Class Time Physical Activity Programs for Primary School Aged Children at Specialist Schools: A Systematic Mapping Review

 ,
,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Eligibility Criteria
2.1.1. Population
2.1.2. Intervention
2.1.3. Comparison
2.1.4. Outcome
2.1.5. Study Type
2.2. Information Sources
2.3. Search Strategy
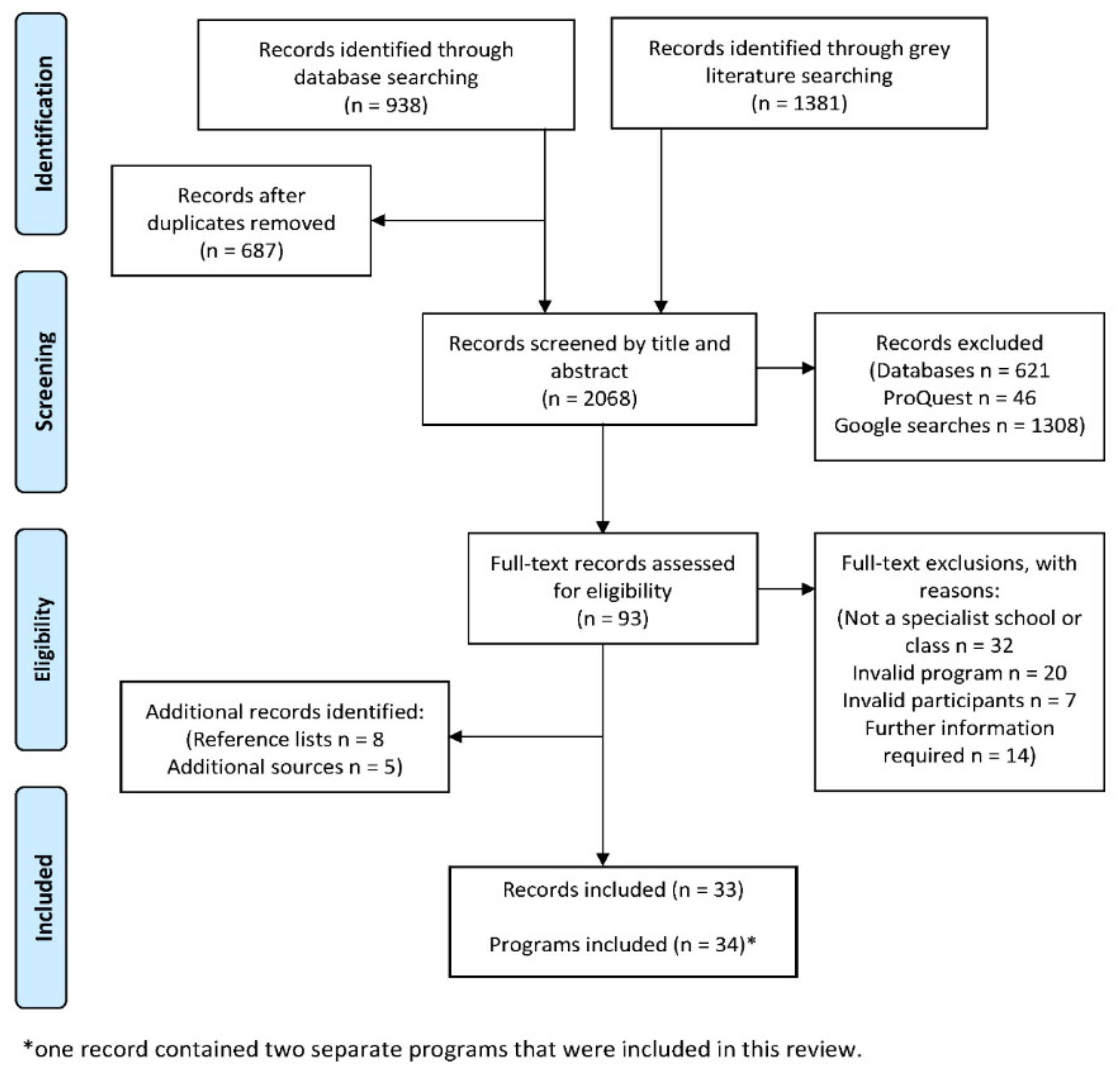
2.4. Study Selection
2.5. Data Extraction
2.6. Risk of Bias
2.7. Data Analysis
3. Results
3.1. Study Characteristics
3.2. What PA Programs Have Been Implemented in Specialist Schools and Classes, and What Have They Involved?
3.2.1. Dance/Drama
3.2.2. Motor Activities
3.2.3. Games/Play
3.2.4. Running
3.2.5. Swimming
3.2.6. Stretching
3.2.7. Other Activities
3.3. Types of Programs Implemented with Particular Disability Populations
4. Discussion
4.1. Program Components
4.2. Classroom “Break” Programs
4.3. Program Evaluations
4.4. Considerations for Particular Disability Populations
4.5. Risk of Bias
4.6. Strengths and Limitations
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- World Health Organization. World Report on Disability; World Health Organization: Geneva, Switzerland, 2011. [Google Scholar]
- Australian Bureau of Statistics. Children with a disability. In Australian Social Trends; Australian Bureau of Statistics: Canberra, Australia, 2012. [Google Scholar]
- Australian Institute of Health and Welfare. Children with Disabilities in Australia; AIHW cat. no. DIS 38; Australian Institute of Health and Welfare: Canberra, Australia, 2004.
- Gadow, K.D.; Guttmann-Steinmetz, S.; Rieffe, C.; DeVincent, C.J. Depression symptoms in boys with autism spectrum disorder and comparison samples. J. Autism Dev. Disord. 2012, 42, 1353–1363. [Google Scholar] [CrossRef] [PubMed]
- World Health Organization. Summary World Report on Disability; World Health Organization: Geneva, Switzerland, 2011. [Google Scholar]
- Martin, J. Benefits and barriers to physical activity for individuals with disabilities: A social-relational model of disability perspective. Disabil. Rehabil. 2013, 35, 2030–2037. [Google Scholar] [CrossRef] [PubMed]
- Jung, J.; Leung, W.; Schram, B.M.; Yun, J. Meta-Analysis of Physical Activity Levels in Youth With and Without Disabilities. Adapt Phys. Activ. Q 2018, 35, 381–402. [Google Scholar] [CrossRef]
- Poitras, V.J.; Gray, C.E.; Borghese, M.M.; Carson, V.; Chaput, J.P.; Janssen, I.; Katzmarzyk, P.T.; Pate, R.R.; Connor Gorber, S.; Kho, M.E. Systematic review of the relationships between objectively measured physical activity and health indicators in school-aged children and youth. Appl. Physiol. Nutr. Metab. 2016, 41, S197–S239. [Google Scholar] [CrossRef]
- Strong, W.B.; Malina, R.M.; Blimkie, C.J.; Daniels, S.R.; Dishman, R.K.; Gutin, B.; Hergenroeder, A.C.; Must, A.; Nixon, P.A.; Pivarnik, J.M. Evidence based physical activity for school-age youth. J. Pediatr. 2005, 146, 732–737. [Google Scholar] [CrossRef]
- Johnson, C.C. The benefits of physical activity for youth with developmental disabilities: A systematic review. Am. J. Health Promot. 2009, 23, 157–167. [Google Scholar] [CrossRef]
- Murphy, N.A.; Carbone, P.S. Promoting the participation of children with disabilities in sports, recreation, and physical activities. Pediatrics 2008, 121, 1057–1061. [Google Scholar] [CrossRef] [Green Version]
- Dahan-Oliel, N.; Shikako-Thomas, K.; Majnemer, A. Quality of life and leisure participation in children with neurodevelopmental disabilities: A thematic analysis of the literature. Qual. Life Res. 2012, 21, 427–439. [Google Scholar] [CrossRef]
- Wachob, D.; Lorenzi, D.G. Brief report: Influence of physical activity on sleep quality in children with autism. J. Autism Dev. Disord. 2015, 45, 2641–2646. [Google Scholar] [CrossRef]
- Janssen, I.; LeBlanc, A.G. Systematic review of the health benefits of physical activity and fitness in school-aged children and youth. Int. J. Behav. Nutr. Phys. Act. 2010, 7, 40. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Howells, K.; Sivaratnam, C.; May, T.; Lindor, E.; McGillivray, J.; Rinehart, N. Efficacy of Group-Based Organised Physical Activity Participation for Social Outcomes in Children with Autism Spectrum Disorder: A Systematic Review and Meta-analysis. J. Autism Dev. Disord. 2019, 49, 3290–3308. [Google Scholar] [CrossRef] [PubMed]
- World Health Organization. Global Recommendations on Physical Activity for Health; World Health Organization: Geneva, Switzerland, 2010. [Google Scholar]
- Fuezeki, E.; Engeroff, T.; Banzer, W. Health benefits of light-intensity physical activity: A systematic review of accelerometer data of the National Health and nutrition examination survey (NHANES). Sports Med. 2017, 47, 1769–1793. [Google Scholar] [CrossRef] [PubMed]
- Powell, K.E.; Paluch, A.E.; Blair, S.N. Physical activity for health: What kind? How much? How intense? On top of what? Annu. Rev. Public Health 2011, 32, 349–365. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Rosenbaum, P.; Gorter, J. The ‘F-words’ in childhood disability: I swear this is how we should think! Child Care Health Dev. 2012, 38, 457–463. [Google Scholar] [CrossRef]
- Anderson, L.S.; Heyne, L.A. Physical activity for children and adults with disabilities: An issue of “amplified” importance. Disabil. Health J. 2010, 3, 71–73. [Google Scholar] [CrossRef]
- Maiano, C. Prevalence and risk factors of overweight and obesity among children and adolescents with intellectual disabilities. Obes. Rev. 2011, 12, 189–197. [Google Scholar] [CrossRef]
- Einarsson, I.O.; Olafsson, A.; Hinriksdóttir, G.; Jóhannsson, E.; Daly, D.; Arngrímsson, S.A. Differences in physical activity among youth with and without intellectual disability. Med. Sci. Sports Exerc. 2015, 47, 411–418. [Google Scholar] [CrossRef]
- Carlon, S.L.; Taylor, N.F.; Dodd, K.J.; Shields, N. Differences in habitual physical activity levels of young people with cerebral palsy and their typically developing peers: A systematic review. Disabil. Rehabil. 2013, 35, 647–655. [Google Scholar] [CrossRef]
- Hinckson, E.A.; Curtis, A. Measuring physical activity in children and youth living with intellectual disabilities: A systematic review. Res. Dev. Disabil. 2013, 34, 72–86. [Google Scholar] [CrossRef]
- Rimmer, J.A.; Rowland, J.L. Physical activity for youth with disabilities: A critical need in an underserved population. Dev. Neurorehabil. 2008, 11, 141–148. [Google Scholar] [CrossRef]
- Jones, R.A.; Downing, K.; Rinehart, N.J.; Barnett, L.M.; May, T.; McGillivray, J.A.; Papadopoulos, N.V.; Skouteris, H.; Timperio, A.; Hinkley, T. Physical activity, sedentary behavior and their correlates in children with autism spectrum disorder: A systematic review. PLoS ONE 2017, 12, e0172482. [Google Scholar] [CrossRef] [PubMed]
- Boddy, L.M.; Downs, S.J.; Knowles, Z.R.; Fairclough, S.J. Physical activity and play behaviours in children and young people with intellectual disabilities: A cross-sectional observational study. Sch. Psychol. Int. 2015, 36, 154–171. [Google Scholar] [CrossRef] [Green Version]
- Leung, W.; Siebert, E.A.; Yun, J. Measuring physical activity with accelerometers for individuals with intellectual disability: A systematic review. Res. Dev. Disabil. 2017, 67, 60–70. [Google Scholar] [CrossRef] [PubMed]
- Downs, S.J.; Fairclough, S.J.; Knowles, Z.R.; Boddy, L.M. Physical activity patterns in youth with intellectual disabilities. Adapt. Phys. Activ. Q 2016, 33, 374–390. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Wouters, M.; Evenhuis, H.M.; Hilgenkamp, T.I. Physical activity levels of children and adolescents with moderate-to-severe intellectual disability. J. Appl. Res. Intell. Disab. 2019, 32, 131–142. [Google Scholar] [CrossRef]
- Webster, C.A.; Russ, L.; Vazou, S.; Goh, T.; Erwin, H. Integrating movement in academic classrooms: Understanding, applying and advancing the knowledge base. Obes. Rev. 2015, 16, 691–701. [Google Scholar] [CrossRef]
- Hills, A.P.; Dengel, D.R.; Lubans, D.R. Supporting public health priorities: Recommendations for physical education and physical activity promotion in schools. Prog. Cardiovasc. Dis. 2015, 57, 368–374. [Google Scholar] [CrossRef] [Green Version]
- Einarsson, I.O.; Johannsson, E.; Daly, D.; Arngrímsson, S.Á. Physical activity during school and after school among youth with and without intellectual disability. Res. Dev. Disabil. 2016, 56, 60–70. [Google Scholar] [CrossRef]
- Telama, R.; Yang, X.; Viikari, J.; Välimäki, I.; Wanne, O.; Raitakari, O. Physical activity from childhood to adulthood: A 21-year tracking study. Am. J. Prev. Med. 2005, 28, 267–273. [Google Scholar] [CrossRef]
- McMinn, D.; Rowe, D.A.; Trim, V. Classroom-based physical activity breaks: Potential for use with children with special educational needs. Int. J. Phys. Educ. 2011, 20–30. [Google Scholar]
- Society of Health and Physical Educators (SHAPE) America. What is CSPAP? Available online: https://www.shapeamerica.org/cspap/what.aspx (accessed on 22 May 2019).
- Sit, C.; McKenzie, T.L.; Cerin, E.; Chow, B.C.; Huang, W.Y.; Yu, J. Physical Activity and Sedentary Time among Children with Disabilities at School. Med. Sci. Sports Exerc. 2017, 49, 292–297. [Google Scholar] [CrossRef] [PubMed]
- Sit, C.H.P.; McKenzie, T.L.; Cerin, E.; McManus, A.; Lian, J. Physical activity for children in special school environment. Hong Kong Med. J. 2013, 19, S42–S44. [Google Scholar]
- Powell, E.; Woodfield, L.A.; Nevill, A.A. Children’s physical activity levels during primary school break times: A quantitative and qualitative research design. Eur. Phy. Educ. Rev. 2016, 22, 82–98. [Google Scholar] [CrossRef]
- Erwin, H.; Beighle, A.; Carson, R.L.; Castelli, D.M. Comprehensive school-based physical activity promotion: A review. Quest 2013, 65, 412–428. [Google Scholar] [CrossRef]
- Dinkel, D.; Schaffer, C.; Snyder, K.; Lee, J.M. They just need to move: Teachers’ perception of classroom physical activity breaks. Teach. Teach. Educ. 2017, 63, 186–195. [Google Scholar] [CrossRef]
- Goh, T.L.; Hannon, J.; Webster, C.; Podlog, L.; Newton, M. Effects of a TAKE 10! classroom-based physical activity intervention on third-to fifth-grade children’s on-task behavior. J. Phys. Act. Health 2016, 13, 712–718. [Google Scholar] [CrossRef]
- Lowden, K.; Powney, J.; Davidson, J.; James, C. The Class Moves!® Pilot in Scotland and Wales: An evaluation; SCRE Research Report No 100; The Scottish Council for Research in Education: Glasgow, Scotland, 2001. [Google Scholar]
- Pangrazi, R.P.; Beighle, A.; Vehige, T.; Vack, C. Impact of Promoting Lifestyle Activity for Youth (PLAY) on children’s physical activity. J. Sch. Health 2003, 73, 317–321. [Google Scholar] [CrossRef]
- Mahar, M.T.; Murphy, S.K.; Rowe, D.A.; Golden, J.; Shields, A.T.; Raedeke, T.D. Effects of a classroom-based program on physical activity and on-task behavior. Med. Sci. Sports Exerc. 2006, 38, 2086. [Google Scholar] [CrossRef] [Green Version]
- Liu, A.; Hu, X.; Ma, G.; Cui, Z.; Pan, Y.; Chang, S.; Zhao, W.; Chen, C. Evaluation of a classroom-based physical activity promoting programme. Obes. Rev. 2008, 9, 130–134. [Google Scholar] [CrossRef]
- Smedegaard, S. Move for Well-being in Schools: Implementing physical activity in the Danish Public School. ACHPER Act. Healthy Mag. 2016, 23, 30–35. [Google Scholar]
- Naylor, P.J.; Nettlefold, L.; Race, D.; Hoy, C.; Ashe, M.C.; Higgins, J.W.; McKay, H.A. Implementation of school based physical activity interventions: A systematic review. Prev. Med. 2015, 72, 95–115. [Google Scholar] [CrossRef] [PubMed]
- McMullen, J.; Kulinna, P.; Cothran, D. Physical activity opportunities during the school day: Classroom teachers’ perceptions of using activity breaks in the classroom. J. Teach. Phys. Educ. 2014, 33, 511–527. [Google Scholar] [CrossRef]
- Kibbe, D.L.; Hackett, J.; Hurley, M.; McFarland, A.; Schubert, K.G.; Schultz, A.; Harris, S. Ten Years of TAKE 10!®: Integrating physical activity with academic concepts in elementary school classrooms. Prev. Med. 2011, 52, S43–S50. [Google Scholar] [CrossRef] [PubMed]
- Watson, A.; Timperio, A.; Brown, H.; Best, K.; Hesketh, K.D. Effect of classroom-based physical activity interventions on academic and physical activity outcomes: A systematic review and meta-analysis. Int. J. Behav. Nutr. Phys. Act. 2017, 14, 114. [Google Scholar] [CrossRef] [Green Version]
- Martin, R.; Murtagh, E.M. Effect of active lessons on physical activity, academic, and health outcomes: A systematic review. Res. Q. Exerc. Sport 2017, 88, 149–168. [Google Scholar] [CrossRef]
- Erwin, H.; Fedewa, A.; Beighle, A.; Ahn, S. A quantitative review of physical activity, health, and learning outcomes associated with classroom-based physical activity interventions. J. Appl. Sch. Psychol. 2012, 28, 14–36. [Google Scholar] [CrossRef]
- Bloemen, M.; Van Wely, L.; Mollema, J.; Dallmeijer, A.; de Groot, J. Evidence for increasing physical activity in children with physical disabilities: A systematic review. Dev. Med. Child Neurol. 2017, 59, 1004–1010. [Google Scholar] [CrossRef]
- Frey, G.C.; Temple, V.A.; Stanish, H.I. Interventions to promote physical activity for youth with intellectual disabilities. Salud. Publica. Mex. 2017, 59, 437–445. [Google Scholar] [CrossRef]
- McGarty, A.; Downs, S.; Melville, C.; Harris, L. A systematic review and meta-analysis of interventions to increase physical activity in children and adolescents with intellectual disabilities. J. Intellect. Disabil. Res. 2018, 62, 312–329. [Google Scholar] [CrossRef] [Green Version]
- Biddle, S.J.; Fox, K.; Boutcher, S. Physical Activity and Psychological Well-Being; Routledge: London, UK, 2003. [Google Scholar]
- Thomas, B.; Ciliska, D.; Dobbins, M.; Micucci, S. A process for systematically reviewing the literature: Providing the research evidence for public health nursing interventions. Worldviews Evid. Based Nurs. 2004, 1, 176–184. [Google Scholar] [CrossRef]
- Organisation for Economic Co-Operation and Development (OECD). CO1.9: Child Disability; OECD: Paris, France, 2012. [Google Scholar]
- Halladay, A.K.; Bishop, S.; Constantino, J.N.; Daniels, A.M.; Koenig, K.; Palmer, K.; Messinger, D.; Pelphrey, K.; Sanders, S.J.; Singer, A.T. Sex and gender differences in autism spectrum disorder: Summarizing evidence gaps and identifying emerging areas of priority. Mol. Autism 2015, 6, 36. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Singer, J.D.; Butler, J.A.; Palfrey, J.S.; Walker, D.K. Characteristics of special education placements: Findings from probability samples in five metropolitan school districts. J. Spec. Educ. 1986, 20, 319–337. [Google Scholar] [CrossRef]
- Carnahan, C.; Musti-Rao, S.; Bailey, J. Promoting Active Engagement in Small Group Learning Experiences for Students with Autism and Significant Learning Needs. Educ. Treat. Children 2009, 32, 37–61. [Google Scholar] [CrossRef]
- Moher, D.; Liberati, A.; Tetzlaff, J.; Altman, D.G.; The PRISMA Group. Preferred reporting items for systematic reviews and meta-analyses: The PRISMA statement. PLoS Med. 2009, 6. [Google Scholar] [CrossRef] [Green Version]
- Lu, L.; Petersen, F.; Lacroix, L.; Rousseau, C. Stimulating creative play in children with autism through sandplay. Arts Psychother 2010, 37, 56–64. [Google Scholar] [CrossRef]
- Hall, S.L.; Deacon, K.F. Effects noted from the use of the Frostig training program with trainable retardates. Train. Sch. Bull. (Vinel.) 1970, 67, 20–24. [Google Scholar]
- Allen, J.I. Jogging can modify disruptive behaviors. Teach Except Child 1980, 12, 66–70. [Google Scholar] [CrossRef]
- Allen, B.J. The Effect of Dance/Movement on the Self-Concept of Developmentally Handicapped Fourth and Fifth Grade Students. Ph.D. Thesis, The Ohio State University, Columbus, OH, USA, 1989. [Google Scholar]
- Barton, B. The Effects of an Aerobic Dance Program on the Self- Concept and the Development of Physical Fitness in Educable Mentally Retarded Children. Master’s Thesis, The Pennsylvania State University, University Park, PA, USA, 1979. [Google Scholar]
- Bass, C.K. Running Can Modify Classroom Behavior. J. Learn. Disabil. 1985, 18, 160–161. [Google Scholar] [CrossRef]
- Bellitto, F.C. A Correlation between Gross Motor Development and Academic Success for Children Exhibiting Gross Motor Deficiencies upon Entering School. Ph.D. Thesis, University of Nebraska, Lincoln, NE, USA, 1981. [Google Scholar]
- Bernstein, B. Becoming involved: Spolin theater games in classes for the educationally handicapped. Theory Pract. 1985, 24, 219–223. [Google Scholar] [CrossRef]
- Bothma, J.-M.v.d.M.; Dunn, M.; Kokot, S. The impact of a developmental movement programme on the performance of rural hearing-impaired children on the Griffiths Scales of Mental Development. S. Afr. J. Psychol. 2014, 44, 36–47. [Google Scholar] [CrossRef]
- Bruce, S.; Fasy, C.; Gulick, J.; Jones, J.; Pike, E. Making Morning Circle Meaningful. Teach Except Child Plus 2006, 2. [Google Scholar]
- Davis, K.; Zhang, G.; Hodson, P. Promoting health-related fitness for elementary students with intellectual disabilities through a specifically designed activity program. J. Policy Pract. Intellect. Disabil. 2011, 8, 77–84. [Google Scholar] [CrossRef]
- Dickinson, K.; Place, M. The impact of a computer-based activity program on the social functioning of children with autistic spectrum disorder. Games Health J. 2016, 5, 209–215. [Google Scholar] [CrossRef] [PubMed]
- Doherty, G. The Effects of Specific Perceptual-Motor Training on the Physical Fitness, Perceptual-Motor Skills, Academic Readiness, and Academic Functioning of Educable Mentally Retarded Children. Ph.D. Thesis, York University, Toronto, ON, Canada, 1971. [Google Scholar]
- Everhart, B.; Dimon, C.; Stone, D.; Desmond, D.; Casilio, M. The influence of daily structured physical activity on academic progress of elementary students with intellectual disabilities. Education 2012, 133, 298–312. [Google Scholar]
- Fontana, D.; Diaper, R. Effects of a Special Remedial Movement Programme upon Linguistic Development in ESN (M) Boys. Educ. Psychol. (Lond.) 1981, 1, 261–266. [Google Scholar] [CrossRef]
- Gitter, L.L. Montessori principles applied in a class of mentally retarded children. Ment. Retard. 1967, 5, 26. [Google Scholar] [PubMed]
- Government of Western Australia (Department of Health). WA Healthy Schools Project Case Studies 2014; Government of Western Australia: Perth, Australia, 2015.
- Halle, J.W.; Silverman, N.A.; Regan, L. The effects of a data-based exercise program on physical fitness of retarded children. Educ. Train. Ment. Retard. 1983, 18, 221–225. [Google Scholar]
- Miller, H.; Rynders, J.E.; Schleien, S.J. Drama: A medium to enhance social interaction between students with and without mental retardation. Ment. Retard. 1993, 31, 228–233. [Google Scholar]
- Ministry of Education Singapore. Special Education for Exceptional Lives; Ministry of Education: Singapore, 2018.
- Nelson, C.; Paul, K.; Barnhill, B.A. Creative Dance-Based Communication Intervention for Children With Multiple Disabilities Including Sensory Impairment. Perspect. ASHA Spec. Interest Groups 2017, 2, 70–80. [Google Scholar] [CrossRef]
- Nicholson, H. The Effects of Antecedent Physical Activity on the Academic Engagement of Children with Autism Spectrum Disorders. Ph.D. Thesis, University of Connecticut, Storrs, CT, USA, 2008. [Google Scholar]
- Nunley, R.L. A physical fitness program for the mentally retarded in the public schools. Phys. Ther. 1965, 45, 947. [Google Scholar]
- Oriel, K.N.; George, C.L.; Peckus, R.; Semon, A. The effects of aerobic exercise on academic engagement in young children with autism spectrum disorder. Pediatr. Phys. Ther. 2011, 23, 187–193. [Google Scholar] [CrossRef] [PubMed]
- Roswal, P.M.; Sherrill, C.; Roswal, G.M. A comparison of data based and creative dance pedagogies in teaching mentally retarded youth. Adapt. Phys. Activ. Q. 1988, 5, 212–222. [Google Scholar] [CrossRef]
- Mary Brooksbank School. Mary Brooksbank School Annual School Report; Mary Brooksbank School: Rosemeadow, Australia, 2011.
- Eastern Ranges School. Curriculum Specialist: Aquatics. Available online: https://easternrangesschool.vic.edu.au/curriculum/ (accessed on 3 September 2019).
- Eastern Ranges School. Curriculum Specialist: Outdoor Education. Available online: https://easternrangesschool.vic.edu.au/curriculum/ (accessed on 3 September 2019).
- South Ballajura Campus. Students with Special Needs: Community Access in Education Support. Available online: https://southballajuraps.wa.edu.au/students-with-special-needs/ (accessed on 3 September 2019).
- Seham, J. Dance partners: A model of inclusive arts education for children and teens with different abilities. In The Intersection of Arts Education and Special Education: Exemplary Programs and Approaches; Malley, S., Ed.; The John F. Kennedy Center for the Performing Arts: Washington, DC, USA, 2012; pp. 81–100. [Google Scholar]
- Spanbauer, P. Movement Arts: Unlocking the World. Perspect. Educ. Deaf. 1990, 8, 12–15. [Google Scholar]
- Taylor, L.N. Developmental Dance in the Education of the Educable Mentally Handicapped Child. Ph.D. Thesis, University of Illinois at Urbana-Champaign, Champaign, IL, USA, 1964. [Google Scholar]
- Walton, W.T. The use of a relaxation curriculum and biofeedback training in the classroom to reduce inappropriate behaviors of emotionally handicapped children. Behav. Disord. 1979, 5, 10–18. [Google Scholar] [CrossRef]
- Odom, S.L.; Brantlinger, E.; Gersten, R.; Horner, R.H.; Thompson, B.; Harris, K.R. Research in special education: Scientific methods and evidence-based practices. Except. Child. 2005, 71, 137–148. [Google Scholar] [CrossRef] [Green Version]
- Skoning, S.N. Movement and Dance in the Inclusive Classroom. Teach. Except. Child Plus 2008, 4, 1–11. [Google Scholar]
- Zitomer, M.R. ‘Dance Makes Me Happy’: Experiences of children with disabilities in elementary school dance education. Res. Danc. Educ. 2016, 17, 218–234. [Google Scholar] [CrossRef]
- May, T.; Chan, E.S.; Lindor, E.; McGinley, J.; Skouteris, H.; Austin, D.; McGillivray, J.; Rinehart, N.J. Physical, cognitive, psychological and social effects of dance in children with disabilities: Systematic review and meta-analysis. Disabil. Rehabil. 2019, 21, 1–14. [Google Scholar] [CrossRef]
- Water Safety and Swimming. Available online: https://education.qld.gov.au/curriculum/school-curriculum/water-safety-and-swimming (accessed on 26 April 2019).
- Swimming and Water Safety Education. Available online: https://www.education.vic.gov.au/school/teachers/teachingresources/discipline/physed/Pages/swimmingsafety.aspx (accessed on 26 April 2019).
- Interm Swimming. Available online: https://www.education.wa.edu.au/interm-swimming (accessed on 26 April 2019).
- Downs, S.J.; Boddy, L.M.; Knowles, Z.R.; Fairclough, S.J.; Stratton, G. Exploring opportunities available and perceived barriers to physical activity engagement in children and young people with Down syndrome. Eur. J. Spec. Needs Educ. 2013, 28, 270–287. [Google Scholar] [CrossRef] [Green Version]
- Mayes, S.D.; Calhoun, S.L. Learning, attention, writing, and processing speed in typical children and children with ADHD, autism, anxiety, depression, and oppositional-defiant disorder. Child Neuropsychol. 2007, 13, 469–493. [Google Scholar] [CrossRef]
- Pesce, C.; Leone, L.; Motta, A.; Marchetti, R.; Tomporowski, P.D. From Efficacy to Effectiveness of a “Whole Child” Initiative of Physical Activity Promotion. Transl. J. Am. Coll. Sports Med. 2016, 1, 18–29. [Google Scholar] [CrossRef]
- Han, J.C.; Lawlor, D.A.; Kimm, S.Y. Childhood obesity. Lancet 2010, 375, 1737–1748. [Google Scholar] [CrossRef]
- Barr-Anderson, D.J.; AuYoung, M.; Whitt-Glover, M.C.; Glenn, B.A.; Yancey, A.K. Integration of short bouts of physical activity into organizational routine: A systematic review of the literature. Am. J. Prev. Med. 2011, 40, 76–93. [Google Scholar] [CrossRef] [PubMed]
- Einfeld, S.L.; Ellis, L.A.; Emerson, E. Comorbidity of intellectual disability and mental disorder in children and adolescents: A systematic review. J. Intellect. Dev. Disabil. 2011, 36, 137–143. [Google Scholar] [CrossRef]
- Biddle, S.J. Emotion, mood and physical activity. In Physical Activity and Psychological Well-Being; Biddle, S.J., Fox, K., Boutcher, S., Eds.; Routledge: London, UK, 2003; pp. 75–97. [Google Scholar]
- Biddle, S.J.; Asare, M. Physical activity and mental health in children and adolescents: A review of reviews. Br. J. Sports Med. 2011, 45, 886–895. [Google Scholar] [CrossRef] [Green Version]
- Katz, D.L.; Cushman, D.; Reynolds, J.; Njike, V.; Treu, J.A.; Katz, C.; Walker, J.; Smith, E. Peer reviewed: Putting physical activity where it fits in the school day: Preliminary results of the ABC (Activity Bursts in the Classroom) for fitness program. Prev. Chronic Dis. 2010, 7, A82. [Google Scholar]
- Rimmer, J.H.; Chen, M.-D.; McCubbin, J.A.; Drum, C.; Peterson, J. Exercise intervention research on persons with disabilities: What we know and where we need to go. Am. J. Phys. Med. Rehabil. 2010, 89, 249–263. [Google Scholar] [CrossRef]
- Makel, M.C.; Plucker, J.A.; Freeman, J.; Lombardi, A.; Simonsen, B.; Coyne, M. Replication of special education research: Necessary but far too rare. Remedial. Spec. Educ. 2016, 37, 205–212. [Google Scholar] [CrossRef]
- Oliver, J.N. The effect of physical conditioning exercises and activities on the mental characteristics of educationally sub-normal boys. Br. J. Educ. Psychol. 1958, 28, 155–165. [Google Scholar] [CrossRef]
- Chasey, W.C.; Wyrick, W. Effects of a physical developmental program on psychomotor ability of retarded children. Am. J. Ment. Defic. 1971, 75, 566–570. [Google Scholar]







{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Concept | Search String |
|---|---|
| Participant | ((child*) OR (youth) OR (pediatric) OR (paediatric) OR (minors) OR (girls) OR (boys) OR (kid*) OR (student*)) |
| Participant | ((disab*) OR (“special needs”) OR (“developmental* challenge*”) OR (impair*) OR (handicap*) OR (“neurodevelopmental disorder*”) OR (retard*) OR (“development* disorder*”) OR (ASD) OR (“Autism Spectrum Disorder*”) OR (autis*) OR (ADHD) OR (“Attention Deficit Hyperactivity Disorder”) OR (“Cerebral Palsy”) OR (“Developmental Coordination Disorder”) OR (Blind) OR (Deaf*) OR (wheelchair) OR (“Down Syndrome”) OR (“Emotion* Behavio* Problem*”) OR (“Fragile X”) OR (Dyspraxia) OR (“Cystic Fibrosis”) OR (“Mental Disorder*”) OR (anxiety)) |
| Setting | ((classroom*) OR (class) OR (classes)) |
| Setting | ((“special* school*”) OR (“special education school*”) OR (“primary school*”) OR (“elementary school*”) OR (“junior school*”) OR (“infant school*”) OR (“special needs school*”) OR (“special development* school”)) |
| Intervention | ((“physical activit*”) OR (exercis*) OR (movement) OR (moving) OR (fitness) OR (“adapted physical education”) OR (“motor activit*”)) |
| Author (Year) | Country | Study Design | Comparison | Total Sample Size | Participant Sex | Participant Age in Years | Participant Disability Category | Participant Disability Description |
|---|---|---|---|---|---|---|---|---|
| Allen (1980) [66] | USA | Post-only | Days without jogging | N = 12 | M: 12 F: 0 | Range: - M: - | Special needs | Behavioural and/or perceptual disorders and limited gross motor skills in a class for children with learning difficulties. |
| Allen (1989) [67] | USA | Pre-post | Two classes at a different school continued with normal routine (1 h PE every week) | N = 28 | M: 15 F: 13 | Range: 9–15 M: 11.8 | Special needs | All had a developmental disability with MIQ of 69. The IQ range for the intervention group was 63–74 (MIQ = 68.5) and for the comparison group was 59–80 (MIQ = 69.5). |
| Barton (1979) [68] | USA | Pre-post | None | N = 21 | M: 13 F: 8 | Range: 9–16 M: - | ID | All had an ID. |
| Bass (1985) [69] | USA | Reversal | Non-running days | N = 6 | M: 4 F: 2 | Range: 8–11 M: - | Special needs | All had learning disabilities but did not receive medication. |
| Bellitto (1981) [70] | USA | Pre-post | None | N = 10 a | M: 7 F: 3 | Range: - M: - | ID | ID with deficits in gross and fine motor abilities, as well as auditory perception skills. |
| Bernstein (1985) [71] | USA | Observational | None | N = 48 | M: 42 F: 6 | Range: 6–9 M: - | Special needs | Majority had learning disorders and/or social adjustment difficulties. Many were 2 years behind anticipated age/grade levels. |
| Bothma, Dunn and Kokot (2014) [72] | South Africa | Pre-post | Comparison group took part in placebo activities | N = 18 | M: 10 F: 8 | Range: 4.5–8 M: - | Sensory impairments | All had severe to profound bilateral hearing loss. |
| Bruce, Fasy, Gulick, Jones and Pike (2006) [73] | USA | No evaluation reported | None | N = - | M: - F: - | Range: 3–10 M: - | Multiple disabilities | Severe and multiple disabilities including developmental delays, autism, physical disabilities and congenital deafblindness. |
| Carnahan, Musti-Rao and Bailey (2009) [62] | USA | Reversal | Not applicable b | N = 6 | M: 5 F: 1 | Range: 6–11 M: 9 y 1 m | ASD | Autism or “other health impairment”. All were 2–5 years below grade level functioning and had difficulties with academic engagement. |
| Davis, Zhang and Hodson (2011) [74] | USA | Pre-post | None | N = 25 | M: 16 F: 9 | Range: 8–12 M: 9.7 | ID | All had mild to moderate ID. |
| Dickinson and Place (2016) [75] | UK | RCT | Control group received standard school PE program | N = 67 a | M: 54 F: 13 | Range: not reported -11 M: - | ASD | ASD and a moderate or severe intellectual difficulty in classes for children with marked ASD. |
| Doherty (1971) [76] | Canada | Controlled trial | Control group received the usual PE | N = 29 | M: 16 F: 13 | Range: 8–12 M: - | ID | IQ between 49 and 65. Perceptual Motor program group: MIQ = 57.3. Physical Conditioning program group: MIQ = 55.8. Control group: MIQ = 56.7. |
| Everhart, Dimon, Stone, Desmond and Casilio (2012) [77] | USA | Reversal | Non-intervention periods | N = 13 | M: - F: - | Range: - M: - | ID | All had an ID. |
| Fontana and Diaper (1981) [78] | UK | Controlled trial | Control group continued with usual classroom tasks | N = 20 | M: 20 F: 0 | Range: 7–9 M: - | ID | Average IQ was 68.7 and 66.8 for the experimental and control groups respectively. Many did not meet the reading age classification and showed signs of significant maladjustment. |
| Gitter (1967) [79] | USA | No evaluation reported | None | N = 13 | M: 13 F: 0 | Range: 8–11 M: - | Special needs | IQ ranged from 58 to 72. |
| Government of WA, Department of Health (2015) [80] | Australia | No evaluation reported | None | N = 33 | M: - F: - | Range: - M: - | ID | All had an ID. |
| Hall and Deacon (1970) [65] | USA | Pre-post | Control group engaged in the usual special class curriculum | N = 40 a | M: - F: - | Range: 8–15 M: - | ID | All had an ID. Group 1 IQ: 30–53. Group 2 IQ: 30–54. |
| Halle, Silverman and Regan (1983) [81] | USA | Pre-post | None | N = 9 | M: - F: - | Range: 6.25–11.75 M: 8.5 | ID | All had an ID. |
| Lu, Petersen, Lacroix and Rousseau (2010) [64] | Canada | Action research | None | N = 25 | M: 23 F: 2 | Range: 7–12 M: 9.9 | ASD | All had ASD. Some also had motor delays and impaired hearing. |
| Miller, Rynders and Schleien (1993) [82] | USA | Controlled trial | Children were allocated to either the drama or cooperative games group | N = 8 a | M: - F: - | Range: - M: - c | ID | ID ranged from moderate to profound difficulty. |
| Ministry of Education, Singapore (2018) [83] | Singapore | No evaluation reported | None | N = - | M: - F: - | Range: - M: - | ID | All had an ID. |
| Nelson, Paul and Barnhill (2017) [84] | USA | No evaluation reported | None | N = - | M: - F: - | Range: 4–7 M: - | Sensory impairments | All had significant visual impairments and additional disabilities in a class for children who are blind or vision impaired. |
| Nicholson (2008) [85] | USA | Single subject multiple baseline | None | N = 4 | M: 4 F: 0 | Range: 9–9 M: - | ASD | All had high-functioning ASD. Two had a diagnosis of Asperger’s and two had a diagnosis of autism. |
| Nunley (1965) [86] | USA | Pre-post | None | N = 11 | M: - F: - | Range: 9–14 M: 12.5 | ID | All had a moderate ID. IQ ranged from 36 to 55. |
| Oriel, George, Peckus and Semon (2011) [87] | USA | RCT | Control condition where children did a classroom task without first doing aerobic exercise | N = 9 | M: 7 F: 2 | Range: 3–6 M: 5.2 | ASD | All met educational criteria for ASD, seven of which had a formal diagnosis of autism. One had a primary diagnosis of ID and one had a primary diagnosis of developmental delay. |
| Roswal, Sherrill and Roswal (1988) [88] | USA | Controlled trial | Classes were allocated to either the data-based dance pedagogy or the creative dance pedagogy | N = 35 | M: 23 F: 12 | Range: 11–16 M: - | ID | All had a moderate ID. |
| School Annual Report (2011) [89] | Australia | No evaluation reported | None | N = - | M: - F: - | Range: - M: - | ID | All had a moderate or severe ID. |
| School Website- Aquatics (n.d) [90] | Australia | No evaluation reported | None | N = - | M: - F: - | Range: - M: - | ASD | All had a diagnosis of ASD and many also had an ID, a language disorder and complex behaviours. |
| School Website- Outdoor Education (n.d) [91] | Australia | No evaluation reported | None | N = - | M: - F: - | Range: - M: - | ASD | All had a diagnosis of ASD and many also had an ID, a language disorder and complex behaviours. |
| School Website- Swimming (n.d) [92] | Australia | No evaluation reported | None | N = - | M: - F: - | Range: - M: - | Multiple disabilities | All had ASD and ID. |
| Seham (2012) [93] | USA | No evaluation reported | None | N = - | M: - F: - | Range: - M: - | Multiple disabilities | Severe physical, cognitive and emotional disabilities. |
| Spanbauer (1990) [94] | USA | No evaluation reported | None | N = - | M: - F: - | Range: - M: - | Sensory impairments | All had hearing impairments. There was also a Special Opportunities class for children who had other conditions in addition to deafness. |
| Taylor (1964) [95] | USA | Pre-post | None | N = 10 | M: 0 F: 10 | Range: 7–11 M: - | Special needs | IQ from 61 to 79 and all were functioning 2 to 4 years behind in school. |
| Walton (1979) [96] | USA | Pre-post | None | N = 5 | M: 5 F: 0 | Range: 12–14 M: - | Emotional difficulties | All had severe emotional difficulties. |
| Author (Year) | Program Category | Program Description | Program Duration | Program Delivered by | Program Location | Outcome Category(ies) | Outcome(s) Evaluated |
|---|---|---|---|---|---|---|---|
| Allen (1980) [66] | Running | Exercise periods consisting of warm up stretches, 5–10 min of continuous movement (run, jog or walk) and cool down stretches. | A 15 min session, twice per week for 6 weeks. | The classroom teacher | School grounds (on a 1/3 mile track around the school playground) | Behavioural | Classroom behaviour. |
| Allen (1989) [67] | Dance/drama | A dance/movement program. Lesson themes were based on Laban’s principles. Lessons aimed to increase body awareness, teach self-expression and communication through movement, and develop movement vocabulary. Lessons also aimed to increase social, psychomotor, cognitive and affective skills. Each lesson included a warm up, exploration of the daily theme, movement sequences, demonstration to the class and cool-down. | A 1 h session, every school morning for 2 weeks. | Researchers | School gymnasium (or large space in the school) | Psychological | Self-concept. |
| Barton (1979) [68] | Dance/drama | An aerobic dance program. Each lesson consisted of a warm-up, sit-ups, work-out and cool-down. The work-out segment (25–30 min) involved learning dance routines with a focus on monitoring the children’s heart rate to dictate intensity level. | A 45 min session, 3 times per week for 8 weeks. | Researchers (a graduate student helped with delivery) | School gymnasium (or ‘all purpose room’) | Physical Psychological | Physical fitness. Self-concept. |
| Bass (1985) [69] | Running | A running program. Children ran with the whole class on a quarter-mile track. | A 45 min session on alternate mornings for 4 weeks. | Not reported | Other (on a quarter-mile track) | Cognitive Behavioural | Attention span. Impulse control. |
| Bellitto (1981) [70] | Motor activities Games/play | A gross motor curriculum involving body image, non-locomotor and locomotor tasks. Body image tasks involved identifying body parts and included games such as the Hokey Pokey. Non-locomotor tasks involved activities such as balance, pushing/pulling, twisting and bouncing, and used games such as Simon Says and parachute play. Locomotor tasks involved activities such as running, hopping, lifting and leaping, and included games such as hopscotch and pretending to be animals. | A 45 min session, every school morning for 30 weeks. | The classroom teacher (who was also the researcher) | The classroom | Academic Physical | Academic abilities. Gross motor skills. |
| Bernstein (1985) [71] | Dance/drama | Spolin theatre games. These activities consist of more than 200 non-competitive group theatre games and exercises that promote social interaction and creativity. | A 45 min session, twice per week for 10 weeks. | Researchers | Not reported | Social | Children’s social relations. |
| Bothma, Dunn and Kokot (2014) [72] | Motor activities | The Wired to Learn program. This movement program consists of 10 main activities. Children learn and continue to practice the first movement activity until they can do it with ease. Children then proceed through the movement activities in order. | A 15–25 min session a, once per day (5 times per week) for 14 weeks. | Researchers | School room (the school clinic) | Other Physical Social Cognitive | Total developmental age. Locomotor development. Personal-social development. Language development. Eye-hand coordination development. Performance development. Practical reasoning development. |
| Bruce, Fasy, Gulick, Jones and Pike (2006) [73] | Stretching | Morning Circle meetings. Among many components, stretching and yoga have been included in Morning Circle meetings. The stretching component involved imitating the teacher. The yoga component consisted of students taking turns to select a yoga position and everyone imitating the position depicted. | Yoga components lasted no longer than 10 min. Other stretching activities were less than 10 min. | The classroom teacher | The classroom | No outcomes evaluated | None. |
| Carnahan, Musti-Rao and Bailey (2009) [62] | Dance/drama | A 30 min class group activity which consists of peer greetings, a calendar activity, a picture book activity and a movement/dancing activity. The movement or dancing time included activities such as the Hokey Pokey and YMCA. | Every school day for 8 weeks. The duration of the movement component specifically is unclear. | The classroom teacher | The classroom | Not applicable | Not applicable. |
| Davis, Zhang and Hodson (2011) [74] | Motor activities Games/play | The Motivate, Adapt, and Play program. Each 30 min session consisted of a warm up, cardiovascular activities, strength activities and a flexibility/closure activity. Tasks were designed to be fun activities presented in a game-style format that is appropriate and motivating for students with ID. | A 30 min session every school day for 8 weeks. | Classroom teacher 3 times a week. Graduate students twice a week. | Not reported | Physical | BMI. Cardiovascular endurance. Muscular endurance. Arm strength. Flexibility. |
| Dickinson and Place (2016) [75] | Games/play | Mario & Sonic at the Olympic Games on the Nintendo (Kyoto, Japan) Wii™. Children were able to choose to play athletics, aquatics, fencing or table tennis games electronically using the motion sensor of the Wii console remote. | A 15 min session, 3 times per week for 9 months. | Other (school staff) | School room (where PE would normally take place) | Social Other | Social functioning. Family functioning. |
| Doherty (1971) [76] | Motor activities Games/play | Two experimental programs; a Perceptual Motor program and a Physical Conditioning program. The Perceptual Motor program included activities such as balancing, throwing, hopping, crawling and obstacle courses. The Physical Conditioning program included activities such as races, tag, tug-of-war, sit ups and jumping. Activities gradually increased in difficulty and each child progressed at their own rate. | A 45 min session, 3 times per week for 5 months. | Researchers (university PE students and housewives assisted) | School gymnasium | Physical Academic Cognitive Other | Physical fitness. Perceptual motor abilities. Sensory integration skills. Academic functioning. Cognitive development. |
| Everhart, Dimon, Stone, Desmond and Casilio (2012) [77] | Dance/drama Other | Primary students followed a 10 min aerobic dance DVD. Intermediate students followed a 10 min TaeBo DVD. | A 10 min session on 19 days over a 30 day period. | The classroom teacher | Not reported | Academic | Mathematics academic activity. Language arts academic activity. |
| Fontana and Diaper (1981) [78] | Motor activities | A remedial movement program involving group and individual activities including locomotor, coordination, body awareness, laterality, rhythm and balance tasks. | A 45 min session, twice per week for 12 weeks. | Researchers | Not reported | Cognitive | Psycho-linguistic ability. |
| Gitter (1967) [79] | Motor activities | A circle or ellipse was drawn in the classroom and children were taught to walk along the line. Difficulty was applied by asking the child to balance objects (e.g., glass of water, a bell or a bean bag) while walking the line. | Not reported. | The classroom teacher | The classroom | No outcomes evaluated | None. |
| Government of WA, Department of Health (2015) [80] | Motor activities | Daily morning PA sessions. The sessions involve engaging in a set of gross movement skills in line with class therapy plans. The program also focuses on reflexes, with specific goals for each student. Some classes join mainstream groups in various fitness activity stations around the school. | A 15–20 min session a every school day. | The classroom teacher (sometimes Education Assistants). | Not reported | No outcomes evaluated. | None. |
| Hall and Deacon (1970) [65] | Motor activities | The Frostig Program for the Development of Visual Perception. This involved 60 min of work sheet activities and 30 min of physical activities. | A 30 min session every school day for 7 months. | Not reported | Not reported | Not applicable | Not applicable. |
| Halle, Silverman and Regan (1983) [81] | Running | A running program. Children ran a quarter mile track four times per week and a 600 yard track on the fifth day. Goals were set for each student to determine the distance they were required to run and the time they were required to complete it in. | A 15 min session, once per day for 7 months. | The classroom teacher | School grounds (perimeter of the playground or a footpath across school grounds) | Physical Other | Fitness. Program satisfaction. |
| Lu, Petersen, Lacroix and Rousseau (2010) [64] | Games/play | Sandplay workshops. Each session involved an opening ritual (5–10 min of physical, verbal and imaginary activities including mirroring, naming feelings and play-acting to encourage fine and gross motor movements and rhythm; e.g., pretending to be animals and eat different foods), sandplay, storytelling, and a closing ritual (a period of handclapping and dynamic physical movements). | 1 session per week for 10 weeks. The duration of the movement components specifically are not known. | Other (two art therapists) | The classroom | Not applicable | Not applicable. |
| Miller, Rynders and Schleien (1993) [82] | Dance/drama Games/play | A drama program and a cooperative games program. Each session commenced with a warm up exercise and brief instruction. Activities then took place for approx. 30 min before finishing with a brief discussion. The drama group engaged in theatre games and acting exercises designed by Spolin. The games group participated in non-competitive indoor and outdoor cooperative games. | One approx. 40 min session per week for 3 months. | Other (special education school staff) | Not reported | Social | Initiates positive social interactions. Target of positive social interactions. Quality of friendship. |
| Ministry of Education, Singapore (2018) [83] | Other | The 1–3-5 fitness program which involves students and teachers exercising together on Mondays, Wednesdays and Fridays b. The Friday exercise includes walking activities (e.g., climbing stairs and walking around the school hall). | A 15–20 min session a every Friday. | The classroom teacher | School room (hall) | No outcomes evaluated | None. |
| Nelson, Paul and Barnhill (2017) [84] | Motor activities Dance/drama | A greeting activity based on the BEST (Body, Energy, Space and Time) model that encouraged children to share their name and a body movement with the class. The activity also used rhythm and music to provide dance time and opportunities to repeat body movements. | Not reported. | Other (instructors and classroom aides) | The classroom | No outcomes evaluated | None. |
| Nicholson (2008) [85] | Running | A 12 min jog followed by five minutes of cool down exercises (i.e., walking and stretching). | A 12 min session, 3 times per week for 5 weeks. | Not reported | School gymnasium | Academic | Academic engaged time. |
| Nunley (1965) [86] | Motor activities | A PA program involving basic neuromuscular tasks and modified activities from the “Youth Physical Fitness: Elements of a School Centered Program”. Activities were added to target mobilization, strength and coordination and included tasks such as crawling, rolling, hopping, skipping, jumping, push-ups and star-jumps. Activities were changed according to performance improvements or indications of boredom. | A 30–45 min session a every school day for 15 months. | The classroom teacher (classroom aide also contributed). | School room (auditorium) | Physical Behavioural | Motor abilities. Endurance. Behaviour. |
| Oriel, George, Peckus and Semon (2011) [87] | Running | A period of running/jogging as a group. If children would not run, jumping on a mini trampoline was provided as an alternative. The session finished with light stretching and a glass of water. | 15 min sessions for 3 weeks. Total number of sessions not reported. | Researchers | Not reported | Academic Behavioural | Correct academic responses. Incorrect academic responses. Stereotypic behaviours. On-task behaviour. |
| Roswal, Sherrill and Roswal (1988) [88] | Dance/drama | Two experimental programs that aimed to teach children 10 skills relevant to dance using different approaches. The Data Based Dance group used a turn-taking approach where the teacher individually taught children the relevant skill while the rest waited for their turn. The Creative Dance group involved the teacher using 15 different lesson plans to teach the dance skills using movement exploration activities and games. | 40 lessons over 8 weeks. Each session lasted 30 min. | The classroom teacher (the investigator sometimes assisted) | Not reported | Physical Psychological | Dance skills. Motor performance. Self-concept. |
| School Annual Report (2011) [89] | Swimming | A swimming program. Children develop their swimming abilities and stroke skills and some also engage in hydrotherapy. | At least 1 session per week for the school year. Sessions ranged from 15 min to 1 h. | Specialist subject teacher (professional swimming instructors) | Not reported | No outcomes evaluated | None. |
| School Website- Aquatics (n.d) [90] | Swimming | An aquatics program. The program focuses on water safety (e.g., floating skills, water entry skills and rescue techniques) and swimming stroke skills (e.g., freestyle and backstroke). | A 30 min session, once per week for the school year. | Specialist subject teacher (swimming teachers) | Not reported | No outcomes evaluated | None. |
| School Website- Outdoor education (n.d) [91] | Games/play Other | An outdoor education program. Sessions involve a range of different community engagement activities including learning to share equipment, road safety, playing outdoor games and going on walking excursions. | 1 session every week of the school year. Session length varies depending on the class. | The classroom teacher (with a specialist teacher) | Mixed (in the classroom, outdoors and in the community) | No outcomes evaluated | None. |
| School Website- Swimming (n.d) [92] | Swimming | In-term swimming lessons to develop swimming skills. | A 45 min session every school day for 2 weeks. | Not reported | Not reported | No outcomes evaluated | None. |
| Seham (2012) [93] | Dance/drama | Dance sessions. Students from a special education class were partnered with typically developing children. Each lesson generally included an introduction game, warm-up stretching, learning and practicing choreography, ‘across the floor dancing’ and a ‘thank-you’. | 1, 45–55 min session a per week for a school year. | Specialist subject teacher (dance teachers with classroom teachers and therapists) | Not reported | No outcomes evaluated c | None. |
| Spanbauer (1990) [94] | Dance/drama | The ‘Movement Arts’ program, which combines dancing, acting, poetry and signed singing to assist children to learn to express themselves. Children also make connections between movement, emotions and language. | A 52 min session at least once per week for the school year. | Specialist subject teacher (a Movement Arts teacher) | School room (a Movement Arts classroom/ dance studio) | No outcomes evaluated | None. |
| Taylor (1964) [95] | Dance/drama | A dance program. Each session involved (1) gathering children using music and actions, (2) introduction of the daily activities which included tasks involving musical instruments and props, locomotor movements, games, learning dance routines, imagery movement tasks and improvising dances, for example, (3) an activity requested by students, (4) a relaxation period. | A 30–45 min session a, twice per week for just over 3 months. | Specialist subject teacher (dance teacher) | Mixed (one session in the gymnasium and the other in the classroom) | Cognitive Physical Other | Psycho-linguistic abilities. Sensori-motor skills. Visual perception skills. Auditory discrimination abilities. |
| Walton (1979) [96] | Stretching | Relaxation training. The sessions consisted of mental, physical (e.g., tensing and relaxing the body) and movement relaxation (e.g., slow-motion exercises). This program was accompanied by one, 20 min bio-feedback training session per week. | A 15 min session, 3 times per week for 16 weeks. | The classroom teacher | The classroom | Behavioural Physical | Inappropriate behaviours. Muscle tension. |
© 2019 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Emonson, C.; McGillivray, J.; Kothe, E.J.; Rinehart, N.; Papadopoulos, N. Class Time Physical Activity Programs for Primary School Aged Children at Specialist Schools: A Systematic Mapping Review. Int. J. Environ. Res. Public Health 2019, 16, 5140. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph16245140
Emonson C, McGillivray J, Kothe EJ, Rinehart N, Papadopoulos N. Class Time Physical Activity Programs for Primary School Aged Children at Specialist Schools: A Systematic Mapping Review. International Journal of Environmental Research and Public Health. 2019; 16(24):5140. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph16245140
Chicago/Turabian StyleEmonson, Chloe, Jane McGillivray, Emily J. Kothe, Nicole Rinehart, and Nicole Papadopoulos. 2019. "Class Time Physical Activity Programs for Primary School Aged Children at Specialist Schools: A Systematic Mapping Review" International Journal of Environmental Research and Public Health 16, no. 24: 5140. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph16245140