Health-Related Quality of Life of Medical Students in a Chinese University: A Cross-Sectional Study

 and
and
Abstract
:1. Introduction
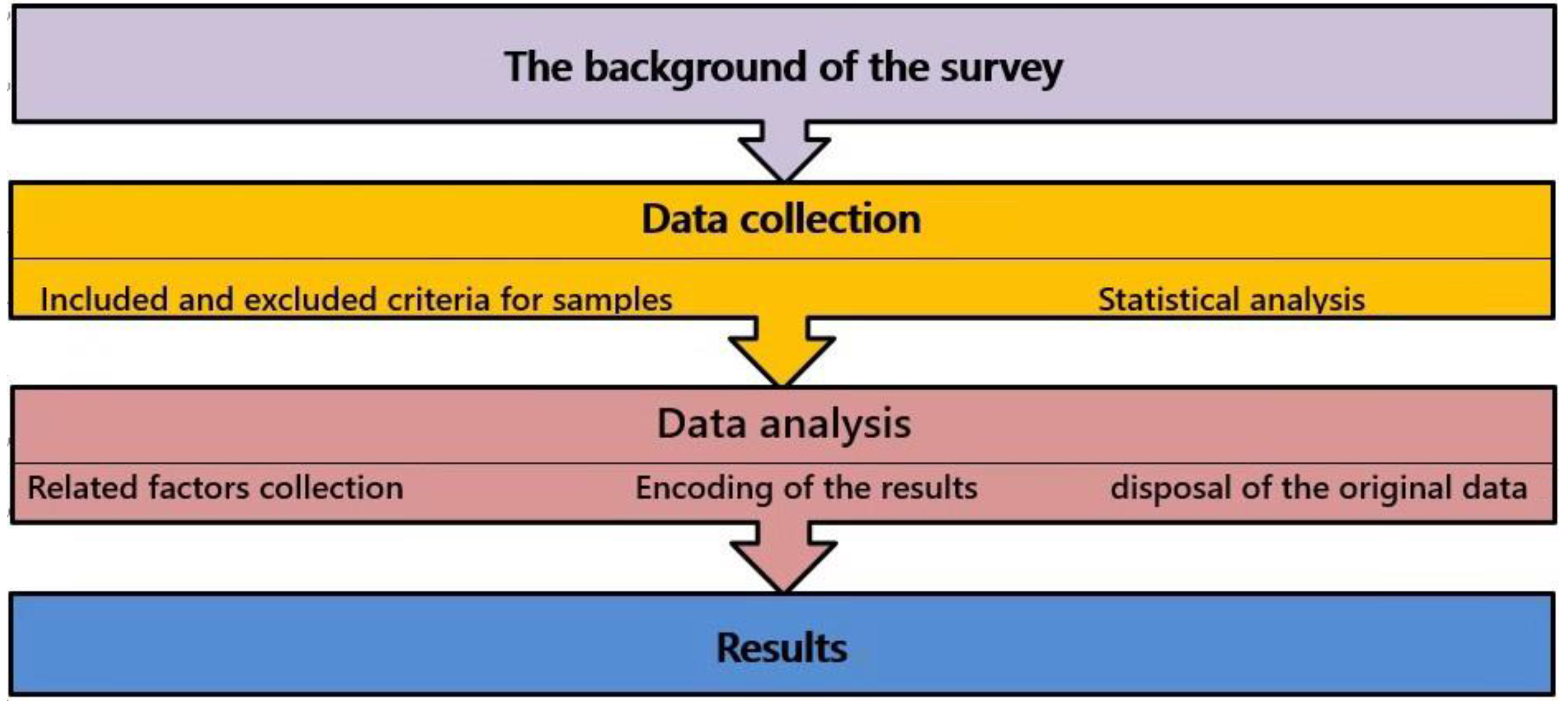
2. Materials and Methods
2.1. Sample
2.2. Measures and Procedures
2.3. Data Analysis
3. Results
4. Discussion
Strengths and Limitations of This Study
5. Conclusions
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- Wolf, T.M. Stress, coping and health: Enhancing well-being during medical school. Med. Educ. 1994, 28, 8–17. [Google Scholar] [CrossRef] [PubMed]
- Tempski, P.; Bellodi, P.L.; Paro, H.B.; Enns, S.C.; Martins, M.A.; Schraiber, L.B. What do medical students think about their quality of life? A qualitative study. BMC Med. Educ. 2012, 12, 106. [Google Scholar] [CrossRef] [PubMed]
- Paro, H.B.; Morales, N.M.; Silva, C.H.; Rezende, C.H.; Pinto, R.M.; Morales, R.R.; Mendonça, T.M.; Prado, M.M. Health-related quality of life of medical students. Med. Educ. 2010, 44, 227–235. [Google Scholar] [CrossRef] [PubMed]
- Lins, L.; Carvalho, F.M.; Menezes, M.S.; Porto-Silva, L.; Damasceno, H. Health-related quality of life of students from a private medical school in Brazil. Int. J. Med. Educ. 2015, 6, 149–154. [Google Scholar] [CrossRef] [PubMed]
- Whoqol Group. The World Health Organization Quality of Life assessment (WHOQOL): Position paper from the World Health Organization. Soc. Sci. Med. 1995, 41, 1403–1409. [Google Scholar] [CrossRef]
- WHOQOL Group. Study protocol for the World Health Organization project to develop a Quality of Life assessment instrument (WHOQOL). Qual. Life Res. 1993, 2, 153–159. [Google Scholar] [CrossRef]
- Strous, R.D.; Shoenfeld, N.; Lehman, A.; Wolf, A.; Snyder, L.; Barzilai, O. Medical students’ self-report of mental health conditions. Int. J. Med. Educ. 2012, 3, 1–5. [Google Scholar] [CrossRef] [Green Version]
- Ware, J.J.; Sherbourne, C.D. The MOS 36-item short-form health survey (SF-36). I. Conceptual framework and item selection. Med. Care 1992, 30, 473–483. [Google Scholar] [CrossRef]
- Zhang, Y.; Qu, B.; Lun, S.S.; Guo, Y.; Liu, J. The 36-item short form health survey: Reliability and validity in Chinese medical students. Int. J. Med. Sci. 2012, 9, 521–526. [Google Scholar] [CrossRef] [Green Version]
- Krageloh, C.U.; Henning, M.A.; Hawken, S.J.; Zhao, Y.; Shepherd, D.; Billington, R. Validation of the WHOQOL-BREF quality of life questionnaire for use with medical students. Educ. Health 2011, 24, 545. [Google Scholar]
- Huang, I.C.; Wu, A.W.; Frangakis, C. Do the SF-36 and WHOQOL-BREF measure the same constructs? Evidence from the Taiwan population. Qual. Life Res. 2006, 15, 15–24. [Google Scholar] [CrossRef] [PubMed]
- Li, N.; Liu, C.; Li, J.; Ren, X. The norms of SF-36 scale scores in urban and rural residents of Sichuan province. Hua Xi Yi Ke Da Xue Xue Bao 2001, 32, 43–47. (In Chinese) [Google Scholar] [PubMed]
- Wang, R.; Wu, C.; Zhao, Y.; Yan, X.; Ma, X.; Wu, M.; Liu, W.; Gu, Z.; Zhao, J.; He, J. Health related quality of life measured by SF-36: A population-based study in Shanghai, China. BMC Public Health 2008, 8, 292. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Li, L.; Wang, H.M.; Shen, Y. Chinese SF-36 health survey: Translation, cultural adaptation, validation, and normalisation. J. Epidemiol. Community Health 2003, 57, 259–263. [Google Scholar] [CrossRef]
- White, M.K.; Maher, S.M.; Rizio, A.A.; Bjorner, J.B. A meta-analytic review of measurement equivalence study findings of the SF-36® and SF-12® Health Surveys across electronic modes compared to paper administration. Qual. Life Res. 2018, 27, 1757–1767. [Google Scholar] [CrossRef]
- Fleiss, J.L. Design and Analysis of Clinical Experiments; John Wiley & Sons: Hoboken, NJ, USA, 2011. [Google Scholar]
- Ren, X.S.; Amick, B.R.; Zhou, L.; Gandek, B. Translation and psychometric evaluation of a Chinese version of the SF-36 Health Survey in the United States. J. Clin. Epidemiol. 1998, 51, 1129–1138. [Google Scholar] [CrossRef]
- Tseng, H.M.; Lu, J.F.; Gandek, B. Cultural issues in using the SF-36 Health Survey in Asia: Results from Taiwan. Health Qual. Life Outcomes 2003, 1, 72. [Google Scholar] [CrossRef] [Green Version]
- Lam, C.L.; Lauder, I.J.; Lam, T.P.; Gandek, B. Population based norming of the Chinese (HK) version of the SF-36 health survey. Hong Kong Pract. 1999, 21, 460–470. [Google Scholar]
- Rao, Y.; Xu, X.; Liu, D.; Reis, C.; Newman, I.; Qin, L.; Sharma, M.; Shen, J.; Zhao, Y. Health-related quality of life in patients with arthritis: A cross-sectional survey among middle-aged adults in Chongqing, China. Int. J. Environ. Res. Public Health 2018, 15, 768. [Google Scholar] [CrossRef] [Green Version]
- Zhang, Y.; Zhou, F.; Sun, Y. Assessment of health-related quality of life using the SF-36 in Chinese cervical spondylotic myelopathy patients after surgery and its consistency with neurological function assessment: A cohort study. Health Qual. Life Outcomes 2015, 13, 39. [Google Scholar] [CrossRef] [Green Version]
- Zhong, X.; Liu, Y.; Pu, J.; Tian, L.; Gui, S.; Song, X.; Xu, S.; Zhou, X.; Wang, H.; Zhou, W.; et al. Depressive symptoms and quality of life among Chinese medical postgraduates: A national cross-sectional study. Psychol. Health Med. 2019, 24, 1015–1027. [Google Scholar] [CrossRef] [PubMed]
- Domantay, J.A.A. Health-related quality of life of future physicians at a medical school in the Philippines. SAGE Open 2014, 4, 2000136751. [Google Scholar] [CrossRef] [Green Version]
- Dyrbye, L.N.; Thomas, M.R.; Power, D.V.; Durning, S.; Moutier, C.; Massie, F.S., Jr.; Harper, W.; Eacker, A.; Szydlo, D.W.; Sloan, J.A.; et al. Burnout and serious thoughts of dropping out of medical school: A multi-institutional study. Acad. Med. 2010, 85, 94–102. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Tempski, P.; Santos, I.S.; Mayer, F.B.; Enns, S.C.; Perotta, B.; Paro, H.B.; Gannam, S.; Peleias, M.; Garcia, V.L.; Baldassin, S.; et al. Relationship among medical student resilience, educational environment and quality of life. PLoS ONE 2015, 10, e131535. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Li, D.; Xu, H.; Kang, M.; Ma, S. Empathy in Chinese eight-year medical program students: Differences by school year, educational stage, and future career preference. BMC Med. Educ. 2018, 18, 241. [Google Scholar] [CrossRef]
- Schulze, C.; Becker, M.; Finze, S.; Holtherm, C.; Hinder, J.; Lison, A. An evaluation of the significance of individual endogenous risk factors and medical and orthopaedic conditions on physical fitness in military executives. US Army Med. Dep. J. 2017, 105–110. [Google Scholar]
- Selvaraj, P.R.; Bhat, C.S. Predicting the mental health of college students with psychological capital. J. Ment. Health 2018, 27, 279–287. [Google Scholar] [CrossRef]
- Hew, K.F.; Lo, C.K. Flipped classroom improves student learning in health professions education: A meta-analysis. BMC Med. Educ. 2018, 18, 38. [Google Scholar] [CrossRef] [Green Version]
- Zeng, R.; Xiang, L.; Yue, R.; Zeng, J.; Wan, X.; Zuo, C. Friend or foe? Flipped classroom for undergraduate electrocardiogram learning: A randomized controlled study. BMC Med. Educ. 2017, 17, 53. [Google Scholar]
- Tang, F.; Chen, C.; Zhu, Y.; Zuo, C.; Zhong, Y.; Wang, N.; Zhou, L.; Zou, Y.; Liang, D. Comparison between flipped classroom and lecture-based classroom in ophthalmology clerkship. Med. Educ. Online 2017, 22, 1395679. [Google Scholar] [CrossRef]
- Gill, D.L.; Hammond, C.C.; Reifsteck, E.J.; Jehu, C.M.; Williams, R.A.; Adams, M.M.; Lange, E.H.; Becofsky, K.; Rodriguez, E.; Shang, Y.T. Physical activity and quality of life. J. Prev. Med. Public Health 2013, 46, S28–S34. [Google Scholar] [CrossRef] [PubMed]
- Peleias, M.; Tempski, P.; Paro, H.B.; Perotta, B.; Mayer, F.B.; Enns, S.C.; Gannam, S.; Pereira, M.A.; Silveira, P.S.; Santos, I.S.; et al. Leisure time physical activity and quality of life in medical students: Results from a multicentre study. BMJ Open Sport Exerc. Med. 2017, 3, e213. [Google Scholar] [CrossRef] [PubMed]
- Bize, R.; Johnson, J.A.; Plotnikoff, R.C. Physical activity level and health-related quality of life in the general adult population: A systematic review. Prev. Med. 2007, 45, 401–415. [Google Scholar] [CrossRef] [PubMed]
- Klavestrand, J.; Vingard, E. The relationship between physical activity and health-related quality of life: A systematic review of current evidence. Scand. J. Med. Sci. Sports 2009, 19, 300–312. [Google Scholar] [CrossRef] [PubMed]
- Ball, S.; Bax, A. Self-care in medical education: Effectiveness of health-habits interventions for first-year medical students. Acad. Med. 2002, 77, 911–917. [Google Scholar] [CrossRef]
- Gandevia, S.C. Some central and peripheral factors affecting human motoneuronal output in neuromuscular fatigue. Sports Med. 1992, 13, 93–98. [Google Scholar] [CrossRef]
- Marcora, S.M.; Staiano, W.; Manning, V. Mental fatigue impairs physical performance in humans. J. Appl. Physiol. (1985) 2009, 106, 857–864. [Google Scholar] [CrossRef]
- Tel, H. Sleep quality and quality of life among the elderly people. Neurol. Psychiatry Brain Res. 2013, 19, 48–52. [Google Scholar] [CrossRef]
- Chen, X.; Sekine, M.; Hamanishi, S.; Wang, H.; Gaina, A.; Yamagami, T.; Kagamimori, S. Lifestyles and health-related quality of life in Japanese school children: A cross-sectional study. Prev. Med. 2005, 40, 668–678. [Google Scholar] [CrossRef]
- Cirelli, C.; Tononi, G. Is sleep essential? PLoS Biol. 2008, 6, e216. [Google Scholar] [CrossRef]
- Besedovsky, L.; Lange, T.; Born, J. Sleep and immune function. Pflug. Arch. 2012, 463, 121–137. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Leproult, R.; Van Cauter, E. Role of sleep and sleep loss in hormonal release and metabolism. Endocr. Dev. 2010, 17, 11–21. [Google Scholar] [PubMed] [Green Version]
- Cheng, S.H.; Shih, C.C.; Lee, I.H.; Hou, Y.W.; Chen, K.C.; Chen, K.T.; Yang, Y.K.; Yang, Y.C. A study on the sleep quality of incoming university students. Psychiatry Res. 2012, 197, 270–274. [Google Scholar] [CrossRef] [PubMed]
- Correa, C.C.; Oliveira, F.K.; Pizzamiglio, D.S.; Ortolan, E.; Weber, S. Sleep quality in medical students: A comparison across the various phases of the medical course. J. Bras. Pneumol. 2017, 43, 285–289. [Google Scholar] [CrossRef] [PubMed]
- Halson, S.L. Sleep in elite athletes and nutritional interventions to enhance sleep. Sports Med. 2014, 44 (Suppl. S1), S13–S23. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kelley, G.A.; Kelley, K.S. Exercise and sleep: A systematic review of previous meta-analyses. J. Evid. Based Med. 2017, 10, 26–36. [Google Scholar] [CrossRef]



{kind=link}
{kind=link}
| Dimension | Item Number | Reliability | Spearman’s Correlation Coefficient | ||
|---|---|---|---|---|---|
| Split-Half Reliability | Cronbach’s α Coefficient | PCS | MCS | ||
| PF | 10 | 0.894 | 0.813 | 0.481 | 0.240 |
| RP | 4 | 0.877 | 0.864 | 0.863 | 0.444 |
| BP | 2 | 0.897 | 0.879 | 0.706 | 0.328 |
| GH | 5 | 0.851 | 0.839 | 0.740 | 0.472 |
| VT | 4 | 0.841 | 0.713 | 0.362 | 0.716 |
| SF | 2 | 0.516 | 0.481 | 0.452 | 0.691 |
| RE | 3 | 0.846 | 0.839 | 0.414 | 0.867 |
| MH | 5 | 0.829 | 0.770 | 0.393 | 0.754 |
| Variable | N(%) (n = 416) | PF | RP | BP | GH | VT | SF | RE | MH |
|---|---|---|---|---|---|---|---|---|---|
| Gender | |||||||||
| Male | 159 (38.22%) | 93.52 (12.15) | 69.30 (39.62) | 73.48 (20.52) | 61.86 (20.63) | 61.10 (17.59) | 77.43 (19.58) | 46.96 (43.45) | 61.43 (17.29) |
| Female | 257 (61.78%) | 93.23 (8.72) | 70.43 (37.71) | 71.42 (19.74) | 58.70 (19.01) | 61.46 (16.66) | 78.99 (16.88) | 41.89 (42.75) | 60.33 (16.91) |
| Major | |||||||||
| Clinical medicine (eight-year programme) in the 4th year | 75 (18.03%) | 92.07 (11.69) | 61.24 b (43.05) | 70.35 a (18.61) | 56.71 a (20.58) | 56.93 a (16.25) | 77.19 a (18.17) | 40.44 (42.90) | 57.87 a (18.59) |
| Clinical medicine (five-year programme) in the 4th year | 92 (22.12%) | 94.08 (7.98) | 68.48 (38.31) | 73.49 (19.43) | 59.85 (20.62) | 61.03 (15.17) | 79.59 (18.07) | 44.93 (44.87) | 60.61 (15.39) |
| Preventive medicine in the 4th year | 85 (20.43%) | 91.76 (14.88) | 72.35 (38.77) | 77.11 (20.00) | 62.11 (18.07) | 63.94 (17.85) | 78.82 (15.68) | 47.06 (42.82) | 63.53 (15.61) |
| Oral medicine in the 4th year | 81 (19.47%) | 94.32 (7.15) | 78.40 (35.30) | 71.72 (20.74) | 66.47 (16.65) | 65.93 (15.43) | 82.03 (15.87) | 50.62 (43.82) | 65.73 (14.35) |
| Clinical medicine (five-year programme) in the 3rd year | 83 (19.95%) | 94.34 (6.71) | 68.98 (35.48) | 67.92 (20.56) | 54.22 (20.30) | 58.43 (18.87) | 74.16 (20.98) | 35.74 (39.91) | 55.81 (19.49) |
| Total | 416 (100%) | 93.34 (10.16) | 70.00 (38.41) | 72.20 (20.04) | 59.91 (19.68) | 61.32 (17.00) | 78.39 (17.96) | 43.83 (43.04) | 60.75 (17.04) |
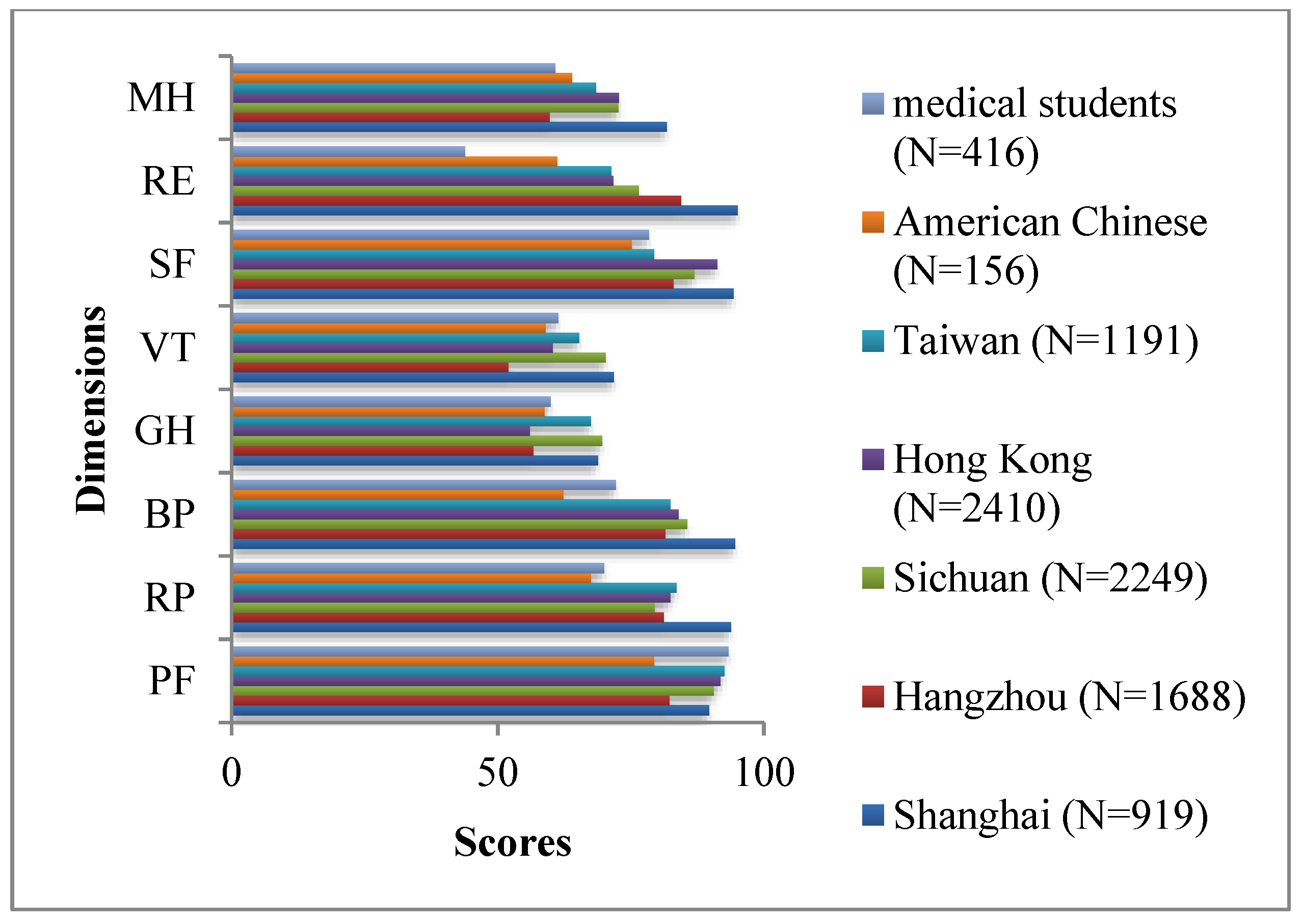
| Dimension | Medical Students (N = 416) | American Chinese (N = 156) | Taiwanese (N = 1191) | Hong Kong (N = 2410) | Sichuan (N = 2249) | Hangzhou (N = 1688) | Shanghai (N = 919) |
|---|---|---|---|---|---|---|---|
| PF | 93.34 (10.16) | 79.4 (23.4) | 92.6 (11.5) | 91.8 (12.9) | 90.6 (15.4) | 82.2 (19.8) | 89.7 (14.8) |
| RP | 70.00 (38.41) | 67.5 (37.3) | 83.6 (28.9) | 82.4 (31.0) | 79.5 (34.7) | 81.2 (33.6) | 93.8 (22.6) |
| BP | 72.20 (20.04) | 62.3 (21.9) | 82.4 (16.8) | 84.0 (21.9) | 85.6 (18.4) | 81.5 (20.5) | 94.6 (13.8) |
| GH | 59.91 (19.68) | 58.8 (22.7) | 67.5 (18.2) | 56.0 (20.2) | 69.6 (21.3) | 56.7 (20.2) | 68.8 (19.4) |
| VT | 61.32 (17.00) | 59.0 (20.3) | 65.3 (15.2) | 60.3 (18.7) | 70.3 (17.1) | 52.0 (20.9) | 71.8 (18.3) |
| SF | 78.39 (17.96) | 75.1 (22.7) | 79.4 (16.0) | 91.2 (16.5) | 86.9 (17.3) | 83.0 (17.8) | 94.3 (12.1) |
| RE | 43.83 (43.04) | 61.2 (43.7) | 71.3 (37.0) | 71.7 (38.4) | 76.5 (38.5) | 84.4 (32.4) | 95.1 (20.6) |
| MH | 60.75 (17.04) | 63.9 (20.4) | 68.4 (14.7) | 72.8 (16.6) | 72.7 (16.8) | 59.7 (22.7) | 81.8 (14.7) |
| Variables | N (%) (n2 = 416) | PF | RP | BP | GH | VT | SF | RE | MH |
|---|---|---|---|---|---|---|---|---|---|
| Physical exercise times per week | |||||||||
| Never | 185 (44.47%) | 92.27 a (10.17) | 68.48 (38.77) | 69.94 (20.07) | 55.50 a (19.22) | 58.89 a (17.17) | 77.12 (18.32) | 41.62 (42.60) | 58.03 a (17.24) |
| 1–2 | 152 (36.54%) | 93.62 (9.28) | 69.90 (38.85) | 73.21 (20.22) | 61.39 (19.43) | 63.59 (16.43) | 79.17 (17.64) | 45.83 (43.20) | 62.18 (16.98) |
| 3–4 | 63 (15.14%) | 96.35 (10.21) | 73.02 (37.65) | 74.32 (18.91) | 68.32 (18.73) | 63.10 (17.40) | 80.07 (17.87) | 48.15 (44.31) | 65.14 (16.02) |
| >4 | 16 (3.85%) | 91.25 (15.11) | 76.56 (34.72) | 80.50 (20.32) | 63.69 (19.00) | 60.94 (16.45) | 79.17 (17.63) | 33.33 (42.16) | 61.25 (15.37) |
| Post-exercise status | |||||||||
| Pleasant | 158 (37.98%) | 94.81 b (11.42) | 78.64 b (33.01) | 75.20 a (19.09) | 67.54 a (18.43) | 67.78 a (14.02) | 80.45 (16.66) | 47.68 (44.41) | 66.20 a (15.34) |
| Somewhat invigorated | 134 (32.21%) | 93.54 (7.22) | 68.66 (38.74) | 69.99 (18.97) | 56.19 (18.55) | 57.80 (17.76) | 79.10 (16.24) | 41.79 (41.02) | 58.51 (16.32) |
| No change | 39 (9.38%) | 92.05 (7.76) | 66.03 (42.72) | 74.49 (21.98) | 56.33 (16.50) | 59.10 (17.05) | 78.35 (18.19) | 47.86 (45.75) | 59.59 (20.06) |
| A little exhausted | 68 (16.35%) | 91.18 (11.75) | 59.46 (43.29) | 68.43 (21.34) | 53.01 (20.95) | 56.25 (17.73) | 73.86 (20.48) | 40.20 (42.93) | 53.71 (17.77) |
| Exhausted | 17 (4.09%) | 89.71 (13.40) | 51.47 (35.87) | 71.71 (24.39) | 54.00 (20.21) | 54.41 (15.80) | 71.90 (26.97) | 29.41 (38.88) | 58.59 (13.34) |
| Satisfaction with your family | |||||||||
| Very satisfied | 141 (33.89%) | 93.55 a (11.33) | 70.57 (38.42) | 74.62 a (19.56) | 64.22 a (18.54) | 65.71 a (16.24) | 80.69 b (17.65) | 46.57 b (42.52) | 64.28 a (18.18) |
| Relatively satisfied | 198 (47.60%) | 93.33 (10.08) | 72.31 (37.61) | 73.51 (19.93) | 59.46 (19.17) | 61.72 (15.75) | 79.63 (15.38) | 47.31 (43.16) | 61.62 (15.02) |
| General | 57 (13.70%) | 94.04 (6.37) | 63.16 (38.41) | 64.35 (19.83) | 54.39 (21.27) | 51.84 (18.44) | 71.15 (20.34) | 30.99 (42.66) | 51.86 (17.71) |
| Relatively dissatisfied | 16 (3.85%) | 93.44 (6.76) | 68.75 (45.19) | 64.75 (17.10) | 55.19 (18.75) | 55.00 (13.90) | 74.31 (19.76) | 33.33 (40.37) | 53.25 (15.91) |
| Very dissatisfied | 4 (0.96%) | 76.25 (14.93) | 37.50 (43.30) | 64.00 (29.74) | 27.50 (14.43) | 47.50 (31.23) | 55.56 (52.12) | 0.00 (0.00) | 50.00 (15.14) |
| Distressing family events in one year | |||||||||
| Yes | 60 (14.42%) | 92.33 (14.66) | 61.25c (42.29) | 69.68 (22.45) | 59.20 (20.95) | 60.75 (18.29) | 75.37 (22.32) | 40.00 (44.60) | 59.93 (17.39) |
| No | 356 (85.58%) | 93.51 (9.20) | 71.47 (37.58) | 72.63 (19.61) | 60.03 (19.49) | 61.42 (16.80) | 78.90 (17.10) | 44.48 (42.80) | 60.89 (17.00) |
| Time for extracurricular research (T1) | |||||||||
| None | 237 (56.97%) | 93.12 (10.97) | 69.28 (38.26) | 71.47 (20.38) | 59.12 (20.72) | 60.49 (18.48) | 79.13 (18.43) | 43.32 (42.62) | 60.86 (17.81) |
| T1 < 2 h | 106 (25.48%) | 93.77 (8.04) | 68.40 (41.16) | 73.51 (19.95) | 60.04 (19.25) | 62.59 (14.63) | 78.41 (16.72) | 41.82 (42.68) | 61.81 (16.15) |
| 2 ≤ T1 < 4 h | 32 (7.69%) | 93.75 (7.30) | 72.66 (37.22) | 73.31 (17.14) | 63.09 (18.31) | 65.47 (12.85) | 76.39 (15.39) | 47.92 (46.33) | 61.75 (13.48) |
| 4 ≤ T1 < 6 h | 12 (2.88%) | 91.25 (21.12) | 66.67 (40.36) | 71.17 (19.80) | 57.00 (16.51) | 60.83 (15.79) | 77.78 (17.08) | 55.56 (43.42) | 55.00 (12.20) |
| T1 ≥ 6 h | 29 (6.97%) | 93.97 (5.88) | 80.17 (29.41) | 72.66 (21.62) | 63.59 (14.92) | 59.14 (16.91) | 74.71 (21.60) | 45.98 (45.79) | 57.24 (18.98) |
| Relationship with roommates | |||||||||
| Very good | 101 (24.28%) | 93.81 (12.00) | 77.72 b (34.80) | 77.07 a (17.64) | 61.61 a (19.62) | 66.04 a (15.63) | 83.94 b (15.19) | 53.47 a (43.23) | 67.45 b (13.42) |
| Good | 232 (55.77%) | 93.68 (9.37) | 71.44 (37.45) | 70.70 (19.97) | 60.80 (18.91) | 61.29 (16.33) | 78.54 (17.56) | 41.95 (42.78) | 61.14 (16.43) |
| General | 72 (17.31%) | 91.74 (9.90) | 56.50 (42.45) | 70.81 (21.29) | 56.25 (21.86) | 57.36 (18.15) | 73.46 (17.65) | 39.81 (42.84) | 52.61 (19.26) |
| Bad or very bad | 11 (2.64%) | 92.27 (9.58) | 56.82 (41.97) | 68.45 (28.36) | 49.45 (17.62) | 44.55 (20.18) | 56.57 (26.97) | 21.21 (34.23) | 44.36 (12.58) |
| Sleep quality | |||||||||
| Very good | 74 (17.79%) | 95.34 a (7.82) | 80.74 b (30.84) | 78.00 a (16.26) | 68.45 b (19.54) | 69.59 a (14.16) | 81.38 b (19.30) | 56.31 b (44.46) | 67.89 a (13.75) |
| Good | 147 (35.34%) | 94.29 (852) | 78.23 (33.01) | 74.04 (19.49) | 63.80 (16.47) | 64.63 (14.83) | 81.56 (16.53) | 48.30 (43.65) | 64.14 (15.13) |
| General | 126 (30.29%) | 92.42 (12.72) | 62.30 (41.44) | 70.87 (21.35) | 56.50 (20.53) | 59.68 (16.39) | 78.48 (14.99) | 42.06 (42.20) | 59.21 (17.01) |
| Bad or very bad | 69 (16.59%) | 90.87 (9.81) | 54.97 (43.29) | 64.51 (20.16) | 48.68 (18.31) | 48.41 (17.61) | 68.28 (20.81) | 24.15 (34.72) | 48.70 (17.73) |
| Variable | PF | RP | BP | GH | VT | SF | RE | MH |
|---|---|---|---|---|---|---|---|---|
| Clinical medicine (eight-year programme) in the 4th year | NI | NS | NS | NS | NS | NS | NI | NS |
| Clinical medicine (five-year programme) in the 4th year | NI | NS | NS | NS | NS | NS | NI | NS |
| Preventive medicine in the 4th year | NI | NS | 0.124 | NS | 0.113 | NS | NI | 0.131 |
| Oral medicine in the 4th year | NI | NS | NS | 0.136 | 0.124 | NS | NI | 0.144 |
| Clinical medicine (five-year programme) in the 3rd year | NI | NS | NS | NS | NS | NS | NI | NS |
| Physical exercise times per week | NI | NI | NI | 0.160 | NS | NI | NI | NS |
| Post-exercise status | 0.122 | 0.145 | NS | 0.136 | 0.150 | NI | NI | 0.126 |
| Satisfaction with your family | NS | NI | 0.103 | 0.106 | 0.130 | 0.107 | NS | 0.101 |
| Relationship with roommates | NI | 0.113 | NS | NS | 0.124 | 0.209 | NS | 0.240 |
| Sleep quality | 0.121 | 0.189 | 0.175 | 0.250 | 0.269 | 0.138 | 0.223 | 0.222 |
© 2019 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Qiu, Y.; Yao, M.; Guo, Y.; Zhang, X.; Zhang, S.; Zhang, Y.; Huang, Y.; Zhang, L. Health-Related Quality of Life of Medical Students in a Chinese University: A Cross-Sectional Study. Int. J. Environ. Res. Public Health 2019, 16, 5165. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph16245165
Qiu Y, Yao M, Guo Y, Zhang X, Zhang S, Zhang Y, Huang Y, Zhang L. Health-Related Quality of Life of Medical Students in a Chinese University: A Cross-Sectional Study. International Journal of Environmental Research and Public Health. 2019; 16(24):5165. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph16245165
Chicago/Turabian StyleQiu, Yanli, Mingkang Yao, Yiwei Guo, Xiaowei Zhang, Shuoyang Zhang, Yuting Zhang, Yixiang Huang, and Lingling Zhang. 2019. "Health-Related Quality of Life of Medical Students in a Chinese University: A Cross-Sectional Study" International Journal of Environmental Research and Public Health 16, no. 24: 5165. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph16245165