Effects of an Educational Intervention on Angolan Adolescents’ Knowledge of Human Reproduction: A Quasi-Experimental Study

 ,
,  and
and
Abstract
:1. Introduction
2. Materials and Methods
3. Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
Appendix A
Appendix B
Appendix C
 |  |
| 1. Pubic hair | 1. Ovary |
| 2. Labia major | 2. Fallopian tube |
| 3. Vagina | 3. Uterus |
| 4. Anus | 4. Vagina |
 |  |
| 1. Pubic hair | 1. Testicles |
| 2. Penile body | 2. Prostate |
| 3. Scrotum | 3. Penis |
| 4. Glans covered by foreskin | |
| (P2AF) | (P2AM) |
| The feminine reproductive cell is denominated: | The reproductive masculine cell is denominated: |
| 1. Follicular cell | 1. Spermatogonia |
| 2. Ovule | 2. Sertoli’s cell |
| 3. Germinative cell | 3. Germinal cell |
| 4. Ovogonia | 4. Spermatozoid |
| (P2BF) This cell is produced in the: | (P2BM) This cell is produced in the: |
| 1. Uterus | 1. Testicle |
| 2. Fallopian tubes | 2. Vas deferens (sperm duct) |
| 3. Ovary | 3. Prostate gland |
| 4. Epididymis | |
| (P2CF) The normal formation process of the feminine reproductive cells is: | (P2CM) The normal masculine cells process of formation is: |
| 1. Continuous | 1. Continuous |
| 2. Cyclic | 2. Cyclic |
| 3. Irregular | 3. Irregular |
| 4. Alternative | 4. Alternative |
| (P2DF) The reproductive feminine cell is liberated: | (P2DM) The masculine reproductive cell is liberated: |
| 1. Every 7 days | 1. Every 7 days |
| 2. Every 14 days | 2. Every 14 days |
| 3. Every 28 days | 3. Every 28 days |
| 4. In a permanent way | 4. In a permanent way |
References
- García, A.I.; Ángel, Á.P.; Herrera, L.F.; Morales, M.M.P. And What Do You Know about “That”? Youth Sexual Education Handbook; Centro de Ediciones de la Diputación de Málaga: Málaga, Spain, 2011. [Google Scholar]
- Reis, B.; Lopes, D.; Franco, P.; Vilela, R. Law, Religion, Right to Live and Abortion; Center of R&D about Law and Society: Lisbon, Portugal, 2015. [Google Scholar]
- United Nations Population Fund-Information and External Relations Division (UNFPA). Early Maternity: Facing the Challenge of Teenage Pregnancy. World Population Situation, 1st ed.; Kollodge, R., Ed.; Photographics, Inc.: New York, NY, USA, 2013. [Google Scholar]
- National Statistical Institute (INE). General Census of Population and Housing: Definitive Results; INE: Luanda, Angola, 2016.
- Mwale, M.; Muula, A.S. Systematic review: A review of adolescent behavior change interventions [BCI] and their effectiveness in HIV and AIDS prevention in sub-Saharan Africa. BMC Public Health 2017, 17, 1–9. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Michielsen, K.; Temmerman, M.; Van Rossem, R. Limited effectiveness of HIV prevention for young people in sub-Saharan Africa: Studying the role of intervention and evaluation. Facts Views Vis. ObGyn 2013, 5, 196–208. [Google Scholar] [PubMed]
- Guimarães Nebenzahl, H.; Lopes, A.; Castro, R.; Pereira, F. Prevalence of human immunodeficiency virus, hepatitis C virus, hepatitis B virus and syphilis among individuals attending anonymous testing for HIV in Luanda, Angola. S. Afr. Med. J. 2013, 103, 186–188. [Google Scholar]
- Masha, S.C.; Cools, P.; Sanders, E.J.; Vaneechoutte, M.; Crucitti, T. Trichomonas vaginalis and HIV infection acquisition: A systematic review and meta-analysis. Sex. Transm. Infect. 2019, 95, 36–42. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Augusto, G.F. Use of services for prevention of mother-to-child transmission in Angola: A retrospective analysis. J. Public Health 2016, 38, 371–377. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- De Almeida, N.P.S. Youth Sexual Education and Prevention of Unwanted Pregnancy, 1st ed.; Education, M., Ed.; Mayamba Education: Luanda, Angola, 2015. [Google Scholar]
- Unicef OGE Education 2016, 1st ed.; ADRA: Luanda, Angola, 2016.
- Ministry of Education. 2015 National Exam of Education for All: Angola, 1st ed.; Republic of Angola, Ed.; Ministry of Education: Luanda, Angola, 2015.
- Capurchande, R.; Coene, G.; Schockaert, I.; Macia, M.; Meulemans, H. “It is challenging... oh, nobody likes it!”: A qualitative study exploring Mozambican adolescents and young adults’ experiences with contraception. BMC Womens Health 2016, 16, 1–17. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Emelumadu, O.F.; Ezeama, N.N.; Ifeadike, C.O.; Ubajaka, C.F.; Adogu, P.O.U.; Umeh, U.; Nwamoh, U.N.; Ukegbu, A.U.; Onyeonoro, U.U. Parents’ perceptions of timing of initiation of sexuality discussion with adolescents in anambra state, south eastern nigeria. J. Pediatr. Adolesc. Gynecol. 2014, 27, 294–300. [Google Scholar] [CrossRef] [PubMed]
- Kebede, A.; Molla, B.; Gerensea, H. Assessment of risky sexual behavior and practice among Aksum University students, Shire Campus, Shire Town, Tigray, Ethiopia, 2017. BMC Res. Notes 2018, 11, 7–12. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- De Almeida, N.; Teixeira, A.; Capoco Sachiteque, A.; Molina, J.R.; dos Prazeres Tavares, H.; Ramalho, C. Characterisation of induced abortion and consequences to women’s health at Hospital Central do Huambo -Angola. J. Obstet. Gynaecol. 2019. [Google Scholar] [CrossRef] [PubMed]
- Gebresllasie, F.; Tsadik, M.; Berhane, E. Potential predictors of risk sexual behavior among private college students in Mekelle City, North Ethiopia. Pan Afr. Med. J. 2017, 28, 1–11. [Google Scholar] [CrossRef] [PubMed]
- Prata, N.; Vahidnia, F.; Fraser, A. Gender and relationship differences in condom use among 15–24-year-olds in Angola. Int. Fam. Plan. Perspect. 2005, 31, 192–199. [Google Scholar] [CrossRef] [PubMed]
- Madlala, S.T.; Sibiya, M.N.; Ngxongo, T.S.P. Perceptions of young men at the Free State School of Nursing with regards to teenage pregnancy. Afr. J. Prim. Health Care Fam. Med. 2018, 10, 1–7. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Woodhams, E.; Sipsma, H.; Hill, B.J.; Gilliam, M. Perceived responsibility for pregnancy and sexually transmitted infection prevention among young African American men: An exploratory focus group study. Sex. Reprod. Healthc. 2018, 16, 86–91. [Google Scholar] [CrossRef] [PubMed]
- Velonjara, J.; Crouthamel, B.; O’Malley, G.; Wiggins, M.; Matemo, D.; John-Stewart, G.; Unger, J.A.; Kinuthia, J.; Drake, A.L. Motherhood increases support for family planning among Kenyan adolescents. Sex. Reprod. Healthc. 2018, 16, 124–131. [Google Scholar] [CrossRef] [PubMed]
- Koffi, T.B.; Weidert, K.; Bitasse, E.O.; Mensah, M.A.E.; Emina, J.; Mensah, S.; Bongiovanni, A.; Prata, N. Engaging Men in Family Planning: Perspectives From Married Men in Lomé, Togo. Glob. Health Sci. Pract. 2018, 6, 316–327. [Google Scholar] [CrossRef] [PubMed]
- Cardoso, L.C. Birth Control. A View from Sub-Saharan Africa; Faculty of Theology, Department of Moral and Pastoral Theology: Madrid, Spain, 2015. [Google Scholar]
- Zuilkowski, S.S.; Jukes, M.C.H. The impact of education on sexual behavior in sub-Saharan Africa: A review of the evidence. AIDS Care-Psychol. Socio-Med. Asp. AIDS/HIV 2012, 24, 562–576. [Google Scholar] [CrossRef] [PubMed]
- Tchivandja, Q. Causes of Material Deaths for Hypertensive Disease of Pregnancy in Angola 2001–2005 and in the Special Material of Children of Kiaban Kilaean Luanda, from January to December 2007. Ph.D. Thesis, Università degli Studi di Trieste, Trieste, Italy, 2007. [Google Scholar]
- Dos Tavares, H.P. Obstetric, Socio-Demographic and Psychosocial Aspects of Adolescent Mothers Assisted at the Maternity of Central Hospital of Huambo, Province of Huambo-Angola/Hamilton dos Prazeres Tavares. Master’s Thesis, University Estácio de Sá, Rio de Janeiro, Brazil, 2011. [Google Scholar]
- Small, E.; Nikolova, S.P.; Narendorf, S.C. Synthesizing gender based HIV interventions in sub-sahara Africa: A systematic review of the evidence. AIDS Behav. 2013, 17, 2831–2844. [Google Scholar] [CrossRef] [PubMed]


{kind=link}
| Variables | EG n = 241 | CG n = 348 | p-Value |
|---|---|---|---|
| Gender, n (%) | n = 241 | n = 348 | <0.001 a,* |
| Males | 98 (29.3) | 236 (70.7) | |
| Females | 143 (56.1) | 112 (43.9) | |
| Age (years), Med [Q1;Q3] | n = 241 15 [14; 16] | n = 348 18 [17; 19] | <0.001 b,* |
| Marital status, n (%) | n = 230 | n = 337 | 0.086 a |
| Not married | 206 (42.0) | 285 (58.0) | |
| Married or marital# | 24 (31.6) | 52 (68.4) | |
| Father’s education, n (%) | n = 231 | n = 304 | <0.001 a,* |
| No schooling | 7 (41.2) | 10 (58.8) | |
| Primary education | 1 (11.1) | 8 (88.9) | |
| Secondary education | 17 (50.0) | 17 (50.0) | |
| Higher education | 20 (23.5) | 65 (76.5) | |
| University education | 85 (42.9) | 113 (57.1) | |
| Post-graduation | 101 (52.6) | 91 (47.4) | |
| Mother’s education, n (%) | n = 234 | n = 304 | 0.039 a,* |
| No schooling | 12 (44.4) | 15 (55.6) | |
| Primary education | 5 (22.7) | 17 (77.3) | |
| Secondary education | 17 (38.6) | 27 (61.4) | |
| Higher education | 35 (33.7) | 69 (66.3) | |
| University education | 101 (48.1) | 109 (51.9) | |
| Post-graduation | 64 (48.9) | 67 (51.1) | |
| Usually talks with parents about sexuality, n (%) | n = 221 | n = 320 | 0.008 a |
| No | 94 (35.2) | 173 (64.8) | |
| Yes | 127 (46.4) | 147 (53.6) | |
| Age of first sexual relation, females (years), Med [Q1; Q3] | n = 15 15 [14; 17] | n = 39 16 [16; 17] | 0.017 b,* |
| Previous pregnancy, females, n (%) | n = 137 | n = 104 | <0.001 a,* |
| No | 137 (60.1) | 91 (39.9) | |
| Yes | 0 (0.0) | 13 (100.0) | |
| Previous abortion, females, n (%) | n = 142 | n = 108 | 0.432 c |
| No | 142 (57.0) | 107 (43.0) | |
| Yes | 0 (0.0) | 1 (100.0) | |
| Age of first sexual relation, males (years), Med [Q1;Q3] | n = 65 13 [11.5; 14] | n = 187 14 [12; 15] | <0.001 b,* |
| Sexual experience, n (%) | |||
| Kisses | n = 189 | n = 307 | <0.001 a,* |
| No | 46 (25.1) | 137 (74.9) | |
| Yes | 143 (45.7) | 170 (54.3) | |
| Caressing | n = 190 | n = 307 | 0.945 a |
| No | 112 (38.4) | 180 (61.6) | |
| Yes | 78 (38.0) | 127 (62.0) | |
| Masturbation | n = 189 | n = 305 | 0.005 a,* |
| No | 166 (41.2) | 237 (58.8) | |
| Yes | 23 (25.3) | 68 (74.7) | |
| Sexual intercourse | n = 189 | n = 309 | <0.001 a,* |
| No | 134 (58.3) | 96 (41.7) | |
| Yes | 55 (20.5) | 213 (79.5) | |
| Age at first sexual intercourse (years), Med [Q1; Q3] | n = 72 14 [12; 14] | n = 216 15 [14; 16.75] | <0.001 b,* |
| Feels worried (bad) when engaging in sex, n (%) | n = 130 | n = 254 | 0.589a |
| No | 37 (25.5) | 108 (74.5) | |
| Yes | 35 (28.5) | 88 (71.5) |
| Before | After | EG (before vs. after) | CG (before vs. after) | ||||
|---|---|---|---|---|---|---|---|
| EG | CG | p-Value | EG | CG | p-Value | p-Value | p-Value |
| P1F-Correct identification of females sexual organs, Med [Q1;Q3]: | |||||||
| n = 241 4 [2.5; 5] | n = 348 4 [0; 5] | 0.566 a | n = 210 6 [5; 7] | n = 320 4 [3; 6] | <0.001 a,* | <0.001 b,* | <0.001 b,* |
| P1M-Correct identification of males sexual organs, Med [Q1;Q3]: | |||||||
| n = 241 2 [1; 4] | n = 348 3 [0; 5] | 0.066 a | n = 210 5 [4; 6] | n = 320 4 [2.25; 5] | <0.001 a,* | <0.001 b,* | <0.001 b,* |
| P2AF-Correct knowledge about denomination of the feminine reproductive cell, n (%) | |||||||
| n = 150 123 (82.0) | n = 192 168 (87.5) | 0.157 c | n = 201 186 (92.5) | n = 242 208 (86.0) | 0.028 c,* | <0.001 d,* | 1.000 d |
| P2AM-Correct knowledge about denomination of the masculine reproductive cell, n (%) n (%) | |||||||
| n = 154 127 (82.5) | n = 220 190 (86.4) | 0.157 c | n = 197 161 (81.7) | n = 247 208 (84.2) | 0.488 c | 1.000 d | 0.742 d |
| P2BF-Correct knowledge on the production site of feminine reproductive cells, n (%) | |||||||
| n = 149 64 (43.0) | n = 195 98 (50.3) | 0.179 c | n = 196 124 (63.3) | n = 235 128 (54.5) | 0.065 c | 0.001 d,* | 0.016 d,* |
| P2BM-Correct knowledge on the production site of masculine reproductive cells, n (%), n (%) | |||||||
| n = 114 92 (80.7) | n = 196 171 (87.2) | 0.121 c | n = 189 155 (82.0) | n = 232 193 (83.2) | 0.751 c | 0.523 d | 0.584 d |
| P2CF-Correct knowledge about the normal process of female reproductive cell formation, n (%) | |||||||
| n = 132 53 (40.2) | n = 162 92 (56.8) | 0.005 c,* | n = 194 94 (48.5) | n = 224 116 (51.8) | 0.497 c | 0.080 d | 0.280 d |
| P2CM-Correct knowledge about the normal process of male reproductive cell formation, n (%) | |||||||
| n = 121 66 (54.5) | n = 180 140 (77.8) | <0.001 c,* | n = 190 150 (78.9) | n = 224 170 (75.9) | 0.460 c | <0.001 d,* | 1.000 d |
| P2DF-Correct knowledge of the site of reproductive feminine cells release, n (%) | |||||||
| n = 110 38 (34.5) | n = 149 54 (36.2) | 0.778 c | n = 188 112 (59.6) | n = 207 44 (21.3) | <0.001 c,* | <0.001 d,* | 0.001 d,* |
| P2DM-Correct knowledge of the site of reproductive masculine cells release, n (%) | |||||||
| n = 109 69 (63.3) | n = 167 114 (68.3) | 0.394 c | n = 182 158 (86.8) | n = 218 158 (72.5) | <0.001 c,* | <0.001 d,* | 0.486 d |
| n = 109 69 (63.3) | n = 167 114 (68.3) | 0.394 c | n = 182 158 (86.8) | n = 218 158 (72.5) | <0.001 c,* | <0.001 d,* | 0.486 d |
| P3A-Answer correctly to the following statement “Menarche is the women’s first period” (True/False), n (%) | |||||||
| n = 159 151 (95.0) | n = 163 155 (95.1) | 0.959 c | n = 192 186 (96.9) | n = 219 197 (90.0) | 0.005 c,* | 0.581 d | 0.227 d |
| P3B-Answer correctly to the following statement “Menarche’s age is the same in all the women” (True/False), n (%) | |||||||
| n = 157 137 (87.3) | n = 168 147 (87.5) | 0.948 c | n = 187 161 (86.1) | n = 213 183 (85.9) | 0.959 c | 0.678 d | 0.581 d |
| P3C-Answer correctly to the following statement “After the beginning of the menarche the woman can already get pregnant” (True/False), n (%) | |||||||
| n = 163 146 (89.6) | n = 168 154 (91.7) | 0.513c | n = 189 175 (92.6) | n = 217 189 (87.1) | 0.070 c | 0.629 d | 0.057 d |
| P3D-Answer correctly to the following statement “After the menarche the woman is already capable of having children” (True/False), n (%) | |||||||
| n = 159 48 (30.2) | n = 166 76 (45.8) | 0.004 c,* | n = 192 110 (57.3) | n = 215 90 (41.9) | 0.002 c,* | <0.001 d,* | 0.542 d |
| P3E-Answer correctly to the following statement “Is normal that the first menstrual cycles are irregular” (True/False), n (%) | |||||||
| n = 158 142 (89.9) | n = 171 136 (79.5) | 0.010 c,* | n = 191 176 (92.1) | n = 217 178 (82.0) | 0.003 c,* | 0.481 d | 0.424 d |
| P4A-Correct knowledge of reproductive organs involved in women’s sexual cycle, n (%) | |||||||
| n = 151 46 (30.5) | n = 193 73 (37.8) | 0.154 c | n = 189 117 (61.9) | n = 252 88 (34.9) | <0.001 c,* | <0.001 d,* | 0.532 d |
| P4B-Correct knowledge about hormones involved in regulating the sexual cycle in women, n (%) | |||||||
| n = 85 12 (14.1) | n = 109 29 (26.6) | 0.035 c,* | n = 170 77 (45.3) | n = 153 16 (10.5) | <0.001 c,* | <0.001 d,* | 0.031 d,* |
| P4C-Correct knowledge about when you are most likely to become pregnant, n (%) | |||||||
| n = 155 17 (11.0) | n = 194 28 (14.4) | 0.337 c | n = 187 49 (26.2) | n = 246 41 (16.7) | 0.015 c,* | <0.001 d,* | 0.472 d |
| P4D-Correct knowledge about what risk they consider most important when having sex in adolescence, n (%) | |||||||
| n = 177 72 (40.7) | n = 260 132 (50.8) | 0.038 c,* | n = 199 120 (60.3) | n = 297 153 (51.5) | 0.054 c | <0.001 d,* | 0.918 d |
| P4EA-Answer correctly to the following statement “The ripe ovule in the woman’s gynecological apparatus stays during every menstrual cycle” (True/False), n (%) | |||||||
| n = 108 30 (27.8) | n = 146 81 (55.5) | <0.001 c,* | n = 170 85 (50.0) | n = 164 77 (47.0) | 0.577 c | <0.001 d,* | 0.216 d |
| P4EB-Answer correctly to the following statement “The spermatozoids can stay alive in the woman’s genital organs for 10 days” (True/False), n (%) | |||||||
| n = 120 44 (36.7) | n = 167 98 (58.7) | <0.001 c,* | n = 176 115 (65.3) | n = 187 108 (57.8) | 0.138 c | <0.001 d,* | 0.857 d |
| P4EC-Answer correctly to the following statement “The menstrual cycle is the interval of time that elapses between the first day of period and the first day of the following period” (True/False), n (%) | |||||||
| n = 99 57 (57.6) | n = 145 98 (67.6) | 0.111 c | n = 168 129 (76.8) | n = 162 93 (57.4) | <0.001 c,* | 0.002 d,* | 0.289 d |
| P4ED-Answer correctly to the following statement “A duration of a normal cycle can go from 21 to 35 days. Being like this, the woman can have regular or irregular cycles” (True/False), n (%) | |||||||
| n = 117 89 (76.1) | n = 152 107 (70.4) | 0.300 c | n = 176 142 (80.7) | n = 182 126 (69.2) | 0.013 c,* | 0.450 d | 0.450 d |
| P5A-Correct knowledge of the most characteristic sign of the masculine puberty, n (%) | |||||||
| n = 162 24 (14.8) | n = 234 35 (15.0) | 0.969 c | n = 200 106 (53.0) | n = 266 55 (20.7) | <0.001 c,* | <0.001 d,* | 0.050 d,* |
| P5B-Correct knowledge of the most visible characteristic sign of the feminine puberty, n (%) | |||||||
| n = 170 125 (73.5) | n = 232 145 (62.5) | 0.020 c,* | n = 202 160 (79.2) | n = 274 188 (68.6) | 0.010 c,* | 0.268 d | 0.034 d,* |
| P5C-Correct knowledge about human sexual maturation, n (%) | |||||||
| n = 132 13 (9.8) | n = 198 26 (13.1) | 0.365 c | n = 186 80 (43.0) | n = 236 28 (11.9) | <0.001 c,* | <0.001 d,* | 0.845 d |
| P5D-Correct knowledge about the basis of sexual relationship onset, n (%) | |||||||
| n = 172 72 (41.9) | n = 236 109 (46.2) | 0.385 c | n = 200 142 (71.0) | n = 277 116 (41.9) | <0.001 c,* | <0.001 d,* | 0.476 d |
| P6A-Correct knowledge about the existing contraceptive methods, n (%) | |||||||
| n = 159 98 (61.6) | n = 231 156 (67.5) | 0.230 c | n = 196 142 (72.4) | n = 276 185 (67.0) | 0.208 c | 0.105 d | 0.810 d |
| P6B-Correct knowledge about who should use contraceptive methods, n (%) | |||||||
| n = 160 92 (57.5) | n = 239 145 (60.7) | 0.527 c | n = 202 164 (81.2) | n = 280 179 (63.9) | <0.001 c,* | <0.001 d,* | 0.657 d |
| P6C-Knowledge about the contraceptive methods they had heard about, Med [Q1; Q3] | |||||||
| n = 241 1 [0; 3] | n = 348 1.5 [0; 4] | 0.013 a,* | n = 209 4 [3; 6] | n = 320 3 [1; 5] | <0.001 a,* | <0.001 b,* | <0.001 b,* |
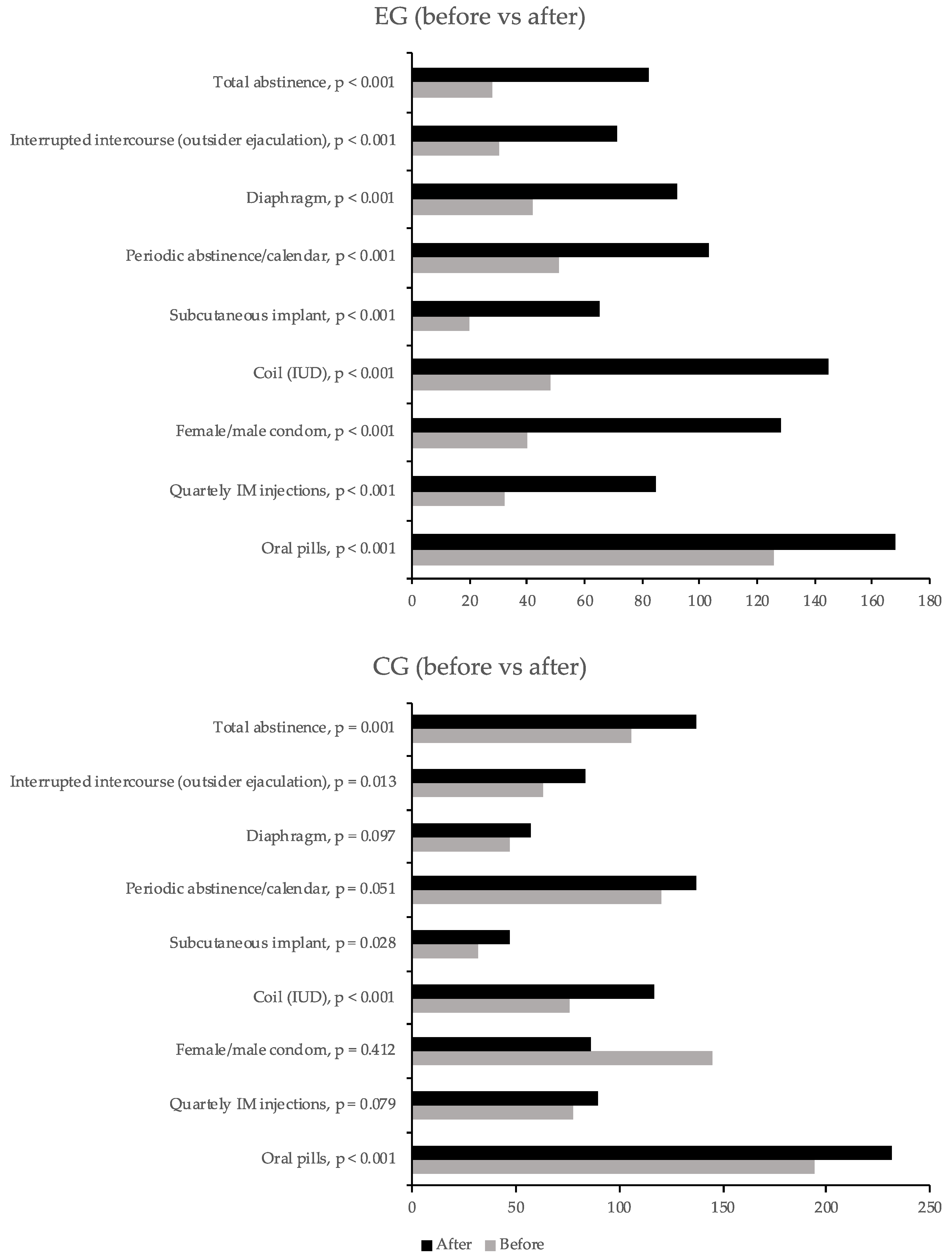
| Questions | Before | After | ||||
|---|---|---|---|---|---|---|
| EG | CG | p-Value | EG | CG | p-Value | |
| Oral pills, n (%) | n = 241 126 (52.3) | n = 347 194 (55.9) | 0.385 a | n = 209 168 (80.4) | n = 320 232 (72.5) | 0.039 a,* |
| Quarterly IM injections, n (%) | n = 241 32 (13.3) | n = 347 78 (22.5) | 0.005 a,* | n = 209 85 (40.7) | n = 320 90 (28.1) | 0.003 a,* |
| Female/Male condom, n (%) | n = 241 40 (57.5) | n = 239 145 (60.7) | 0.527 a | n = 209 128 (61.2) | n = 320 86 (26.9) | <0.001 a,* |
| Coil (IUD), n (%) | n = 241 48 (19.9) | n = 347 76 (21.9) | 0.562 a | n = 209 145 (69.4) | n = 320 117 (36.6) | <0.001a,* |
| Subcutaneous implant, n (%) | n = 241 20 (8.3) | n = 347 32 (9.2) | 0.698 a | n = 209 65 (31.1) | n = 320 47 (14.7) | <0.001 a,* |
| Periodic abstinence/calendar, n (%) | n = 241 51 (21.2) | n = 347 120 (34.6) | <0.001 a,* | n = 209 103 (49.3) | n = 320 137 (42.8) | 0.144 a |
| Diaphragm n (%) | n = 241 42 (17.4) | n = 347 47 (13.5) | 0.196 a | n = 209 92 (44.0) | n = 320 57 (17.8) | <0.001 a,* |
| Interrupted intercourse (outsider ejaculation), n (%) | n = 241 30 (12.4) | n = 347 63 (18.2) | 0.062 a | n = 209 71 (34.0) | n = 320 84 (26.3) | 0.056 a |
| Total abstinence n (%) | n = 241 28 (11.6) | n = 347 106 (30.5) | <0.001 a,* | n = 209 82 (39.2) | n = 318 137 (43.1) | 0.381 a |
© 2019 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Almeida, N.; Teixeira, A.; Garcia, J.; Martins, N.; Ramalho, C. Effects of an Educational Intervention on Angolan Adolescents’ Knowledge of Human Reproduction: A Quasi-Experimental Study. Int. J. Environ. Res. Public Health 2019, 16, 5155. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph16245155
Almeida N, Teixeira A, Garcia J, Martins N, Ramalho C. Effects of an Educational Intervention on Angolan Adolescents’ Knowledge of Human Reproduction: A Quasi-Experimental Study. International Journal of Environmental Research and Public Health. 2019; 16(24):5155. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph16245155
Chicago/Turabian StyleAlmeida, Natércia, Andreia Teixeira, José Garcia, Natália Martins, and Carla Ramalho. 2019. "Effects of an Educational Intervention on Angolan Adolescents’ Knowledge of Human Reproduction: A Quasi-Experimental Study" International Journal of Environmental Research and Public Health 16, no. 24: 5155. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph16245155