Do Sleep Disorders Positively Correlate with Dry Eye Syndrome? Results of National Claim Data



Abstract
:1. Introduction
2. Methods
2.1. Study Population
2.2. Variables
2.3. Statistical Analysis
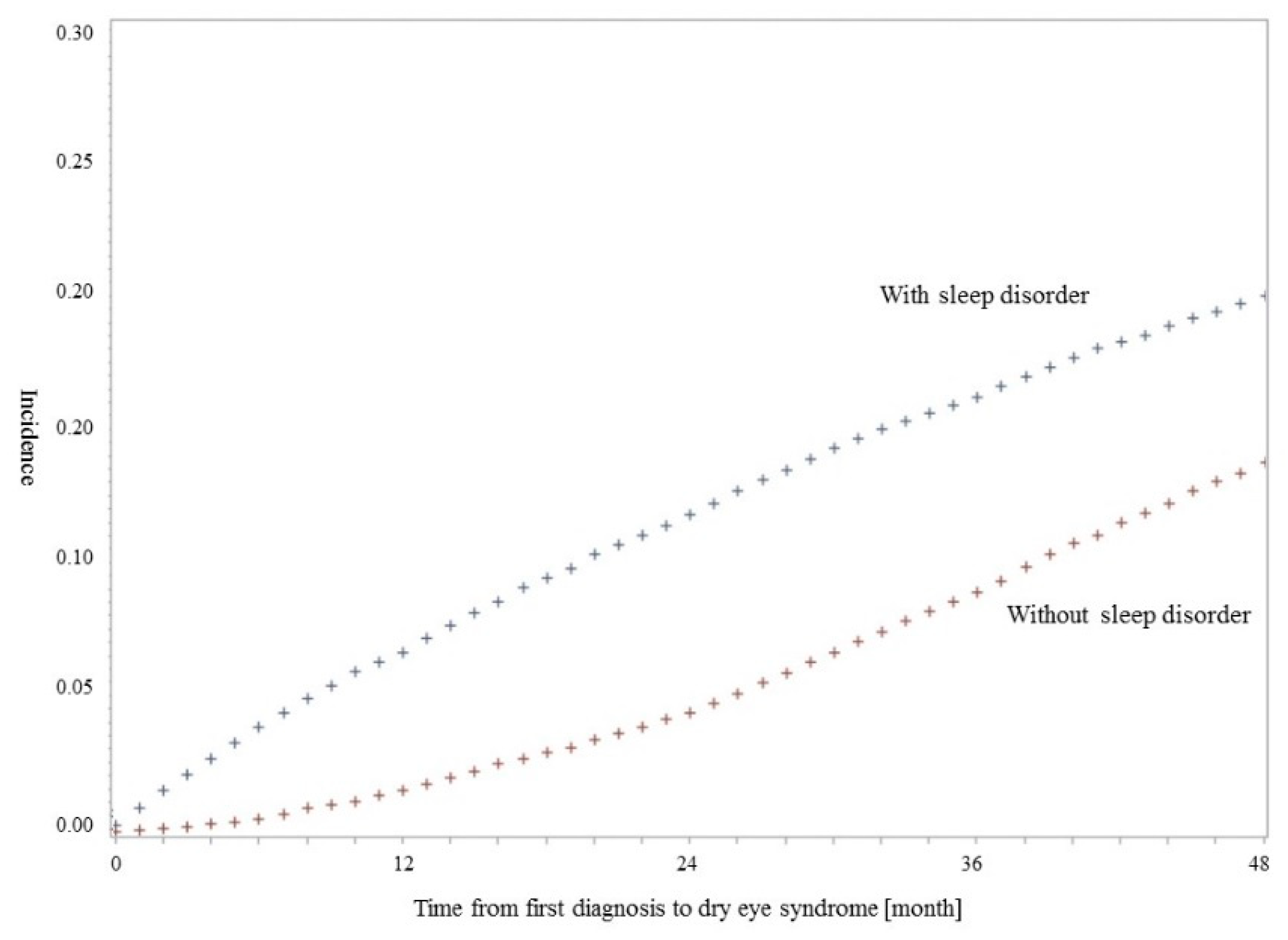
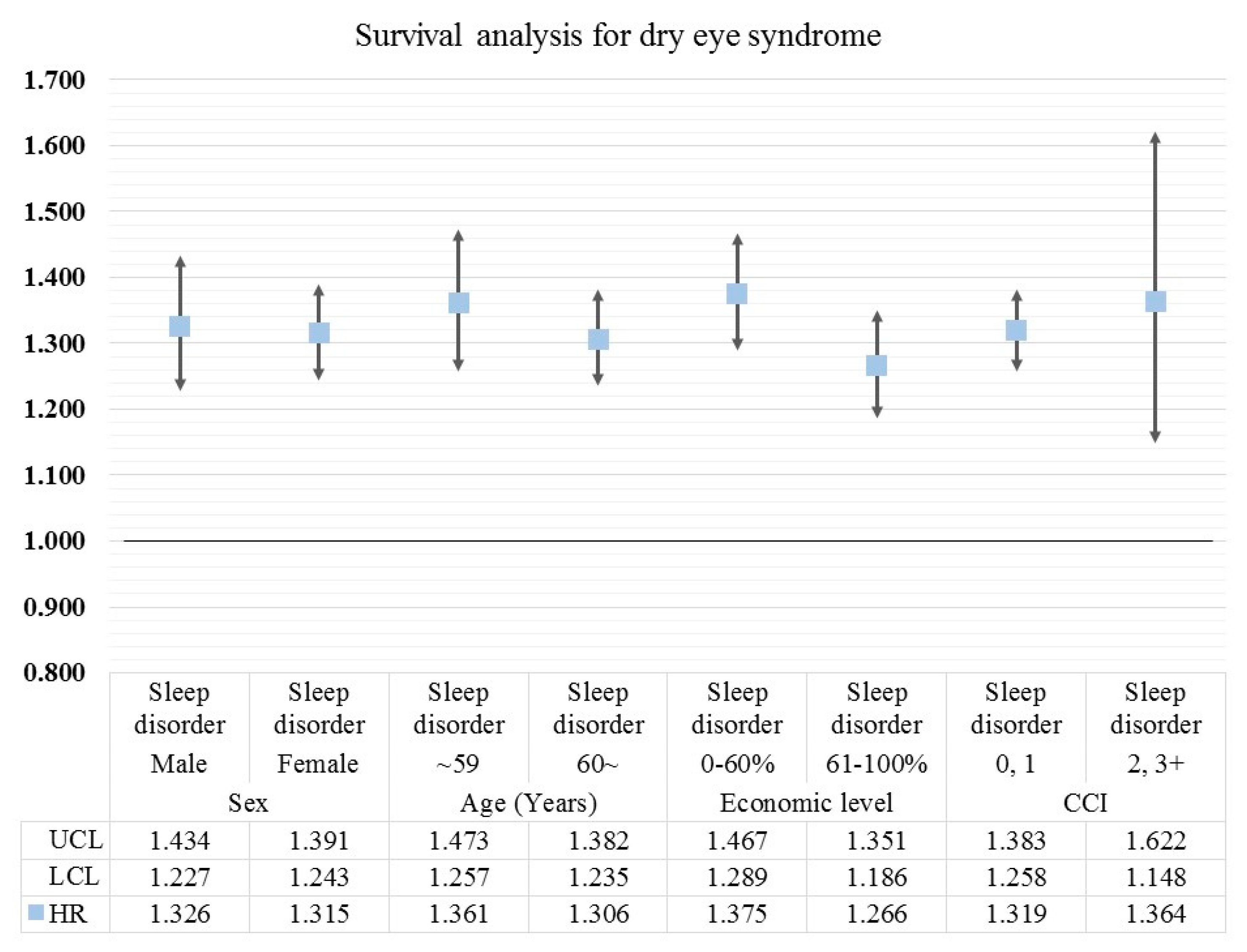
3. Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Conflicts of Interest
References
- Liu, W.-C.; Hsu, C.-M. The role of financial development in economic growth: The experiences of Taiwan, Korea, and Japan. J. Asian Econ. 2006, 17, 667–690. [Google Scholar] [CrossRef]
- Kwon, S. Thirty years of national health insurance in South Korea: Lessons for achieving universal health care coverage. Health Policy Plan. 2008, 24, 63–71. [Google Scholar] [CrossRef] [PubMed]
- Cho, M.J.; Nam, J.J.; Suh, G.H. Prevalence of symptoms of depression in a nationwide sample of Korean adults. Psychiatry Res. 1998, 81, 341–352. [Google Scholar] [CrossRef]
- Kuppermann, M.; Lubeck, D.P.; Mazonson, P.D.; Patrick, D.L.; Stewart, A.L.; Buesching, D.P.; Filer, S.K. Sleep problems and their correlates in a working population. J. Gen. Intern. Med. 1995, 10, 25–32. [Google Scholar] [CrossRef] [PubMed]
- Han, K.T.; Kim, W.; Kim, S.J.; Jang, S.Y.; Ju, Y.J.; Chun, S.Y.; Lee, S.G.; Park, E.C. Sleep disorders and risk of hospitalization in patients with mood disorders: Analysis of the National Sample Cohort over 10 years. Psychiatry Res. 2016, 245, 259–266. [Google Scholar] [CrossRef] [PubMed]
- Park, H.J.; Kim, M.S.; Park, E.C.; Jang, S.Y.; Kim, W.; Han, K.T. Association between sleep disorder and panic disorder in South Korea: Nationwide nested case-control study of data from 2004 to 2013. Psychiatry Res. 2018, 260, 286–291. [Google Scholar] [CrossRef] [PubMed]
- National Health Insurance Service. Statistics for Diseases: Sleep Disorder; National Health Insurance Service: Wonju, Korea, 2018. [Google Scholar]
- Dewald, J.F.; Meijer, A.M.; Oort, F.J.; Kerkhof, G.A.; Bögels, S.M. The influence of sleep quality, sleep duration and sleepiness on school performance in children and adolescents: A meta-analytic review. Sleep Med. Rev. 2010, 14, 179–189. [Google Scholar] [CrossRef] [PubMed]
- Suzuki, E.; Yorifuji, T.; Ueshima, K.; Takao, S.; Sugiyama, M.; Ohta, T.; Ishikawa-Takata, K.; Doi, H. Sleep duration, sleep quality and cardiovascular disease mortality among the elderly: A population-based cohort study. Prev. Med. 2009, 49, 135–141. [Google Scholar] [CrossRef] [PubMed]
- Knutson, K.L.; Ryden, A.M.; Mander, B.A.; Van Cauter, E. Role of sleep duration and quality in the risk and severity of type 2 diabetes mellitus. Arch. Intern. Med. 2006, 166, 1768–1774. [Google Scholar] [CrossRef] [PubMed]
- National Health Insurance Service. Statistics for Diseases: Dry Eye Syndrome; National Health Insurance Service: Wonju, Korea, 2018. [Google Scholar]
- Park, J.S.; Choi, M.J.; Ma, J.E.; Moon, J.H.; Moon, H.J. Influence of cellular phone videos and games on dry eye syndrome in university students. J. Korean Acad. Community Health Nurs. 2014, 25, 12–23. [Google Scholar] [CrossRef]
- Blehm, C.; Vishnu, S.; Khattak, A.; Mitra, S.; Yee, R.W. Computer vision syndrome: A review. Surv. Ophthalmol. 2005, 50, 253–262. [Google Scholar] [CrossRef] [PubMed]
- Miljanović, B.; Dana, R.; Sullivan, D.A.; Schaumberg, D.A. Impact of dry eye syndrome on vision-related quality of life. Am. J. Ophthalmol. 2007, 143, 409–415.e2. [Google Scholar] [CrossRef] [PubMed]
- Lee, C.J.; Levitt, R.C.; Felix, E.R.; Sarantopoulos, C.D.; Galor, A. Evidence that dry eye is a comorbid pain condition in a US veteran population. Pain Rep. 2017, 2, e629. [Google Scholar] [CrossRef] [PubMed]
- Ayaki, M.; Kawashima, M.; Negishi, K.; Kishimoto, T.; Mimura, M.; Tsubota, K. Sleep and mood disorders in dry eye disease and allied irritating ocular diseases. Sci. Rep. 2016, 6, 22480. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ayaki, M.; Kawashima, M.; Negishi, K.; Tsubota, K. High prevalence of sleep and mood disorders in dry eye patients: Survey of 1,000 eye clinic visitors. Neuropsychiatr. Dis. Treat. 2015, 11, 889. [Google Scholar] [CrossRef] [PubMed]
- Charlson, M.; Szatrowski, T.P.; Peterson, J.; Gold, J. Validation of a combined comorbidity index. J. Clin. Epidemiol. 1994, 47, 1245–1251. [Google Scholar] [CrossRef]
- Organization for Economic Co-operation and Development (OECD). Society at a Glance 2009, in OECD Social Indicators; OECD Publishing: Paris, France, 2009. [Google Scholar]
- Galor, A.; Seiden, B.E.; Park, J.J.; Feuer, W.J.; McClellan, A.L.; Felix, E.R.; Levitt, R.C.; Sarantopoulos, C.D.; Wallace, D.M. The association of dry eye symptom severity and comorbid insomnia in US veterans. Eye Contact Lens 2018, 44, S118–S124. [Google Scholar] [CrossRef] [PubMed]
- Ong, E.S.; Alghamdi, Y.A.; Levitt, R.C.; McClellan, A.L.; Lewis, G.; Sarantopoulos, C.D.; Felix, E.R.; Galor, A. Longitudinal examination of frequency of and risk factors for severe dry eye symptoms in US veterans. JAMA Ophthalmol. 2017, 135, 116–123. [Google Scholar] [CrossRef] [PubMed]
- Ayaki, M.; Tsubota, K.; Kawashima, M.; Kishimoto, T.; Mimura, M.; Negishi, K. Sleep Disorders are a Prevalent and Serious Comorbidity in Dry Eye. Investig. Ophthalmol. Vis. Sci. 2018, 59, DES143–DES150. [Google Scholar] [CrossRef] [PubMed]
- Lee, W.; Lim, S.S.; Won, J.U.; Roh, J.; Lee, J.H.; Seok, H.; Yoon, J.H. The association between sleep duration and dry eye syndrome among Korean adults. Sleep Med. 2015, 16, 1327–1331. [Google Scholar] [CrossRef] [PubMed]
- Lee, Y.B.; Koh, J.W.; Hyon, J.Y.; Wee, W.R.; Kim, J.J.; Shin, Y.J. Sleep Deprivation Reduces Tear Secretion and Impairs the Tear FilmSleep Deprivation Effect on Tear Secretion and Tear Film. Investig. Ophthalmol. Vis. Sci. 2014, 55, 3525–3531. [Google Scholar] [CrossRef] [PubMed]
- Moss, S.E.; Klein, R.; Klein, B.E. Prevalence of and risk factors for dry eye syndrome. Arch. Ophthalmol. 2000, 118, 1264–1268. [Google Scholar] [CrossRef] [PubMed]
- Ickovics, J.R.; Kershaw, T.S.; Westdahl, C.; Rising, S.S.; Klima, C.; Reynolds, H.; Magriples, U. Group prenatal care and preterm birth weight: Results from a matched cohort study at public clinics. Obstet. Gynecol. 2003, 102, 1051–1057. [Google Scholar] [CrossRef] [PubMed]
- Nowell, P.D.; Mazumdar, S.; Buysse, D.J.; Dew, M.A.; Reynolds, C.F.; Kupfer, D.J. Benzodiazepines and zolpidem for chronic insomnia: A meta-analysis of treatment efficacy. JAMA 1997, 278, 2170–2177. [Google Scholar] [CrossRef] [PubMed]



{kind=link}
{kind=link}
| Variables | Total | Dry Eye Syndrome | ||||
|---|---|---|---|---|---|---|
| Diagnosed | None | |||||
| N | % | N | % | N | % | |
| Sleep disorder | ||||||
| Yes | 22,183 | 50.00 | 4397 | 19.82 | 17,786 | 80.18 |
| No | 22,183 | 50.00 | 3032 | 13.67 | 19,151 | 86.33 |
| Sex | ||||||
| Male | 19,893 | 44.84 | 2564 | 12.89 | 17,329 | 87.11 |
| Female | 24,473 | 55.16 | 4865 | 19.88 | 19,608 | 80.12 |
| Age (Years) | ||||||
| <29 | 1312 | 2.96 | 125 | 9.53 | 1187 | 90.47 |
| 30–39 | 3498 | 7.88 | 515 | 14.72 | 2983 | 85.28 |
| 40–49 | 5694 | 12.83 | 736 | 12.93 | 4958 | 87.07 |
| 50–59 | 7804 | 17.59 | 1145 | 14.67 | 6659 | 85.33 |
| 60–69 | 10,385 | 23.41 | 1902 | 18.31 | 8483 | 81.69 |
| 70–79 | 7227 | 16.29 | 1466 | 20.29 | 5761 | 79.71 |
| >80 | 8446 | 19.04 | 1540 | 18.23 | 6906 | 81.77 |
| Economic level | ||||||
| <30% (low) | 12,195 | 27.49 | 2007 | 16.46 | 10,188 | 83.54 |
| 31–60% | 10,805 | 24.35 | 1659 | 15.35 | 9146 | 84.65 |
| 61–90% | 14,577 | 32.86 | 2504 | 17.18 | 12,073 | 82.82 |
| >91% (high) | 6789 | 15.30 | 1259 | 18.54 | 5530 | 81.46 |
| Types of insurance coverage | ||||||
| Medical aid | 1984 | 4.47 | 307 | 15.47 | 1677 | 84.53 |
| NHI, self–employed insured | 14,581 | 32.87 | 2362 | 16.20 | 12,219 | 83.80 |
| NHI, employee insured | 27,801 | 62.66 | 4760 | 17.12 | 23,041 | 82.88 |
| Charlson comorbidity index | ||||||
| 0 | 37,081 | 83.58 | 6226 | 16.79 | 30,855 | 83.21 |
| 1 | 4682 | 10.55 | 802 | 17.13 | 3880 | 82.87 |
| 2 | 1771 | 3.99 | 280 | 15.81 | 1491 | 84.19 |
| 3+ | 832 | 1.88 | 121 | 14.54 | 711 | 85.46 |
| Region | ||||||
| Metropolitan | 20,021 | 45.13 | 3496 | 17.46 | 16,525 | 82.54 |
| Others | 24,345 | 54.87 | 3933 | 16.16 | 20,412 | 83.84 |
| Total | 44,366 | 100.00 | 7429 | 16.74 | 36,937 | 83.26 |
| Variables | Dry Eye Syndrome | |||
|---|---|---|---|---|
| HR | 95% CI | p-Value | ||
| Lower | Upper | |||
| Sleep disorder | ||||
| Yes | 1.320 | 1.261 | 1.382 | <0.0001 |
| No | 1.000 | – | – | – |
| Sex | ||||
| Male | 0.640 | 0.615 | 0.667 | <0.0001 |
| Female | 1.000 | – | – | – |
| Age (Years) | ||||
| <29 | 1.000 | – | – | – |
| 30–39 | 1.594 | 1.350 | 1.882 | <0.0001 |
| 40–49 | 1.473 | 1.255 | 1.729 | <0.0001 |
| 50–59 | 1.688 | 1.445 | 1.973 | <0.0001 |
| 60–69 | 2.123 | 1.822 | 2.475 | <0.0001 |
| 70–79 | 2.479 | 2.124 | 2.894 | <0.0001 |
| >80 | 2.225 | 1.906 | 2.597 | <0.0001 |
| Economic level | ||||
| <30% (low) | 1.000 | – | – | – |
| 31–60% | 0.960 | 0.907 | 1.016 | 0.1622 |
| 61–90% | 1.029 | 0.977 | 1.084 | 0.2844 |
| >91% (high) | 1.086 | 1.020 | 1.155 | 0.0094 |
| Types of insurance coverage | ||||
| Medical aid | 0.949 | 0.858 | 1.049 | 0.3056 |
| NHI, self–employed insured | 0.940 | 0.902 | 0.980 | 0.0037 |
| NHI, employee insured | 1.000 | – | – | – |
| Charlson comorbidity index | ||||
| 0 | 1.000 | – | – | – |
| 1 | 1.053 | 0.991 | 1.119 | 0.0931 |
| 2 | 1.019 | 0.928 | 1.119 | 0.6983 |
| 3+ | 1.012 | 0.882 | 1.161 | 0.8621 |
| Region | ||||
| Metropolitan | 1.080 | 1.039 | 1.122 | <0.0001 |
| Others | 1.000 | – | – | – |
© 2019 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Han, K.-T.; Nam, J.H.; Park, E.-C. Do Sleep Disorders Positively Correlate with Dry Eye Syndrome? Results of National Claim Data. Int. J. Environ. Res. Public Health 2019, 16, 878. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph16050878
Han K-T, Nam JH, Park E-C. Do Sleep Disorders Positively Correlate with Dry Eye Syndrome? Results of National Claim Data. International Journal of Environmental Research and Public Health. 2019; 16(5):878. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph16050878
Chicago/Turabian StyleHan, Kyu-Tae, Ji Hyung Nam, and Eun-Cheol Park. 2019. "Do Sleep Disorders Positively Correlate with Dry Eye Syndrome? Results of National Claim Data" International Journal of Environmental Research and Public Health 16, no. 5: 878. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph16050878