Effect of an 8-Week Individualized Training Program on Blood Biomarkers, Adipokines and Endothelial Function in Obese Young Adolescents with and without Metabolic Syndrome

 , ,
, ,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Participants
2.2. Experimental Design
2.3. Biochemical Assays
2.4. Laser Doppler Flowmetry Combined with Iontophoresis of Ach and Temperature Elevation
2.5. Ventilatory Parameters and Lipid Oxidation Assay
2.6. Training Program
2.7. Statistical Analysis
3. Results
3.1. Effect of Training on Anthropometric Characteristics and Aerobic Capacity
3.2. Effect of Training on Blood Biomarkers and Adipokines
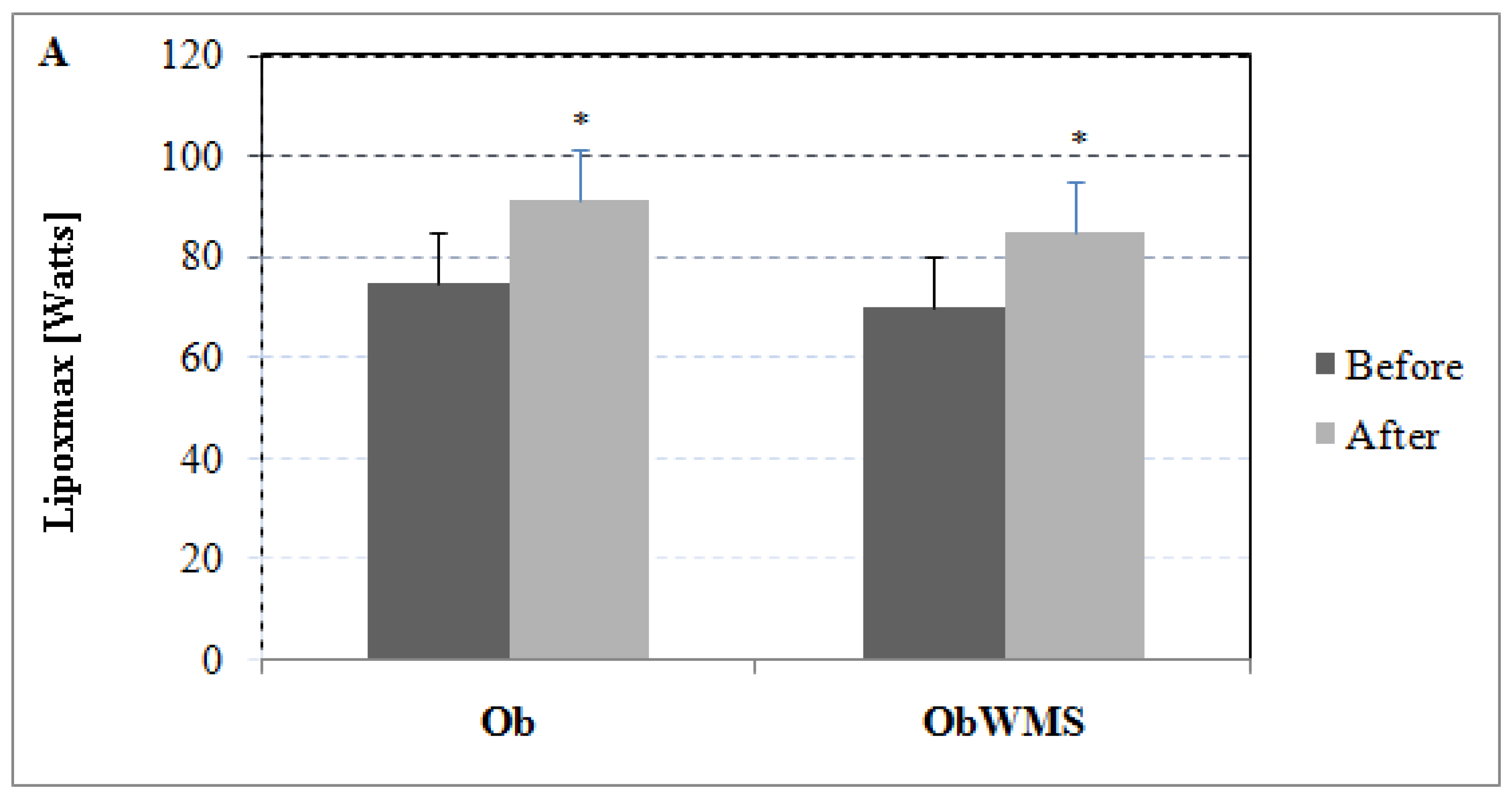
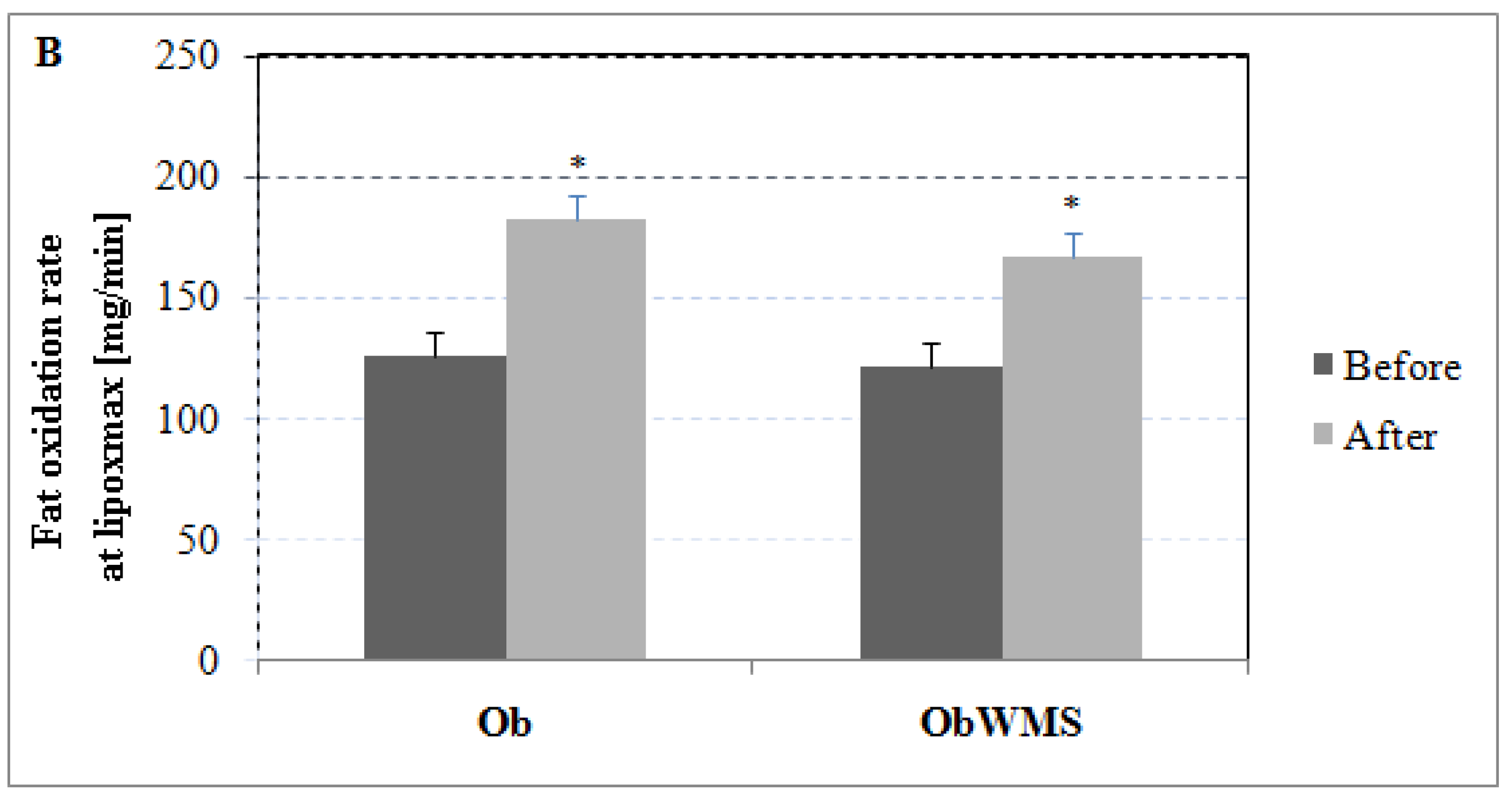
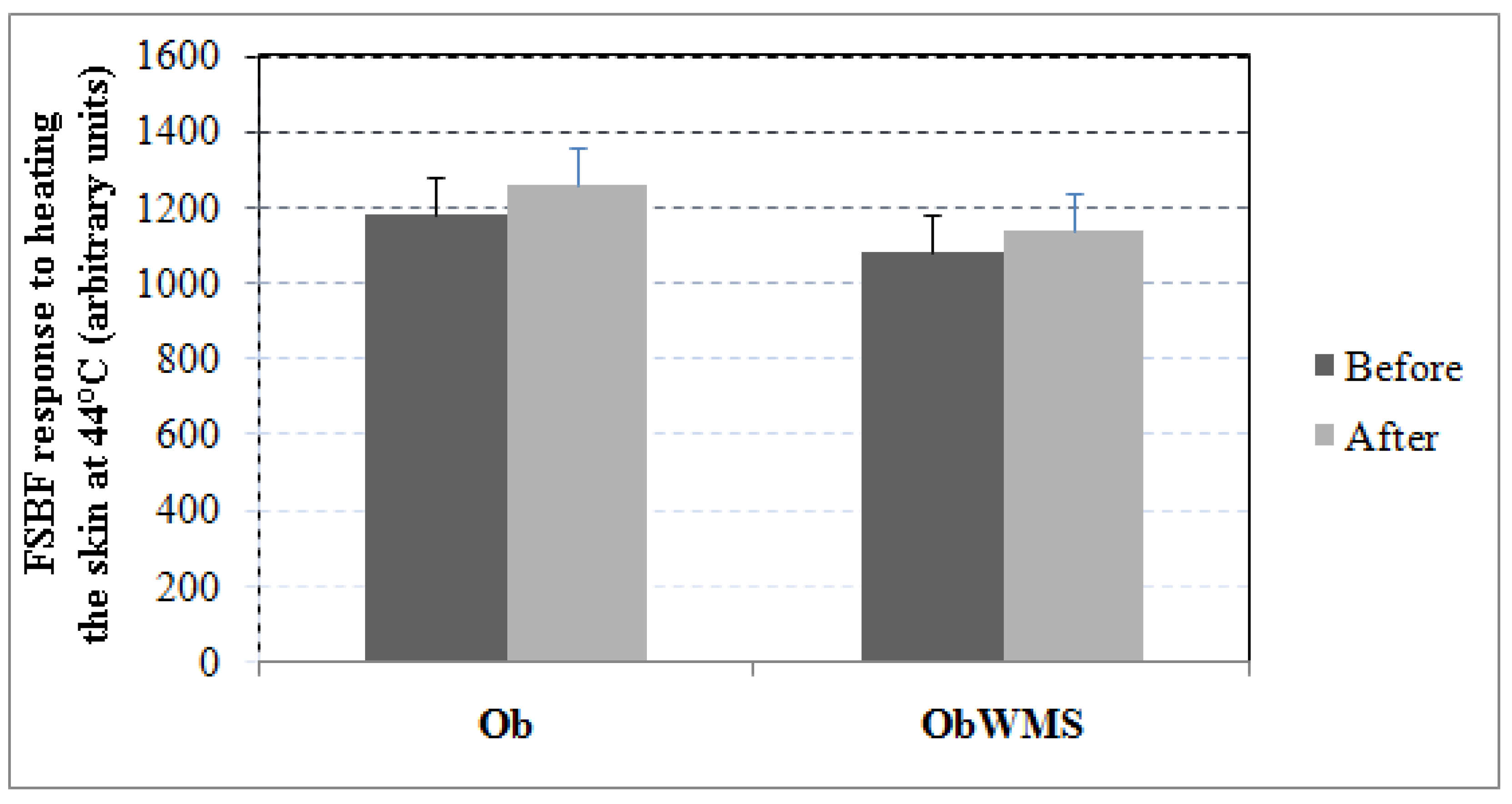
3.3. Effect of Training on Endothelial Function
4. Discussion
4.1. Effect of Training on Blood Biomarkers
4.2. Effect of Training on Adipokines
4.3. Effect of Training on Endothelial Function
5. Conclusions
Author Contributions
Funding
Conflicts of Interest
References
- Dehghan, M.; Akhtar-Danesh, N.; Merchant, A.T. Childhood obesity, prevalence and prevention. Nutr. J. 2005, 4, 24. [Google Scholar] [CrossRef] [PubMed]
- Mokhtar, N.; Elati, J.; Chabir, R.; Bour, A.; Elkari, K.; Schlossman, N.P.; Caballero, B.; Aguenaou, H. Diet culture and obesity in northern Africa. J. Nutr. 2001, 131, 887S–892S. [Google Scholar] [CrossRef] [PubMed]
- Steinberger, J.; Daniels, S.R.; Eckel, R.H.; Hayman, L.; Lustig, R.H.; McCrindle, B.; Mietus-Snyder, M.L.; American Heart Association Atherosclerosis, Hypertension, and Obesity in the Young Committee of the Council on Cardiovascular Disease in the Young; Council on Cardiovascular Nursing; Council on Nutrition, Physical Activity, and Metabolism. Progress and challenges in metabolic syndrome in children and adolescents: A scientific statement from the American Heart Association Atherosclerosis, Hypertension, and Obesity in the Young Committee of the Council on Cardiovascular Disease in the Young; Council on Cardiovascular Nursing; and Council on Nutrition, Physical Activity, and Metabolism. Circulation 2009, 119, 628–647. [Google Scholar] [PubMed]
- Klop, B.; Elte, J.W.; Cabezas, M.C. Dyslipidemia in obesity: Mechanisms and potential targets. Nutrients 2013, 5, 1218–1240. [Google Scholar] [CrossRef] [PubMed]
- Ekmen, N.; Helvaci, A.; Gunaldi, M.; Sasani, H.; Yildirmak, S.T. Leptin as an important link between obesity and cardiovascular risk factors in men with acute myocardial infarction. Indian Heart J. 2016, 68, 132–137. [Google Scholar] [CrossRef] [PubMed]
- Lobato, N.S.; Filgueira, F.P.; Akamine, E.H.; Tostes, R.C.; Carvalho, M.H.; Fortes, Z.B. Mechanisms of endothelial dysfunction in obesity-associated hypertension. Braz. J. Med. Biol. Res. 2012, 45, 392–400. [Google Scholar] [CrossRef] [PubMed]
- Singhal, A. Endothelial dysfunction: Role in obesity-related disorders and the early origins of CVD. Proc. Nutr. Soc. 2005, 64, 15–22. [Google Scholar] [CrossRef] [PubMed]
- Keighron, C.; Lyons, C.J.; Creane, M.; O’Brien, T.; Liew, A. Recent Advances in Endothelial Progenitor Cells Toward Their Use in Clinical Translation. Front. Med. (Lausanne) 2018, 5, 354. [Google Scholar] [CrossRef] [PubMed]
- Bruyndonckx, L.; Hoymans, V.Y.; Lemmens, K.; Ramet, J.; Vrints, C.J. Childhood obesity-related endothelial dysfunction: An update on pathophysiological mechanisms and diagnostic advancements. Pediatr. Res. 2016, 79, 831–837. [Google Scholar] [CrossRef] [PubMed]
- Bruyndonckx, L.; Hoymans, V.Y.; De Guchtenaere, A.; Van Helvoirt, M.; Van Craenenbroeck, E.M.; Frederix, G.; Lemmens, K.; Vissers, D.K.; Vrints, C.J.; Ramet, J.; et al. Diet, exercise, and endothelial function in obese adolescents. Pediatrics 2015, 135, e653–e661. [Google Scholar] [CrossRef] [PubMed]
- Bruyndonckx, L.; Hoymans, V.Y.; Frederix, G.; De Guchtenaere, A.; Franckx, H.; Vissers, D.K.; Vrints, C.J.; Ramet, J.; Conraads, V.M. Endothelial progenitor cells and endothelial microparticles are independent predictors of endothelial function. J. Pediatr. 2014, 165, 300–305. [Google Scholar] [CrossRef] [PubMed]
- Oladejo, A.O. Overview of the metabolic syndrome; an emerging pandemic of public health significance. Ann. Ib. Postgrad. Med. 2011, 9, 78–82. [Google Scholar] [PubMed]
- DeFronzo, R.A.; Ferrannini, E. Insulin resistance. A multifaceted syndrome responsible for NIDDM, obesity, hypertension, dyslipidemia, and atherosclerotic cardiovascular disease. Diabetes Care 1991, 14, 173–194. [Google Scholar] [CrossRef] [PubMed]
- Meigs, J.B.; Wilson, P.W.; Fox, C.S.; Vasan, R.S.; Nathan, D.M.; Sullivan, L.M.; D’Agostino, R.B. Body mass index, metabolic syndrome, and risk of type 2 diabetes or cardiovascular disease. J. Clin. Endocrinol. Metab. 2006, 91, 2906–2912. [Google Scholar] [CrossRef] [PubMed]
- Falkner, B.; Cossrow, N.D. Prevalence of metabolic syndrome and obesity-associated hypertension in the racial ethnic minorities of the United States. Curr. Hypertens. Rep. 2014, 16, 449. [Google Scholar] [CrossRef] [PubMed]
- Morandi, A.; Maffeis, C. Predictors of metabolic risk in childhood obesity. Horm. Res. Paediatr. 2014, 82, 3–11. [Google Scholar] [CrossRef] [PubMed]
- Eckel, R.H.; Alberti, K.G.; Grundy, S.M.; Zimmet, P.Z. The metabolic syndrome. Lancet 2010, 375, 181–183. [Google Scholar] [CrossRef]
- Simmons, R.K.; Alberti, K.G.; Gale, E.A.; Colagiuri, S.; Tuomilehto, J.; Qiao, Q.; Ramachandran, A.; Tajima, N.; Brajkovich Mirchov, I.; Ben-Nakhi, A.; et al. The metabolic syndrome: Useful concept or clinical tool? Report of a WHO Expert Consultation. Diabetologia 2010, 53, 600–605. [Google Scholar] [CrossRef] [PubMed]
- Cameron, A.J.; Zimmet, P.Z.; Shaw, J.E.; Alberti, K.G. The metabolic syndrome: In need of a global mission statement. Diabet. Med. 2009, 26, 306–309. [Google Scholar] [CrossRef] [PubMed]
- Kim, E.S.; Im, J.A.; Kim, K.C.; Park, J.H.; Suh, S.H.; Kang, E.S.; Kim, S.H.; Jekal, Y.; Lee, C.W.; Yoon, Y.J.; et al. Improved insulin sensitivity and adiponectin level after exercise training in obese Korean youth. Obesity (Silver Spring) 2007, 15, 3023–3030. [Google Scholar] [CrossRef] [PubMed]
- Meyer, A.A.; Kundt, G.; Lenschow, U.; Schuff-Werner, P.; Kienast, W. Improvement of early vascular changes and cardiovascular risk factors in obese children after a six-month exercise program. J. Am. Coll. Cardiol. 2006, 48, 1865–1870. [Google Scholar] [CrossRef] [PubMed]
- Foschini, D.; Araujo, R.C.; Bacurau, R.F.; De Piano, A.; De Almeida, S.S.; Carnier, J.; Rosa, T.D.; De Mello, M.T.; Tufik, S.; Dâmaso, A.R. Treatment of obese adolescents: The influence of periodization models and ACE genotype. Obesity (Silver Spring) 2010, 18, 766–772. [Google Scholar] [CrossRef] [PubMed]
- Johnston, C.A.; Tyler, C.; Fullerton, G.; McFarlin, B.K.; Poston, W.S.; Haddock, C.K.; Reeves, R.S.; Foreyt, J.P. Effects of a school-based weight maintenance program for Mexican-American children: Results at 2 years. Obesity 2010, 18, 542–547. [Google Scholar] [CrossRef] [PubMed]
- Davis, J.N.; Gyllenhammer, L.E.; Vanni, A.A.; Meija, M.; Tung, A.; Schroeder, E.T.; Spruijt-Metz, D.; Goran, M.I. Startup circuit training program reduces metabolic risk in Latino adolescents. Med. Sci. Sports Exerc. 2011, 43, 2195–2203. [Google Scholar] [CrossRef] [PubMed]
- Rademacher, E.; Mauer, M.; Jacobs, DR.; Chavers, B.; Steinke, J.; Sinaiko, A. Albumin excretion rate in normal adolescents: Relation to insulin resistance and cardiovascular risk factors and comparisons to type 1 diabetes mellitus patients. Clin. J. Am. Soc. Nephrol. 2008, 3, 998–1005. [Google Scholar] [CrossRef] [PubMed]
- Huang, P.L. A comprehensive definition for metabolic syndrome. Dis. Model. Mech. 2009, 2, 231–237. [Google Scholar] [CrossRef] [PubMed]
- Roberts, W.C. The Friedewald-Levy-Fredrickson formula for calculating low-density lipoprotein cholesterol, the basis for lipid-lowering therapy. Am. J. Cardiol. 1988, 62, 345–346. [Google Scholar] [CrossRef]
- Morris, S.J.; Shore, A.C. Skin blood flow responses to the iontophoresis of acetylcholine and sodium nitroprusside in man: Possible mechanisms. J. Physiol. 1996, 496, 531–542. [Google Scholar] [CrossRef] [PubMed]
- Droog, E.J.; Henricson, J.; Nilsson, G.E.; Sjöberg, F. A protocol for iontophoresis of acetylcholine and sodium nitroprusside that minimises nonspecific vasodilatory effects. Microvasc. Res. 2004, 67, 197–202. [Google Scholar] [CrossRef] [PubMed]
- Brandou, F.; Savy-Pacaux, A.M.; Marie, J.; Brun, J.F.; Mercier, J. Comparison of the type of substrate oxidation during exercise between pre and post pubertal markedly obese boys. Int. J. Sports Med. 2006, 27, 407–414. [Google Scholar] [CrossRef] [PubMed]
- Myers, J.; Kaminsky, L.A.; Lima, R.; Christle, J.W.; Ashley, E.; Arena, R. A Reference Equation for Normal Standards for VO2 Max: Analysis from the Fitness Registry and the Importance of Exercise National Database (FRIEND Registry). Prog. Cardiovasc. Dis. 2017, 60, 21–29. [Google Scholar] [CrossRef] [PubMed]
- Zguira, M.S.; Vincent, S.; Le Douairon Lahaye, S.; Malarde, L.; Tabka, Z.; Saïag, B. Intense exercise training is not effective to restore the endothelial NO-dependent relaxation in STZ-diabetic rat aorta. Cardiovasc. Diabetol. 2013, 12, 32. [Google Scholar] [CrossRef] [PubMed]
- Lahaye Sle, D.; Gratas-Delamarche, A.; Malardé, L.; Vincent, S.; Zguira, M.S.; Morel, S.L.; Delamarche, P.; Zouhal, H.; Carré, F.; Bekono, F.R. Intense exercise training induces adaptation in expression and responsiveness of cardiac β-adrenoceptors in diabetic rats. Cardiovasc. Diabetol. 2010, 9, 72. [Google Scholar] [CrossRef] [PubMed]
- Zguira, M.S.; Khouaja, I.; Zghal, F.; Zguira, H.; Debbabi, H.; Saiag, B.; Tabka, Z. Effects of an Acute Exercise on Endothelium Function in Athletics Young Subjects: A Case Control Study. Cardiovasc. Pharm. Open Access 2015, 4, 163. [Google Scholar]
- Ben Ounis, O.; Elloumi, M.; Lac, G.; Makni, E.; Van Praagh, E.; Zouhal, H.; Tabka, Z.; Amri, M. Two-month effects of individualized exercise training with or without caloric restriction on plasma adipocytokine levels in obese female adolescents. Ann. Endocrinol. (Paris) 2009, 70, 235–241. [Google Scholar] [CrossRef] [PubMed]
- Nassis, G.P.; Papantakou, K.; Skenderi, K.; Triandafillopoulou, M.; Kavouras, S.A.; Yannakoulia, M.; Chrousos, G.P.; Sidossis, L.S. Aerobic exercise training improves insulin sensitivity without changes in body weight, body fat, adiponectin, and inflammatory markers in overweight and obese girls. Metabolism 2005, 54, 1472–1479. [Google Scholar] [CrossRef] [PubMed]
- Wong, P.C.; Chia, M.Y.; Tsou, I.Y.; Wansaicheong, G.K.; Tan, B.; Wang, J.C.; Tan, J.; Kim, C.G.; Boh, G.; Lim, D. Effects of a 12-week exercise training programme on aerobic fitness, body composition, blood lipids and C-reactive protein in adolescents with obesity. Ann. Acad. Med. Singap. 2008, 37, 286–293. [Google Scholar] [PubMed]
- Van Der Heijden, G.J.; Wang, Z.J.; Chu, Z.; Toffolo, G.; Manesso, E.; Sauer, P.J.; Sunehag, A.L. Strength exercise improves muscle mass and hepatic insulin sensitivity in obese youth. Med. Sci. Sports Exerc. 2010, 42, 1973–1980. [Google Scholar] [CrossRef] [PubMed]
- Lee, S.; Bacha, F.; Hannon, T.; Kuk, J.L.; Boesch, C.; Arslanian, S. Effects of aerobic versus resistance exercise without caloric restriction on abdominal fat, intrahepatic lipid, and insulin sensitivity in obese adolescent boys: A randomized, controlled trial. Diabetes 2012, 61, 2787–2795. [Google Scholar] [CrossRef] [PubMed]
- Jenkins, N.T.; Witkowski, S.; Spangenburg, E.E.; Hagberg, J.M. Effects of acute and chronic endurance exercise on intracellular nitric oxide in putative endothelial progenitor cells: Role of NAPDH oxidase. Am. J. Physiol. Heart Circ. 2009, 297, H1798–H1805. [Google Scholar] [CrossRef] [PubMed]
- Vasconcellos, F.; Seabra, A.; Katzmarzyk, P.T.; Kraemer-Aguiar, L.G.; Bouskela, E.; Farinatti, P. Physical activity in overweight and obese adolescents: Systematic review of the effects on physical fitness components and cardiovascular risk factors. Sports Med. 2014, 44, 1139–1152. [Google Scholar] [CrossRef] [PubMed]
- De Mello, M.T.; de Piano, A.; Carnier, J.; Sanches Pde, L.; Corrêa, F.A.; Tock, L.; Ernandes, R.M.; Tufik, S.; Dâmaso, A.R. Long-term effects of aerobic plus resistance training on the metabolic syndrome and adiponectinemia in obese adolescents. J. Clin. Hypertens. (Greenwich) 2011, 13, 343–350. [Google Scholar] [CrossRef] [PubMed]
- Balagopal, P.; George, D.; Yarandi, H.; Funanage, V.; Bayne, E. Reversal of obesity-related hypoadiponectinemia by lifestyle intervention: A controlled, randomized study in obese adolescents. J. Clin. Endocrinol. Metab. 2005, 90, 6192–6197. [Google Scholar] [CrossRef] [PubMed]
- Tjønna, A.E.; Stølen, T.O.; Bye, A.; Volden, M.; Slørdahl, S.A.; Odegård, R.; Skogvoll, E.; Wisløff, U. Aerobic interval training reduces cardiovascular risk factors more than a multitreatment approach in overweight adolescents. Clin. Sci. (Lond.) 2009, 116, 317–326. [Google Scholar] [CrossRef] [PubMed]
- Kondo, T.; Kobayashi, I.; Murakami, M. Effect of exercise on circulating adipokine levels in obese young women. Endocr. J. 2006, 53, 189–195. [Google Scholar] [CrossRef] [PubMed]
- Ozcelik, O.; Celik, H.; Ayar, A.; Serhatlioglu, S.; Kelestimur, H. Investigation of the influence of training status on the relationship between the acute exercise and serum leptin levels in obese females. Neuroendocrinol. Lett. 2004, 25, 381–385. [Google Scholar] [PubMed]
- Polak, J.; Klimcakova, E.; Moro, C.; Viguerie, N.; Berlan, M.; Hejnova, J.; Richterova, B.; Kraus, I.; Langin, D.; Stich, V. Effect of aerobic training on plasma levels and subcutaneous abdominal adipose tissue gene expression of adiponectin, leptin, interleukin 6, and tumor necrosis factor 𝛼 in obese women. Metabolism 2006, 55, 1375–1381. [Google Scholar] [CrossRef] [PubMed]
- Gutin, B.; Ramsey, L.; Barbeau, P.; Cannady, W.; Ferguson, M.; Litaker, M.; Owens, S. Plasma leptin concentrations in obese children: Changes during 4-mo periods with and without physical training. Am. J. Clin. Nutr. 1999, 69, 388–394. [Google Scholar] [CrossRef] [PubMed]
- Kraemer, R.R.; Kraemer, G.R.; Acevedo, E.O.; Hebert, E.P.; Temple, E.; Bates, M.; Etie, A.; Haltom, R.; Quinn, S.; Castracane, V.D. Effects of aerobic exercise on serum leptin levels in obese women. Eur. J. Appl. Physiol. Occup. Physiol. 1999, 80, 154–158. [Google Scholar] [CrossRef] [PubMed]
- Cohen, N.D.; Dunstan, D.W.; Robinson, C.; Vulikh, E.; Zimmet, P.Z.; Shaw, J.E. Improved endothelial function following a 14-month resistance exercise training program in adults with type 2 diabetes. Diabetes Res. Clin. Pract. 2008, 79, 405–411. [Google Scholar] [CrossRef] [PubMed]
- Tinken, T.M.; Thijssen, D.H.J.; Hopkins, N.; Dawson, E.A.; Cable, N.T.; Green, D.J. Shear-stress mediates endothelial adaptations to exercise training in humans. Hypertension 2010, 55, 312–318. [Google Scholar] [CrossRef] [PubMed]
- Tjønna, A.E.; Lee, S.J.; Rognmo, Ø.; Stølen, T.O.; Bye, A.; Haram, P.M.; Loennechen, J.P.; Al-Share, Q.Y.; Skogvoll, E.; Slørdahl, S.A.; Kemi, O.J.; et al. Aerobic interval training versus continuous moderate exercise as a treatment for the metabolic syndrome: A pilot study. Circulation 2008, 118, 346–354. [Google Scholar] [CrossRef] [PubMed]
- Maiorana, A.; O’Driscoll, G.; Taylor, R.; Green, D. Exercise and the nitric oxide vasodilator system. Sports Med. 2003, 33, 1013–1035. [Google Scholar] [CrossRef] [PubMed]
- Green, D.J.; Walsh, J.H.; Maiorana, A.; Best, M.J.; Taylor, R.R.; O’Driscoll, J.G. Exercise-induced improvement in endothelial dysfunction is not mediated by changes in CV risk factors: Pooled analysis of diverse patient populations. Am. J. Physiol. Heart Circ. Physiol. 2003, 285, H2679–H2687. [Google Scholar] [CrossRef] [PubMed]
- Middlebrooke, A.R.; Elston, L.M.; Macleod, K.M.; Mawson, D.M.; Ball, C.I.; Shore, A.C.; Tooke, J.E. Six months of aerobic exercise does not improve microvascular function in type 2 diabetes mellitus. Diabetologia 2006, 49, 2263–2271. [Google Scholar] [CrossRef] [PubMed]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Parameter | Ob | ObWMS | ||
|---|---|---|---|---|
| Before | After | Before | After | |
| Age (years) | 13.3 ± 1.5 | 13.6 ± 1.2 | ||
| Body mass (kg) | 71.1 ± 7.6 | 68.2 ± 7.7 * | 90.1 ± 16.1 # | 86.7 ± 16.5 |
| Height (m) | 1.63 ± 0.06 | 1.64 ± 0.05 | ||
| BMI (kg·m−2) | 27.8 ± 2.1 | 27.2 ± 2.2 | 32.8 ± 5 # | 31 ± 5.1 |
| WC (cm) | 93.7 ± 5.6 | 89.7 ± 5.8 ** | 106.5 ± 5.2 # | 103.4 ± 5.3 * |
| Parameter | Ob (n = 71) | ObWMS (n = 51) | Overall P | ||||||
|---|---|---|---|---|---|---|---|---|---|
| Before | After | ES | P | Before | After | ES | P | ||
| Glucose (mmol/L) | 4.74 ± 0.22 | 4.50 ± 0.18 | −1.20 | <0.0001 | 5.11 ± 0.15 | 4.94 ± 0.26 | −0.80 | 0.0001 | 0.058 |
| TG (mmol/L) | 1.41 ± 0.16 | 1.30 ± 0.17 | −0.67 | 0.0001 | 1.79 ± 0.25 | 1.71 ± 0.12 | −0.42 | 0.040 | 0.34 |
| TC (mmol/L) | 4.09 ± 0.52 | 3.61 ± 0.61 | −0.85 | <0.0001 | 4.42 ± 0.55 | 3.99 ± 0.78 | −0.64 | 0.001 | 0.65 |
| LDL (mmol/L) | 2.35 ± 0.5 | 1.99 ± 0.32 | −0.86 | <0.0001 | 2.67 ± 0.4 | 2.41 ± 0.2 | −0.83 | <0.0001 | 0.14 |
| Adiponectin (µg/mL) | 2.25 ± 0.95 | 4.43 ± 1.48 | 1.76 | <0.0001 | 2.56 ± 0.9 | 3.55 ± 1.14 | 0.97 | <0.0001 | <0.0001 |
| Leptin (ng/mL) | 21.99 ± 5.15 | 19.23 ± 3.3 | −0.64 | 0.0002 | 26.51 ± 4.92 | 23.09 ± 5.54 | −0.65 | 0.001 | 0.44 |
© 2019 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Zguira, M.S.; Slimani, M.; Bragazzi, N.L.; Khrouf, M.; Chaieb, F.; Saïag, B.; Tabka, Z. Effect of an 8-Week Individualized Training Program on Blood Biomarkers, Adipokines and Endothelial Function in Obese Young Adolescents with and without Metabolic Syndrome. Int. J. Environ. Res. Public Health 2019, 16, 751. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph16050751
Zguira MS, Slimani M, Bragazzi NL, Khrouf M, Chaieb F, Saïag B, Tabka Z. Effect of an 8-Week Individualized Training Program on Blood Biomarkers, Adipokines and Endothelial Function in Obese Young Adolescents with and without Metabolic Syndrome. International Journal of Environmental Research and Public Health. 2019; 16(5):751. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph16050751
Chicago/Turabian StyleZguira, Mohamed Sami, Maamer Slimani, Nicola Luigi Bragazzi, Meriem Khrouf, Faten Chaieb, Bernard Saïag, and Zouhair Tabka. 2019. "Effect of an 8-Week Individualized Training Program on Blood Biomarkers, Adipokines and Endothelial Function in Obese Young Adolescents with and without Metabolic Syndrome" International Journal of Environmental Research and Public Health 16, no. 5: 751. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph16050751