3D Printed Temporary Veneer Restoring Autotransplanted Teeth in Children: Design and Concept Validation Ex Vivo

 , and
, and 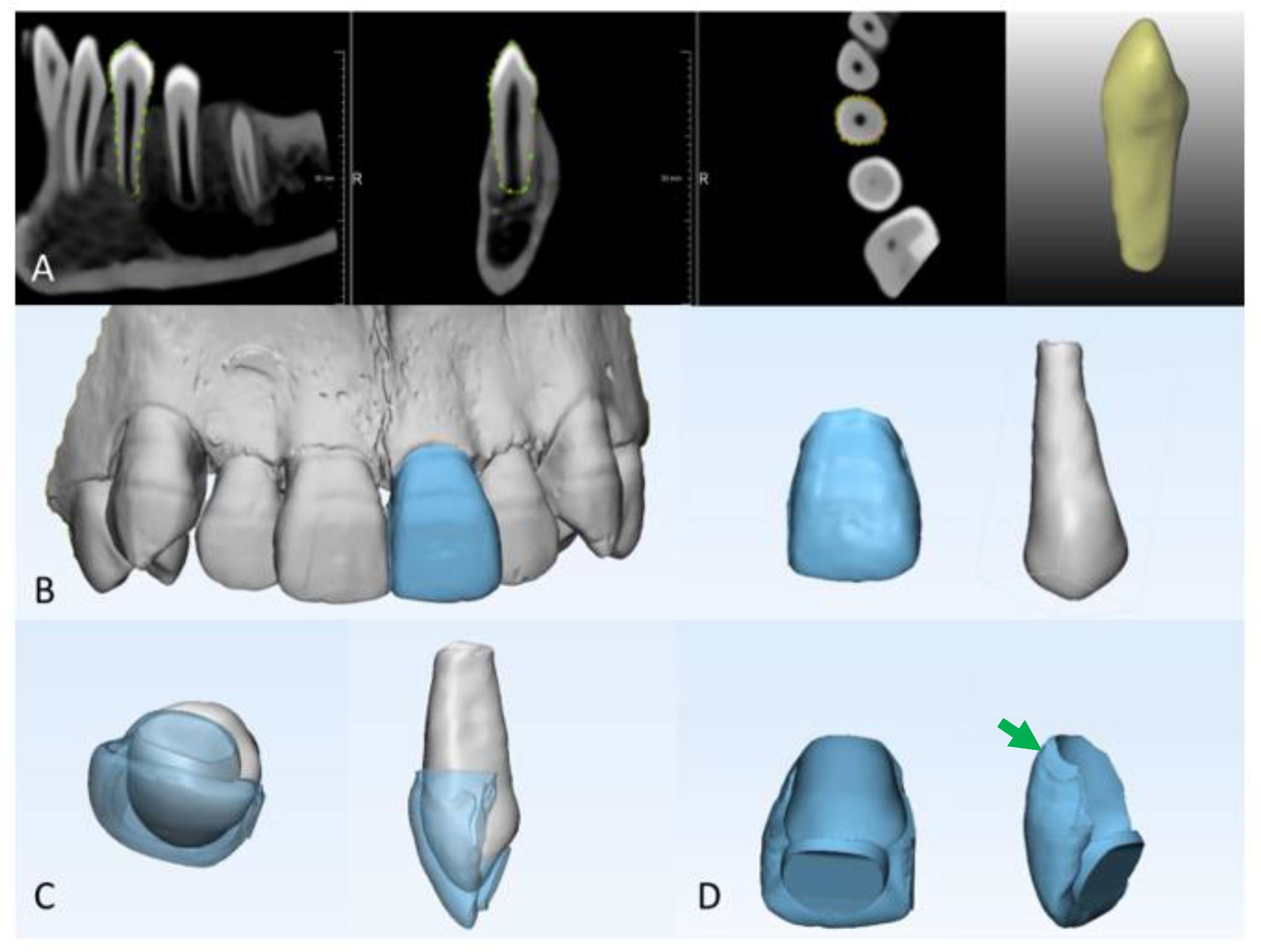{kind=link}
{kind=link}
{kind=link}
Abstract
:1. Introduction
2. Materials and Methods
2.1. Image Acquisition
2.2. Segmentation Protocol
2.3. Designing of Temporary Veneers
2.4. Three-Dimensional Printing of Temporary Veneers
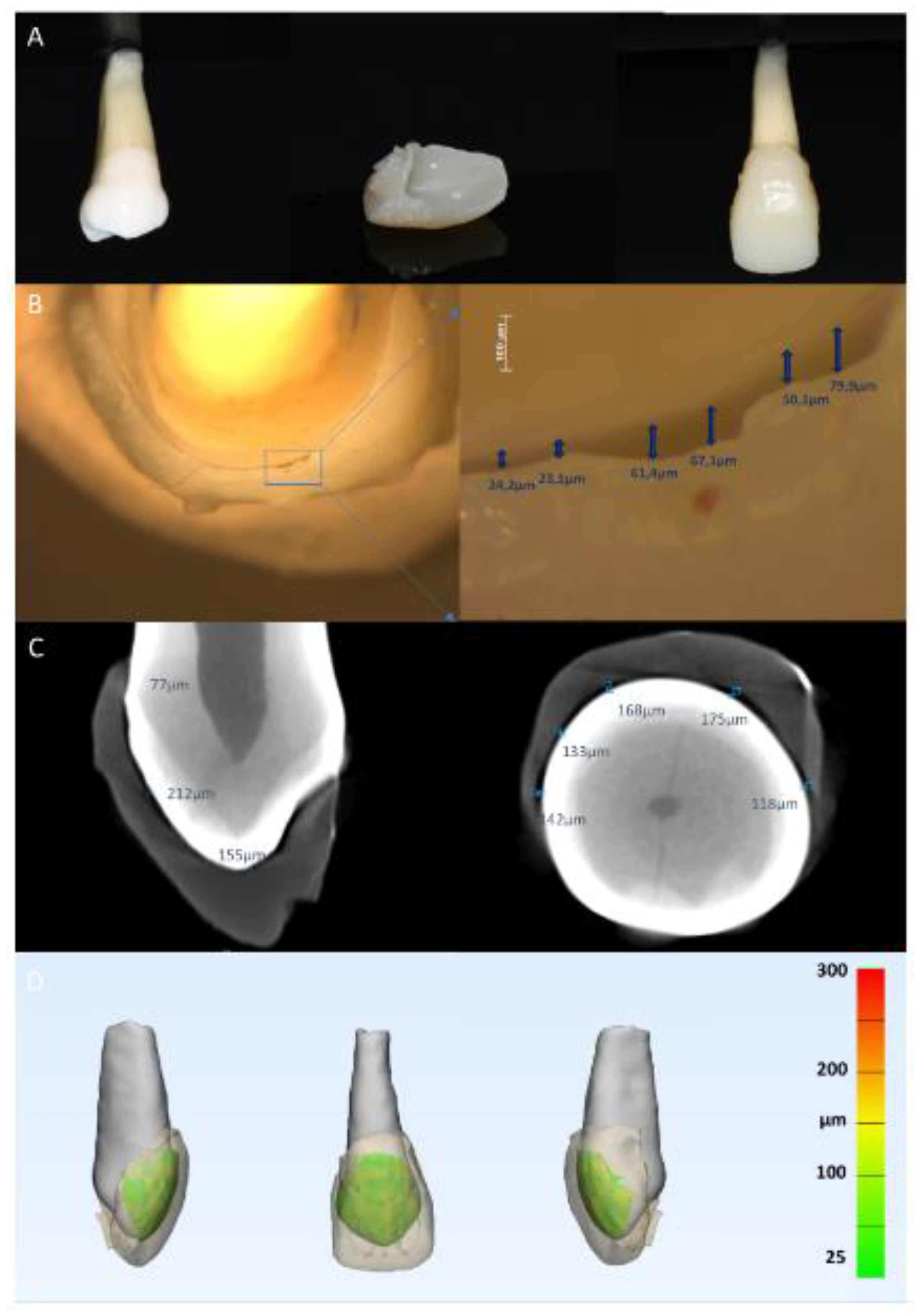
2.5. Evaluation of Veneer Seating and Marginal Adaptation
2.6. Evaluation of Internal Adaptation Using Micro-Computed Tomographic Imaging
Image Acquisition
2.7. Segmentation Protocol, 3D Reconstruction, and Quantitative Analysis of Gap Thickness
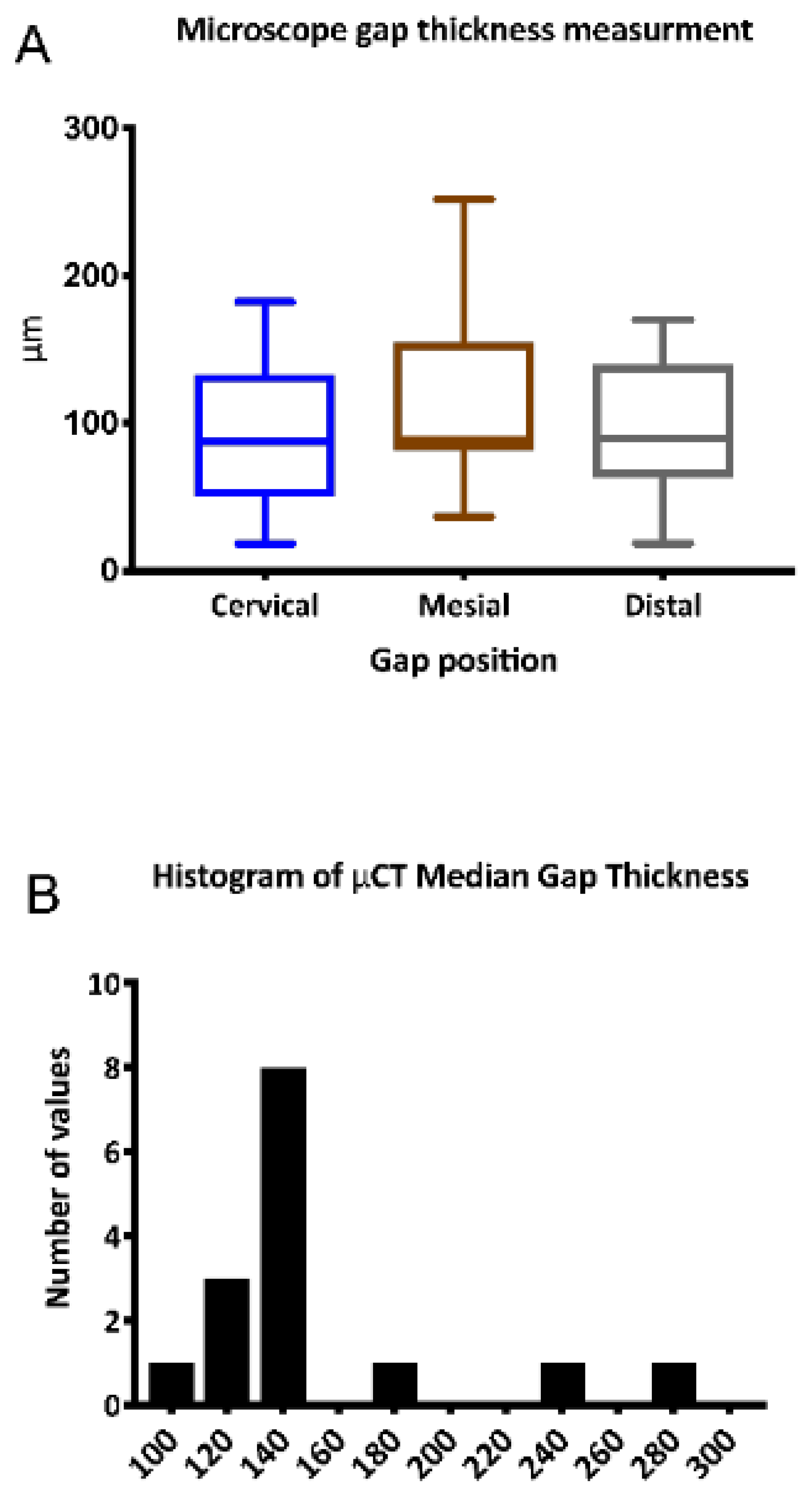
3. Statistical Analysis
4. Results
5. Discussion
6. Conclusions
Author Contributions
Funding
Conflicts of Interest
References
- Duret, F.; Preston, J.D. CAD/CAM imaging in dentistry. Curr. Opin. Dent. 1991, 1, 150–154. [Google Scholar] [PubMed]
- Miyazaki, T.; Hotta, Y.; Kunii, J.; Kuriyama, S.; Tamaki, Y. A review of dental CAD/CAM: Current status and future perspectives from 20 years of experience. Dent. Mater. J. 2009, 28, 44–56. [Google Scholar] [CrossRef] [PubMed]
- Torabi, K.; Farjood, E.; Hamedani, S. Rapid prototyping technologies and their applications in prosthodontics, a Review of Literature. J. Dent. (Shiraz) 2015, 16, 1–9. [Google Scholar]
- Van Assche, N.; Vercruyssen, M.; Coucke, W.; Teughels, W.; Jacobs, R.; Quirynen, M. Accuracy of computer-aided implant placement. Clin. Oral. Implants. Res. 2012, 23, 112–123. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Vercruyssen, M.; Coucke, W.; Naert, I.; Jacobs, R.; Teughels, W.; Quirynen, M. Depth and lateral deviations in guided implant surgery: An RCT comparing guided surgery with mental navigation or the use of a pilot-drill template. Clin. Oral. Implants Res. 2015, 26, 1315–1320. [Google Scholar] [CrossRef] [PubMed]
- Vercruyssen, M.; van de Wiele, G.; Teughels, W.; Naert, I.; Jacobs, R.; Quirynen, M. Implant- and patient-centred outcomes of guided surgery, a 1-year follow-up: An RCT comparing guided surgery with conventional implant placement. J. Clin. Periodontol. 2014, 41, 1154–1160. [Google Scholar] [CrossRef] [PubMed]
- Colombo, M.; Mangano, C.; Mijiritsky, E.; Krebs, M.; Hauschild, U.; Fortin, T. Clinical applications and effectiveness of guided implant surgery: A critical review based on randomized controlled trials. BMC Oral Health 2017, 17, 150. [Google Scholar] [CrossRef] [PubMed]
- Krastl, G.; Zehnder, M.S.; Connert, T.; Weiger, R.; Kuhl, S. Guided Endodontics: A novel treatment approach for teeth with pulp canal calcification and apical pathology. Dent. Traumatol. 2016, 32, 240–246. [Google Scholar] [CrossRef] [PubMed]
- Torres, A.; Shaheen, E.; Lambrechts, P.; Politis, C.; Jacobs, R. Microguided Endodontics: A case report of a maxillary lateral incisor with pulp canal obliteration and apical periodontitis. Int. Endod. J. 2018. [Google Scholar] [CrossRef] [PubMed]
- Lee, S.J.; Jung, I.Y.; Lee, C.Y.; Choi, S.Y.; Kum, K.Y. Clinical application of computer-aided rapid prototyping for tooth transplantation. Dent. Traumatol. 2001, 17, 114–119. [Google Scholar] [CrossRef]
- Shahbazian, M.; Jacobs, R.; Wyatt, J.; Denys, D.; Lambrichts, I.; Vinckier, F.; Willems, G. Validation of the cone beam computed tomography-based stereolithographic surgical guide aiding autotransplantation of teeth: Clinical case-control study. Oral Surg. Oral Med. Oral Pathol. Oral Radiol. 2013, 115, 667–675. [Google Scholar] [CrossRef] [PubMed]
- Shahbazian, M.; Jacobs, R.; Wyatt, J.; Willems, G.; Pattijn, V.; Dhoore, E.; Van Lierde, C.; Vinckier, F. Accuracy and surgical feasibility of a CBCT-based stereolithographic surgical guide aiding autotransplantation of teeth: In vitro validation. J. Oral Rehabil. 2010, 37, 854–859. [Google Scholar] [CrossRef] [PubMed]
- Kim, S.Y.; Shin, Y.S.; Jung, H.D.; Hwang, C.J.; Baik, H.S.; Cha, J.Y. Precision and trueness of dental models manufactured with different 3-dimensional printing techniques. Am. J. Orthod. Dentofacial Orthop. 2018, 153, 144–153. [Google Scholar] [CrossRef] [PubMed]
- Dawood, A.; Marti Marti, B.; Sauret-Jackson, V.; Darwood, A. 3D printing in dentistry. Br. Dent. J. 2015, 219, 521–529. [Google Scholar] [CrossRef] [PubMed]
- Shaheen, E.; Alhelwani, A.; Van De Casteele, E.; Politis, C.; Jacobs, R. Evaluation of dimensional changes of 3D printed models after sterilization: A pilot study. Open Dent. J. 2018, 12, 72–79. [Google Scholar] [CrossRef] [PubMed]
- Shaheen, E.; Coopman, R.; Jacobs, R.; Politis, C. Optimized 3D virtually planned intermediate splints for bimaxillary orthognathic surgery: A clinical validation study in 20 patients. J. Craniomaxillofac. Surg. 2018, 46, 1441–1447. [Google Scholar] [CrossRef] [PubMed]
- Shaheen, E.; Sun, Y.; Jacobs, R.; Politis, C. Three-dimensional printed final occlusal splint for orthognathic surgery: Design and validation. Int. J. Oral Maxillofac. Surg. 2017, 46, 67–71. [Google Scholar] [CrossRef] [PubMed]
- EzEldeen, M.; Stratis, A.; Coucke, W.; Codari, M.; Politis, C.; Jacobs, R. As low dose as sufficient quality: Optimization of cone-beam computed tomographic scanning protocol for tooth autotransplantation planning and follow-up in children. J. Endod. 2017, 43, 210–217. [Google Scholar] [CrossRef] [PubMed]
- Loubele, M.; Bogaerts, R.; Van Dijck, E.; Pauwels, R.; Vanheusden, S.; Suetens, P.; Marchal, G.; Sanderink, G.; Jacobs, R. Comparison between effective radiation dose of CBCT and MSCT scanners for dentomaxillofacial applications. Eur. J. Radiol. 2009, 71, 461–468. [Google Scholar] [CrossRef]
- Albdour, E.A.; Shaheen, E.; Vranckx, M.; Mangano, F.G.; Politis, C.; Jacobs, R. A novel in vivo method to evaluate trueness of digital impressions. BMC Oral Health 2018, 18, 117. [Google Scholar] [CrossRef]
- Mangano, F.; Gandolfi, A.; Luongo, G.; Logozzo, S. Intraoral scanners in dentistry: A review of the current literature. BMC Oral Health 2017, 17, 149. [Google Scholar] [CrossRef] [PubMed]
- Stanley, M.; Paz, A.G.; Miguel, I.; Coachman, C. Fully digital workflow, integrating dental scan, smile design and CAD-CAM: Case report. BMC Oral Health 2018, 18, 134. [Google Scholar] [CrossRef] [PubMed]
- Joda, T.; Zarone, F.; Ferrari, M. The complete digital workflow in fixed prosthodontics: A systematic review. BMC Oral Health 2017, 17, 124. [Google Scholar] [CrossRef] [PubMed]
- Kim, G.B.; Lee, S.; Kim, H.; Yang, D.H.; Kim, Y.H.; Kyung, Y.S.; Kim, C.S.; Choi, S.H.; Kim, B.J.; Ha, H.; et al. Three-dimensional printing: Basic principles and applications in medicine and radiology. Korean J. Radiol. 2016, 17, 182–197. [Google Scholar] [CrossRef] [PubMed]
- Czochrowska, E.M.; Stenvik, A.; Album, B.; Zachrisson, B.U. Autotransplantation of premolars to replace maxillary incisors: A comparison with natural incisors. Am. J. Orthod. Dentofacial Orthop. 2000, 118, 592–600. [Google Scholar] [CrossRef] [PubMed]
- Day, P.; Duggal, M. Autotransplantation for failing and missing anterior teeth. Pediatr. Dent. 2008, 30, 286–287. [Google Scholar] [PubMed]
- Paulsen, H.U.; Andreasen, J.O.; Schwartz, O. Tooth loss treatment in the anterior region: Autotransplantation of premolars and cryopreservation. World J. Orthod. 2006, 7, 27–34. [Google Scholar] [CrossRef] [PubMed]
- Akhlef, Y.; Schwartz, O.; Andreasen, J.O.; Jensen, S.S. Autotransplantation of teeth to the anterior maxilla: A systematic review of survival and success, aesthetic presentation and patient-reported outcome. Dent. Traumatol. 2018, 34, 20–27. [Google Scholar] [CrossRef] [PubMed]
- Rohof, E.C.M.; Kerdijk, W.; Jansma, J.; Livas, C.; Ren, Y. Autotransplantation of teeth with incomplete root formation: A systematic review and meta-analysis. Clin. Oral Investig. 2018, 22, 1613–1624. [Google Scholar] [CrossRef]
- Sharma, A.B.; Vargervik, K. Using implants for the growing child. J. Calif. Dent. Assoc. 2006, 34, 719–724. [Google Scholar]
- Kanavakis, G.; Ludwig, B.; Rosa, M.; Zachrisson, B.; Hourfar, J. Clinical outcomes of cases with missing lateral incisors treated with the ‘T’-Mesialslider. J. Orthod. 2014, 41, S33–S38. [Google Scholar] [CrossRef] [PubMed]
- Becker, K.; Wilmes, B.; Grandjean, C.; Vasudavan, S.; Drescher, D. Skeletally anchored mesialization of molars using digitized casts and two surface-matching approaches: Analysis of treatment effects. J. Orofac. Orthop. 2018, 79, 11–18. [Google Scholar] [CrossRef] [PubMed]
- Andreasen, J.O.; Paulsen, H.U.; Yu, Z.; Schwartz, O. A long-term study of 370 autotransplanted premolars. Part III. Periodontal healing subsequent to transplantation. Eur. J. Orthod. 1990, 12, 25–37. [Google Scholar] [CrossRef] [PubMed]
- Kallu, R.; Vinckier, F.; Politis, C.; Mwalili, S.; Willems, G. Tooth transplantations: A descriptive retrospective study. Int. J. Oral Maxillofac. Surg. 2005, 34, 745–755. [Google Scholar] [CrossRef] [PubMed]
- Denys, D.; Shahbazian, M.; Jacobs, R.; Laenen, A.; Wyatt, J.; Vinckier, F.; Willems, G. Importance of root development in autotransplantations: A retrospective study of 137 teeth with a follow-up period varying from 1 week to 14 years. Eur. J. Orthod. 2013, 35, 680–688. [Google Scholar] [CrossRef] [PubMed]
- Day, P.F.; Kindelan, S.A.; Spencer, J.R.; Kindelan, J.D.; Duggal, M.S. Dental trauma: Part 2. Managing poor prognosis anterior teeth-treatment options for the subsequent space in a growing patient. J. Orthod. 2008, 35, 143–155. [Google Scholar] [CrossRef] [PubMed]
- Andreasen, J.O.; Paulsen, H.U.; Yu, Z.; Bayer, T.; Schwartz, O. A long-term study of 370 autotransplanted premolars. Part II. Tooth survival and pulp healing subsequent to transplantation. Eur. J. Orthod. 1990, 12, 14–24. [Google Scholar] [CrossRef]
- Czochrowska, E.M.; Stenvik, A.; Zachrisson, B.U. The esthetic outcome of autotransplanted premolars replacing maxillary incisors. Dent. Traumatol. 2002, 18, 237–245. [Google Scholar] [CrossRef]
- EzEldeen, M.; Van Gorp, G.; Van Dessel, J.; Vandermeulen, D.; Jacobs, R. 3-dimensional analysis of regenerative endodontic treatment outcome. J. Endod. 2015, 41, 317–324. [Google Scholar] [CrossRef]
- Barrett, W.A.; Mortensen, E.N. Interactive live-wire boundary extraction. Med.Image Anal. 1997, 1, 331–341. [Google Scholar] [CrossRef] [Green Version]
- Suetens, P. Fundamentals of Medical Imaging, 2nd ed.; Cambridge University Press: New York, NY, USA, 2009; p. 264. [Google Scholar]
- Heckel, F.; Konrad, O.; Hahn, H.K.; Peitgen, H.-O. Interactive 3D medical image segmentation with energy-minimizing implicit functions. Comput. Gr. 2011, 35, 275–287. [Google Scholar] [Green Version]
- Zachrisson, B.U.; Stenvik, A.; Haanæs, H.R. Management of missing maxillary anterior teeth with emphasis on autotransplantation. Am. J. Orthod. Dentofacial Orthop. 2004, 126, 284–288. [Google Scholar] [CrossRef]
- Bader, J.D.; Rozier, R.G.; McFall, W.T.; Ramsey, D.L. Effect of crown margins on periodontal conditions in regularly attending patients. J. Prosthet. Dent. 1991, 65, 75–79. [Google Scholar] [CrossRef]
- Bergenholtz, G.; Cox, C.F.; Loesche, W.J.; Syed, S.A. Bacterial leakage around dental restorations: Its effect on the dental pulp. J. Oral Pathol. 1982, 11, 439–450. [Google Scholar] [CrossRef] [PubMed]
- Fransson, B.; Oilo, G.; Gjeitanger, R. The fit of metal-ceramic crowns, a clinical study. Dent. Mater. 1985, 1, 197–199. [Google Scholar] [CrossRef]
- McLean, J.W.; von Fraunhofer, J.A. The estimation of cement film thickness by an in vivo technique. Br. Dent. J. 1971, 131, 107–111. [Google Scholar] [CrossRef] [PubMed]
- Borba, M.; Cesar, P.F.; Griggs, J.A.; Della Bona, Á. Adaptation of all-ceramic fixed partial dentures. Dent. Mater. 2011, 27, 1119–1126. [Google Scholar] [CrossRef] [Green Version]
- Pelekanos, S.; Koumanou, M.; Koutayas, S.O.; Zinelis, S.; Eliades, G. Micro-CT evaluation of the marginal fit of different In-Ceram alumina copings. Eur. J. Esthet. Dent. 2009, 4, 278–292. [Google Scholar]
- Harasani, M.H.; Isidor, F.; Kaaber, S. Marginal fit of porcelain and indirect composite laminate veneers under in vitro conditions. Scand. J. Dent. Res. 1991, 99, 262–268. [Google Scholar] [CrossRef]
- Tetsuya, A.; Ryunosuke, K.; Takashi, O.; Masayoshi, F. Adaptation of laminate veneer restorations fabricated with the CEREC 3 system. J. Adhes. Dent. 2006, 24, 179–184. [Google Scholar]
- Yuce, M.; Ulusoy, M.; Turk, A.G. Comparison of marginal and internal adaptation of heat-pressed and CAD/CAM porcelain laminate veneers and a 2-Year follow-up. J. Prosthodont 2017. [Google Scholar] [CrossRef] [PubMed]



© 2019 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Al-Rimawi, A.; EzEldeen, M.; Schneider, D.; Politis, C.; Jacobs, R. 3D Printed Temporary Veneer Restoring Autotransplanted Teeth in Children: Design and Concept Validation Ex Vivo. Int. J. Environ. Res. Public Health 2019, 16, 496. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph16030496
Al-Rimawi A, EzEldeen M, Schneider D, Politis C, Jacobs R. 3D Printed Temporary Veneer Restoring Autotransplanted Teeth in Children: Design and Concept Validation Ex Vivo. International Journal of Environmental Research and Public Health. 2019; 16(3):496. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph16030496
Chicago/Turabian StyleAl-Rimawi, Ali, Mostafa EzEldeen, Danilo Schneider, Constantinus Politis, and Reinhilde Jacobs. 2019. "3D Printed Temporary Veneer Restoring Autotransplanted Teeth in Children: Design and Concept Validation Ex Vivo" International Journal of Environmental Research and Public Health 16, no. 3: 496. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph16030496