Evidence-based Birth Attendance in Spain: Private versus Public Centers

 ,
,  ,
, 
Abstract
:1. Introduction
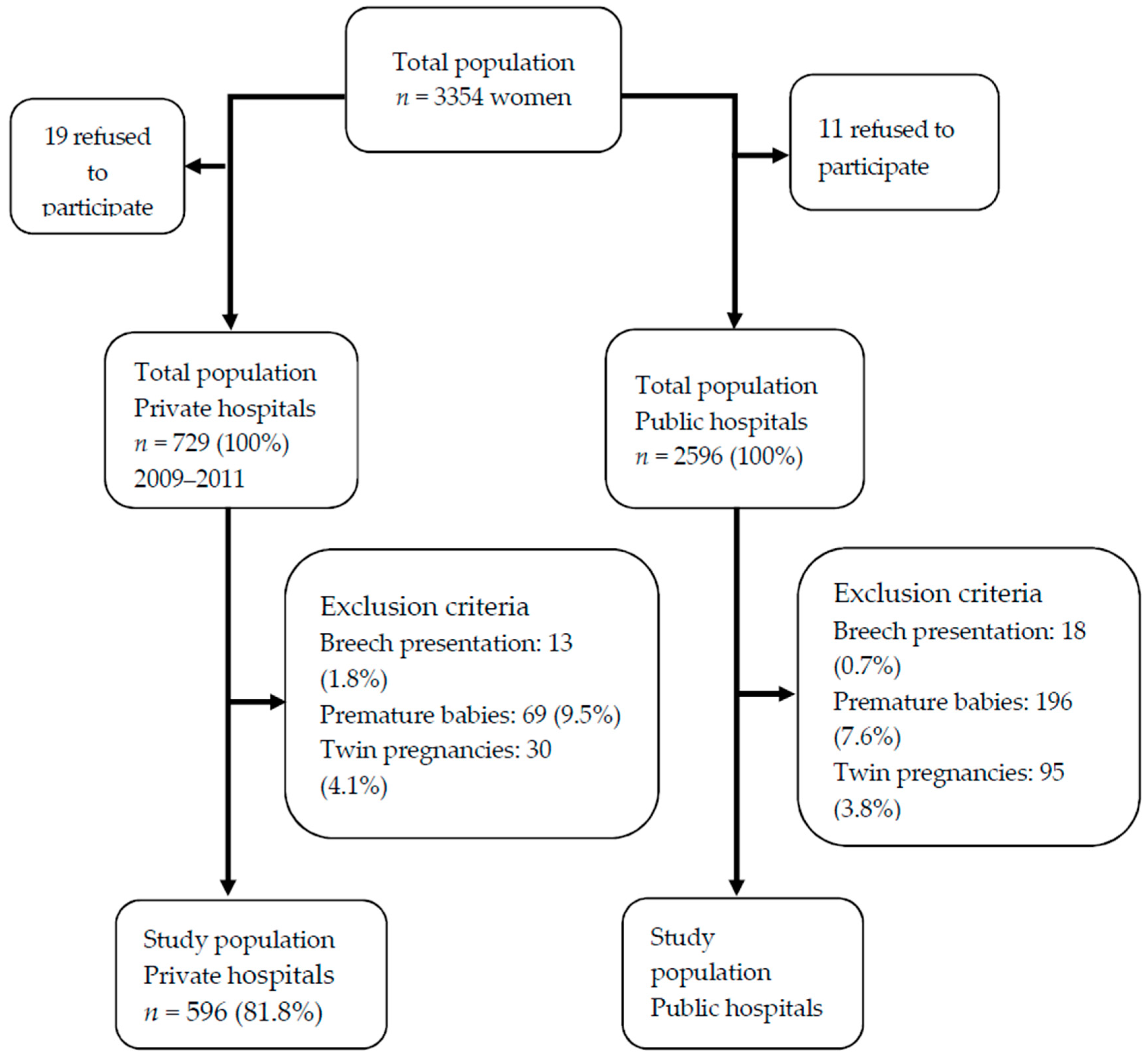
2. Materials and Methods
2.1. Information Sources
2.2. The Following Variables were Collected
2.3. Statistical Analysis
2.4. Ethic-Legal Considerations
3. Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Conflicts of Interest
References
- World Health Organization. Appropriate technology for birth. Lancet 1985, 2, 436–437. [Google Scholar]
- Ministerio de Sanidad y Consumo. Estrategia de atención al parto normal en el Sistema Nacional de Salud; Ministerio de Sanidad y Consumo: Madrid, Spain, 2008.
- National Institute for Health and Care Excellence. Intrapartum care: Care of healthy women and their babies during childbirth. NICE Clin Guidel 190 [Internet]. 2014. Available online: http://www.nice.org.uk/guidance/index.jsp?action=folder&o=67642 (accessed on 10 June 2018).
- Ministerio de Salud de Chile. Manual de atención personalizada en el proceso reproductivo. 2008. Available online: https://diprece.minsal.cl/wrdprss_minsal/wp-content/uploads/2015/10/2008_Manual-de-Atencion-personalizada-del-Proceso-reproductivo.pdf (accessed on 10 June 2018).
- Party MCW. Making Normal Birth a Reality: Consensus Statement from the Maternity Care Working Party [Internet]. London, UK, 2007. Available online: http://bhpelopartonormal.pbh.gov.br/estudos_cientificos/arquivos/normal_birth_consensus.pdf (accessed on 10 June 2018).
- FAME (Federación de Asociaciones de Matronas de España). Iniciativa Parto Normal de la FAME [Internet]. Barcelona, 2007. Available online: http://www.federacion-matronas.org/documentos/profesionales/iniciativa-parto-normal-de-la-fame/ (accessed on 10 June 2018).
- Lee, L.; Dy, J.; Azzam, H. Management of Spontaneous Labour at Term in Healthy Women. J. Obstet. Gynaecol. Can. 2016, 38, 843–865. [Google Scholar] [CrossRef] [PubMed]
- García-Armesto, S.; Begoña Abadía-Taira, M.; Durán, A.; Hernández-Quevedo, C.; Bernal-Delgado, E. Spain: Health system review. Health Syst. Transit. 2010, 12, 1–295. [Google Scholar] [PubMed]
- Chevreul, K.; Berg Brigham, K.; Durand-Zaleski, I.; Hernandez-Quevedo, C. France: Health System Review. Health Syst. Transit. 2015, 17, 1–218. [Google Scholar]
- Boyle, S. United Kingdom (England): Health system review. Health Syst Transit. 2011, 13, 1–483. [Google Scholar] [PubMed]
- Belló, M.; Becerril-Montekio, V.M. The health system of Argentina. Salud Publ. Mex. 2011, 53 (Suppl. 2), s96–s108. [Google Scholar]
- Miller, Y.D.; Prosser, S.J.; Thompson, R. Going public: Do risk and choice explain differences in cesarean birth rates between public and private places of birth in Australia? Midwifery 2012, 28, 627–635. [Google Scholar] [CrossRef]
- Marchildon, G. Canada Health system review Health Systems in Transition. Health Syst. Transit. 2013, 15, 1–179. [Google Scholar]
- Chi, C.; Pang, D.; Aris, I.M.; Teo, W.T.; Li, S.W.; Biswas, A.; et al. Trends and predictors of cesarean birth in Singapore, 2005–2014: A population-based cohort study. Birth 2018, 45, 399–408. [Google Scholar] [CrossRef]
- Organización Panamericana de la salud. Perfil del Sistema de Salud Estados Unidos de America. 2002. Available online: http://www.paho.org/hq/dmdocuments/2010/Perfil_Sistema_Salud-Estados_Unidos_America_2002.pdf (accessed on 10 June 2018).
- Sinnott, S.J.; Brick, A.; Layte, R.; Cunningham, N.; Turner, M.J. National Variation in Cesarean Section Rates: A Cross Sectional Study in Ireland. PLoS ONE 2016, 11, e0156172. [Google Scholar] [CrossRef]
- Coulm, B.; Ray, C.; Lelong, N.; Drewniak, N.; Zeitlin, J.; Blondel, B. Obstetric Interventions for Low-Risk Pregnant Women in France: Do Maternity Unit Characteristics Make a Difference? Birth 2012, 39, 183–191. [Google Scholar] [CrossRef] [PubMed]
- Ministerio de Sanidad, Consumo y Bienestar Social. Información estadística de hospitales. Estadística de Centros Sanitarios de Atención Especializada [Internet]. Estadística de Centros Sanitarios de Atención Especializada. Hospitales y Centros sin Internamiento, 2015. Available online: https://www.msssi.gob.es/estadEstudios/estadisticas/estHospiInternado/inforAnual/homeESCRI.htm (accessed on 10 June 2018).
- Lutomski, J.E.; Murphy, M.; Devane, D.; Meaney, S.; Greene, R.A. Private health care coverage and increased risk of obstetric intervention. BMC Pregnancy Child. 2014, 14, 13. [Google Scholar] [CrossRef] [PubMed]
- Hoxha, I.; Syrogiannouli, L.; Braha, M.; Goodman, D.C.; da Costa, B.R.; Jüni, P. Cesarean sections and private insurance: Systematic review and meta-analysis. BMJ Open 2017, 7, e016600. [Google Scholar] [CrossRef] [PubMed]
- Movsas, T.Z.; Wells, E.; Mongoven, A.; Grigorescu, V. Does medical insurance type (private vs public) influence the physician’s decision to perform Cesarean delivery? J. Med. Eth. 2012, 38, 470–473. [Google Scholar] [CrossRef] [PubMed]
- Phadungkiatwattana, P.; Tongsakul, N. Analyzing the impact of private service on the cesarean section rate in public hospital Thailand. Arch. Gynecol. Obstet. 2011, 284, 1375–1379. [Google Scholar] [CrossRef] [PubMed]
- Robson, S.J.; Laws, P.; Sullivan, E.A. Adverse outcomes of labour in public and private hospitals in Australia: A population-based descriptive study. Med. J. Aust. 2009, 190, 474–477. [Google Scholar] [PubMed]
- Alonso, B.D.; Silva, F.M.B.D.; Latorre, M.D.R.D.O.; Diniz, C.S.G.; Bick, D. Cesarean birth rates in public and privately funded hospitals: A cross-sectional study. Rev. Saude Publ. 2017, 51, 101. [Google Scholar] [CrossRef]
- Wilkes, E.; Gamble, J.; Adam, G.; Creedy, D.K. Reforming maternity services in Australia: Outcomes of a private practice midwifery service. Midwifery 2015, 31, 935–940. [Google Scholar] [CrossRef]
- Suárez-López, L.; Campero, L.; De la Vara-Salazar, E.; Rivera-Rivera, L.; Hernández-Serrato, M.I.; Walker, D.; Lazcano-Ponce, E. Sociodemographic and reproductive characteristics associated with the increase of cesarean section practice in Mexico. Salud Publ. Mex. 2013, 55 (Suppl. 2), S225–S234. [Google Scholar] [CrossRef]
- Márquez-Calderón, S.; Ruiz-Ramos, M.; Juárez, S.; Librero López, J. Cesarean delivery in Andalusia, Spain: Relationship with social, clinical and health services factors (2007–2009). Rev. Esp. Salud Publ. 2011, 85, 205–215. [Google Scholar] [CrossRef]
- Mossialos, E.; Allin, S.; Karras, K.; Davaki, K. An investigation of Cesarean sections in three Greek hospitals. Eur. J. Public Health 2005, 15, 288–295. [Google Scholar] [CrossRef] [PubMed]
- Coulm, B.; Blondel, B.; Alexander, S.; Boulvain, M.; Le Ray, C. Elective induction of labour and maternal request: A national population-based study. BJOG Int. J. Obstet. Gynaecol. 2016, 123, 2191–2197. [Google Scholar] [CrossRef]
- Prado, D.S.; Mendes, R.B.; Gurgel, R.Q.; Barreto ID de, C.; Bezerra, F.D.; Cipolotti, R.; Gurgel, R.Q. Practices and obstetric interventions in women from a state in the Northeast of Brazil. Rev. Assoc. Med. Bras. 2017, 63, 1039–1048. [Google Scholar] [CrossRef] [Green Version]
- Dahlen, H.G.; Tracy, S.; Tracy, M.; Bisits, A.; Brown, C.; Thornton, C. Rates of obstetric intervention among low-risk women giving birth in private and public hospitals in NSW: A population-based descriptive study. BMJ Open 2012, 2, e001723. [Google Scholar] [CrossRef]
- Escuriet, R.; Pueyo, M.J.; Perez-Botella, M.; Espada, X.; Salgado, I.; Gómez, A.; Biescas, H.; Espiga, I.; White, J.; Fernandez, R.; et al. Cross-sectional study comparing public and private hospitals in Catalonia: Is the practice of routine episiotomy changing? BMC Health Serv. Res. 2015, 15, 95. [Google Scholar] [CrossRef]


{kind=link}
| Variable | Primiparous | Multiparous | ||||
|---|---|---|---|---|---|---|
| Hospital Type | p | Hospital Type | p | |||
| Private n (%) 274 | Public n (%) 1223 | Private n (%) 322 | Public n (%) 1087 | |||
| Mother’s age | 0.007 | 0.001 | ||||
| <35 years | 145 (52.9) | 755 (61.7) | 110 (43.2) | 480 (44.2) | ||
| ≥35 years | 129 (47.1) | 468 (38.3) | 212 (65.8) | 607 (55.8) | ||
| Level of education | 0.010 | <0.001 | ||||
| No qualifications | 0 (0.0) | 5 (0.4) | 0 (0.0) | 2 (0.2) | ||
| Primary education | 4 (1.5) | 48 (3.9) | 6 (1.9) | 75 (6.9) | ||
| Secondary education | 85 (31.0) | 462 (37.8) | 94 (29.2) | 415 (38.2) | ||
| University education | 185 (67.5) | 708 (57.9) | 222 (68.9) | 595 (54.7) | ||
| Attendance to antenatal classes | 0.802 | <0.001 | ||||
| No | 22 (8.0) | 112 (9.2) | 173 (53.7) | 429 (39.5) | ||
| Yes, but fewer than five classes | 37 (13.5) | 155 (12.7) | 41 (12.7) | 143 (13.2) | ||
| Yes, a minimum of five classes | 215 (78.5) | 956 (78.2) | 108 (33.5) | 515 (47.4) | ||
| Nationality | 0.680 | 0.760 | ||||
| Spanish | 262 (95.6) | 1176 (96.2) | 313 (97.2) | 1053 (96.9) | ||
| Other | 12 (4.4) | 47 (3.8) | 9 (2.8) | 34 (3.1) | ||
| Health problems during pregnancy | 0.812 | 0.043 | ||||
| No | 200 (73.0) | 884 (72.3) | 243 (75.5) | 757 (69.6) | ||
| Yes | 74 (27.0) | 339 (27.3) | 79 (24.5) | 330 (30.4) | ||
| Previous cesarean | NA | 0.140 | ||||
| No | 274 (100) | 1223 (100) | 276 (85.7) | 947 (87.1) | ||
| Yes | NA | NA | 46 (14.3) | 140 (12.9) | ||
| Variable | Hospital | OR 95% CI | aOR 95% CI | |
|---|---|---|---|---|
| Private n (%) | Public n (%) | |||
| Induced birth | ||||
| No | 162 (59.1) | 752 (61.5) | 1 (ref.) | 1 (ref.) a |
| Yes | 112 (40.9) | 471 (38.5) | 1.11 (0.85–1.44) | 1.05 (0.78–1.42) |
| Birth plan | ||||
| No | 218 (79.6) | 954 (77.9) | 1 (ref.) | 1 (ref.) b |
| Yes | 56 (20.4) | 270 (22.1) | 0.91 (0.66–1.25) | 0.90 (0.65–1.24) |
| Use of epidural/rachianesthesia | ||||
| No | 29 (10.6) | 194 (15.9) | 1 (ref.) | 1 (ref.) c |
| Yes | 245 (89.4) | 1029 (84.1) | 1.59 (1.05–2.41) | 1.57 (1.03–1.40) |
| Use of natural methods to ease pain | ||||
| No | 197 (71.9) | 822 (67.3) | 1 (ref.) | 1 (ref.) d |
| Yes | 77 (28.1) | 399 (32.7) | 0.81 (0.60–1.08) | 0.79 (0.58–1.07) |
| Kristeller maneuver | ||||
| No | 148 (54.0) | 733 (59.9) | 1 (ref.) | 1 (ref.) d |
| Yes | 126 (46.0) | 490 (40.1) | 1.11 (0.85–1.44) | 1.27 (0.97–1.66) |
| Type of vaginal birth | ||||
| Eutocic/normal | 96 (55.2) | 617 (66.6) | 1 (ref.) | 1 (ref.) e |
| Instrumental | 78 (44.8) | 310 (33.4) | 1.62 (1.17–2.25) | 1.53 (1.09–2.15) |
| Cesarean | ||||
| No | 174 (63.5) | 927 (75.8) | 1 (ref.) | 1 (ref.) f |
| Yes | 100 (36.5) | 296 (24.2) | 1.80 (1.36–2.38) | 1.77 (1.33–2.37) |
| Severe tearing (grade III/IV) | ||||
| No | 166 (95.4) | 854 (92.1) | 1 (ref.) | 1 (ref.) g |
| Yes | 8 (4.6) | 73 (7.9) | 0.56 (0.27–1.19) | 0.49 (0.23–1.05) |
| Episiotomy | ||||
| No | 76 (43.7) | 362 (39.1) | 1 (ref.) | 1 (ref.) g |
| Yes | 98 (56.3) | 565 (60.9) | 0.83 (0.60–1.15) | 0.67 (0.47–0.96) |
| Mother admitted to an ICU | ||||
| No | 271 (98.9) | 1202 (98.3) | 1 (ref.) | 1 (ref.) h |
| Yes | 3 (1.1) | 21 (1.7) | 0.63 (1.89–2.14) | 0.44 (0.13–1.52) |
| Post-birth surgery | ||||
| No | 268 (97.8) | 1188 (97.1) | 1 (ref.) | 1 (ref.) h |
| Yes | 6 (2.2) | 35 (2.9) | 0.76 (0.32–1.83) | 0.74 (0.31–1.80) |
| Readmitted to hospital after discharge from hospital | ||||
| No | 266 (97.1) | 1181 (96.6) | 1 (ref.) | 1 (ref.) h |
| Yes | 8 (2.9) | 42 (3.4) | 0.85 (0.39–3.52) | 0.84 (0.34–1.82) |
| Variable | Hospital | OR 95% CI | aOR 95% CI | |
|---|---|---|---|---|
| Private n (%) | Public n (%) | |||
| Induced birth | ||||
| No | 215 (66.8) | 807 (74.2) | 1 (ref.) | 1 (ref.) a |
| Yes | 107 (33.2) | 280 (25.8) | 1.44 (1.06–1.88) | 1.49 (1.11–2.00) |
| Birth plan | ||||
| No | 265 (82.3) | 856 (78.7) | 1 (ref.) | 1 (ref.) b |
| Yes | 57 (17.7) | 231 (21.3) | 0.80 (0.58–1.10) | 0.81 (0.58–1.13) |
| Use of epidural/rachianesthesia | ||||
| No | 52 (16.1) | 389 (35.8) | 1 (ref.) | 1 (ref.) c |
| Yes | 270 (83.9) | 697 (64.2) | 2.89 (2.10–3.99) | 2.58 (1.83–3.63) |
| Use of natural methods to ease pain | ||||
| No | 271 (84.2) | 799 (73.5) | 1 (ref.) | 1 (ref.) d |
| Yes | 51 (15.8) | 288 (26.5) | 0.52 (1.38–0.73) | 0.51 (0.35–0.73) |
| Kristeller maneuver | ||||
| No | 239 (74.2) | 859 (79.0) | 1 (ref.) | 1 (ref.) d |
| Yes | 83 (25.8) | 228 (21.0) | 1.31 (0.98–1.75) | 1.20 (0.89–1.62) |
| Type of vaginal birth | ||||
| Eutocic/normal | 197 (82.1) | 831 (87.1) | 1 (ref.) | 1 (ref.) e |
| Instrumental | 43 (17.9) | 123 (12.9) | 1.48 (1.01–2.16) | 1.19 (0.78–1.80) |
| Cesarean | ||||
| No | 240 (74.5) | 954 (87.8) | 1 (ref.) | 1 (ref.) f |
| Yes | 82 (25.5) | 133 (12.2) | 2.45 (1.80–3.34) | 2.50 (1.81–3.46) |
| Severe tearing (grade III/IV) | ||||
| No | 232 (96.7) | 918 (96.2) | 1 (ref.) | 1 (ref.) g |
| Yes | 8 (3.3) | 36 (3.8) | 0.75 (0.88–1.92) | 0.71 (0.32–1.60) |
| Episiotomy | ||||
| No | 126 (52.5) | 593 (62.2) | 1 (ref.) | 1 (ref.) g |
| Yes | 114 (47.5) | 361 (37.8) | 1.49 (1.12–1.98) | 1.26 (0.92–1.72) |
| Mother admitted to an ICU | ||||
| No | 318 (98.8) | 1075 (98.9) | 1 (ref.) | 1 (ref.) h |
| Yes | 4 (1.2) | 12 (1.1) | 1.13 (0.36–3.52) | 0.77 (0.24–2.47) |
| Post-birth surgery | ||||
| No | 314 (97.5) | 1069 (98.3) | 1 (ref.) | 1 (ref.) h |
| Yes | 8 (2.5) | 18 (1.7) | 1.51 (0.65–3.52) | 1.19 (0.50–2.81) |
| Readmitted to hospital after discharge from hospital | ||||
| No | 316 (98.1) | 1055 (97.1) | 1 (ref.) | 1 (ref.) h |
| Yes | 6 (1.9) | 32 (2.9) | 0.63 (0.26–1.51) | 0.52 (0.21–1.27) |
| Variable | Hospital Type | OR 95% CI | aOR 95% CI | |
|---|---|---|---|---|
| Private n (%) | Public n (%) | |||
| Primiparous | ||||
| Skin-to-skin contact | ||||
| No | 96 (35.0) | 418 (34.2) | 1 (ref.) | 1 (ref.) a |
| Yes | 178 (65.0) | 805 (65.8) | 0.96 (0.73–1.27) | 1.65 (1.17–2.34) |
| Newborn admitted to hospital | ||||
| No | 257 (93.8) | 1120 (91.6) | 1 (ref.) | 1 (ref.) b |
| Yes | 17 (6.2) | 103 (8.4) | 0.72 (0.42–1.22) | 0.69 (0.40–1.18) |
| Artificial feeding/milk | ||||
| No | 182 (66.4) | 821 (67.1) | 1 (ref.) | 1 (ref.) c |
| Yes | 92 (33.6) | 402 (32.9) | 1.03 (0.78–1.36) | 0.99 (0.75–1.34) |
| Multiparous | ||||
| Skin-to-skin contact | ||||
| No | 107 (33.2) | 223 (20.5) | 1 (ref.) | 1 (ref.) a |
| Yes | 215 (66.8) | 864 (79.5) | 0.52 (0.39–0.68) | 0.75 (0.54–1.05) |
| Newborn admitted to hospital | ||||
| No | 308 (95.7) | 1022 (94.0) | 1 (ref.) | 1 (ref.) b |
| Yes | 14 (4.3) | 65 (6.0) | 0.72 (0.40–1.29) | 0.59 (0.32–1.09) |
| Artificial feeding/milk | ||||
| No | 260 (80.7) | 876 (80.6) | 1 (ref.) | 1 (ref.) c |
| Yes | 62 (19.3) | 211 (19.4) | 1.03 (0.78–1.36) | 0.95 (0.68–1.33) |
© 2019 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Hernández-Martínez, A.; Martínez-Galiano, J.M.; Rodríguez-Almagro, J.; Delgado-Rodríguez, M.; Gómez-Salgado, J. Evidence-based Birth Attendance in Spain: Private versus Public Centers. Int. J. Environ. Res. Public Health 2019, 16, 894. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph16050894
Hernández-Martínez A, Martínez-Galiano JM, Rodríguez-Almagro J, Delgado-Rodríguez M, Gómez-Salgado J. Evidence-based Birth Attendance in Spain: Private versus Public Centers. International Journal of Environmental Research and Public Health. 2019; 16(5):894. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph16050894
Chicago/Turabian StyleHernández-Martínez, Antonio, Juan Miguel Martínez-Galiano, Julián Rodríguez-Almagro, Miguel Delgado-Rodríguez, and Juan Gómez-Salgado. 2019. "Evidence-based Birth Attendance in Spain: Private versus Public Centers" International Journal of Environmental Research and Public Health 16, no. 5: 894. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph16050894