Roadside Exposure and Inflammation Biomarkers among a Cohort of Traffic Police in Kathmandu, Nepal

Abstract
:1. Introduction
2. Method
2.1. Study Population
2.2. Sampling
2.3. Blood Sample Collection and Biomarker Analysis
2.4. Air Pollution Exposure
2.5. Data Analysis
3. Results
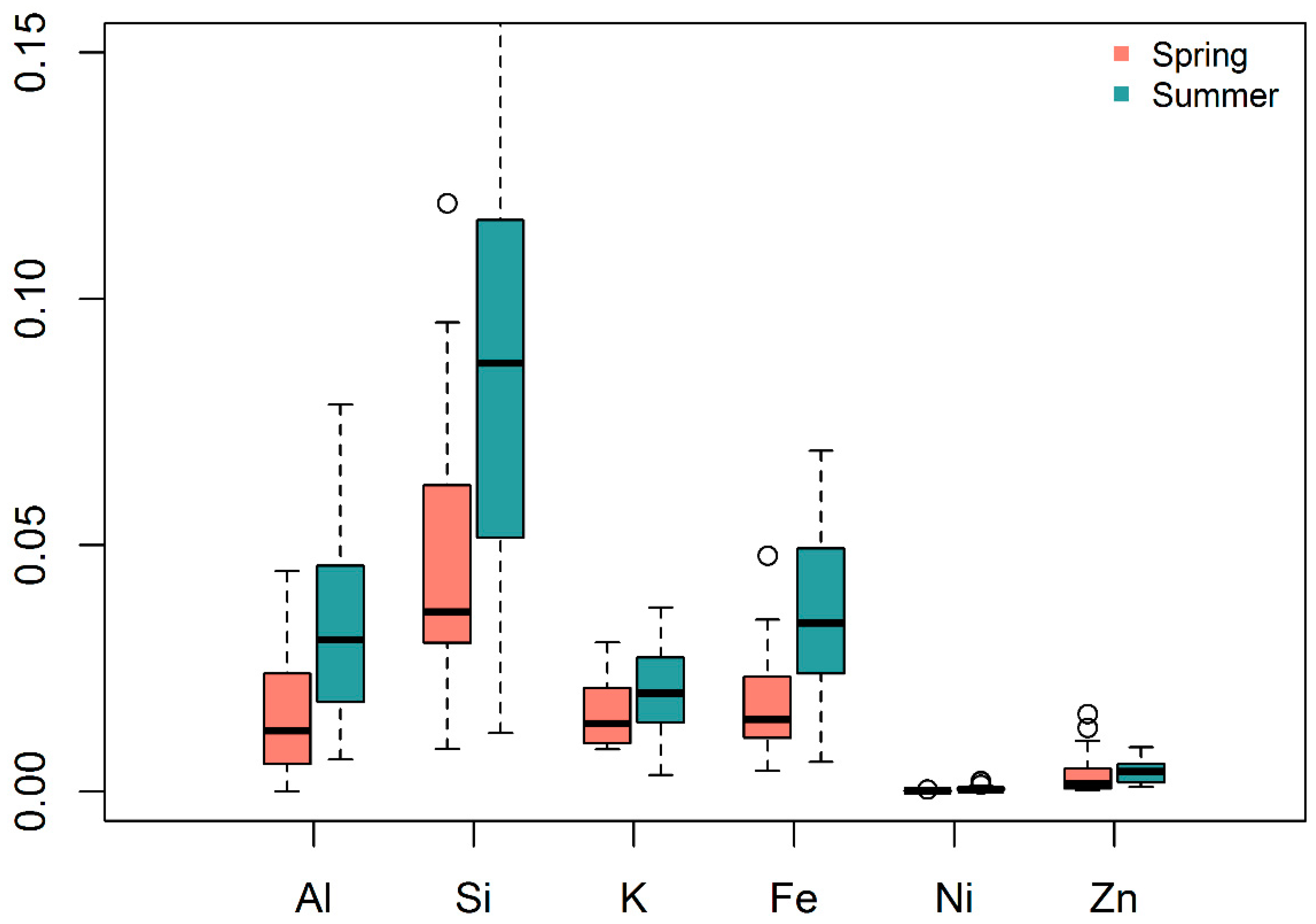
3.1. Air Pollution Exposure over Seasons
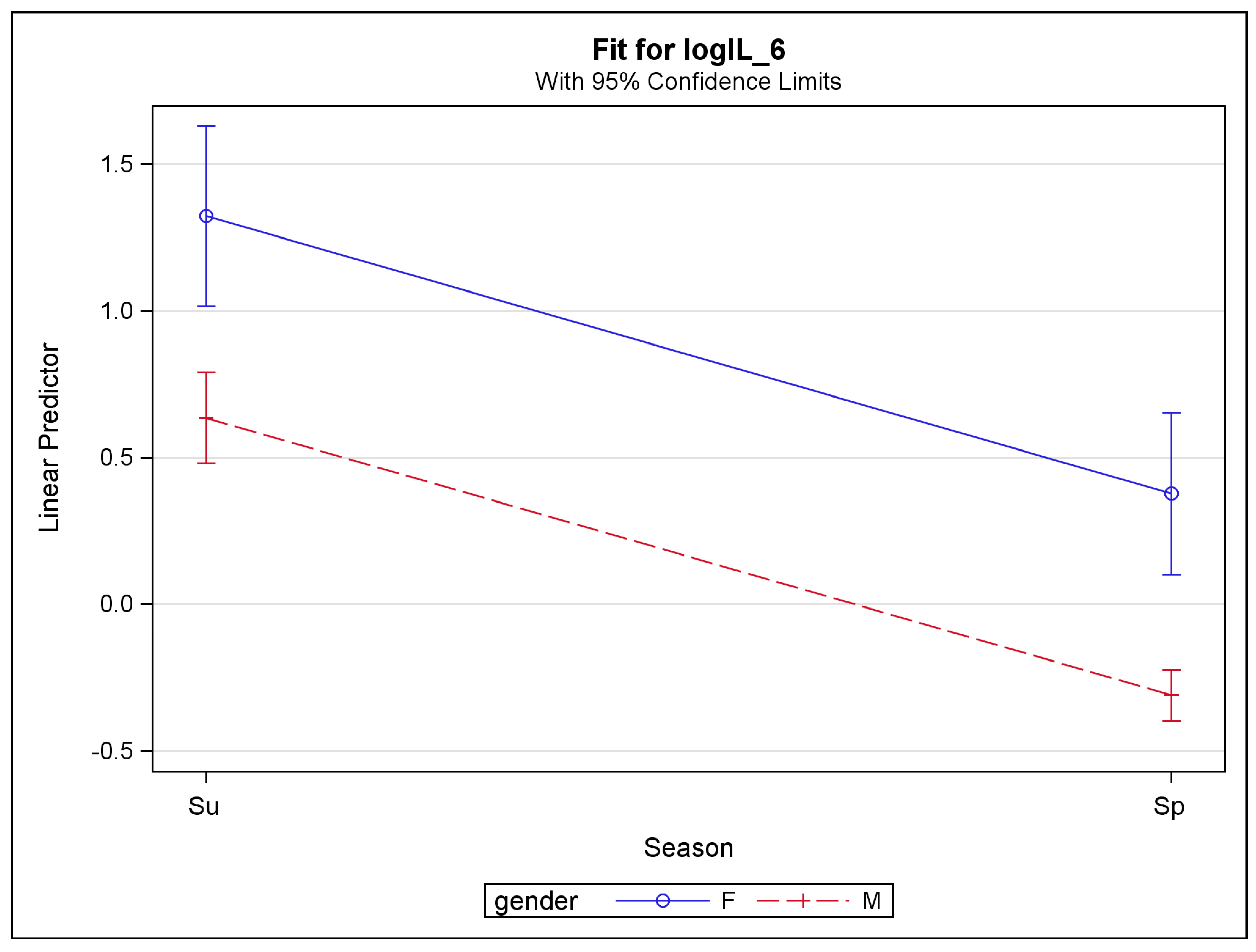
3.2. Biomarkers over Seasons
3.3. Effects of Air Pollution and Various Factors on Biomarkers
4. Discussion
4.1. Air Pollution Exposure
4.2. Biomarkers
4.3. Limitations
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- Brook, R.D. You are what you breathe: Evidence linking air pollution and blood pressure. Curr. Hypertens. Rep. 2005, 7, 427–434. [Google Scholar] [CrossRef]
- Brugge, D.; Durant, J.L.; Rioux, C. Near-highway pollutants in motor vehicle exhaust: A review of epidemiologic evidence of cardiac and pulmonary health risks. Environ. Health 2007, 6, 23. [Google Scholar] [CrossRef] [Green Version]
- Shakya, K.M.; Rupakheti, M.; Aryal, K.; Peltier, R.E. Respiratory effects of high levels of particulate exposure in a cohort of traffic police in Kathmandu, Nepal. J. Occup. Environ. Med. 2016, 58, e218–e225. [Google Scholar] [CrossRef] [PubMed]
- Jerrett, M.; McConnell, R.; Chang, C.C.R.; Wolch, J.; Reynolds, K.; Lurmann, F.; Gilliland, F.; Berhane, K. Automobile traffic around the home and attained body mass index: A longitudinal cohort study of children aged 10–18 years. Prev. Med. 2015, 50, S50–S58. [Google Scholar] [CrossRef] [PubMed]
- Malley, C.S.; Kuylenstierna, J.C.I.; Vallack, H.W.; Henze, D.K.; Blencowe, H.; Ashmore, M.R. Preterm birth associated with maternal fine particulate matter exposure: A global, regional and national assessment. Environ. Int. 2017, 101, 173–182. [Google Scholar] [CrossRef] [PubMed]
- Weisskopf, M.G.; Kioumourtzoglou, M.A.; Roberts, A.L. Air pollution and autism spectrum disorders: Causal or confounded? Curr. Environ. Health Rep. 2015, 2, 430–439. [Google Scholar] [CrossRef]
- Bowe, B.; Xie, Y.; Li, T.; Yan, Y.; Xian, H.; Al-Aly, Z. Associations of ambient coarse particulate matter, nitrogen dioxide, and carbon monoxide with the risk of kidney disease: A cohort study. Lancet Planet Health 2017, 1, 267–276. [Google Scholar] [CrossRef]
- Power, M.C.; Adar, S.D.; Yanosky, J.D.; Weuve, J. Exposure to air pollution as a potential contributor to cognitive function, cognitive decline, brain imaging, and dementia: A systematic review of epidemiologic research. Neurotoxicology 2016, 56, 235–253. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Dockery, D.W.; Pope, C.A.; Xu, X.; Spengler, J.D.; Ware, J.H.; Fay, M.E.; Ferris, B.G., Jr.; Speizer, F.E. An association between air pollution and mortality in six U.S. cities. N. Engl. J. Med. 1993, 329, 1753–1759. [Google Scholar] [CrossRef]
- Beil, L. The list of diseases linked to air pollution is growing. Sci. News 2017, 192, 18. [Google Scholar]
- Ghio, A.J.; Kim, C.; Devlin, R.B. Concentrated ambient air particles induce mild pulmonary inflammation in healthy human volunteers. Am. J. Respir. Crit. Care Med. 2000, 162, 981–988. [Google Scholar] [CrossRef] [PubMed]
- Pope, C.A., III; Hansen, M.L.; Long, R.W.; Nielsen, K.R.; Eatough, N.L.; Wilson, W.E.; Eatough, D.J. Ambient particulate air pollution, heart rate variability, and blood markers of inflammation in a panel of elderly subjects. Environ. Health Perspect. 2004, 112, 339–345. [Google Scholar] [CrossRef] [PubMed]
- Kido, T.; Tamagawa, E.; Bai, N.; Suda, K.; Yang, H.H.; Li, Y.; Chiang, G.; Yatera, K.; Mukae, H.; Sin, D.D.; Van Eeden, S.F. Particulate matter induces translocation of IL-6 from the lung to the systemic circulation. Am. J. Respir. Cell Mol. Biol. 2011, 44, 197–204. [Google Scholar] [CrossRef] [PubMed]
- Alfaro-Moreno, E.; Garcia-Cuellar, C.; De-Vizcaya-Ruiz, A.; Rojas-Bracho, L.; Osornio-Vargas, A. Cellular mechanisms behind particulate matter air pollution related health effects. In Air Pollution: Health and Environmental Impacts; Taylor & Francis Group: Boca Raton, FL, USA, 2010. [Google Scholar]
- Takizawa, H.; Abe, S.; Ohtoshi, T.; Kawasaki, S.; Takami, K.; Desaki, M.; Sugawara, I.; Hashimoto, S.; Azuma, A.; Nakahara, K.; Kudoh, S. Diesel exhaust particles up-regulate expression of intercellular adhesion molecules-1 (ICAM-1) in human bronchial epithelial cells. Clin. Exp. Immunol. 2000, 120, 356–362. [Google Scholar] [CrossRef]
- Ishii, H.; Fujii, T.; Hogg, J.C.; Hayashi, S.; Mukae, H.; Vincent, R.; van Eeden, S.F. Contribution of IL-1 beta and TNF-alpha to the initiation of the peripheral lung response to atmospheric particulates (PM10). Am. J. Physiol. Lung Cell Mol. Physiol. 2004, 287, L176–L183. [Google Scholar] [CrossRef] [PubMed]
- Fujimaki, H.; Kurokawa, S.; Yamamoto, S.; Satoh, M. Distinct requirements for interleukin-6 in airway inflammation induced by diesel exhaust in mice. Immunopharmacol. Immunotoxicol. 2006, 28, 703–714. [Google Scholar] [CrossRef]
- Zhang, X.; Staimer, N.; Gillen, D.L.; Tjoa, T.; Schauer, J.J.; Shafer, M.M.; Hasheminassab, S.; Pakbin, P.; Vaziri, N.D.; Sioutas, C.; Delfino, R.J. Associations of oxidative stress and inflammatory biomarkers with chemically-characterized air pollutant exposures in an elderly cohort. Environ. Res. 2016, 150, 306–319. [Google Scholar] [CrossRef] [Green Version]
- Rioux, C.L.; Tucker, K.L.; Mwamburi, M.; Gute, D.M.; Cohen, S.A.; Brugge, D. Residential traffic exposure, pulse pressure, and C-reactive protein: Consistency and contrast among exposure characterization methods. Environ. Health Perspect. 2010, 118, 803–811. [Google Scholar] [CrossRef] [PubMed]
- Devlin, R.B.; Duncan, K.E.; Jardim, M.; Schmitt, M.T.; Rappold, A.G.; Diaz-Sanchez, D. Controlled exposure of healthy young volunteers to ozone causes cardiovascular effects. Circulation 2012, 126, 104–111. [Google Scholar] [CrossRef]
- Plummer, L.E.; Pinkerton, K.E.; Madl, A.K.; Wilson, D.W. Effects of nanoparticles on the pulmonary vasculature. In Cardiovascular Effects of Inhaled Ultrafine and Nanosized Particles; John Wiley & Sons, Inc.: Hoboken, NJ, USA, 2011. [Google Scholar]
- Brucker, N.; Moro, A.M.; Charão, M.F.; Durgante, J.; Freitas, F.; Baierle, M.; Nascimento, S.; Gauer, B.; Bulcão, R.P.; Bubols, G.B.; et al. Biomarkers of occupational exposure to air pollution, inflammation and oxidative damage in taxi drivers. Sci. Total Environ. 2013, 463–464, 884–893. [Google Scholar] [CrossRef] [PubMed]
- Chiu, Y.-H.M.; Garshick, E.; Hart, J.E.; Spiegelman, D.; Dockery, D.W.; Smith, T.J.; Laden, F. Occupational vehicle-related particulate exposure and inflammatory markers in trucking industry workers. Environ. Res. 2016, 148, 310–317. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Sun, Q.; Yue, P.; Deiuliis, J.A.; Lumeng, C.N.; Kampfrath, T.; Mikolaj, M.B.; Cai, Y. Ambient air pollution exaggerates adipose inflammation and insulin resistance in a mouse model of diet-induced obesity. Circulation 2009, 119, 538–546. [Google Scholar] [CrossRef]
- Kodavanti, U.P.; Chen, L.-C.; Costa, D.L. Experimental studies in animals. In Cardiovascular Effects of Inhaled Ultrafine and Nanosized Particles; John Wiley & Sons, Inc.: Hoboken, NJ, USA, 2011. [Google Scholar]
- Møller, P.; Danielsen, P.H.; Karottki, G.D.; Jantzen, K.; Roursgaard, M.; Klingberg, H.; Jensen, D.M.; Chrotophersen, D.V.; Hemmingsen, J.G.; Cao, Y.; et al. Oxidative stress and inflammation generated DNA damage by exposure to air pollution particles. Mutat. Res. 2014, 762, 133–166. [Google Scholar] [CrossRef] [PubMed]
- Vattanasit, U.; Navasumri, P.; Khadka, M.B.; Kanitwithayanun, J.; Promvijit, J.; Autrup, H.; Ruchirawat, M. Oxidative DNA damage and inflammatory responses in cultured human cells and in humans exposed to traffic-related particles. Int. J. Hyg. Environ. Health 2014, 217, 23–33. [Google Scholar] [CrossRef] [PubMed]
- Alexeeff, S.E.; Coull, B.A.; Gryparis, A.; Suh, H.; Sparrow, D.; Vokonas, P.S.; Schwartz, J. Medium-term exposure to traffic-related air pollution and markers of inflammation and endothelial function. Environ. Res. Perspect. 2011, 119, 481–486. [Google Scholar] [CrossRef]
- Zhao, J.; Gao, Z.; Tian, Z.; Xie, Y.; Xin, F.; Jiang, R.; Kan, H.; Song, W. The biological effects of individual-level PM2.5 exposure on systemic immunity and inflammatory response in traffic policemen. Occup. Environ. Med. 2013, 70, 426–431. [Google Scholar] [CrossRef]
- Neophytou, A.M.; Hart, J.E.; Cavallari, J.M.; Smith, T.J.; Dockery, D.W.; Coull, B.A.; Garshick, E.; Laden, F. Traffic-related exposures and biomarkers of systemic inflammation, endothelial activation and oxidative stress: A panel study in the US trucking industry. Environ. Health 2013, 12, 105. [Google Scholar] [CrossRef]
- Dobreva, Z.G.; Kostadinova, G.S.; Popov, B.N.; Petkov, G.S.; Stanilova, S.A. Proinflammatory and anti-inflammatory cytokines in adolescents from Southeast Bulgarian cities with different levels of air pollution. Toxicol. Ind. Health 2015, 31, 1210–1217. [Google Scholar] [CrossRef]
- Ghio, A.J.; Hall, A.; Bassett, M.A.; Cascio, W.E.; Devlin, R.B. Exposure to concentrated ambient air particles alters hematologic indices in humans. Inhal. Toxicol. 2003, 15, 1465–1478. [Google Scholar] [CrossRef]
- Mills, N.L.; Robinson, S.D.; Fokkens, P.H.; Leseman, D.L.; Miller, M.R.; Anderson, D.; Freney, E.J.; Heal, M.R.; Donovan, R.J.; Blomberg, A.; et al. Exposure to concentrated ambient particles does not affect vascular function in patients with coronary heart disease. Environ. Health Perspect. 2008, 116, 709–715. [Google Scholar] [CrossRef]
- Brook, R.D.; Urch, B.; Dvonch, J.T.; Bard, R.L.; Speck, M.; Keeler, G.; Morishita, M.; Marsik, F.J.; Kamal, A.S.; Kaciroti, N.; et al. Insights into the mechanisms and emdiators of the effects of air pollution exposure on blood pressure and vascular function in healthy humans. Hypertension 2009, 54, 659–667. [Google Scholar] [CrossRef]
- Strak, M.; Hoek, G.; Godri, K.J.; Gosens, I.; Mudway, I.S.; van Oerle, R.; Spronk, H.M.; Cassee, F.R.; Lebret, E.; Kelly, F.J.; et al. Composition of PM affects acute vascular inflammatory and coagulative markers—The RAPTES Project. PLoS ONE 2013, 8, e58944. [Google Scholar] [CrossRef] [PubMed]
- Bind, M.A.; Coull, B.; Suh, H.; Wright, R.; Baccarelli, A.; Vokonas, P.; Schwartz, J. A novel genetic score approach using instruments to investigate interactions between pathways and environment: Application to air pollution. PLoS ONE 2014, 9, e96000. [Google Scholar] [CrossRef] [PubMed]
- Dutta, A.; Roychoudhury, S.; Chowdhury, S.; Ray, M.R. Changes in sputum cytology, airway inflammation and oxidative stress due to chronic inhalation of biomass smoke during cooking in premenopausal rural Indian women. Int. J. Hyg. Environ. Health 2013, 216, 301–318. [Google Scholar] [CrossRef]
- Aryal, R.K.; Lee, B.-K.; Karki, R.; Gurung, A.; Kandasamy, J.; Pathak, B.K.; Sharma, S.; Giri, N. Seasonal PM10 dynamics in Kathmandu Valley. Atmos. Environ. 2008, 42, 8623–8633. [Google Scholar] [CrossRef]
- Kiros, F.; Shakya, K.M.; Rupakheti, M.; Regmi, R.P.; Maharjan, R.; Byanju, R.M.; Naja, M.; Mahata, K.; Kathayat, B.; Peltier, R.E. Variability of anthropogenic gases: Nitrogen oxides, sulfur dioxide, ozone and ammonia at Kathmandu Valley, Nepal. Aerosol Air Qual. Res. 2016, 16, 3088–3101. [Google Scholar] [CrossRef]
- Shakya, K.M.; Rupakheti, M.; Shahi, A.; Maskey, R.; Pradhan, B.; Panday, A.; Puppala, S.P.; Lawrence, M.; Peltier, R.E. Near-road sampling of PM2.5, BC, and fine-particle chemical components in Kathmandu Valley, Nepal. Atmos. Chem. Phys. 2017, 17, 6503–6516. [Google Scholar] [CrossRef]
- Shakya, K.M.; Peltier, R.E.; Shrestha, H.; Byanju, R.M. Measurements of TSP, PM10, PM2.5, BC, and PM chemical composition from an urban residential location in Nepal. Atmos. Pollut. Res. 2017, 8, 1123–1131. [Google Scholar] [CrossRef]
- Chen, P.; Kang, S.; Li, C.; Rupakheti, M.; Yan, F.; Li, Q.; Ji, Z.; Zhang, Q.; Luo, W.; Sillanpaa, M. Characteristics and sources of polycylic aromatic hydrocarbons in atmospheric aerosols in the Kathmandu Valley, Nepal. Sci. Total Environ. 2015, 538, 86–92. [Google Scholar] [CrossRef]
- Kim, B.M.; Park, J.-S.; Kim, S.-W.; Kim, H.; Jeon, H.; Cho, C.; Kim, J.-H.; Hong, S.; Rupakheti, M.; Panday, A.K.; et al. Source apportionment of PM10 mass and particulate carbon in the Kathmandu Valley, Nepal. Atmos. Environ. 2015, 123, 190–199. [Google Scholar] [CrossRef]
- Tripathee, L.; Kang, S.; Rupakheti, D.; Zhang, Q.; Huang, J.; Sillanpaa, M. Water-soluble ionic composition of aerosols at urban location in the foothills of Himalaya, Pokhara Valley, Nepal. Atmosphere 2016, 7, 102. [Google Scholar] [CrossRef]
- Crebelli, R.; Tomei, F.; Zijno, A.; Ghittori, S.; Imbriani, M.; Gamberale, D.; Martini, A.; Carere, A. Exposure to benzene in urban workers: Environmental and biological monitoring of traffic police in Rome. Occup. Environ. Med. 2001, 58, 165–171. [Google Scholar] [CrossRef] [PubMed]
- Burgaz, S.; Demircigil, G.C.; Karahalil, B.; Karakaya, A.E. Chromosomal damage in peripheral blood lymphocytes of traffic policemen and taxi drivers exposed to urban air pollution. Chemosphere 2002, 47, 57–64. [Google Scholar] [CrossRef]
- Kamal, A.; Cincinelli, A.; Martellini, T.; Malik, R.N. Linking mobile source-PAHs and biological effects in traffic police officers and drivers in Rawalpindi (Pakistan). Ecotoxicol. Environ. Saf. 2016, 127, 135–143. [Google Scholar] [CrossRef]
- Carroll, R.J.; Ruppert, D. Transformation and Weighting in Regression; Chapman and Hall: London, UK, 1988. [Google Scholar]
- Cook, R.D.; Weisberg, S. Residuals and Influence in Regression; Chapman and Hall: New York, NY, USA, 1982. [Google Scholar]
- Schwarz, G. Estimating the dimension of a model. Ann. Stat. 1978, 6, 461–464. [Google Scholar] [CrossRef]
- Lawrence, S.; Sokhi, R.; Ravindra, K.; Mao, H.; Prain, H.D.; Bull, I.D. Source apportionments of traffic emissions of particulate matter using tunnel measurements. Atmos. Environ. 2013, 77, 548–557. [Google Scholar] [CrossRef]
- Invernizzi, G.; Ruprecht, A.; Mazza, R.; De Marco, C.; Mocnik, G.; Sioutas, C.; Westerdahl, D. Measurement of black carbon concentration as an indicator of air quality benefits of traffic restriction policies within the ecopass zone in Milan, Italy. Atmos. Environ. 2011, 45, 3522–3527. [Google Scholar] [CrossRef]
- Targino, A.C.; Gibson, M.D.; Krecl, P.; Rodrigues, M.V.C.; dos Santos, M.M.; Correa, M.P. Hotspots of black carbon and PM2.5 in an urban area and relationships to traffic characteristics. Environ. Pollut. 2016, 218, 475–486. [Google Scholar] [CrossRef]
- Liu, M.; Peng, X.; Meng, Z.; Zhou, T.; Long, L.; She, Q. Spatial characteristics and determinants of in-traffic black carbon in Shanghai, China: Combination of mobile monitoring and land use regression model. Sci. Total Environ. 2019, 658, 51–61. [Google Scholar] [CrossRef]
- Carter, J.D.; Ghio, A.J.; Samet, J.M.; Devlin, R.B. Cytokine production by human airway epithelial cells after exposure to an air pollution particle is metal-dependent. Toxicol. Appl. Pharmacol. 1997, 146, 180–188. [Google Scholar] [CrossRef]
- Brucker, N.; Moro, A.; Charão, M.; Bubols, G.; Nascimento, S.; Goethel, G.; Barth, A.; Prohmann, A.C.; Rocha, R.; Moresco, R.; et al. Relationship between blood metals and inflammation in taxi drivers. Clin. Chim. Acta 2015, 444, 176–181. [Google Scholar] [CrossRef]
- Ying, Z.; Rajagopalan, S. Hyptertension and vascular toxicity of PM. In Environmental Cardiology; The Royal Science of Chemistry: Cambridge, UK, 2011. [Google Scholar]
- Visser, M.; Bouter, L.M.; McQuillan, G.M.; Wener, M.H.; Harris, T.B. Elevated C-reactive protein levels in overweight and obese adults. JAMA 1999, 282, 2131–2135. [Google Scholar] [CrossRef]
- Yudkin, J.S.; Kumari, M.; Humphries, S.E.; Mohamed-Ali, V. Inflammation, obesity, stress and coronary heart diseas: Is interleukin-6 the link? Atherosclerosis 2000, 148, 209–214. [Google Scholar] [CrossRef]
- Wu, W.; Jin, Y.; Carlsten, C. Inflammatory health effects of indoor and outdoor particulate matter. J. Allergy Clin. Immunol. 2018, 141, 833–844. [Google Scholar] [CrossRef] [PubMed]
- Rückerl, R.; Hampel, R.; Breitner, S.; Cyrys, J.; Kraus, U.; Carter, J.; Dailey, L.; Devlin, R.B.; Diaz-Sanchez, D.; Koenig, W.; et al. Associations between ambient air pollution and blood markers of inflammation and coagulation/fibrinolysis in susceptible populations. Environ. Int. 2014, 70, 32–49. [Google Scholar] [CrossRef]
- Rückerl, R.; Schneider, A.; Hampel, R.; Breitner, S.; Cyrys, J.; Kraus, U.; Gu, J.; Soentgen, J.; Koenig, W.; Peters, A. Association of novel metrics of particulate matter with vascular markers of inflammation and coagulation in susceptible populations–results from a panel study. Environ. Res. 2016, 150, 337–347. [Google Scholar] [CrossRef] [PubMed]
- Zeltser, D.; Rogowski, O.; Berliner, S.; Mardi, T.; Justo, D.; Serov, J.; Rozenblat, M.; Avitzour, D.; Shapira, I. Sex differences in the expression of haemoorheological determinants in individuals with atherothrombotic risk factors and in apparently healthy people. Heart 2004, 90, 277–281. [Google Scholar] [CrossRef] [PubMed]
- Khera, A.; McGuire, D.K.; Murphy, S.A.; Stanek, H.G.; Das, S.R.; Vongpatanasin, W.; Wians, F.H., Jr.; Grundy, S.M.; de Lemos, J.A. Race and gender differences in C-reactive protein levels. J. Am. Coll. Cardiol. 2005, 46, 464–469. [Google Scholar] [CrossRef] [PubMed]
- Toker, S.; Shirom, A.; Shapira, I.; Berliner, S.; Melamed, S. The association between burnout, depression, anxiety, and inflammation biomarkers: C-reactive protein and fibrinogen in men and women. J. Occup. Health Psychol. 2005, 10, 344–362. [Google Scholar] [CrossRef]




{kind=link}
{kind=link}
{kind=link}
| Parameter | Spring | Summer | |||
|---|---|---|---|---|---|
| Mean | SD | Mean | SD | p-value 4 | |
| a. Description of subjects 1 | |||||
| BMI (kg/m2) | 32 | 5 | 32 | 3 | |
| Age | 28 | 5 | 28 | 5 | |
| Employment (years) | 5 | 3 | |||
| b. Air pollution measurements | |||||
| PM2.5 (μg/m3) 2 | 123.51 | 38.66 | 45.21 | 24.09 | 0.000 |
| BC (μgC/m3) 2 | 18.80 | 7.68 | 16.46 | 7.52 | 0.124 |
| Passive sampling 3 | |||||
| Ozone (μg/m3) | 14.02 | 9.57 | 16.6 | 6.52 | 0.633 |
| Sulfur dioxide (μg/m3) | 6.75 | 0.35 | 25.46 | 10.99 | 0.098 |
| Nitrogen dioxide (μg/m3) | 103.94 | 15.65 | 102.02 | 51.21 | 0.939 |
| Nitric oxide (μg/m3) | 134.03 | 41.64 | 126.33 | 94.30 | 0.903 |
| Biomarkers | Independent Samples | Dependent Samples | |||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|
| Summer | Spring | Independent t-Test | Summer–Spring | t-Test | Wilcox Test | ||||||
| Mean | Std. Dev. | Mean | Std. Dev. | t stat. | p-value | Mean Diff. | Std. Dev. Diff. | t stat | p-value | p-value | |
| CRP 1 | 4.11 | 3.26 | 2.47 | 2.59 | 1.91 | 0.064 | 1.98 | 2.71 | 2.53 | 0.028 * | 0.042 * |
| SAA 1 | 2.16 | 2.29 | 0.81 | 1.11 | 2.59 | 0.014 * | 1.49 | 1.76 | 2.94 | 0.013 * | 0.016 * |
| ICAM-1 1 | 0.83 | 0.41 | 0.64 | 0.21 | 2.07 | 0.046 * | 0.15 | 0.53 | 0.96 | 0.356 | 0.380 |
| VCAM-1 1 | 0.76 | 0.39 | 0.59 | 0.21 | 1.77 | 0.086 | 0.18 | 0.51 | 1.22 | 0.249 | 0.176 |
| IFN-γ 2 | 25.53 | 7.89 | 17.76 | 7.73 | 2.56 | 0.014 * | 5.58 | 8.89 | 2.17 | 0.052 | 0.064 |
| IL-1β 2 | 3.03 | 1.94 | 1.46 | 0.28 | 3.91 | 0.001 *** | 0.59 | 0.53 | 3.85 | 0.003 ** | 0.001 *** |
| IL-2 2 | 7.42 | 2.41 | 3.53 | 1.35 | 6.89 | 0.000 *** | 4.96 | 3.16 | 5.43 | 0.000 *** | 0.001 *** |
| IL-4 2 | 0.37 | 0.11 | 0.19 | 0.08 | 6.34 | 0.000 *** | 0.18 | 0.09 | 6.84 | 0.000 *** | 0.001 *** |
| IL-6 2 | 2.26 | 0.82 | 0.89 | 0.40 | 7.33 | 0.000 *** | 1.21 | 0.71 | 5.93 | 0.004 ** | 0.001 *** |
| IL-8 2 | 64.29 | 63.54 | 12.98 | 4.76 | 3.78 | 0.001 ** | 78.93 | 74.56 | 3.67 | 0.001 *** | 0.001 *** |
| IL-10 2 | 2.31 | 0.59 | 1.28 | 0.62 | 5.83 | 0.000 *** | 1.13 | 0.81 | 4.85 | 0.008 ** | 0.002 ** |
| IL-12 2 | 2.18 | 0.51 | 1.42 | 0.43 | 5.56 | 0.000 *** | 0.61 | 0.65 | 3.25 | 0.003 ** | 0.012 * |
| IL-13 2 | 1.49 | 0.59 | 0.56 | 0.34 | 6.64 | 0.000 *** | 0.62 | 0.57 | 3.78 | 0.008 ** | 0.005 ** |
| TNF-α 2 | 5.16 | 2.09 | 3.23 | 1.19 | 3.90 | 0.000 *** | 1.79 | 2.15 | 2.88 | 0.015 * | 0.001 ** |
| Effects | Categories | Estimate | Std. Error | DF | t Value | Pr > |t| |
|---|---|---|---|---|---|---|
| CRP 1 | ||||||
| Season | Summer | 0.3462 | 0.0616 | 53 | 1.90 | 0.0630 |
| PM2.5 | 0.0010 | 0.0005 | 53 | 5.62 | <0.0001 | |
| SAA 2 | ||||||
| Season | Summer | 1.4828 | 0.2742 | 59 | 5.41 | <0.0001 |
| PM2.5 | 0.0029 | 0.0026 | 59 | 1.13 | 0.2637 | |
| Gender | Female | 0.9548 | 0.3167 | 59 | 3.01 | 0.0038 |
| VCAM-1 2 | ||||||
| Season | Summer | 0.3154 | 0.0908 | 59 | 3.47 | 0.0010 |
| ICAM-1 2 | ||||||
| Season | Summer | 0.3679 | 0.0831 | 70 | 4.43 | <0.0001 |
| IL-1β 2 | ||||||
| Season | Summer | 0.3829 | 0.1124 | 67 | 3.41 | 0.0011 |
| PM2.5 | −0.0018 | 0.0007 | 67 | −2.45 | 0.0171 | |
| IL-2 2 | ||||||
| Season | Summer | 0.8941 | 0.06547 | 72 | 13.59 | <0.0001 |
| Gender | Female | 0.5940 | 0.1334 | 72 | 4.45 | <0.0001 |
| IL-4 | ||||||
| Season | Summer | 0.1812 | 0.0154 | 66 | 11.77 | <0.0001 |
| Gender | Female | 0.2077 | 0.01931 | 66 | 10.76 | <0.0001 |
| IL-6 2 | ||||||
| Season | Summer | 0.9458 | 0.08211 | 71 | 11.52 | <0.0001 |
| Gender | Female | 0.6877 | 0.1463 | 71 | 4.70 | <0.0001 |
| IL-8 2 | ||||||
| Season | Summer | 1.1651 | 0.1411 | 59 | 8.26 | <0.0001 |
| IL-10 | ||||||
| Season | Summer | 1.2331 | 0.1417 | 57 | 8.71 | <0.0001 |
| PM2.5 | 0.0028 | 0.0009 | 57 | 3.07 | 0.0033 | |
| BC | −2 × 10−5 | 4.44 × 10−6 | 57 | −3.55 | 0.0008 | |
| Mask | No | −0.1199 | 0.0477 | 57 | −2.52 | 0.0147 |
| Gender | Female | 1.1191 | 0.2337 | 57 | 4.79 | <0.0001 |
| IL-12 | ||||||
| Season | Summer | 0.6483 | 0.1048 | 62 | 6.19 | <0.0001 |
| PM2.5 | −0.0021 | 8.56 × 10−4 | 62 | −2.42 | 0.0184 | |
| Mask | No | −0.2006 | 0.0506 | 62 | −3.97 | 0.0002 |
| Gender | Female | 0.8294 | 0.1720 | 62 | 4.82 | <0.0001 |
| IL-13 | ||||||
| Season | Summer | 0.6104 | 0.1014 | 58 | 6.02 | <0.0001 |
| PM2.5 | −0.0019 | 0.0005 | 58 | −4.08 | <0.0001 | |
| Mask | No | −0.0963 | 0.0297 | 58 | −3.24 | 0.0020 |
| Gender | Female | 0.9112 | 0.0576 | 58 | 15.81 | <0.0001 |
| IFN-γ 3 | ||||||
| PM2.5 | −0.0044 | 0.0014 | 68 | −3.22 | 0.0019 | |
| Gender | Female | 0.9682 | 0.2299 | 68 | 4.21 | <0.0001 |
| TNF-α | ||||||
| Season | Summer | 1.4738 | 0.2158 | 65 | 6.83 | <0.0001 |
| BC | −5.00 × 10−5 | 1.60 × 10−5 | 65 | −3.23 | 0.0020 | |
| Smoker | No | −0.7800 | 0.3269 | 65 | −2.39 | 0.0200 |
© 2019 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Shakya, K.M.; Peltier, R.E.; Zhang, Y.; Pandey, B.D. Roadside Exposure and Inflammation Biomarkers among a Cohort of Traffic Police in Kathmandu, Nepal. Int. J. Environ. Res. Public Health 2019, 16, 377. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph16030377
Shakya KM, Peltier RE, Zhang Y, Pandey BD. Roadside Exposure and Inflammation Biomarkers among a Cohort of Traffic Police in Kathmandu, Nepal. International Journal of Environmental Research and Public Health. 2019; 16(3):377. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph16030377
Chicago/Turabian StyleShakya, Kabindra M., Richard E. Peltier, Yimin Zhang, and Basu D. Pandey. 2019. "Roadside Exposure and Inflammation Biomarkers among a Cohort of Traffic Police in Kathmandu, Nepal" International Journal of Environmental Research and Public Health 16, no. 3: 377. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph16030377