Propagating Change: Using RE-FRAME to Scale and Sustain A Community-Based Childhood Obesity Prevention Initiative

Abstract
:1. Introduction
- (1)
- Enabled effective scale-up of implementation in ‘new’ Live 5-2-1-0 partner communities;
- (2)
- Increased community capacity in new and existing communities to support and sustain Live 5-2-1-0 implementation.
2. Materials and Methods
2.1. The Knowledge Exchange Model—RE-FRAME
- Free, customizable resources (e.g., toolkits, posters, ‘how to’ guides, etc.) through the Live 5-2-1-0 Online Resource Map;
- Quarterly webinars, annual face-to-face summits, and training events to connect stakeholders within and between Live 5-2-1-0 communities to facilitate exchange of stakeholder experiential learning and adaptation of implementation processes, as well as provide coaching and training;
- Ongoing and ad hoc central support to various stakeholder groups for all aspects of Live 5-2-1-0 implementation and monitoring including: community engagement across multiple community sectors, coordination and alignment with regional and provincial initiatives, new resource development and/or adaptation of existing resources, implementation and evaluation of sector-specific projects (i.e., with private business owners or family physicians), analysis and reporting of community-specific process data, among others; and
- Via a two-way linking system (that has been previously described), linkages between the SCOPE team and community stakeholders so that ideas, solutions, tools, and best practice, as well as community priorities, contexts and strengths, can be shared [13].
2.2. Participating Communities
2.3. Data Collection and Analysis
- PTT: A proprietary online progress-tracking platform (username- and password-protected) that allows key community stakeholders to enter data about local partnership formation (e.g., partner organization, sector represented, stage of partnership) and resulting outcomes (e.g., actions implemented and Live 5-2-1-0 resources shared via the partnership).
- CCBT: A valid, reliable tool developed by PHAC that measures capacity in nine evidence-based community capacity domains (Table 2) using a Likert scale (1—Just started; 2—On the road; 3—Nearly there; 4—We’re there) [19]. A community’s capacity in each domain reflects the mean score received for the subset of related response items (2–4 per domain), where all scores are determined by community stakeholder consensus (e.g., at a monthly partnership meeting).
3. Results
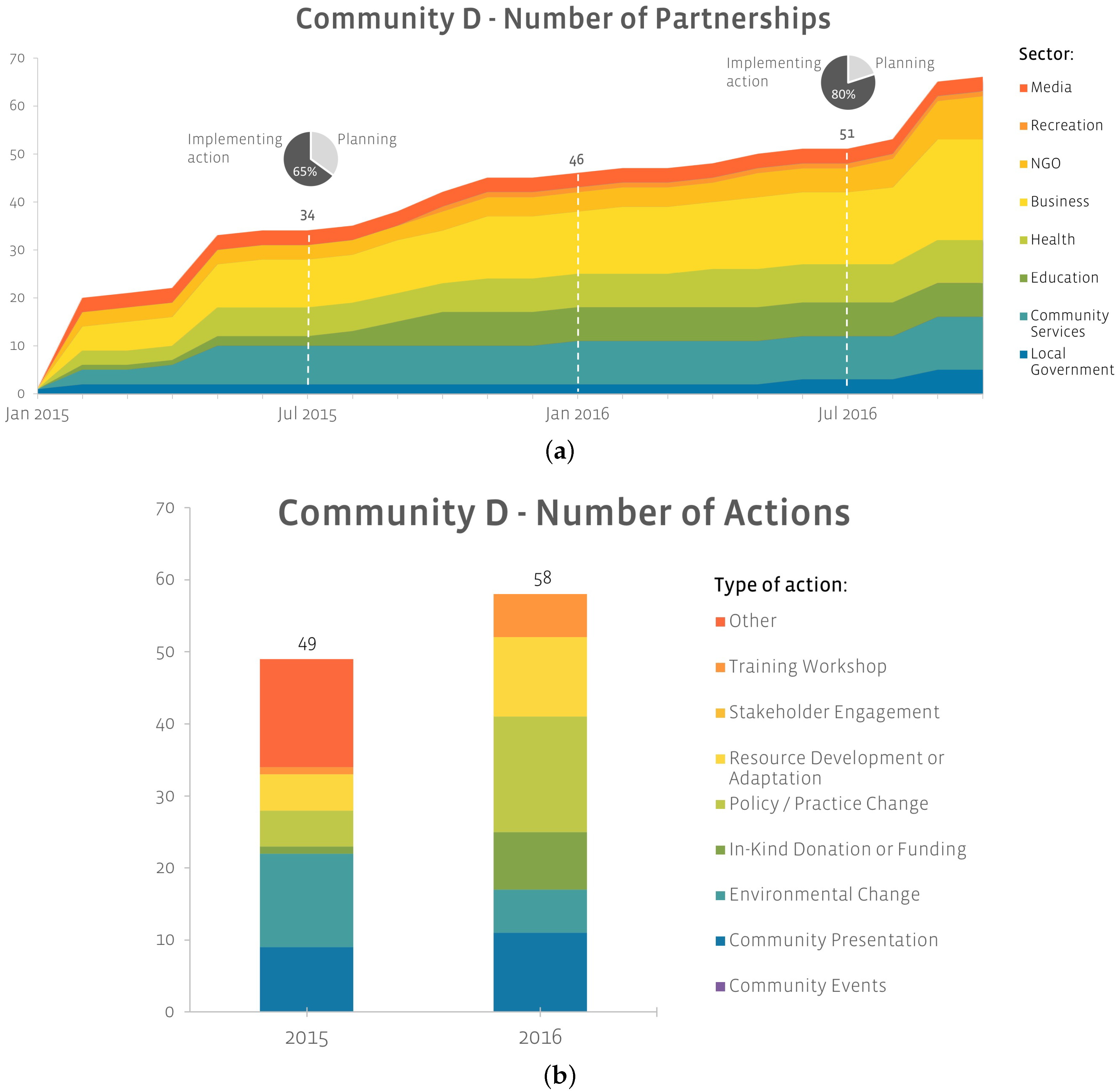
3.1. Multi-sectoral Partnerships Initiated and Sustained Multi-setting Action
- The library stopped serving juice and animal crackers at their pre-school aged story time and began serving fruits and veggies instead;
- The front desk staff at the local Medical Clinic started handing out Healthy Habit Questionnaires to all children or their parents/guardians for discussion with a care provider during primary care visits;
- Students were taken on a supermarket tour to explore healthy food choices, according to the Canada Food Guide and linked to the Live 5-2-1-0 message.
3.2. Community Capacity
3.2.1. Community Capacity Increased over Time
3.2.2. What Increases Community Capacity?
- “I think there just needs to be that shared vision and that shared belief in the message, that this is something that is important to each respective organization, and we think it’s important for the community, and that’s why we’re here.” (A1)
- “The [city’s] healthy communities committee had a strategic planning day…and decided on three priorities, one of which was childhood health and wellness. The committee decided that they would focus on the Live 5-2-1-0 messaging as a strategy to deal with childhood health and wellness.” (C1)
- “I think there needs to be a collaborative project. There needs to be something that gives us a reason to come together and something that’s tangible that we can work towards.” (A1)
- “…One learning we had from the Physician Toolkit, that we didn’t do enough physician engagement around developing the Toolkit. So, that can be improved. And that was big with regards to the Service Provider Toolkit—and through that there is more ownership on what is being created.” (B2)
- “I think a big thing for us again are the Playboxes. So when we are talking about shared responsibility, which I think increases the sustainability—to have all those different partners in the community to partner on the Playboxes, with either financial or in-kind contribution, and then they have their logos on the Playboxes which has made it that much more financial sustainable… I think the more partners you have engaged and visible in the community promoting Live 5-2-1-0, specifically the Playboxes, the more sustainable it becomes, because no one wants to see it taken away and their names attached to it.” (B2)
- “…they’re actively looking for those opportunities for the 5210 message to be further integrated and shared in our community…they’re the ‘ideas’ people… they’re actively looking for new places for this work to expand…” (A1, describing qualities of a champion)
- “I think the challenge is … just finding somebody who truly believes in the message so that you have a champion, because as it shows with the school district, if you have somebody that is a champion then you will get really far but if you don’t have that champion in place it just sort of stalls the whole progress.” (C1)
- “We have a couple new partners that have come on board, and I believe that the reason that those organizations have expressed an interest in becoming a partner is just we’ve had numerous face to face conversations, where we’re exchanging knowledge, where we’re building relationships, and I don’t think it can happen without that.” (A1)
- “…it has been very collaborative. It’s been pretty much across the sectors, with the media, business partners, or the health and wellness folks…And I think our approach on the way we went about it was good, starting with the inner circle to working its way out. I think that it gave the messaging some integrity and leveraging.” (D2)
- “… time is often the barrier but I think just trying to jump on board and create partnerships so that it’s really not a lot of additional work. Say for example, with the story time in the park, it really was no additional work because the story time in the park was already going on and so all I needed to do was give them the [Live 5-2-1-0] tips and they stuck them in the books that they were handing out so it wasn’t any additional work for partners and I think that’s one of the big things. Create these partnerships and just trying to climb on board with things that are already going on so that it’s not really that much additional work and then once you get those easy wins then looking at the harder stuff that maybe does take a bit more time and effort.” (C1)
- “…getting into the consciousness, getting out there, spreading the messaging, and that just leads to more uptake as we go. People are hearing more of the message, they are getting excited about it, they want to share it with their students. And I think that is the strength of their message that is really valuable. Just spreading it out into the community helps with the sustainability. It is a good, simple, strong messaging. I think it’s this kind of stuff that leads to sustainability for sure.” (D2)
- “I think because the message has been in the community long enough, that people know that it’s here to stay, that is not some sort of an aside that the city is going through. So, it’s easier to get organizations on board with distributing materials or allowing us to come in and do presentations.” (A2)
- “I think again because the message is so well established, it’s really easy for people to say yes to it. They do not have to wonder if it’s a good message, is there going to be any blow-back from parents or the community if we start to support this.” (A2)
- “We keep on having those moments, where we see the success of it. We interviewed someone last week and they were really excited about how we had healthy food and beverage messaging. And we say we’re 5-2-1-0 for after school child care and they’re like ‘I think that’s so great you know’. So lots of these moments that make it really worthwhile for us I guess.” (C2)
- “For us, we have these awesome moments with it. … It’s just we kept having comments where our people were like ‘there’s no way kids will eat fruits or vegetables, there’s no way they’re going to have any interest in working in the community garden’. And it’s really funny to see from a year ago, where they didn’t think they would eat it and they didn’t think they would participate and now they’re like ‘they were so excited for that!’ and ‘they’ve been eating so many raspberries all summer!’ or whatever.” (C2)
- “I think for us the big thing is training with staff, so any new staff hired, it’s part of their orientation. It’s in the rec department, to be honest, in part of their training to learn what the 5-2-1-0 program is and what it stands for.” (C2)
- “…the health and wellness community has been integral in pushing the messaging out. They have adopted it amongst their own practices. Many of our practitioners, which is great in terms of sustainability. A number of them have taken it and embraced it within their own practices. Thinking of the [partner name] and [partner name]. Many of them have taken it under their own umbrellas, their own messaging, which is nice to see.” (D2)
- “I think with sustainability, what I think is some of the changes that [local coordinator name] has been mentioning with regards to the food and beverage policy. It sounds like the initial hurdle was a bit challenging, but once the initial changes have been implemented that is huge in making sure that the community is meeting the Live 5-2-1-0 around the recreation facilities.” (C2)
4. Discussion
- (i)
- a common approach and agenda (i.e., Live 5-2-1-0) that all sectors of a community could support and that facilitated cross-sectoral collaborative projects (i.e., playboxes).
- (ii)
- community champions who sought and advocated for opportunities to integrate the initiative into the community’s make-up, sustaining momentum, building credibility and buy-in, and cultivating networks of stakeholder advocates.
5. Conclusions
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- Rodd, C.; Sharma, A.K. Recent Trends in the Prevalence of Overweight and Obesity among Canadian Children. CMAJ 2016, 188, E313–E320. [Google Scholar] [CrossRef] [PubMed]
- Daar, A.S.; Singer, P.A.; Persad, L.; Pramming, S.K.; Matthews, R.; Beaglehole, R.; Borysiewicz, L.K.; Colagiuri, S.; Ganguly, N.; Glass, R.I.; et al. Grand Challenges in Chronic Non-Communicable Diseases. Nature 2007, 450, 494–496. [Google Scholar] [CrossRef] [PubMed]
- Barlow, S.E. Expert Committee Recommendations Regarding the Prevention, Assessment, and Treatment of Child and Adolescent Overweight and Obesity: Summary Report. Pediatrics 2007, 120 (Suppl. 4), S164–S192. [Google Scholar] [CrossRef] [PubMed]
- Fanburg, J. (Ed.) 5210 Pediatric Obesity Clinical Decision Support Chart, 2nd ed.; American Academy of Pediatrics: Itasca, IL, USA, 2014. [Google Scholar]
- Finegood, D.T.; Merth, T.D.N.; Rutter, H. Implications of the Foresight Obesity System Map for Solutions to Childhood Obesity. Obesity 2010, 18 (Suppl. 1), S13–S16. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ogilvie, K.K.; Eggleton, A. Obesity in Canada: A Whole-of-Society Approach for a Healthier Canada. Available online: http://publications.gc.ca/site/eng/9.812199/publication.html (accessed on 20 September 2018).
- Vandenbroek, I.P.; Goossens, J.C.M. Tackling Obesities: Future Choices—Building the System Obesity Map. Available online: http://www.foresight.gov.uk/Obesity/12.pdf (accessed on 20 September 2018).
- Summerbell, C.D.; Waters, E.; de Silva Sanigorski, A.; Hall, B.J.; Brown, T.; Campbell, K.J.; Gao, Y.; Armstrong, R.; Prosser, L. Interventions for Preventing Obesity in Children (Review). Cochrane Collab. 2011, 12, 1–212. [Google Scholar] [CrossRef]
- Skinner, A.C.; Foster, E.M. Systems Science and Childhood Obesity: A Systematic Review and New Directions. J. Obes. 2013, 2013, 129193. [Google Scholar] [CrossRef] [PubMed]
- Allender, S.; Owen, B.; Kuhlberg, J.; Lowe, J.; Nagorcka-Smith, P.; Whelan, J.; Bell, C. A Community Based Systems Diagram of Obesity Causes. PLoS ONE 2015, 10, 1–12. [Google Scholar] [CrossRef] [PubMed]
- Rogers, V.W.; Hart, P.H.; Motyka, E.; Rines, E.N.; Vine, J.; Deatrick, D.A. Impact of Let’s Go! 5-2-1-0: A Community-Based, Multisetting Childhood Obesity Prevention Program. J. Pediatr. Psychol. 2013, 38, 1010–1020. [Google Scholar] [CrossRef] [PubMed]
- Amed, S.; Naylor, P.J.; Pinkney, S.; Shea, S.; Mâsse, L.C.; Berg, S.; Collet, J.P.; Wharf Higgins, J. Creating a Collective Impact on Childhood Obesity: Lessons from the SCOPE Initiative. Can. J. Public Health 2015, 106, e426–e433. [Google Scholar] [CrossRef] [PubMed]
- Amed, S.; Shea, S.; Pinkney, S.; Higgins, J.W.; Naylor, P.J. Wayfinding the Live 5-2-1-0 Initiative—At the Intersection between Systems Thinking and Community-Based Childhood Obesity Prevention. Int. J. Environ. Res. Public Health 2016, 13, 614. [Google Scholar] [CrossRef] [PubMed]
- King, L.; Gill, T.; Allender, S.; Swinburn, B. Best Practice Principles for Community-Based Obesity Prevention: Development, Content and Application. Obes. Rev. 2011, 12, 329–338. [Google Scholar] [CrossRef] [PubMed]
- Millar, L.; Robertson, N.; Allender, S.; Nichols, M.; Bennett, C.; Swinburn, B. Increasing Community Capacity and Decreasing Prevalence of Overweight and Obesity in a Community Based Intervention among Australian Adolescents. Prev. Med. (Baltim.) 2013, 56, 379–384. [Google Scholar] [CrossRef] [PubMed]
- Graham, I.D.; Logan, J.; Harrison, M.B.; Straus, S.E.; Tetroe, J.; Caswell, W.; Robinson, N. Lost in Knowledge Translation: Time for a Map? J. Contin. Educ. Health Prof. 2006, 26, 13–24. [Google Scholar] [CrossRef] [PubMed]
- Glasgow, R.E.; Vogt, T.M.; Boles, S.M. Evaluating the Public Health Impact of Health Promotion Interventions: The RE-AIM Framework. Am. J. Public Health 1999, 89, 1322–1327. [Google Scholar] [CrossRef] [PubMed]
- Gaglio, B.; Glasgow, R.E. Evaluation Approaches for Dissemination and Implementation Research. In Dissemination and Implementation Research in Health—Translating Science into Action; Oxford University Press: New York, NY, USA, 2012. [Google Scholar]
- Public Health Agency of Canada. Analysing Data Collected from the Community Capacity Building Tool: A Manual for Users; Public Health Agency of Canada: Ottawa, ON, Canada, 2007. [Google Scholar]
- Patton, M.Q. Qualitative Research & Evaluation Methods; Sage Publications: Thousand Oaks, CA, USA, 2011. [Google Scholar]
- Kastenholz, E.; Weiler, B.; Black, R.; Hong, J.; Zizzo, N.; Bell, E.; Lafontaine, A.L.; Racine, E.; Zuckerman, D.; Duncan, V.; et al. Achieving Research Impact Through Co-Creation in Community-Based Health Services: Literature Review and Case Study. J. Mark. Res. 2016, 3, 28. [Google Scholar] [CrossRef]
- Worthy, S.L.; Downey, L.; Dyk, P.H.; Monroe, P.A.; Tyler-Mackey, C.; Welborn, R. Turning the Tide on Poverty: Community Champions as Critical Elements of Success in Economically Distressed Communities. Community Dev. 2016, 47, 341–357. [Google Scholar] [CrossRef]
- World Health Organization. Population-Based Approaches to Childhood Obesity Prevention; WHO: Geneva, Switzerland, 2012. [Google Scholar]
- Israel, B.A.; Schulz, A.J.; Parker, E.A.; Becker, A.B. Review of Community-Based Research: Assessing Partnership Approaches to Improve Public Health. Annu. Rev. Public Health 1998, 19, 173–202. [Google Scholar] [CrossRef] [PubMed]
- Willows, N.D.; Hanley, A.J.G.; Delormier, T. A Socioecological Framework to Understand Weight-Related Issues in Aboriginal Children in Canada. Appl. Physiol. Nutr. Metab. 2012, 37, 1–13. [Google Scholar] [CrossRef] [PubMed]
- Sanigorski, A.M.; Bell, A.C.; Kremer, P.J.; Cuttler, R.; Swinburn, B.A. Reducing Unhealthy Weight Gain in Children through Community Capacity-Building: Results of a Quasi-Experimental Intervention Program, Be Active Eat Well. Int. J. Obes. 2008, 32, 1060–1067. [Google Scholar] [CrossRef] [PubMed]
- Higgins, J.W. Navigating through Translational Research: A Social Marketing Compass. Health Mark. Q. 2011, 28, 1–15. [Google Scholar] [CrossRef] [PubMed]
- Johnson-Shelton, D.; Moreno-Black, G.; Evers, C.; Zwink, N. A Community-Based Participatory Research Approach for Preventing Childhood Obesity: The Communities and Schools Together Project. Prog. Community Health Partnersh. Res. Educ. Action 2015, 9, 351–361. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Schell, S.F.; Luke, D.A.; Schooley, M.W.; Elliott, M.B.; Herbers, S.H.; Mueller, N.B.; Bunger, A.C. Public Health Program Capacity for Sustainability: A New Framework. Implement. Sci. 2013, 8, 1–9. [Google Scholar] [CrossRef] [PubMed]




{kind=link}
{kind=link}
{kind=link}
| Model Component | Description |
|---|---|
| Reach | The extent of the key players, partnerships, and collaborations that are actively participating in the development and implementation of the project |
| Engagement | Developing, sustaining and fostering relationships that facilitate knowledge exchange and sharing |
| Facilitation, coaching, training | Technical support and sharing of expertise through active participation of knowledge-users and on-site coaching |
| Resources | Development of new or contextualization of existing resources to enhance self-efficacy and skills around administering childhood obesity prevention initiatives |
| Adaptation | Continuous tailoring and adapting of activities to local settings, contexts, needs and priorities |
| Mobilization of champions | Identifying and mobilizing key champions and early adopters who represent various community sectors |
| Exchange of knowledge | Multiple levels of continuous, bi-directional exchange of knowledge, learning, and expertise |
| CCBT Domain | Description | What It Looks Like |
|---|---|---|
| Participation | Active involvement of community stakeholders in improving health and well-being | Community members and stakeholders are involved in the initiative’s activities, such as making decisions and evaluation |
| Leadership | Engagement of, and support from, formal and informal local leaders | Effective leaders support and encourage community members’ involvement, share leadership, and foster networks that bring people with diverse skill sets together |
| Community Structures | Engagement of community groups and committees | Groups that foster belonging and give the community a chance to express views and exchange information |
| Role of External Supports | Support from local government, foundations, or regional health authorities | Supports can link communities with external resources (e.g., technical expertise) and build early community momentum |
| Asking Why | A process for uncovering root causes for community health issues and potential solutions | The community comes together to critically assess the social, political, and economic influences that result in differing health standards and conditions |
| Obtaining Resources | Finding time, money, leadership, volunteers, and information from both inside and outside the community | Accessing the internal and external resources needed for the initiative to succeed |
| Skills, Knowledge, Learning | Qualities in the project team and broader community stakeholders that are used and developed | Developing skills and knowledge and providing learning opportunities |
| Links with Others | Connections (links) among individuals and organizations through partnerships, networks, and coalitions | Networking, exchanging information, and taking joint action with actors across diverse sectors |
| Sense of Community | Trust, courage, and hope fostered by coming together to address shared community problems | Community members and stakeholders collaborating to develop, implement, and sustain solutions |
| Mean Domain Score * | ||||||||
|---|---|---|---|---|---|---|---|---|
| Community | A | B | C | D | ||||
| Time Point | PRE | POST | PRE | POST | PRE | POST | PRE | POST |
| Participation | 3.00 | – | 3.75 | 3.75 | 2.25 | 2.25 | 2.00 | 2.50 |
| Leadership | 3.33 | – | 2.00 | 4.00 | 1.33 | 2.00 | 2.33 | 2.67 |
| Community Structures | 2.33 | – | 3.00 | 4.00 | 1.67 | 2.67 | 1.67 | 2.33 |
| Role of External Supports | 3.33 | – | 3.33 | 4.00 | 2.75 | 4.00 | 3.25 | 3.75 |
| Asking Why | 2.67 | – | 4.00 | 4.00 | 2.33 | 1.67 | 1.33 | 3.00 |
| Obtaining Resources | 3.50 | – | 4.00 | 4.00 | 4.00 | 3.00 | 4.00 | 4.00 |
| Skills, Knowledge, Learning | 2.50 | – | 3.50 | 4.00 | 2.50 | 3.00 | 3.00 | 3.00 |
| Links with Others | 3.25 | – | 4.00 | 4.00 | 3.00 | 3.00 | 2.50 | 3.00 |
| Sense of Community | 3.00 | – | 4.00 | 4.00 | 2.00 | 3.00 | 3.00 | 3.00 |
| Overall | 2.99 | – | 3.51 | 3.97 | 2.43 | 2.73 | 2.56 | 3.03 |

© 2019 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Kennedy, L.; Pinkney, S.; Suleman, S.; Mâsse, L.C.; Naylor, P.-J.; Amed, S. Propagating Change: Using RE-FRAME to Scale and Sustain A Community-Based Childhood Obesity Prevention Initiative. Int. J. Environ. Res. Public Health 2019, 16, 736. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph16050736
Kennedy L, Pinkney S, Suleman S, Mâsse LC, Naylor P-J, Amed S. Propagating Change: Using RE-FRAME to Scale and Sustain A Community-Based Childhood Obesity Prevention Initiative. International Journal of Environmental Research and Public Health. 2019; 16(5):736. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph16050736
Chicago/Turabian StyleKennedy, Lynn, Susan Pinkney, Selina Suleman, Louise C. Mâsse, Patti-Jean Naylor, and Shazhan Amed. 2019. "Propagating Change: Using RE-FRAME to Scale and Sustain A Community-Based Childhood Obesity Prevention Initiative" International Journal of Environmental Research and Public Health 16, no. 5: 736. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph16050736