Psychosocial Stress, Sedentary Behavior, and Physical Activity during Pregnancy among Canadian Women: Relationships in a Diverse Cohort and a Nationwide Sample

 , ,
, ,  ,
,
Abstract
:1. Introduction
2. Materials and Methods
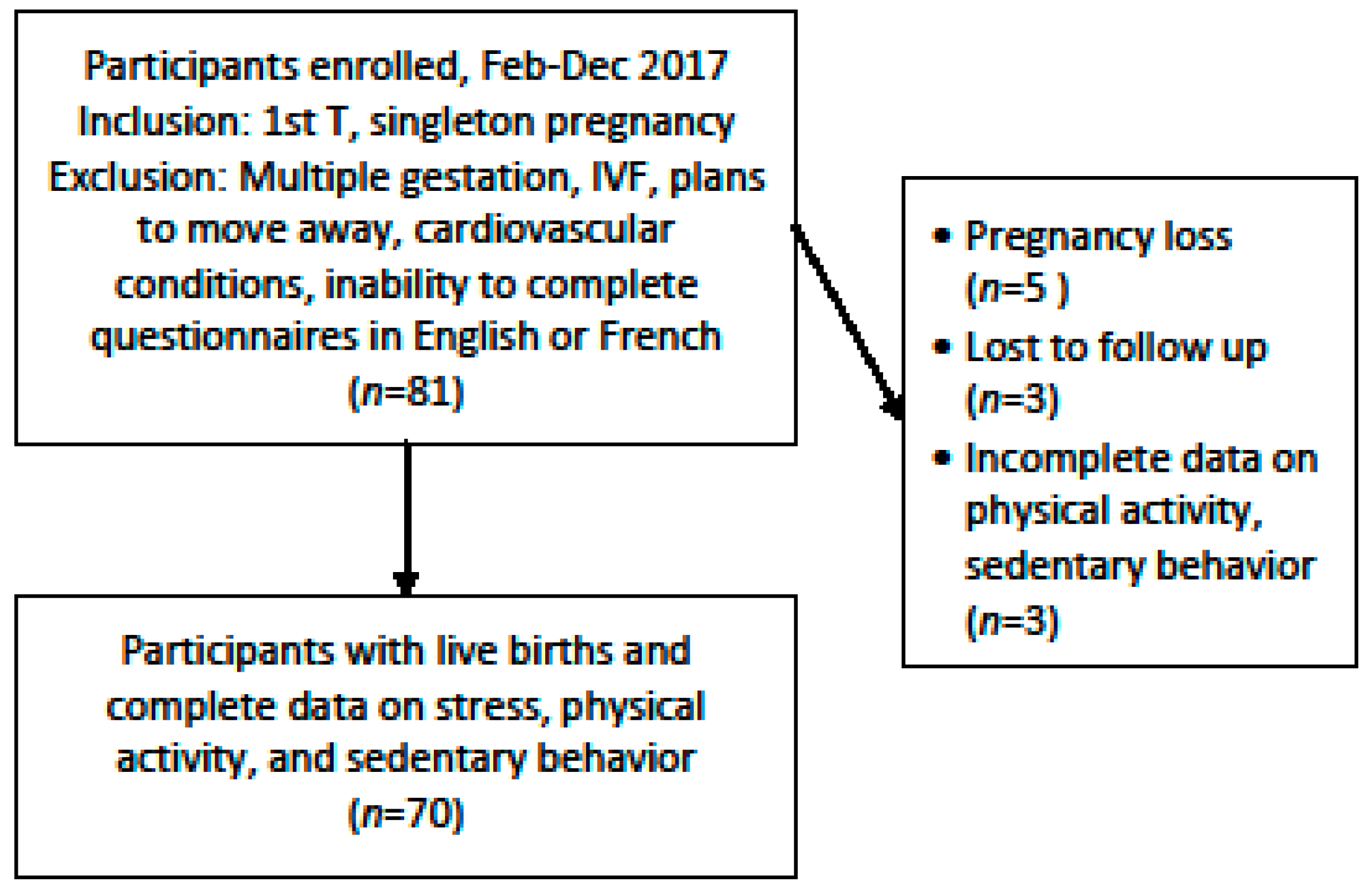
2.1. Montreal Cohort Study
2.1.1. Sample
2.1.2. Variables
2.1.3. Analyses
2.2. Nationally Representative Sample
2.2.1. Sample
2.2.2. Variables
2.2.3. Analyses
3. Results
3.1. Descriptive Statistics
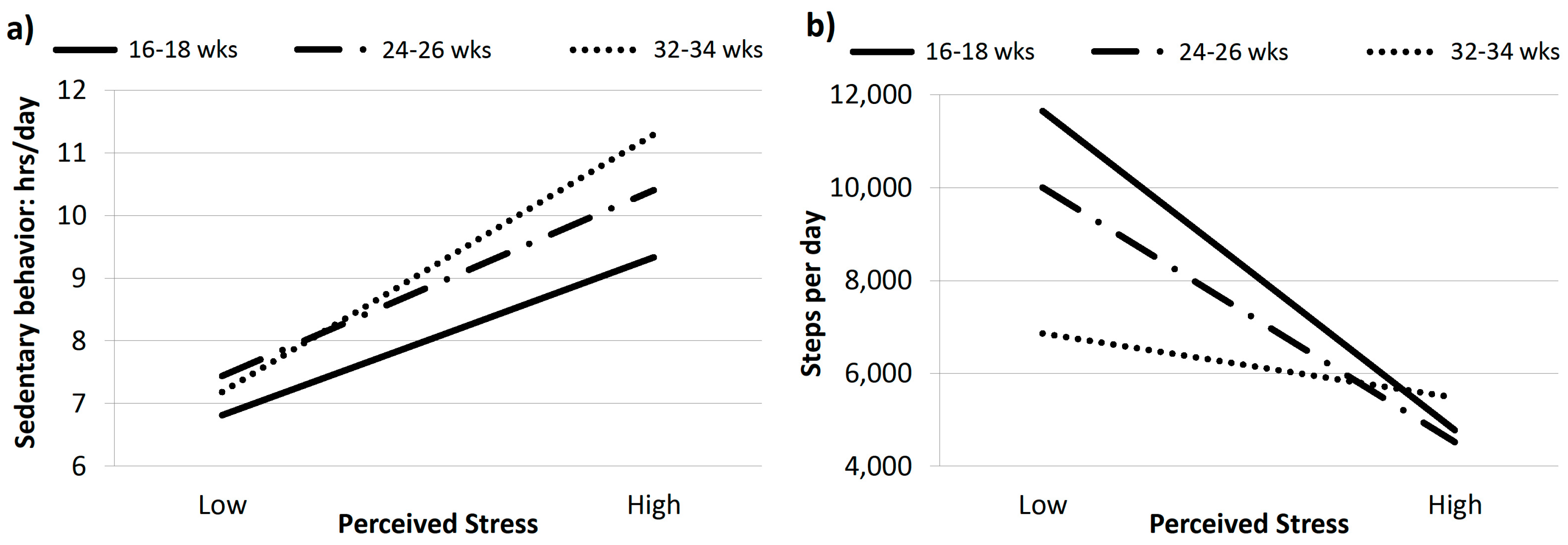
3.2. Relationships Between Perceived Stress and Sedentary Behavior
4. Discussion
4.1. Sedentary Behavior
4.2. Physical Activity
4.3. Strengths, Limitations, and Future Directions
5. Conclusions
Data Access Statement
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- Caspersen, C.J.; Powell, K.E.; Christenson, G.M. Physical activity, exercise, and physical fitness: Definitions and distinctions for health-related research. Public Health Rep. 1985, 100, 126–131. [Google Scholar] [PubMed]
- Entin, P.L.; Munhall, K.M. Recommendations regarding exercise during pregnancy made by private/small group practice obstetricians in the USA. J. Sports Sci. Med. 2006, 5, 449–458. [Google Scholar] [PubMed]
- Evenson, K.R.; Barakat, R.; Brown, W.J.; Dargent-Molina, P.; Haruna, M.; Mikkelsen, E.M.; Mottola, M.F.; Owe, K.M.; Rousham, E.K.; Yeo, S. Guidelines for physical activity during pregnancy: Comparisons from around the world. Am. J. Lifestyle Med. 2014, 8, 102–121. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Mottola, M.F.; Davenport, M.H.; Ruchat, S.M.; Davies, G.A.; Poitras, V.J.; Gray, C.E.; Jaramillo Garcia, A.; Barrowman, N.; Adamo, K.B.; Duggan, M.; et al. 2019 Canadian guideline for physical activity throughout pregnancy. Br. J. Sports Med. 2018, 52, 1339–1346. [Google Scholar] [CrossRef] [Green Version]
- American College of Obstetricians and Gynecologists (ACOG). Physical Activity and Exercise during Pregnancy and the Postpartum Period. Obstet. Gynecol. 2015, 126, e135–e142. [Google Scholar] [CrossRef]
- Tremblay, M.S.; Aubert, S.; Barnes, J.D.; Saunders, T.J.; Carson, V.; Latimer-Cheung, A.E.; Chastin, S.F.; Altenburg, T.M.; Chinapaw, M.J. Sedentary behavior research network (SBRN)—Terminology consensus project process and outcome. Int. J. Behav. Nutr. Phys. Act. 2017, 14, 75. [Google Scholar] [CrossRef] [Green Version]
- Evenson, K.R.; Wen, F. Prevalence and correlates of objectively measured physical activity and sedentary behavior among US pregnant women. Prev. Med. 2011, 53, 39–43. [Google Scholar] [CrossRef]
- Di Fabio, D.R.; Blomme, C.K.; Smith, K.M.; Welk, G.J.; Campbell, C.G. Adherence to physical activity guidelines in mid-pregnancy does not reduce sedentary time: An observational study. Int. J. Behav. Nutr. Phys. Act. 2015, 12, 27. [Google Scholar] [CrossRef] [Green Version]
- Fazzi, C.; Saunders, D.H.; Linton, K.; Norman, J.E.; Reynolds, R.M. Sedentary behaviours during pregnancy: A systematic review. Int. J. Behav. Nutr. Phys. Act. 2017, 14, 32. [Google Scholar] [CrossRef] [Green Version]
- Mikkonen, J.; Raphael, D. Social Determinants of Health: The Canadian Facts; York University: Toronto, ON, Canada, 2010; Available online: https://www.mooddisorders.ca/sites/mooddisorders.ca/files/downloads/the_canadian_facts.pdf (accessed on 6 November 2019).
- World Health Organization (WHO). Social Determinants of Health: The Solid Facts; WHO: Geneva, Switzerland, 2003; Available online: http://www.euro.who.int/__data/assets/pdf_file/0005/98438/e81384.pdf (accessed on 6 November 2019).
- Avison, W.R.; Ali, J.; Walters, D. Family structure, stress, and psychological distress: A demonstration of the impact of differential exposure. J. Health Soc. Behav. 2007, 48, 301–317. [Google Scholar] [CrossRef] [PubMed]
- Drapeau, A.; Marchand, A.; Beaulieu-Prévost, D. Epidemiology of Psychological Distress. In Mental Illnesses: Understanding, Prediction and Control; L’Abate, L., Ed.; InTech: London, UK, 2012. [Google Scholar]
- Stetson, B.A.; Rahn, J.M.; Dubbert, P.M.; Wilner, B.I.; Mercury, M.G. Prospective evaluation of the effects of stress on exercise adherence in community-residing women. Health Psychol. 1997, 16, 515–520. [Google Scholar] [CrossRef]
- Laugero, K.D.; Falcon, L.M.; Tucker, K.L. Relationship between perceived stress and dietary and activity patterns in older adults participating in the Boston Puerto Rican Health Study. Appetite 2011, 56, 194–204. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- St-Pierre, M.; Sinclair, I.; Elgbeili, G.; Bernard, P.; Dancause, K.N. Relationships between psychological distress and health behaviors among Canadian adults: Differences based on gender, income, education, immigrant status, and ethnicity. SSM Popul. Health 2019, 7, 100385. [Google Scholar] [CrossRef] [PubMed]
- Lobel, M.; Cannella, D.L.; Graham, J.E.; DeVincent, C.; Schneider, J.; Meyer, B.A. Pregnancy-specific stress, prenatal health behaviors, and birth outcomes. Health Psychol. 2008, 27, 604–615. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Rodriguez, A.; Bohlin, G.; Lindmark, G. Psychosocial predictors of smoking and exercise during pregnancy. J. Reprod. Infant Psychol. 2000, 18, 203–223. [Google Scholar] [CrossRef]
- Cohen, S.; Kamarck, T.; Mermelstein, R. A global measure of perceived stress. J. Health Soc. Behav. 1983, 24, 385–396. [Google Scholar] [CrossRef]
- Statistics Canada. Canadian Community Health Survey—Annual Component (CCHS). Available online: http://www23.statcan.gc.ca/imdb/p2SV.pl?Function=getSurvey&SDDS=3226 (accessed on 6 November 2019).
- Kessler, R.C.; Andrews, G.; Colpe, L.J.; Hiripi, E.; Mroczek, D.K.; Normand, S.L.; Walters, E.E.; Zaslavsky, A.M. Short screening scales to monitor population prevalences and trends in non-specific psychological distress. Psychol. Med. 2002, 32, 959–976. [Google Scholar] [CrossRef]
- Andrews, G.; Slade, T. Interpreting scores on the Kessler Psychological Distress Scale (K10). Aust. N. Z. J. Public Health 2001, 25, 494–497. [Google Scholar] [CrossRef]
- Australian Bureau of Statistics (ABS). A Guide to the K10 Symptom Scale. Available online: https://www.abs.gov.au/ausstats/[email protected]/lookup/4817.0.55.001Chapter92007-08 (accessed on 6 November 2019).
- Oviedo-Caro, M.A.; Bueno-Antequera, J.; Munguia-Izquierdo, D. Measuring sedentary behavior during pregnancy: Comparison between self-reported and objective measures. Matern. Child Health J. 2018, 22, 968–977. [Google Scholar] [CrossRef]
- Hawkins, M.; Kim, Y.; Gabriel, K.P.; Rockette-Wagner, B.J.; Chasan-Taber, L. Sedentary behavior patterns in non-pregnant and pregnant women. Prev. Med. Rep. 2017, 6, 97–103. [Google Scholar] [CrossRef]
- Badon, S.E.; Littman, A.J.; Chan, K.C.G.; Williams, M.A.; Enquobahrie, D.A. Maternal sedentary behavior during pre-pregnancy and early pregnancy and mean offspring birth size: A cohort study. BMC Pregnancy Childbirth 2018, 18, 267. [Google Scholar] [CrossRef] [PubMed]
- Asztalos, M.; Cardon, G.; De Bourdeaudhuij, I.; De Cocker, K. Cross-Sectional Associations Between Sitting Time and Several Aspects of Mental Health in Belgian Adults. J. Phys. Act. Health 2015, 12, 1112–1118. [Google Scholar] [CrossRef] [PubMed]
- Vasquez, E.; Strizich, G.; Gallo, L.; Marshall, S.J.; Merchant, G.C.; Murillo, R.; Penedo, F.J.; Salazar, C.; Sotres-Alvarez, D.; Shaw, B.A.; et al. The role of stress in understanding differences in sedentary behavior in Hispanic/Latino adults: Results from the Hispanic Community Health Study/Study of Latinos Sociocultural Ancillary Study. J. Phys. Act. Health 2016, 13, 310–317. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Mouchacca, J.; Abbott, G.R.; Ball, K. Associations between psychological stress, eating, physical activity, sedentary behaviours and body weight among women: A longitudinal study. BMC Public Health 2013, 13, 828. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Takahasi, E.H.; Alves, M.T.; Alves, G.S.; Silva, A.A.; Batista, R.F.; Simoes, V.M.; Del-Ben, C.M.; Barbieri, M.A. Mental health and physical inactivity during pregnancy: A cross-sectional study nested in the BRISA cohort study. Cad. Saude Publica 2013, 29, 1583–1594. [Google Scholar] [CrossRef] [PubMed]
- Berntsen, S.; Richardsen, K.R.; Morkrid, K.; Sletner, L.; Birkeland, K.I.; Jenum, A.K. Objectively recorded physical activity in early pregnancy: A multiethnic population-based study. Scand. J. Med. Sci. Sports 2014, 24, 594–601. [Google Scholar] [CrossRef] [Green Version]
- Baena-Garcia, L.; Ocon-Hernandez, O.; Acosta-Manzano, P.; Coll-Risco, I.; Borges-Cosic, M.; Romero-Gallardo, L.; de la Flor-Alemany, M.; Aparicio, V.A. Association of sedentary time and physical activity during pregnancy with maternal and neonatal birth outcomes. The GESTAFIT Project. Scand. J. Med. Sci. Sports 2019, 29, 407–414. [Google Scholar] [CrossRef]
- Abbasi, M.; van den Akker, O. A systematic review of changesin women’s physical activity before and during pregnancy and the postnatal period. J. Reprod. Infant Psychol. 2015, 33, 325–358. [Google Scholar] [CrossRef]
- Derbyshire, E.; Davies, G.J.; Costarelli, V.; Dettmar, P.W. Habitual patterns of physical activity during pregnancy and postnatally. Br. J. Midwifery 2008, 16, 20–24. [Google Scholar] [CrossRef]
- Statistics Canada. Canadian Community Health Survey (CCHS) Derived Variable (DV) Specifications. 2013. Available online: https://library.queensu.ca/madgic/qrdc/metadata/cchs/2012/2012FS1/CCHS_FS1_Derived_Variables.pdf (accessed on 6 November 2019).
- Ng, D.M.; Jeffery, R.W. Relationships between perceived stress and health behaviors in a sample of working adults. Health Psychol. 2003, 22, 638–642. [Google Scholar] [CrossRef]
- Barnett, J.; Aguilar, S.; Brittner, M.; Bonuck, K. Recruiting and retaining low-income, multi-ethnic women into randomized controlled trials: Successful strategies and staffing. Contemp. Clin. Trials 2012, 33, 925–932. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hallgren, M.; Owen, N.; Stubbs, B.; Zeebari, Z.; Vancampfort, D.; Schuch, F.; Bellocco, R.; Dunstan, D.; Trolle Lagerros, Y. Passive and mentally-active sedentary behaviors and incident major depressive disorder: A 13-year cohort study. J. Affect. Disord. 2018, 241, 579–585. [Google Scholar] [CrossRef] [PubMed]
- Gaillard, R.; Wright, J.; Jaddoe, V.W.V. Lifestyle intervention strategies in early life to improve pregnancy outcomes and long-term health of offspring: A narrative review. J. Dev. Orig. Health Dis. 2019, 10, 314–321. [Google Scholar] [CrossRef] [PubMed] [Green Version]



{kind=link}
{kind=link}
| Variable | Mean/Frequency | Range |
|---|---|---|
| Age | 31.1 (5.9) | 19–45 |
| Number of children | 0.9 (1.1) | 0–5 |
| Household Income, n (%) | ||
| <$20,000 | 20 (28.6) | |
| $20,000–50,000 | 35 (50.0) | |
| >$50,000 | 15 (21.4) | |
| Education, n (%) | ||
| Secondary | 21 (30.0) | |
| College | 16 (32.9) | |
| University | 33 (47.1) | |
| Immigrant, n (%) | 46 (65.7) | |
| Visible minority, n (%) | 48 (68.6) | |
| Perceived Stress | ||
| Evaluation #1 | 24.4 (7.0) | 7–44 |
| Evaluation #2 | 22.2 (6.7) | 6–37 |
| Evaluation #3 | 22.0 (7.7) | 5–42 |
| Sedentarity (sitting time, h/day) | ||
| Evaluation #1 | 8.0 (1.9) | 3.8–13.7 |
| Evaluation #2 | 8.7 (1.8) | 5.7–13.4 |
| Evaluation #3 | 8.9 (2.1) | 4.3–14.5 |
| Physical activity (steps/day) | ||
| Evaluation #1 | 7878 (4381) | 1464–26,672 |
| Evaluation #2 | 7644 (3566) | 1948–19,842 |
| Evaluation #3 | 6273 (3136) | 593–15,762 |
| Variable | Sedentary Behavior | Physical Activity | ||||
|---|---|---|---|---|---|---|
| β | p-Value | η2 | β | p-Value | η2 | |
| Evaluation #1 (16–18 weeks pregnancy) | ||||||
| Age (years) | −0.04 | 0.358 | 0.01 | 62.65 | 0.580 | <0.01 |
| No. children | 0.24 | 0.344 | 0.01 | 317.86 | 0.597 | <0.01 |
| Education | 0.23 | 0.045 | 0.06 | −446.81 | 0.101 | 0.04 |
| Household income | −0.39 | 0.256 | 0.02 | 232.22 | 0.779 | <0.01 |
| Immigration status | −1.00 | 0.126 | 0.04 | 417.52 | 0.790 | <0.01 |
| Visible minority status | 0.50 | 0.426 | 0.01 | −386.47 | 0.797 | <0.01 |
| Perceived stress | 0.10 | 0.005 | 0.12 | −227.98 | 0.007 | 0.11 |
| Evaluation #2 (24–26 weeks pregnancy) | ||||||
| Age (years) | 0.00 | 0.955 | <0.01 | 43.55 | 0.623 | <0.01 |
| No. children | 0.19 | 0.420 | 0.01 | 823.12 | 0.087 | 0.05 |
| Education | 0.05 | 0.606 | <0.01 | −350.04 | 0.089 | 0.05 |
| Household income | −0.40 | 0.227 | 0.02 | 132.00 | 0.840 | <0.01 |
| Immigration status | 0.03 | 0.964 | <0.01 | −268.16 | 0.823 | <0.01 |
| Visible minority status | 0.74 | 0.219 | 0.02 | 958.38 | 0.419 | 0.01 |
| Perceived stress | 0.07 | 0.024 | 0.08 | −139.15 | 0.028 | 0.08 |
| Evaluation #3 (32–34 weeks pregnancy) | ||||||
| Age (years) | 0.00 | 0.972 | <0.01 | 6.87 | 0.933 | <0.01 |
| No. children | 0.02 | 0.936 | <0.01 | 439.23 | 0.318 | 0.02 |
| Education | 0.00 | 0.975 | <0.01 | 231.63 | 0.222 | 0.02 |
| Household income | −0.48 | 0.218 | 0.02 | 709.02 | 0.250 | 0.02 |
| Immigration status | −0.30 | 0.676 | <0.01 | −278.83 | 0.807 | <0.01 |
| Visible minority status | 0.31 | 0.661 | <0.01 | −1226.89 | 0.268 | 0.02 |
| Perceived stress | 0.11 | 0.001 | 0.16 | −49.47 | 0.341 | 0.01 |
| Variable | Mean/Frequency |
|---|---|
| Age (Years) | 30.2 (5.7) |
| Number of people <18 years old living in the household | 0.8 (0.9) |
| Household Income, % | |
| <$20,000 | 11.1 |
| $20,000–50,000 | 42.5 |
| >$50,000 | 46.4 |
| Education, % | |
| Secondary | 15.7 |
| College | 42.3 |
| University | 42.0 |
| Immigrant, % | 35.0 |
| Visible minority, % | 34.3 |
| Psychological Distress | 4.0 (3.4) |
| Sedentarity (leisure activities, h/day) | 3.3 (2.0) |
| Physical activity (daily energy expenditure, transportation & leisure activities, kcal/kg/day) | 1.6 (1.6) |
| Variable | Sedentary Behavior | Physical Activity | ||||
|---|---|---|---|---|---|---|
| β | p-Value | η2 | β | p-Value | η2 | |
| Age (years) | 0.00 | 0.905 | 0.00 | 0.00 | 0.908 | <0.00 |
| No. children in household | −0.30 | 0.058 | 0.02 | 0.03 | 0.730 | <0.00 |
| Education | −0.18 | 0.002 | 0.03 | 0.08 | 0.055 | 0.01 |
| Household income | 0.03 | 0.306 | <0.01 | 0.00 | 0.994 | <0.00 |
| Immigration status | −0.25 | 0.252 | <0.01 | 0.37 | 0.045 | 0.01 |
| Visible minority status | 0.01 | 0.582 | <0.01 | 0.00 | 0.899 | <0.00 |
| Perceived stress | 0.09 | 0.001 | 0.02 | 0.01 | 0.580 | <0.00 |
© 2019 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Sinclair, I.; St-Pierre, M.; Elgbeili, G.; Bernard, P.; Vaillancourt, C.; Gagnon, S.; Dancause, K.N. Psychosocial Stress, Sedentary Behavior, and Physical Activity during Pregnancy among Canadian Women: Relationships in a Diverse Cohort and a Nationwide Sample. Int. J. Environ. Res. Public Health 2019, 16, 5150. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph16245150
Sinclair I, St-Pierre M, Elgbeili G, Bernard P, Vaillancourt C, Gagnon S, Dancause KN. Psychosocial Stress, Sedentary Behavior, and Physical Activity during Pregnancy among Canadian Women: Relationships in a Diverse Cohort and a Nationwide Sample. International Journal of Environmental Research and Public Health. 2019; 16(24):5150. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph16245150
Chicago/Turabian StyleSinclair, Isabelle, Myriane St-Pierre, Guillaume Elgbeili, Paquito Bernard, Cathy Vaillancourt, Sonia Gagnon, and Kelsey Needham Dancause. 2019. "Psychosocial Stress, Sedentary Behavior, and Physical Activity during Pregnancy among Canadian Women: Relationships in a Diverse Cohort and a Nationwide Sample" International Journal of Environmental Research and Public Health 16, no. 24: 5150. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph16245150