Chen-Style Tai Chi for Individuals (Aged 50 Years Old or Above) with Chronic Non-Specific Low Back Pain: A Randomized Controlled Trial

 , , and
, , and
Abstract
:1. Introduction
2. Method
2.1. Experimental Design
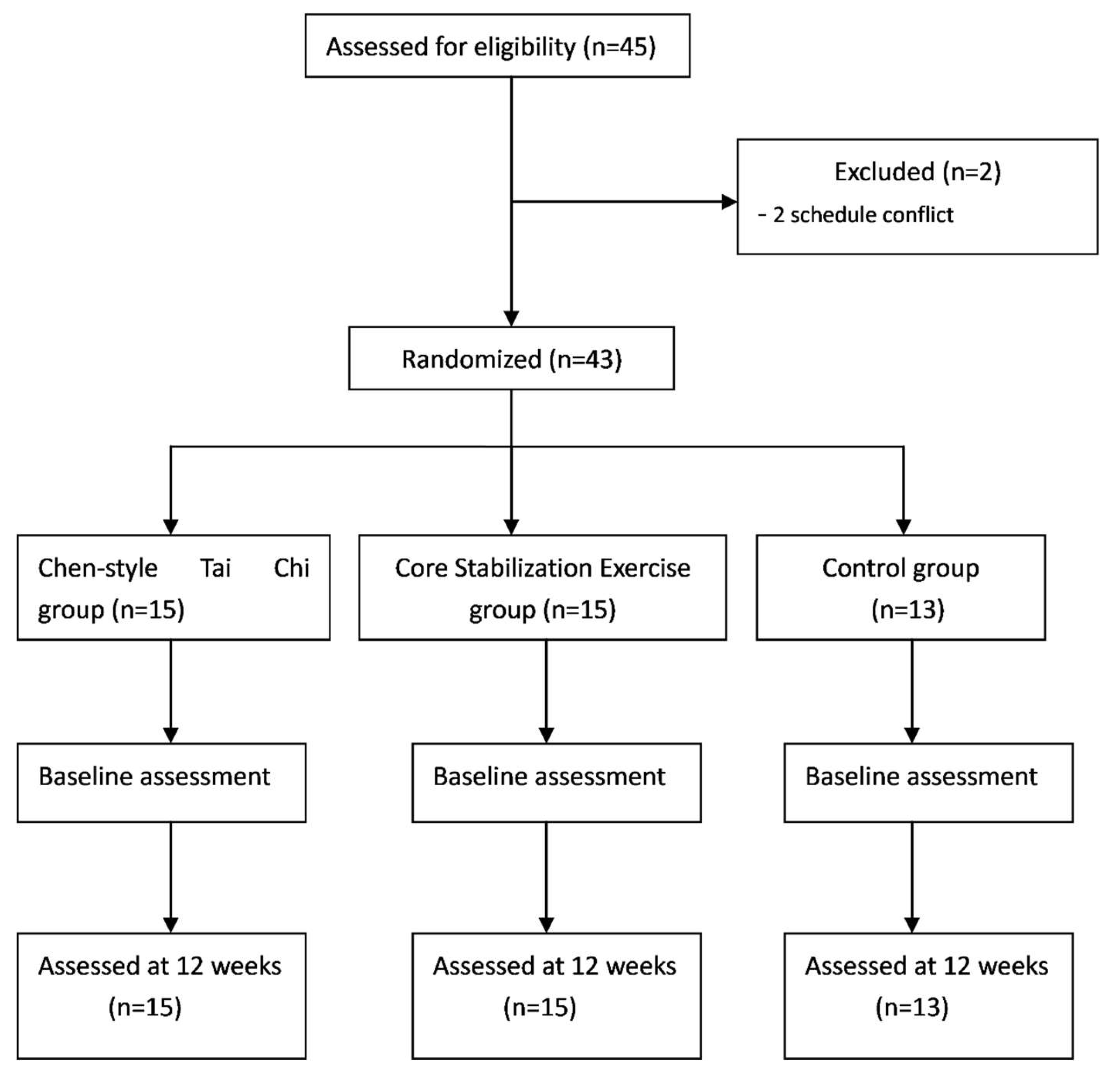
2.2. Participant Recruitment and Randomization
2.3. Intervention Protocol
2.3.1. Chen-Style Tai Chi
2.3.2. Core Stabilization Exercise and Non-Active Control
2.4. Outcome Measures
2.4.1. Visual Analogue Scale (VAS) Test
2.4.2. Active Position Sense Test
2.5. Statistical Analysis
3. Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- Deyo, R.A.; Weinstein, J.N.N. Low back pain. Engl. J. Med. 2001, 344, 363–370. [Google Scholar] [CrossRef] [PubMed]
- Hoy, D.; Bain, C.; Williams, G.; March, L.; Brooks, P.; Blyth, F.; Woolf, A.; Vos, T.; Buchbinder, R. A systematic review of the global prevalence of low back pain. Arthritis Rheum. 2012, 64, 2028–2037. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Murray, C.J.L.; Atkinson, C.; Bhalla, K.; Birbeck, G.; Burstein, R.; Chou, D.; Baddour, L.M.; Bartels, D.H.; Benjamin, E.J.; Bhalla, K.; et al. The state of US health, 1990–2010: Burden of diseases, injuries, and risk factors. JAMA 2013, 310, 591–608. [Google Scholar] [CrossRef] [PubMed]
- Dieleman, J.L.; Baral, R.; Birger, M.; Bui, A.L.; Bulchis, A.; Chapin, A.; Hamavid, H.; Horst, C.; Johnson, E.K.; Joseph, J.; et al. US Spending on Personal Health Care and Public Health, 1996–2013. JAMA 2016, 316, 2627–2646. [Google Scholar] [CrossRef] [PubMed]
- Chenot, J.F.; Greitemann, B.; Kladny, B.; Petzke, F.; Pfingsten, M.; Schorr, S.G. Non-Specific Low Back Pain. Dtsch. Arztebl. Int. 2017, 114, 883–890. [Google Scholar] [CrossRef] [PubMed]
- Koes, B.W.; van Tulder, M.; Lin, C.W.; Macedo, L.G.; McAuley, J.; Maher, C. An updated overview of clinical guidelines for the management of non-specific low back pain in primary care. Eur. Spine J. 2010, 19, 2075–2094. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Maher, C.; Underwood, M.; Buchbinder, R. Non-specific low back pain. The Lancet 2017, 389, 736–747. [Google Scholar] [CrossRef] [Green Version]
- Chou, R.; Turner, J.A.; Devine, E.B.; Hansen, R.N.; Sullivan, S.D.; Blazina, I.; Dana, T.; Bougatsos, C.; Deyo, R.A. The effectiveness and risks for long-term opioid therapy for chronic pain: A systematic review for National Institutes of Health Pathways to prevention workshop. Ann. Intern. Med. 2015, 162, 276–286. [Google Scholar] [CrossRef]
- Liu, J.; Zhao, W.; Yuan, Y.H. Effects of Tai Chi on the event-related potential of patients with chronic non-specific low back pain. Chin. J. Sports Med. 2018, 37, 826–832. [Google Scholar]
- Searle, A.; Spink, M.; Ho, A.; Chuter, V. Exercise interventions for the treatment of chronic low back pain: A systematic review and meta-analysis of randomized controlled trial. Clin. Rehabil. 2015, 29, 1155–1167. [Google Scholar] [CrossRef]
- Yue, Y.-S.; Wang, X.-D.; Xie, B.; Li, Z.-H.; Chen, B.-L.; Wang, X.-Q. Sling Exercise for Chronic Low Back Pain: A Systematic Review and Meta-Analysis. PLoS ONE 2014, 9, e99307. [Google Scholar] [CrossRef] [PubMed]
- Slade, S.C.; Keating, J.L. Trunk-strengthening exercises for chronic low back pain: A systematic review. J. Manip. Physiol. Ther. 2006, 29, 163–173. [Google Scholar] [CrossRef] [PubMed]
- Wang, X.; Zheng, J.; Yu, Z.; Bi, X.; Lou, S.; Liu, J. A meta-analysis of core stability exercise versus general exercise for chronic low back pain. PLoS ONE 2012, 7, e52082. [Google Scholar] [CrossRef] [PubMed]
- Akhtar, M.; Karimi, H.; Gilani, S. Effectiveness of core stabilization exercises and routine exercise therapy in management of pain in chronic nonspecific low back pain: A randomized controlled clinical trial. Pak. J. Med. Sci. 2017, 33, 1002–1006. [Google Scholar] [CrossRef] [PubMed]
- Zou, L.; Wang, H.; Xiao, Z.; Fang, Q.; Zhang, M.; Li, T. Tai chi for health benefits in patients with multiple sclerosis: A systematic review. PLoS ONE 2017, 12, e0170212. [Google Scholar] [CrossRef] [PubMed]
- Zou, L.; Yeung, A.; Quan, X.; Boyden, S.D.; Wang, H. A Systematic Review and Meta-Analysis of Mindfulness-Based (Baduanjin) Exercise for Alleviating Musculoskeletal Pain and Improving Sleep Quality in People with Chronic Diseases. Int. J. Environ. Res. Public Health 2018, 15, 206. [Google Scholar] [CrossRef] [PubMed]
- Zou, L.; Wang, C.; Tian, Z.; Wang, H.; Shu, Y. Effect of Yang-Style Tai Chi on Gait Parameters and Musculoskeletal Flexibility in Healthy Chinese Older Women. Sports 2017, 5, 52. [Google Scholar] [CrossRef] [PubMed]
- Zou, L.; Sasaki, J.; Zeng, N.; Wang, C.; Sun, L. A systematic review with meta-analysis of mindful exercises on rehabilitative outcomes among poststroke patients. Arch. Phys. Med. Rehabil. 2018, 99, 2355–2364. [Google Scholar] [CrossRef]
- Zou, L.; Yeung, A.; Li, C.; Wei, G.-X.; Chen, K.W.; Kinser, P.A.; Chan, J.S.M.; Ren, Z. Effects of Meditative Movements on Major Depressive Disorder: A Systematic Review and Meta-Analysis of Randomized Controlled Trials. J. Clin. Med. 2018, 7, 195. [Google Scholar] [CrossRef]
- Zou, L.; Sasaki, J.E.; Wei, G.-X.; Huang, T.; Yeung, A.S.; Neto, O.B.; Chen, K.W.; Hui, S.-C. Effects of Mind–Body Exercises (Tai Chi/Yoga) on Heart Rate Variability Parameters and Perceived Stress: A Systematic Review with Meta-Analysis of Randomized Controlled Trials. J. Clin. Med. 2018, 7, 404. [Google Scholar] [CrossRef]
- Liu, J.; Wang, X.Q.; Zheng, J.J. Effects of Tai Chi versus Proprioception Exercise Program on Neuromuscular Function of the Ankle in Elderly People: A Randomized Controlled Trial. Evid. Based Complement. Altern. Med. 2012, 2012, 265486. [Google Scholar] [CrossRef] [PubMed]
- Zou, L.; Wang, C.; Wang, H. Effect of a long-term modified Tai Chi-based intervention in attenuating bone mineral density in postmenopausal women in southeast China: Study protocol for a randomized controlled trial. Clin. Trial Degener. Dis. 2017, 2, 46–52. [Google Scholar]
- Zou, L.; Wang, C.; Chen, K.; Shu, Y.; Chen, X.; Luo, L.; Zhao, X. The Effect of Taichi Practice on Attenuating Bone Mineral Density Loss: A Systematic Review and Meta-Analysis of Randomized Controlled Trials. Int. J. Environ. Res. Public Health 2017, 14, 1000. [Google Scholar] [CrossRef] [PubMed]
- Liu, J.; Xie, H.; Liu, M.; Wang, Z.; Zou, L.; Yeung, A.S.; Hui, S.-C.; Yang, Q. The Effects of Tai Chi on Heart Rate Variability in Older Chinese Individuals with Depression. Int. J. Environ. Res. Public Health 2018, 15, 2771. [Google Scholar] [CrossRef] [PubMed]
- Lou, L.; Zou, L.; Fang, Q.; Wang, H.; Liu, Y.; Tian, Z.; Han, Y. Effect of Taichi softball on function-related outcomes in older adults: A randomized control trial. Evid.-Based Complement. Altern. Med. 2017, 2017, 4585424. [Google Scholar] [CrossRef] [PubMed]
- Zou, L.; Yeung, A.; Zeng, N.; Wang, C.; Sun, L.; Thomas, G.; Wang, H. Effects of mind-body exercises for mood and functional capabilities in post-stroke patients: An analytical review of randomized controlled trials. Int. J. Environ. Res. Public Health 2018, 15, 721. [Google Scholar] [CrossRef] [PubMed]
- Wang, X.Q.; Huang, L.Y.; Liu, Y.; Li, J.X.; Wu, X.; Li, H.P.; Wang, L. Effects of tai chi program on neuromuscular function for patients with knee osteoarthritis: Study protocol for a randomized controlled trial. Trials 2013, 14, 375. [Google Scholar] [CrossRef]
- Hall, A.; Maher, C.; Lam, P.; Ferreira, M.; Latimer, J. Tai chi exercise for treatment of pain and disability in people with persistent low back pain: A randomized controlled trial. Arthr. Care Res. 2011, 63, 1576–1583. [Google Scholar] [CrossRef] [Green Version]
- Wu, W.; Aikeremujiang, M.; Chen, C.; Liu, W.; Sun, L. Effectiveness of Tai Chi Practice for Non-Specific Chronic Low Back Pain on Retired Athletes: A Randomized Controlled Study. J. Musculoskelet. Pain 2013, 21, 37–45. [Google Scholar]
- Zou, L.; Han, J.; Li, C.; Yeung, A.; Hui, S.; Tsang, W.; Ren, Z.; Wang, L. Effects of Tai Chi on lower limb proprioception in adults aged over 55: A systematic review and meta-analysis. Arch. Phys. Med. Rehabil. 2018. [Google Scholar] [CrossRef]
- Wang, X.; Zheng, J.; Bi, X.; Liu, J. Effect of Core Stability Training on patients with chronic low back Pain. HealthMed 2012, 6, 754–759. [Google Scholar]
- Hawker, G.A.; Mian, S.; Kendzerska, T.; French, M. Measures of adult pain: Visual Analog Scale for ain (VAS Pain), Numeric Rating Scale for Pain (NRS Pain), McGill Pain Questionnaire (MPQ), Short-Form McGill Pain Questionnaire (SF-MPQ), Chronic Pain Grade Scale (CPGS), Short Form-36 Bodily Pain Scale (SF-36 BPS), and Measure of Intermittent and Constant Osteoarthritis Pain (ICOAP). Arthr. Care Res. 2017, 63, 240–252. [Google Scholar] [CrossRef]
- Lauche, R.; Stumpe, C.; Fehr, J.; Cramer, H.; Cheng, Y.W.; Wayne, P.M.; Rampp, T.; Langhorst, J.; Dobos, G. The effects of Tai Chi and neck exercises in the treatment of chronic nonspecific neck pain: A randomized controlled trial. J. Pain 2016, 17, 1013–1027. [Google Scholar] [CrossRef] [PubMed]
- Teut, M.; Knilli, J.; Daus, D.; Roll, S.; Witt, C.M. Qigong or yoga versus no intervention in older adults with chronic low back pain-A randomized controlled trial. J. Pain 2016, 17, 796–805. [Google Scholar] [CrossRef] [PubMed]
- Shipton, E.A. Physical therapy approaches in the treatment of low back pain. Pain Ther. 2018, 7, 127–137. [Google Scholar] [CrossRef] [PubMed]
- Chang, S.; Zhou, J.; Hong, Y.; Sun, W.; Cong, Y.; Qin, M.; Lian, J.; Yao, J.; Li, W. Effects of 24-week Tai Chi exercise on the knee and ankle proprioception of older women. Res. Sports Med. 2016, 24, 84–93. [Google Scholar] [CrossRef] [PubMed]
- Wang, R.; Li, Y. 16-week Tai Chi Chuan for improving low-limb proprioception in old adults: A randomized controlled trial. J. Henan Norm. Univ. 2016, 44, 172–177. [Google Scholar]
- Chen, E.W.; Fu, A.S.; Chan, K.M.; Tsang, W.W. The effects of Tai Chi on the balance control of elderly persons with visual impairment: A randomised clinical trial. Age Ageing 2012, 41, 254–259. [Google Scholar] [CrossRef]


{kind=link}
| Variable | Tai Chi (n = 15) | Core Stabilization (n = 15) | Control (n = 13) |
|---|---|---|---|
| Female (%) | 73.3 | 73.3 | 76.9 |
| Age(y) | 58.13 ± 5.38 | 58.4 ± 5.08 | 60.67 ± 2.58 |
| Body weight | 58.93 ± 9.93 | 63.33 ± 9.08 | 63.47 ± 12.05 |
| Height | 159.53 ± 7.24 | 162.53 ± 8.21 | 159.00 ± 7.17 |
| Parameters | Tai Chi | Core Stabilization | Control | |||
|---|---|---|---|---|---|---|
| Pre (t = 0) | Post (t = 12 W) | Pre (t = 0) | Post (t = 12 W) | Pre (t = 0) | Post (t = 12 W) | |
| VAS | 5.67 ± 0.81 | 3.47 ± 0.99 ** | 5.67 ± 0.72 | 4.27 ± 0.79 △△ | 5.85 ± 0.89 | 5.85 ± 0.8 |
| JPS of ankle inversion | 9.72 ± 4.88 | 2.35 ± 2.05 | 10.24 ± 7.58 | 6.18 ± 4.46 | 7.37 ± 4.94 | 5.98 ± 3.47 |
| JPS of ankle eversion | 5.14 ± 3.17 | 2.72 ± 1.88 | 6.08 ± 3.39 | 4.59 ± 2.53 | 4.21 ± 3.68 | 6.64 ± 4.51 |
| JPS of knee flexion | 9.98 ± 6.49 | 0.81 ± 0.5 | 9.44 ± 8.69 | 6.46 ± 5.72 | 7.12 ± 2.76 | 5.86 ± 4.51 |
© 2019 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Liu, J.; Yeung, A.; Xiao, T.; Tian, X.; Kong, Z.; Zou, L.; Wang, X. Chen-Style Tai Chi for Individuals (Aged 50 Years Old or Above) with Chronic Non-Specific Low Back Pain: A Randomized Controlled Trial. Int. J. Environ. Res. Public Health 2019, 16, 517. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph16030517
Liu J, Yeung A, Xiao T, Tian X, Kong Z, Zou L, Wang X. Chen-Style Tai Chi for Individuals (Aged 50 Years Old or Above) with Chronic Non-Specific Low Back Pain: A Randomized Controlled Trial. International Journal of Environmental Research and Public Health. 2019; 16(3):517. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph16030517
Chicago/Turabian StyleLiu, Jing, Albert Yeung, Tao Xiao, Xiaopei Tian, Zhaowei Kong, Liye Zou, and Xueqiang Wang. 2019. "Chen-Style Tai Chi for Individuals (Aged 50 Years Old or Above) with Chronic Non-Specific Low Back Pain: A Randomized Controlled Trial" International Journal of Environmental Research and Public Health 16, no. 3: 517. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph16030517