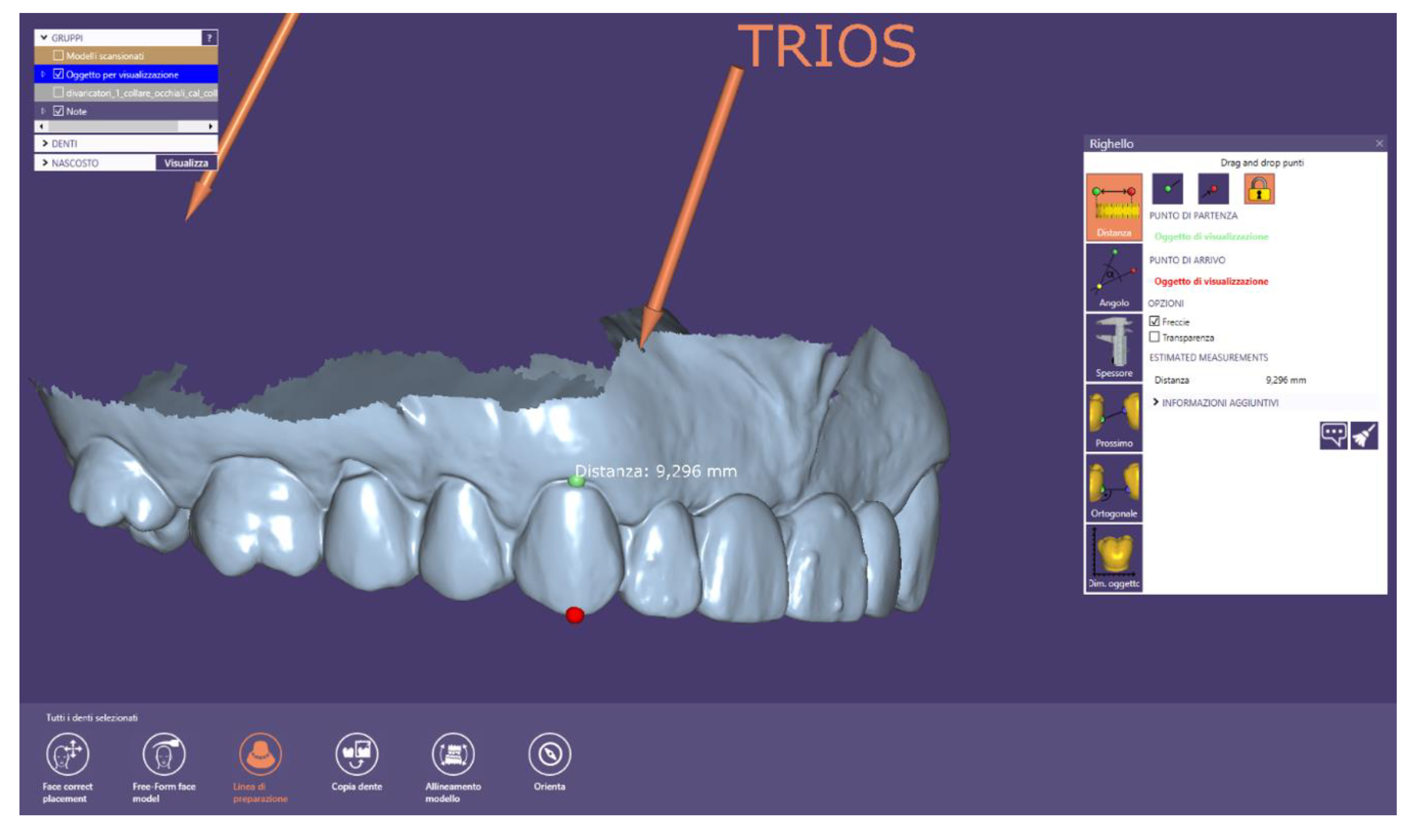
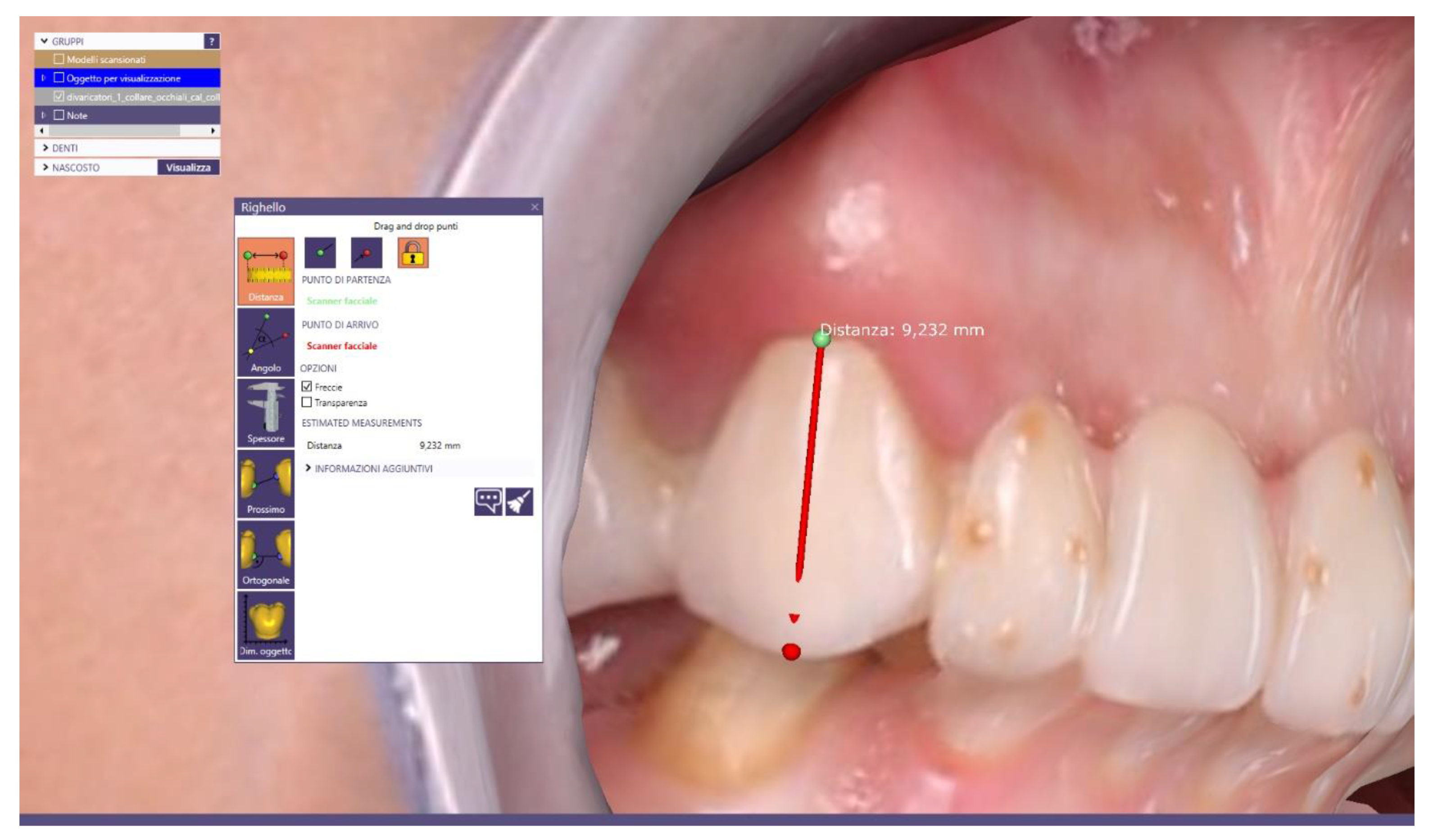
- one in the apico-coronal sense, from the most apical point of the gingival parabola, i.e., the gingival zenith up to the incisal edge;
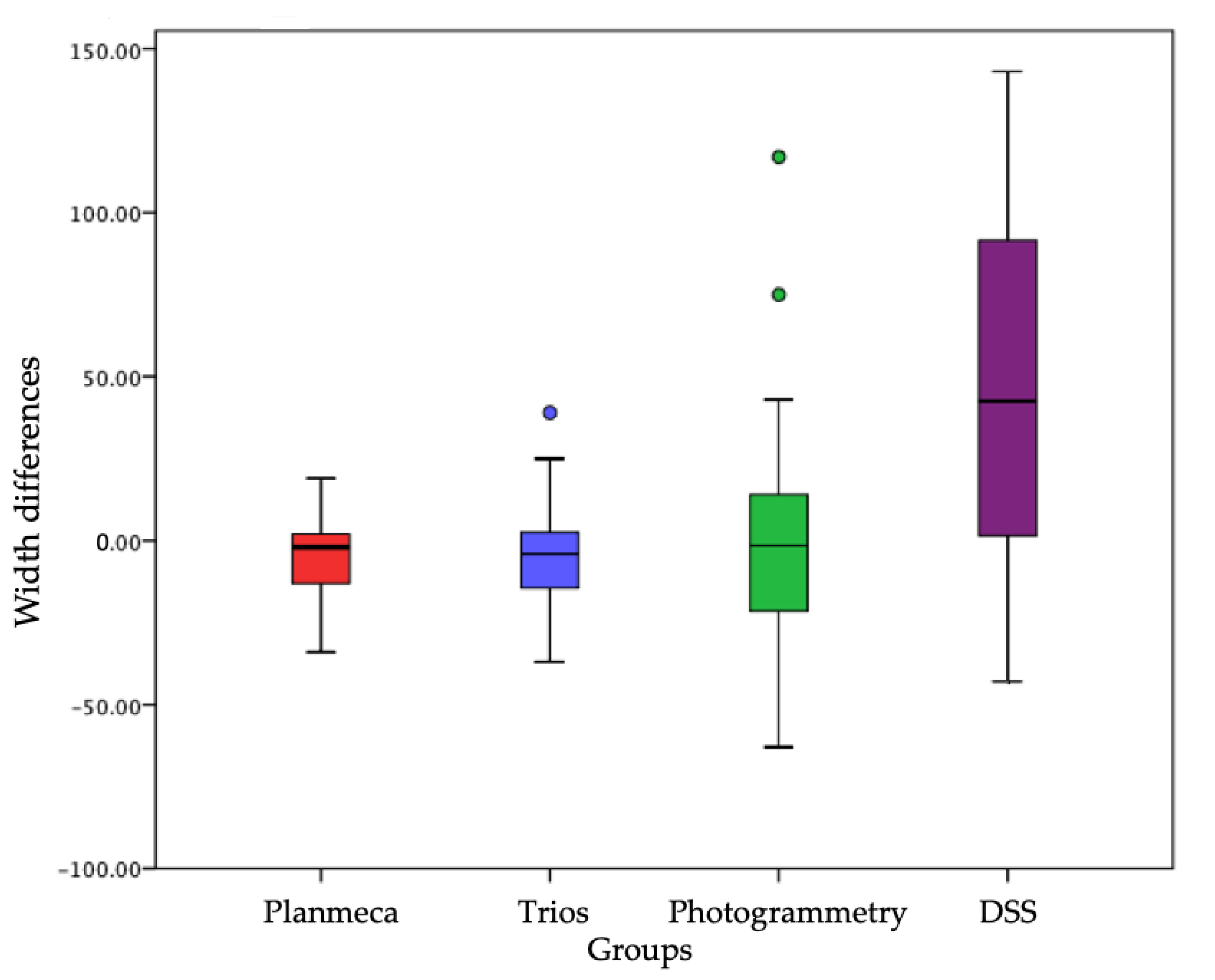
- the other in the mesio-distal direction, at the level of the equator of the dental elements, from the most mesial to the most distal point; i.e., the maximum mesio-distal diameter level.
- 3D model obtained from the scanning in the laboratory of the stone model of the upper arch (figure MODEL IN PLASTER) (Figure A1);
- 3D model of the upper arch created using the Planmeca Emerald intraoral scanner (figure MODEL EMERALD) (Figure A2);
- 3D model of the upper arch acquired with the 3Shape TRIOS intraoral scanner (3shape, Copenhagen, Denmark) (TRIOS MODEL) (Figure A3);
- 3D model of the face detected with the photogrammetric technique (PHOTOGRAMMETRIC EXAMINATION) (Figure A4);
- digital photography of the face according to the Digital Smile System (DSS) photographic protocol (EXAM DSS) (Figure A5).
2.4. Variables and Measurements
- to assess the accuracy of each of the intraoral scanners used (Planmeca Emerald and 3Shape TRIOS) compared to the scan of the plaster model, taken as a reference virtual object;
- to assess which of the two intraoral scanners is accurate; i.e., closer to the reference values;
- to verify the accuracy of the 3D model of the face, obtained with photogrammetric technique and acquired with the cheeks apart, compared to the scan of the plaster model;
- to verify the accuracy of the 2D face photograph, obtained according to the DSS protocol with the cheeks apart, compared to the scan of the plaster model;
- to assess which of the photogrammetry and the DSS protocol is the most precise method—that is, closer to the reference values.
2.5. Statistical Evaluation
3. Results
3.1. Experimental Study Results
3.2. Statistical Evaluation
4. Discussion
5. Conclusions
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
Appendix A





References
- Yilmaz, B.; Abou-Ayash, S. A digital intraoral implant scan technique using a combined healing abutment and scan body system. J. Prosthet. Dent. 2019. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Sailer, I.; Muhlemann, S.; Fehmer, V.; Hammerle, C.H.F.; Benic, G.I. Randomized controlled clinical trial of digital and conventional workflows for the fabrication of zirconia-ceramic fixed partial dentures. Part I: Time efficiency of complete-arch digital scans versus conventional impressions. J. Prosthet. Dent. 2019, 121, 69–75. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Runkel, C.; Guth, J.F.; Erdelt, K.; Keul, C. Digital impressions in dentistry-accuracy of impression digitalisation by desktop scanners. Clin. Oral Investig. 2019. [Google Scholar] [CrossRef] [PubMed]
- De Stefano, R.; Bruno, A.; Muscatello, M.; Cedro, C.; Cervino, G.; Fiorillo, L. Fear and anxiety managing methods during dental treatments: Systematic review of recent data. Minerva Stomatol. 2019, 68. in press. [Google Scholar]
- De Stefano, R. Psychological factors in dental patient care: Odontophobia. Medicina 2019, 55, 678. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Patel, J.; Winters, J.; Walters, M. Intraoral digital impression technique for a neonate with bilateral cleft lip and palate. Cleft Palate-Craniofacial J. 2019, 56, 1120–1123. [Google Scholar] [CrossRef]
- Pagano, S.; Moretti, M.; Marsili, R.; Ricci, A.; Barraco, G.; Cianetti, S. Evaluation of the accuracy of four digital methods by linear and volumetric analysis of dental impressions. Materials 2019, 12, 1958. [Google Scholar] [CrossRef] [Green Version]
- Molinero-Mourelle, P.; Lam, W.; Cascos-Sanchez, R.; Azevedo, L.; Gomez-Polo, M. Photogrammetric and intraoral digital impression technique for the rehabilitation of multiple unfavorably positioned dental implants—A clinical report. J. Oral Implantol. 2019. [Google Scholar] [CrossRef]
- Mangano, F.; Mangano, C.; Margiani, B.; Admakin, O. Combining intraoral and face scans for the design and fabrication of computer-assisted design/computer-assisted manufacturing (cad/cam) polyether-ether-ketone (peek) implant-supported bars for maxillary overdentures. Scanning 2019. [Google Scholar] [CrossRef] [Green Version]
- Kihara, H.; Hatakeyama, W.; Komine, F.; Takafuji, K.; Takahashi, T.; Yokota, J.; Oriso, K.; Kondo, H. Accuracy and practicality of intraoral scanner in dentistry: A literature review. J. Prosthodont. Res. 2019. [Google Scholar] [CrossRef]
- Cicciù, M.; Cervino, G.; Milone, D.; Risitano, G. FEM analysis of dental implant-abutment interface overdenture components and parametric evaluation of Equator® and Locator® prosthodontics attachments. Materials 2019, 12, 592. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Cervino, G.; Fiorillo, L.; Arzukanyan, A.V.; Spagnuolo, G.; Cicciù, M. Dental restorative digital workflow: Digital smile design from aesthetic to function. Dent. J. 2019, 7, 30. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Cappare, P.; Sannino, G.; Minoli, M.; Montemezzi, P.; Ferrini, F. Conventional versus digital impressions for full arch screw-retained maxillary rehabilitations: A randomized clinical trial. Int J. Environ. Res. Public Health 2019, 16, 829. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Cervino, G.; Fiorillo, L.; Herford, A.S.; Laino, L.; Troiano, G.; Amoroso, G.; Crimi, S.; Matarese, M.; D’Amico, C.; Nastro Siniscalchi, E.; et al. Alginate Materials and Dental Impression Technique: A Current State of the Art and Application to Dental Practice. Mar. Drugs 2018, 17, 18. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Zitzmann, N.U.; Kovaltschuk, I.; Lenherr, P.; Dedem, P.; Joda, T. Dental students’ perceptions of digital and conventional impression techniques: A randomized controlled Trial. J. Dent. Educ. 2017, 81, 1227–1232. [Google Scholar] [CrossRef] [PubMed]
- Cicciù, M.; Herford, A.S.; Cervino, G.; Troiano, G.; Lauritano, F.; Laino, L. Tissue fluorescence imaging (VELscope) for quick non-invasive diagnosis in oral pathology. J. Craniofacial Surgery 2017, 28, e112–e115. [Google Scholar] [CrossRef] [PubMed]
- Sakornwimon, N.; Leevailoj, C. Clinical marginal fit of zirconia crowns and patients’ preferences for impression techniques using intraoral digital scanner versus polyvinyl siloxane material. J. Prosthet. Dent. 2017, 118, 386–391. [Google Scholar] [CrossRef]
- Rancitelli, D.; Cicciù, M.; Lini, F.; Fumagalli, D.; Frigo, A.C.; Maiorana, C. Reproducibility of a digital method to evaluate soft tissue modifications: A study of inter and intra-operative measurement concordance. Open Dent. J. 2017, 11, 171–180. [Google Scholar] [CrossRef] [Green Version]
- Joda, T.; Lenherr, P.; Dedem, P.; Kovaltschuk, I.; Bragger, U.; Zitzmann, N.U. Time efficiency, difficulty, and operator’s preference comparing digital and conventional implant impressions: A randomized controlled trial. Clin. Oral Implant. Res. 2017, 28, 1318–1323. [Google Scholar] [CrossRef]
- Joda, T.; Bragger, U. Patient-centered outcomes comparing digital and conventional implant impression procedures: A randomized crossover trial. Clin. Oral Implant. Res. 2016, 27, e185–e189. [Google Scholar] [CrossRef]
- Gjelvold, B.; Chrcanovic, B.R.; Korduner, E.K.; Collin-Bagewitz, I.; Kisch, J. Intraoral digital impression technique compared to conventional impression technique. A randomized clinical trial. J. Prosthodont. 2016, 25, 282–287. [Google Scholar] [CrossRef] [PubMed]
- Gherlone, E.; Cappare, P.; Vinci, R.; Ferrini, F.; Gastaldi, G.; Crespi, R. Conventional versus digital impressions for “all-on-four” restorations. Int. J. Oral Maxillofac. Implant. 2016, 31, 324–330. [Google Scholar] [CrossRef] [PubMed]
- Yuzbasioglu, E.; Kurt, H.; Turunc, R.; Bilir, H. Comparison of digital and conventional impression techniques: Evaluation of patients’ perception, treatment comfort, effectiveness and clinical outcomes. BMC Oral Health 2014, 14, 10. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Newby, E.E.; Bordas, A.; Kleber, C.; Milleman, J.; Milleman, K.; Keogh, R.; Murphy, S.; Butler, A.; Bosma, M.L. Quantification of gingival contour and volume from digital impressions as a novel method for assessing gingival health. Int. Dent. J. 2011, 61, 4–12. [Google Scholar] [CrossRef]
- Lo Giudice, G.; Cutroneo, G.; Centofanti, A.; Artemisia, A.; Bramanti, E.; Militi, A.; Rizzo, G.; Favaloro, A.; Irrera, A.; Lo Giudice, R.; et al. Dentin morphology of root canal surface: A quantitative evaluation based on a scanning electronic microscopy study. BioMed Res. Int. 2015, 2015. [Google Scholar] [CrossRef] [Green Version]
- Cervino, G.; Romeo, U.; Lauritano, F.; Bramanti, E.; Fiorillo, L.; D’Amico, C.; Milone, D.; Laino, L.; Campolongo, F.; Rapisarda, S.; et al. Fem and von mises analysis of OSSTEM ® dental implant structural components: evaluation of different direction dynamic loads. Open Dent. J. 2018, 12, 219–229. [Google Scholar] [CrossRef] [Green Version]
- Bramanti, E.; Matacena, G.; Cecchetti, F.; Arcuri, C.; Cicciù, M. Oral health-related quality of life in partially edentulous patients before and after implant therapy: A 2-year longitudinal study. Oral Implantol. 2013, 6, 37–42. [Google Scholar] [CrossRef]
- Fiorillo, L.; Cervino, G.; Herford, A.S.; Lauritano, F.; D’Amico, C.; Lo Giudice, R.; Laino, L.; Troiano, G.; Crimi, S.; Cicciù, M. Interferon Crevicular Fluid Profile and Correlation with Periodontal Disease and Wound Healing: A Systemic Review of Recent Data. Int. J. Mol. Sci. 2018, 19, 1908. [Google Scholar] [CrossRef] [Green Version]
- Mangano, C.; Perrotti, V.; Shibli, J.A.; Mangano, F.; Ricci, L.; Piattelli, A.; Iezzi, G. Maxillary sinus grafting with biphasic calcium phosphate ceramics: Clinical and histologic evaluation in man. Int. J. Oral Maxillofac. Implant. 2013, 28, 51–56. [Google Scholar] [CrossRef] [Green Version]
- Cattoni, F.; Teté, G.; Calloni, A.M.; Manazza, F.; Gastaldi, G.; Capparè, P. Milled versus moulded mock-ups based on the superimposition of 3D meshes from digital oral impressions: A comparative in vitro study in the aesthetic area. BMC Oral Health 2019, 19, 230. [Google Scholar] [CrossRef]
- Mendes, T.A.; Marques, D.; Lopes, L.P.; Carames, J. Total digital workflow in the fabrication of a partial removable dental prostheses: A case report. SAGE Open Med. Case Rep. 2019, 7, 2050313x19871131. [Google Scholar] [CrossRef] [PubMed]
- Spielau, T.; Hauschild, U.; Katsoulis, J. Computer-assisted, template-guided immediate implant placement and loading in the mandible: A case report. BMC Oral Health 2019, 19, 55. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Mangano, F.G.; Hauschild, U.; Veronesi, G.; Imburgia, M.; Mangano, C.; Admakin, O. Trueness and precision of 5 intraoral scanners in the impressions of single and multiple implants: A comparative in vitro study. BMC Oral Health 2019, 19, 101. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Mangano, C.; Mangano, F.; Shibli, J.A.; Luongo, G.; De Franco, M.; Briguglio, F.; Figliuzzi, M.; Eccellente, T.; Rapani, C.; Piombino, M.; et al. Prospective clinical evaluation of 201 direct laser metal forming implants: Results from a 1-year multicenter study. Lasers Med. Sci. 2012, 27, 181–189. [Google Scholar] [CrossRef] [PubMed]
- Zarone, F.; Ferrari, M.; Mangano, F.G.; Leone, R.; Sorrentino, R. “Digitally Oriented Materials”: Focus on Lithium Disilicate Ceramics. Int. J. Dent. 2016, 2016, 10. [Google Scholar] [CrossRef]
- Giuliani, A.; Manescu, A.; Larsson, E.; Tromba, G.; Luongo, G.; Piattelli, A.; Mangano, F.; Iezzi, G.; Mangano, C. In vivo regenerative properties of coralline-derived (biocoral) scaffold grafts in human maxillary defects: Demonstrative and comparative study with beta-tricalcium phosphate and biphasic calcium phosphate by synchrotron radiation X-Ray microtomography. Clin. Implant Dent. Relat. Res. 2014, 16, 736–750. [Google Scholar] [CrossRef]
- Cervino, G.; Fiorillo, L.; Iannello, G.; Santonocito, D.; Risitano, G.; Cicciù, M. Sandblasted and acid etched titanium dental implant surfaces systematic review and confocal microscopy evaluation. Materials 2019, 12, 1763. [Google Scholar] [CrossRef] [Green Version]
- Cervino, G.; Fiorillo, L.; Monte, I.P.; De Stefano, R.; Laino, L.; Crimi, S.; Bianchi, A.; Herford, A.S.; Biondi, A.; Cicciù, M. Advances in antiplatelet therapy for dentofacial surgery patients: focus on past and present strategies. Materials 2019, 12, 1524. [Google Scholar] [CrossRef] [Green Version]
- Cervino, G.; Fiorillo, L.; Arzukanyan, A.; Spagnuolo, G.; Campagna, P.; Cicciù, M. Application of bioengineering devices for the stress evaluation in dentistry: the last 10 years fem parametric analysis of outcomes and current trends. Minerva Stomatol. 2019, 29, 565–574. [Google Scholar]
- Germano, F.; Bramanti, E.; Arcuri, C.; Cecchetti, F.; Cicciù, M. Atomic force microscopy of bacteria from periodontal subgingival biofilm: Preliminary study results. Eur. J. Dent. 2013, 7, 152–158. [Google Scholar] [CrossRef] [Green Version]
- Maiorana, C.; Beretta, M.; Grossi, G.B.; Santoro, F.; Herford, A.S.; Nagursky, H.; Cicciù, M. Histomorphometric evaluation of anorganic bovine bone coverage to reduce autogenous grafts resorption: Preliminary results. Open Dent. J. 2011, 5, 71–78. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Cicciù, M.; Cervino, G.; Terranova, A.; Risitano, G.; Raffaele, M.; Cucinotta, F.; Santonocito, D.; Fiorillo, L. Prosthetic and mechanical parameters of the facial bone under the load of different dental implant shapes: A parametric study. Prostheses 2020, 1, 41–53. [Google Scholar] [CrossRef] [Green Version]
- Cicciù, M. Prosthesis: new technological opportunities and innovative biomedical devices. Prostheses 2020, 1, 1–2. [Google Scholar] [CrossRef] [Green Version]



{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Intraoral Scanners | PZ01 | PZ02 | PZ03 | PZ04 | ||||
|---|---|---|---|---|---|---|---|---|
| Dental Size | H | W | H | W | H | W | H | W |
| 1.1 Scanner | 6.98 | 6.09 | 9.48 | 8.23 | 8.81 | 8.11 | 8.30 | 8.08 |
| 1.2 Scanner | 5.94 | 3.61 | 7.38 | 6.49 | 7.62 | 6.05 | 6.85 | 6.15 |
| 1.3 Scanner | 9.20 | 7.60 | 9.56 | 7.35 | 9.07 | 7.48 | 7.85 | 7.88 |
| 1.1 Emerald | 6.95 | 6.02 | 9.43 | 8.21 | 9.01 | 8.15 | 8.25 | 8.10 |
| 1.2 Emerald | 5.92 | 3.75 | 6.52 | 6.50 | 7.23 | 6.14 | 6.74 | 6.53 |
| 1.3 Emerald | 9.21 | 7.53 | 9.10 | 7.16 | 8.95 | 7.61 | 7.69 | 7.96 |
| 1.1 Trios | 6.67 | 5.70 | 9.40 | 8.13 | 8.81 | 8.18 | 8.44 | 8.19 |
| 1.2 Trios | 5.90 | 3.47 | 7.09 | 6.42 | 7.11 | 6.02 | 6.73 | 6.34 |
| 1.3 Trios | 9.20 | 7.62 | 9.10 | 7.10 | 8.88 | 7.85 | 7.80 | 7.97 |
| 1.1 Photogrammetry | 6.47 | 5.34 | 9.66 | 8.24 | 8.97 | 8.01 | 8.39 | 8.28 |
| 1.2 Photogrammetry | 6.01 | 3.48 | 7.14 | 6.46 | 7.47 | 6.27 | 6.75 | 6.78 |
| 1.3 Photogrammetry | 9.23 | 7.44 | 9.18 | 7.55 | 9.10 | 7.83 | 7.69 | 7.84 |
| 1.1 DSS | 6.42 | 5.40 | 9.45 | 8.11 | 8.56 | 7.54 | 8.30 | 8.45 |
| 1.2 DSS | 5.96 | 3.33 | 7.17 | 5.48 | 6.90 | 5.23 | 6.59 | 5.72 |
| 1.3 DSS | 8.69 | 9.32 | 8.60 | 7.39 | ||||
| Intraoral Scanners | PZ05 | PZ06 | PZ07 | PZ08 | ||||
|---|---|---|---|---|---|---|---|---|
| Dental Size | H | W | H | W | H | W | H | W |
| 1.1 Scanner | 8.61 | 8.57 | 10.75 | 10.04 | 13.71 | 7.24 | 11.45 | 9.11 |
| 1.2 Scanner | 7.53 | 7.04 | 7.47 | 7.03 | 13.34 | 6.89 | 9.82 | 7.18 |
| 1.3 Scanner | 8.77 | 7.73 | 8.57 | 7.58 | 12.60 | 8.83 | 10.77 | 8.22 |
| 1.1 Emerald | 8.66 | 8.77 | 10.75 | 10.24 | 13.43 | 9.14 | 11.40 | 9.12 |
| 1.2 Emerald | 7.48 | 7.23 | 7.74 | 7.02 | 14.87 | 6.68 | 9.85 | 7.45 |
| 1.3 Emerald | 8.92 | 7.78 | 8.56 | 7.60 | 13.02 | 9.12 | 10.74 | 8.23 |
| 1.1 Trios | 8.54 | 8.88 | 10.71 | 10.06 | 13.53 | 9.11 | 11.36 | 9.12 |
| 1.2 Trios | 7.32 | 7.24 | 7.57 | 7.02 | 14.96 | 6.59 | 9.69 | 7.41 |
| 1.3 Trios | 8.88 | 7.85 | 8.53 | 7.59 | 13.02 | 8.99 | 10.93 | 8.13 |
| 1.1 Photogrammetry | 8.65 | 8.75 | 10.51 | 8.87 | 13.55 | 9.29 | 11.33 | 9.12 |
| 1.2 Photogrammetry | 7.17 | 7.17 | 7.78 | 7.14 | 13.93 | 6.75 | 9.25 | 7.65 |
| 1.3 Photogrammetry | 8.85 | 7.90 | 8.94 | 7.41 | 12.22 | 8.71 | 10.65 | 8.06 |
| 1.1 DSS | 8.77 | 8.61 | 10.77 | 9.83 | 13.52 | 9.07 | 11.08 | 9.22 |
| 1.2 DSS | 7.49 | 5.68 | 7.69 | 5.95 | 14.19 | 5.87 | 9.48 | 6.37 |
| 1.3 DSS | 8.81 | 8.72 | 12.81 | 10.80 | ||||
| Intraoral Scanners | PZ09 | PZ10 | PZ11 | PZ12 | ||||
|---|---|---|---|---|---|---|---|---|
| Dental Size | H | W | H | W | H | W | H | W |
| 1.1 Scanner | 10.75 | 8.87 | 9.15 | 8.72 | 10.61 | 8.15 | 9.02 | 8.05 |
| 1.2 Scanner | 9.35 | 7.08 | 6.69 | 6.45 | 9.10 | 7.18 | 8.15 | 6.27 |
| 1.3 Scanner | 10.34 | 8.70 | 10.35 | 7.69 | 10.02 | 7.87 | 9.18 | 8.09 |
| 1.1 Emerald | 10.93 | 9.22 | 9.09 | 8.92 | 10.57 | 8.13 | 9.14 | 8.09 |
| 1.2 Emerald | 9.20 | 7.05 | 6.72 | 6.70 | 9.09 | 7.52 | 8.12 | 6.40 |
| 1.3 Emerald | 10.17 | 8.64 | 10.43 | 7.54 | 9.92 | 7.56 | 8.97 | 7.97 |
| 1.1 Trios | 10.66 | 9.20 | 9.06 | 8.85 | 10.65 | 8.21 | 9.05 | 7.95 |
| 1.2 Trios | 9.20 | 7.14 | 6.57 | 6.68 | 9.15 | 9.50 | 8.22 | 6.35 |
| 1.3 Trios | 10.10 | 8.78 | 10.41 | 7.67 | 9.95 | 7.64 | 9.20 | 8.03 |
| 1.1 photogrammetry | 10.37 | 9.24 | 9.19 | 8.93 | 10.02 | 7.93 | 9.25 | 8.23 |
| 1.2 photogrammetry | 9.25 | 7.21 | 6.49 | 6.83 | 8.79 | 7.04 | 8.11 | 6.73 |
| 1.3 photogrammetry | 10.04 | 8.87 | 10.58 | 8.22 | 9.91 | 7.44 | 9.43 | 7.86 |
| 1.1 DSS | 10.74 | 8.89 | 8.61 | 9.15 | 10.26 | 8.23 | 8.33 | 7.98 |
| 1.2 DSS | 8.72 | 6.04 | 6.17 | 6.03 | 8.68 | 5.75 | 7.64 | 5.58 |
| 1.3 DSS | 9.74 | 10.20 | 9.69 | 8.82 | ||||
| Intraoral Scanners | 1.1 | 1.2 | 1.3 | |||
|---|---|---|---|---|---|---|
| Mean ± SD and p | Mean ± SD and p | Mean ± SD and p | ||||
| H | W | H | W | H | W | |
| Scanner | 9.80 ± 1.76 | 8.28 ± 0.98 | 8.27 ± 1.96 | 6.45 ± 0.99 | 9.69 ± 1.24 | 7.92 ± 0.47 |
| Emerald | 9.80 ± 1.71 | 8.51 ± 1.02 | 8.29 ± 2.39 | 6.58 ± 0.99 | 9.64 ± 1.37 | 7.89 ± 0.55 |
| p = 0.9991 | p = 0.5800 | p = 0.9823 | p = 0.7501 | p = 0.9261 | p = 0.8987 | |
| Trios | 9.74 ± 1.76 | 8.47 ± 1.07 | 8.29 ± 2.40 | 6.68 ± 1.35 | 9.67 ± 1.36 | 7.94 ± 0.52 |
| p = 0.9324 | p = 0.6623 | p = 0.9802 | p = 0.6390 | p = 0.9654 | p = 0.9348 | |
| Photogrammetry | 9.70 ± 1.73 | 8.35 ± 1.06 | 8.18 ± 2.09 | 6.62 ± 1.05 | 9.65 ± 1.15 | 7.93 ± 0.48 |
| p = 0.8852 | p = 0.8636 | p = 0.9128 | p = 0.6844 | p = 0.9341 | p = 0.9625 | |
| DSS | 9.58 ± 1.83 | 8.37 ± 1.13 | 8.06 ± 2.20 | 5.59 ± 0.77 | 9.47 ± 1.37 | |
| p = 0.7526 | p = 0.8308 | p = 0.8044 | p = 0.0254 | p = 0.6790 | ||
© 2019 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Lavorgna, L.; Cervino, G.; Fiorillo, L.; Di Leo, G.; Troiano, G.; Ortensi, M.; Galantucci, L.; Cicciù, M. Reliability of a Virtual Prosthodontic Project Realized through a 2D and 3D Photographic Acquisition: An Experimental Study on the Accuracy of Different Digital Systems. Int. J. Environ. Res. Public Health 2019, 16, 5139. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph16245139
Lavorgna L, Cervino G, Fiorillo L, Di Leo G, Troiano G, Ortensi M, Galantucci L, Cicciù M. Reliability of a Virtual Prosthodontic Project Realized through a 2D and 3D Photographic Acquisition: An Experimental Study on the Accuracy of Different Digital Systems. International Journal of Environmental Research and Public Health. 2019; 16(24):5139. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph16245139
Chicago/Turabian StyleLavorgna, Luca, Gabriele Cervino, Luca Fiorillo, Giovanni Di Leo, Giuseppe Troiano, Marco Ortensi, Luigi Galantucci, and Marco Cicciù. 2019. "Reliability of a Virtual Prosthodontic Project Realized through a 2D and 3D Photographic Acquisition: An Experimental Study on the Accuracy of Different Digital Systems" International Journal of Environmental Research and Public Health 16, no. 24: 5139. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph16245139