Risk Factors Associated with Dengue Virus Infection in Guangdong Province: A Community-Based Case-Control Study

Abstract
:1. Introduction
2. Materials and Methods
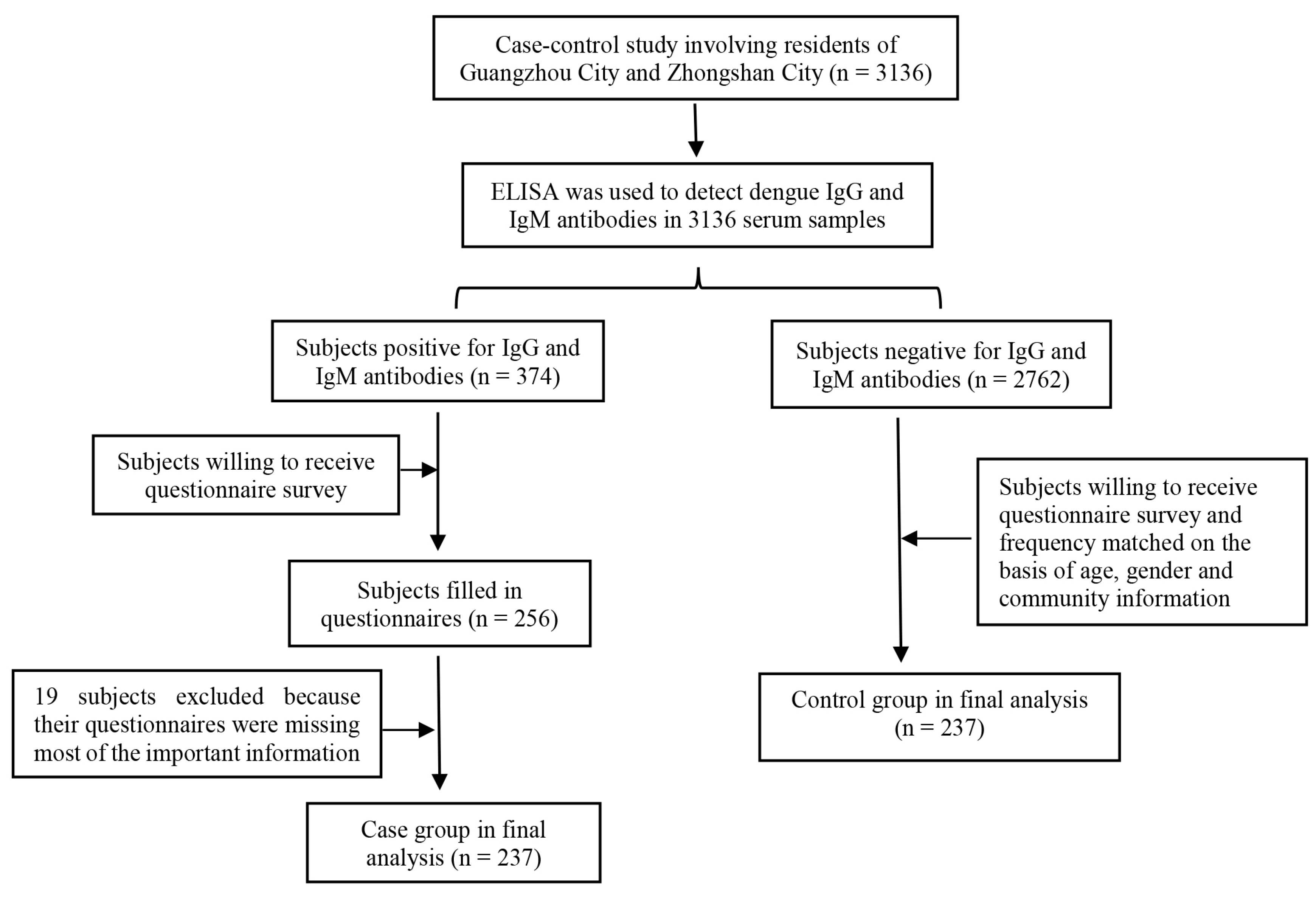
2.1. Community Selection and Study Design
2.2. Ethical Statement
2.3. Enzyme Immunoassay Test
2.4. Case Definition and Control Selection
2.5. Data Collection and Analysis
3. Results
3.1. General Demographic Characteristics of the Samples
3.2. Univariate Analysis
3.3. Multivariate Analysis
4. Discussion
5. Limitations
6. Conclusions
Supplementary Materials
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- World Health Organization. Epidemiology. Available online: https://www.who.int/denguecontrol/epidemiology/en/ (accessed on 14 May 2018).
- Gubler, D.J.; Meltzer, M. Impact of dengue/dengue hemorrhagic fever on the developing world. Adv. Virus Res. 1999, 53, 35–70. [Google Scholar] [CrossRef] [PubMed]
- Wen, J.; Liang, F. An etiological and serological study on Dengue epidemic in Guangdong Province. Zhonghua Shi Yan He Lin Chuang Bing Du Xue Za Zhi 1998, 12, 165–168. [Google Scholar] [PubMed]
- Liu, C.; Liu, Q.; Lin, H.; Xin, B.; Nie, J. Spatial analysis of dengue fever in Guangdong Province, China, 2001–2006. Asia Pac. J. Public Health 2014, 26, 58. [Google Scholar] [CrossRef] [PubMed]
- Zhang, Y.; Wang, T.; Liu, K.; Xia, Y.; Lu, Y.; Jing, Q.; Yang, Z.; Hu, W.; Lu, J. Developing a Time Series Predictive Model for Dengue in Zhongshan, China Based on Weather and Guangzhou Dengue Surveillance Data. PLoS Neglect. Trop. Dis. 2016, 10, e0004473. [Google Scholar] [CrossRef] [PubMed]
- Guo, Y.; Song, Z.; Luo, L.; Wang, Q.; Zhou, G.; Yang, D.; Zhong, D.; Zheng, X. Molecular evidence for new sympatric cryptic species of Aedes albopictus (Diptera: Culicidae) in China: A new threat from Aedes albopictus subgroup? Parasite Vectors 2018, 11, 228. [Google Scholar] [CrossRef] [PubMed]
- Jia, D.S.; Tan, W.L.; Wang, C.J.; Han, Z.J.; Lu, N.H.; Zheng, J. Aedes-borne diseases prevention and control. Chin. J. Hyg. Insect. Equip. 2017, 23, 1–7. [Google Scholar]
- Thein, T.L.; Leo, Y.S.; Fisher, D.A.; Low, J.G.; Oh, H.M.L.; Gan, V.C.; Wong, J.G.X.; Lye, D.C. Risk Factors for Fatality among Confirmed Adult Dengue Inpatients in Singapore: A Matched Case-Control Study. PLoS ONE 2013, 8, e81060. [Google Scholar] [CrossRef]
- Pang, J.; Thein, T.L.; Leo, Y.S.; Lye, D.C. Early clinical and laboratory risk factors of intensive care unit requirement during 2004–2008 dengue epidemics in Singapore: A matched case-control study. BMC Infect. Dis. 2014, 14, 649. [Google Scholar] [CrossRef]
- Moraes, G.H.; De, F.D.E.; Duarte, E.C. Determinants of mortality from severe dengue in Brazil: A population-based case-control study. Am. J. Trop. Med. Hyg. 2013, 88, 670–676. [Google Scholar] [CrossRef]
- Branco, M.R.; Luna, E.J.; Braga Júnior, L.L.; Oliveira, R.V.B.; Rios, L.T.M.; Silva, M.S.; Medeiros, M.N.L.; Silva, G.F.; Nina, F.C.A.F.; Lima, T.J.; et al. Risk factors associated with death in Brazilian children with severe dengue: A case-control study. Clinics 2014, 69, 55–60. [Google Scholar] [CrossRef]
- Van Benthem, B.H.; Khantikul, N.; Panart, K.; Kessels, P.J.; Somboon, p.; Oskam, L. Knowledge and use of prevention measures related to dengue in northern Thailand. Trop. Med. Int. Health 2010, 7, 993–1000. [Google Scholar] [CrossRef]
- Phuanukoonnon, S.; Mueller, I.; Bryan, J.H. Effectiveness of dengue control practices in household water containers in Northeast Thailand. Trop. Med. Int. Health 2005, 10, 755–763. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Luo, L.; Liang, H.Y.; Hu, Y.S.; Liu, W.J.; Wang, Y.L.; Jing, Q.L.; Zheng, X.L.; Yang, Z.C. Epidemiological, virological, and entomological characteristics of dengue from 1978 to 2009 in Guangzhou, China. J. Vector Ecol. 2012, 37, 230–240. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Gu, H.; Leung, K.K.; Jing, Q.; Zhang, W.; Yang, Z.; Lu, J.; Hao, Y.; Zhang, D. Meteorological Factors for Dengue Fever Control and Prevention in South China. Int. J. Environ. Res. Public Health 2016, 13, 867. [Google Scholar] [CrossRef] [PubMed]
- Fan, J.C.; Lin, H.L.; Wu, H.X.; Wang, J.; Yang, S.R.; Liu, Q.Y. Spatial and temporal distribution characteristics of dengue fever in Guangdong province, China during 2006-2011. Chin. J. Vector Biol. Control 2013, 24, 389–391. [Google Scholar] [CrossRef]
- Wang, T.; Wang, M.; Shu, B.; Chen, X.; Luo, L.; Wang, J.; Cen, Y.; Anderson, B.D.; Merrill, M.M.; Mwrrill, H.R.; et al. Evaluation of Inapparent Dengue Infections During an Outbreak in Southern China. PLoS Neglect. Trop. Dis. 2015, 9, e0003677. [Google Scholar] [CrossRef] [PubMed]
- Zhang, J.H.; Yuan, J.; Wang, T. Direct cost of dengue hospitalization in Zhongshan, China: Associations with demographics, virus types and hospital accreditation. PLoS Neglect. Trop. Dis. 2017, 11, e0005784. [Google Scholar] [CrossRef]
- Liu, J.; Deng, Y.; Jing, Q.; Chen, X.; Du, Z.; Liang, T.; Yang, Z.; Zhang, D.; Hao, Y. Dengue Infection Spectrum in Guangzhou: A Cross-Sectional Seroepidemiology Study among Community Residents between 2013 and 2015. Int. J. Environ. Res. Public Health 2018, 15, 1227. [Google Scholar] [CrossRef]
- Rezza, G. Aedes albopictus and the reemergence of Dengue. BMC Public Health 2012, 12, 72. [Google Scholar] [CrossRef]
- Gubler, D.J. Epidemic dengue/dengue hemorrhagic fever as a public health, social and economic problem in the 21st century. Trends Microbiol. 2002, 10, 100–103. [Google Scholar] [CrossRef]
- Jing, Q.L.; Li, Y.L.; Chen, Z.Q. Spatial pattern and driving factors of dengue virus-4 epidemics in Guangzhou. J. Trop. Med. 2016, 16, 244–248. [Google Scholar]
- Velascosalas, Z.I.; Sierra, G.M.; Guzmán, D.M.; Zambrano, J.; Vivas, D.; Comach, G.; Wilschut, J.C.; Tami, A. Dengue Seroprevalence and Risk Factors for Past and Recent Viral Transmission in Venezuela: A Comprehensive Community-Based Study. Am. J. Trop. Med. Hyg. 2014, 91, 1039–1048. [Google Scholar] [CrossRef] [Green Version]
- Wang, H.S.; Huang, X.N.; Jiang, J.X.; Ma, Y.Y.; An, L.; Liu, X.C. Sleep location in Chinese children aged 0~5 years old. Chin. J. Child Health Care 2008, 16, 420–422. [Google Scholar]
- Shen, C.; Luo, L.; Li, L.; Jing, Q.L.; Ou, C.Q.; Yang, Z.C.; Chen, X.G. The Impacts of Mosquito Density and Meteorological Factors on Dengue Fever Epidemics in Guangzhou, China, 2006–2014: A Time-series Analysis. Biomed. Environ. Sci. 2015, 28, 321–329. [Google Scholar] [CrossRef]
- Wu, P.C.; Lay, J.G.; Guo, H.R.; Lin, C.Y.; Lung, S.C.; Su, H.J. Higher temperature and urbanization affect the spatial patterns of dengue fever transmission in subtropical Taiwan. Sci. Total Environ. 2009, 407, 2224–2233. [Google Scholar] [CrossRef]
- Paul, R.; Sarah, L.; Michel, B.; Biggerstaff, B.; Singer, D.; Tiwari, T.; Baber, L.; Amador, M.; Thirion, J.; Hayes, J.; et al. Texas Lifestyle Limits Transmission of Dengue Virus. Emerg. Infect. Dis. 2003, 9, 86–89. [Google Scholar] [CrossRef]
- Gong, D.F.; Zhou, H.N. Progress in Dengue fever important vector Aedes albopictus in China. Chin. J. Vector Biol. Control 2009, 20, 607–610. [Google Scholar]
- Crepeau, T.N.; Healy, S.P.; Bartlett-Healy, K.; Unlu, I.; Farajollahi, A.; Fonseca, D.M. Effects of Biogents Sentinel Trap Field Placement on Capture Rates of Adult Asian Tiger Mosquitoes, Aedes albopictus. PLoS ONE 2013, 8, e60524. [Google Scholar] [CrossRef]
- Vanwambeke, S.O.; van Benthem, B.H.; Khantikul, N.; Burghoorn-Maas, C.; Panart, K.; Oskam, L.; Lambin, E.F.; Somboon, P. Multi-level analyses of spatial and temporal determinants for dengue infection. Int. J. Health Geogr. 2006, 5, 5. [Google Scholar] [CrossRef]
- Kenneson, A.; Beltrán-Ayala, E.; Borbor-Cordova, M.J.; Polhemus, M.E.; Ryan, S.J.; Endy, T.P.; Stewart-Ibarra, A.M. Social-ecological factors and preventive actions decrease the risk of dengue infection at the household-level: Results from a prospective dengue surveillance study in Machala, Ecuador. PLoS Neglect. Trop. Dis. 2017, 11, e0006150. [Google Scholar] [CrossRef]
- Tsuzuki, A.; Thiem, V.D.; Suzuki, M.; Yanai, H.; Matsubayashi, T.; Yoshida, L.-M.; Tho, L.H.; Minh, T.T.; Anh, D.D.; Kilgore, P.E.; et al. Can Daytime Use of Bed Nets Not Treated with Insecticide Reduce the Risk of Dengue Hemorrhagic Fever Among Children in Vietnam? Am. J. Trop. Med. Hyg. 2010, 82, 1157–1159. [Google Scholar] [CrossRef] [Green Version]
- Loroñopino, M.A.; Machainwilliams, C.; Gomezcarro, S.; Loroño-Pino, M.A.; García-Rejón, J.E.; Machain-Williams, C.; Gomez-Carro, S.; Nuñez-Ayala, G.; Nájera-Vázquez, M.R.; Losoya, A.; et al. Towards a Casa Segura: A Consumer Product Study of the Effect of Insecticide-Treated Curtains on Aedes aegypti and Dengue Virus Infections in the Home. Am. J. Trop. Med. Hyg. 2013, 89, 385–397. [Google Scholar] [CrossRef] [Green Version]
- Trpis, M.; Mcclelland, G.A.; Gillett, J.D.; Teesdale, C.; Rao, T.R. Diel periodicity in the landing of Aedes aegypti on man. Bull. World Health Organ. 1973, 48, 623–629. [Google Scholar]
- Lenhart, A.; Orelus, N.; Maskill, R.; Alexander, N.; Streit, T.; McCall, P.J. Insecticide-treated bednets to control dengue vectors: Preliminary evidence from a controlled trial in Haiti. Trop. Med. Int. Health 2008, 13, 56–67. [Google Scholar] [CrossRef]
- Andersson, N.; Navaaguilera, E.; Arosteguí, J.; Morales-Perez, A.; Suazo-Laguna, H.; Legorreta-Soberanis, J.; Hernandez-Alvarez, C.; Fernandez-Salas, I.; Paredes-Solís, S.; Balmaseda, A.; et al. Evidence based community mobilization for dengue prevention in Nicaragua and Mexico (Camino Verde, the Green Way): Cluster randomized controlled trial. BMJ 2015, 351, h3267. [Google Scholar] [CrossRef]
- Pan, H.F.; YE, X.X.; Chen, C.J.; Zhao, J.Y.; Lin, Z.Y. Study on prevention and control of Dengue from perspective of public health. Chin. J. Public Health Manag. 2015, 31, 775–776. [Google Scholar] [CrossRef]
- Guzman, M.G.; Harris, E. Dengue. Lancet 2015, 385, 453–465. [Google Scholar] [CrossRef]


{kind=link}
| Demographic Characteristics a | Cases (n/%) (n = 237) | Controls (n/%) (n = 237) | p-Value |
|---|---|---|---|
| Age (years) ≤15 16–30 31–50 51–65 ≥66 | 15 (6.33) 13 (5.49) 33 (13.92) 43 (18.14) 133 (56.12) | 15 (6.33) 13 (5.49) 33 (13.92) 43 (18.14) 133 (56.12) | - |
| Gender | - | ||
| Male | 89 (37.55) | 89 (37.55) | |
| Female | 148 (62.45) | 148 (62.45) | |
| Residential status | 0.149 | ||
| Permanent residents | 225 (94.94) | 231 (97.47) | |
| Floating population b | 12 (5.06) | 6 (2.53) | |
| Number of residents per household | 0.394 | ||
| 1 | 27 (11.39) | 17 (7.17) | |
| 2–3 | 126 (53.16) | 125 (52.75) | |
| 4–5 | 75 (31.65) | 84 (35.44) | |
| ≥6 | 9 (3.80) | 11 (4.64) | |
| Monthly per capita family income (¥) c | 0.317 | ||
| <2000 | 50 (21.10) | 36 (15.19) | |
| 2000–4999 | 145 (61.18) | 162 (68.35) | |
| 5000–7999 | 35 (14.77) | 31 (13.08) | |
| ≥8000 | 7 (2.95) | 8 (3.38) | |
| Blood type | 0.196 | ||
| A | 18 (7.59) | 14 (5.91) | |
| B | 15 (6.33) | 19 (8.02) | |
| O | 29 (12.24) | 46 (19.40) | |
| AB | 9 (3.80) | 6 (2.53) | |
| Unknown | 166 (70.04) | 152 (64.14) |
| Variables | Cases (n/%) (n = 237) | Controls (n/%) (n = 237) | OR (95% CI) | p-Value |
|---|---|---|---|---|
| Contact with patients with dengue fever | 0.655 | |||
| Yes | 3 (1.27) | 2 (0.84) | 1.51 (0.25–9.10) | |
| No | 234 (98.73) | 235 (99.16) | Reference | |
| Outbound tourism experience | 0.867 | |||
| Yes | 19 (8.02) | 20 (8.44) | Reference | |
| No | 218 (91.98) | 217 (91.56) | 1.06 (0.55–2.04) | |
| Outdoor activities in parks | 0.049 * | |||
| Yes | 200 (84.39) | 183 (77.22) | 1.60 (1.00–2.54) | |
| No | 37 (15.61) | 54 (22.78) | Reference | |
| Participation in outdoor sports | 0.009 * | |||
| Yes | 74 (31.22) | 49 (20.68) | 1.74 (1.15–2.64) | |
| No | 163 (68.78) | 188 (79.32) | Reference | |
| Domestic sewage disposal frequency | 0.655 | |||
| Daily | 125 (52.74) | 118 (49.79) | Reference | |
| 2 days | 25 (10.55) | 20 (8.44) | 1.18 (0.62–2.24) | |
| ≥3 days | 35 (14.77) | 42 (17.72) | 0.79 (0.47–1.32) | |
| No domestic sewage | 52 (21.94) | 57 (24.05) | 0.86 (0.55–1.35) | |
| Garbage disposal frequency | 0.311 | |||
| Daily | 223 (94.09) | 228 (96.20) | Reference | |
| 2 days | 11 (4.64) | 5 (2.11) | 2.25 (0.77–6.58) | |
| ≥3 days | 3 (1.69) | 4 (1.69) | 0.77 (0.17–3.47) | |
| Participation in community hygiene management interventions | 0.104 | |||
| Yes | 77 (32.49) | 94 (39.66) | Reference | |
| No | 160 (67.51) | 143 (60.34) | 1.37 (0.94–1.99) | |
| Location | 0.061 * | |||
| Rural | 15 (6.33) | 11 (4.64) | 0.34 (0.08–1.51) | |
| City | 210 (88.61) | 223 (94.09) | 0.24 (0.07–0.85) | |
| Urban–rural integration | 12 (5.06) | 3 (1.27) | Reference | |
| Housing building structure | 0.871 | |||
| Brick–wood structure | 2 (0.84) | 3 (1.27) | 0.67 (0.11–4.05) | |
| Brick–wood and concrete structure | 31 (13.08) | 29 (12.24) | 1.07 (0.63–1.85) | |
| Concrete structure | 204 (86.08) | 205 (86.49) | Reference | |
| Housing type | 0.040 * | |||
| Single-family apartment | 60 (25.32) | 39 (16.46) | Reference | |
| Commercial residential community | 173 (73.00) | 196 (82.70) | 0.57 (0.37–0.90) | |
| Villa | 4 (1.68) | 2 (0.84) | 1.30 (0.23–7.44) | |
| Housing age (year) | 0.919 | |||
| <10 | 23 (9.71) | 24 (10.13) | Reference | |
| 10–20 | 115 (48.52) | 116 (48.95) | 1.03 (0.54–1.94) | |
| 20–40 | 88 (37.13) | 89 (37.55) | 1.03 (0.54–1.96) | |
| >40 | 11 (4.64) | 8 (3.37) | 1.43 (0.49–4.21) | |
| Number of floors per residential structure | 0.096 * | |||
| 1–3 | 110 (46.41) | 87 (36.71) | Reference | |
| 4–9 | 103 (43.46) | 124 (52.32) | 0.66 (0.45–0.96) | |
| ≥10 | 24 (10.13) | 26 (10.97) | 0.73 (0.39–1.36) | |
| Average numbers of persons per room | <0.001 * | |||
| 1 | 91 (38.40) | 51 (21.52) | Reference | |
| 2 | 123 (51.90) | 160 (67.51) | 0.43 (0.28–0.65) | |
| ≥3 | 23 (9.70) | 26 (10.97) | 0.50 (0.26–0.96) | |
| Housing area (m2) | 0.235 | |||
| <50 | 63 (26.58) | 52 (21.9) | Reference | |
| 51–100 | 150 (63.29) | 169 (71.31) | 0.73 (0.18–1.12) | |
| 101–150 | 19 (8.02) | 11 (4.64) | 1.43 (0.62–3.26) | |
| >150 | 5 (2.11) | 5 (2.11) | 0.83 (0.23–3.01) | |
| Air-conditioner use | 0.013 * | |||
| Never | 26 (10.97) | 11 (4.64) | Reference | |
| Yes | 211(89.03) | 226 (95.36) | 0.40 (0.19–0.82) | |
| Indoor daylight quality | 0.032 * | |||
| Good | 215 (90.72) | 227 (95.78) | Reference | |
| Poor | 22 (9.28) | 10 (4.22) | 2.32 (1.08–5.02) | |
| Ventilation | 0.324 | |||
| Good | 221 (93.25) | 226 (95.36) | Reference | |
| Bad | 16 (6.75) | 11 (4.64) | 1.49(0.68–3.28) | |
| Keeping of pets | 0.800 | |||
| Yes | 38 (16.03) | 36 (15.19) | Reference | |
| No | 199 (83.97) | 201 (84.81) | 0.94 (0.57–1.54) | |
| Raising of poultry | 0.589 | |||
| Yes | 6 (2.53) | 8 (3.38) | 0.74 (0.25–2.18) | |
| No | 231 (97.47) | 229 (96.62) | Reference | |
| Breeding of aquatic plants | 0.578 | |||
| Yes | 54 (20.68) | 49 (20.68) | Reference | |
| No | 183 (77.22) | 188 (79.32) | 0.88 (0.57–1.37) | |
| Use of mosquito nets | 0.361 | |||
| Yes | 185 (78.06) | 193 (81.43) | Reference | |
| No | 52 (21.94) | 44 (18.57) | 1.23 (0.79–1.93) | |
| Use of mosquito repellent | 0.212 | |||
| Never | 122 (51.48) | 116 (48.95) | Reference | |
| Occasionally | 88 (37.13) | 103 (43.46) | 0.81 (0.56–1.19) | |
| Often | 27 (11.39) | 18 (7.59) | 1.43 (0.75–2.73) | |
| Use of electric mosquito-killing devices | 0.150 | |||
| Never | 152 (64.14) | 143 (60.34) | Reference | |
| Occasionally | 57 (24.05) | 74 (31.22) | 0.73 (0.48–1.10) | |
| Often | 28 (11.81) | 20 (8.44) | 1.32 (0.71–2.44) | |
| Use of camphor | 0.649 | |||
| Never | 177 (74.68) | 168 (70.89) | Reference | |
| Occasionally | 42 (17.72) | 48 (20.25) | 0.83 (0.52–1.32) | |
| Often | 18 (7.60) | 21 (8.86) | 0.81 (0.42–1.58) | |
| Existence of garbage collection sites within 200 m around housing | 0.681 | |||
| Yes | 32 (13.50) | 29 (12.24) | 1.12 (0.65–1.92) | |
| No | 205 (86.50) | 208 (87.76) | Reference | |
| Existence of junk yards within 200 m around housing | 0.570 | |||
| Yes | 1 (0.42) | 2 (0.84) | 0.50 (0.05–5.53) | |
| No | 236 (99.58) | 235 (99.16) | Reference | |
| Existence of ponds within 200 m around housing | 0.426 | |||
| Yes | 45 (18.99) | 52 (21.94) | 0.83 (0.53–1.30) | |
| No | 192 (81.01) | 185 (78.06) | Reference | |
| Existence of construction sites within 200 m around housing | 0.639 | |||
| Yes | 24 (10.13) | 21 (8.86) | 1.16 (0.63–2.15) | |
| No | 213 (89.87) | 216 (91.14) | Reference |
| Risk factors | Odds Ratio | 95% CI | p-Value |
|---|---|---|---|
| Participation in outdoor sports | 0.007 * | ||
| Yes | 1.80 | (1.17–2.78) | |
| No | Reference | ||
| Average numbers of occupants per room | <0.001 * | ||
| 1 | Reference | ||
| 2 | 0.43 | (0.28–0.65) | <0.001 * |
| ≥3 | 0.45 | (0.23–0.89) | 0.021 * |
| Air-conditioner use | 0.040 * | ||
| Never | Reference | ||
| Yes | 0.46 | (0.22–0.97) | |
| Indoor daylight quality | 0.043 * | ||
| Good | Reference | ||
| Poor | 2.27 | (1.03–5.03) |
© 2019 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Liu, J.; Tian, X.; Deng, Y.; Du, Z.; Liang, T.; Hao, Y.; Zhang, D. Risk Factors Associated with Dengue Virus Infection in Guangdong Province: A Community-Based Case-Control Study. Int. J. Environ. Res. Public Health 2019, 16, 617. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph16040617
Liu J, Tian X, Deng Y, Du Z, Liang T, Hao Y, Zhang D. Risk Factors Associated with Dengue Virus Infection in Guangdong Province: A Community-Based Case-Control Study. International Journal of Environmental Research and Public Health. 2019; 16(4):617. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph16040617
Chicago/Turabian StyleLiu, Jundi, Xiaolu Tian, Yu Deng, Zhicheng Du, Tianzhu Liang, Yuantao Hao, and Dingmei Zhang. 2019. "Risk Factors Associated with Dengue Virus Infection in Guangdong Province: A Community-Based Case-Control Study" International Journal of Environmental Research and Public Health 16, no. 4: 617. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph16040617