Association of Consecutive Influenza Vaccinations and Pneumonia: A Population-Based Case-Control Study

 ,
,  , and
, and
Abstract
:1. Introduction
2. Materials and Methods
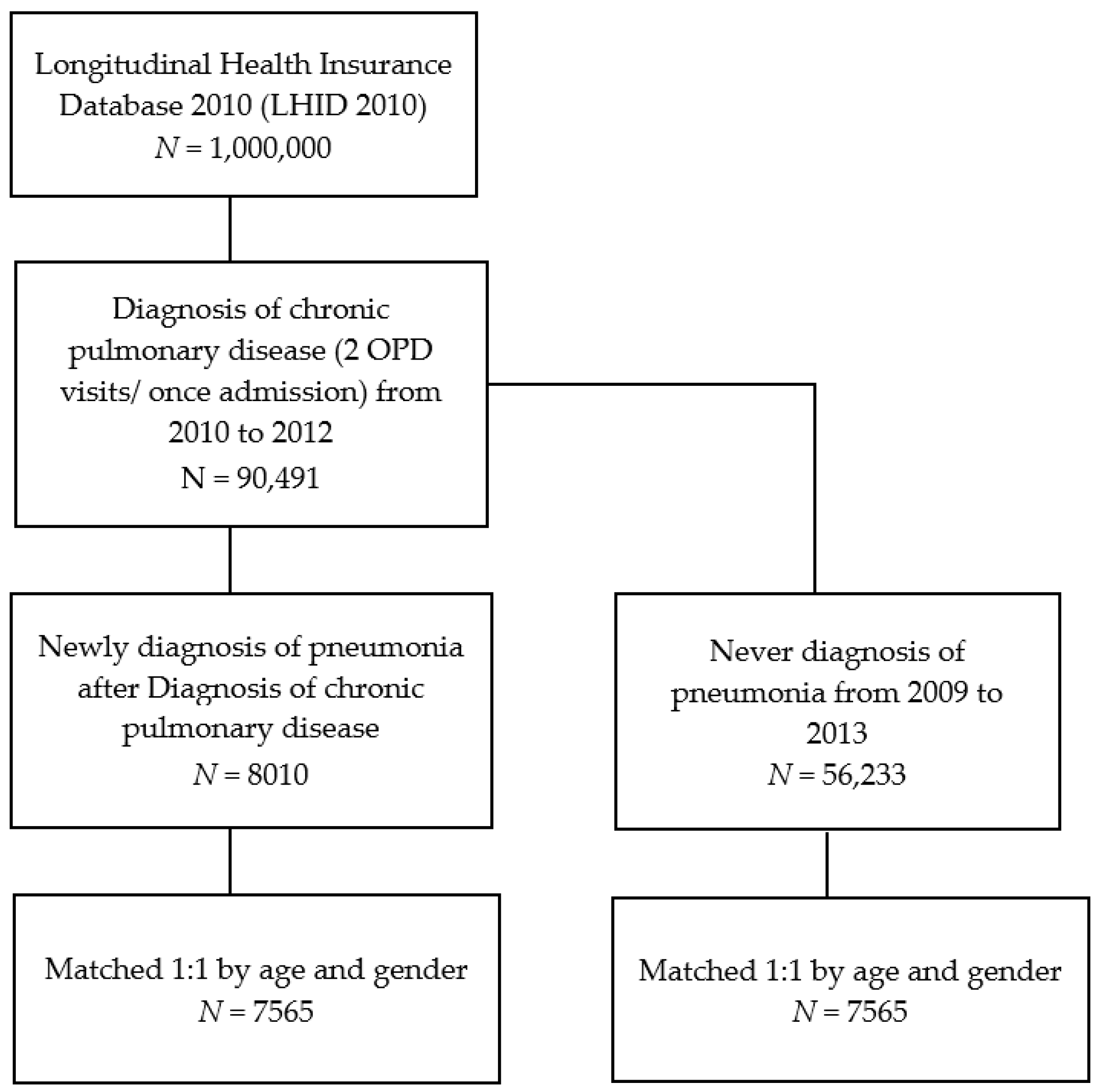
2.1. Data Source
2.2. Study Groups
2.3. Exposure Measurement
2.4. Statistical Analysis
3. Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- Cheng, C.W.; Chien, M.H.; Su, S.C.; Yang, S.F. New markers in pneumonia. Clin. Chim. Acta Int. J. Clin. Chem. 2013, 419, 19–25. [Google Scholar]
- Anand, N.; Kollef, M.H. The alphabet soup of pneumonia: CAP, HAP, HCAP, NHAP, and VAP. Semin. Respir. Crit. Care Med. 2009, 30, 3–9. [Google Scholar] [CrossRef] [PubMed]
- American Thoracic Society, & Infectious Diseases Society of America. Guidelines for the management of adults with hospital-acquired, ventilator-associated, and healthcare-associated pneumonia. Am. J. Respir. Crit. Care Med. 2005, 171, 388–416. [Google Scholar] [CrossRef] [PubMed]
- Jereb, M.; Kotar, T. Usefulness of procalcitonin to differentiate typical from atypical community-acquired pneumonia. Wien. Klin. Wochenschr. 2006, 118, 170–174. [Google Scholar] [CrossRef]
- Chang, G.M.; Tung, Y.C. Factors associated with pneumonia outcomes: A nationwide population-based study over the 1997–2008 period. J. Gen. Intern. Med. 2012, 27, 527–533. [Google Scholar] [CrossRef]
- Chiu, C.Y.; Chen, C.J.; Wong, K.S.; Tsai, M.H.; Chiu, C.H.; Huang, Y.C. Impact of bacterial and viral coinfection on mycoplasmal pneumonia in childhood community-acquired pneumonia. J. Microbiol. Immunol. Infect. = Wei Mian Yu Gan Ran Za Zhi 2015, 48, 51–56. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Cordoba, E.; Maduro, G.; Huynh, M.; Varma, J.K.; Vora, N.M. Deaths from pneumonia-New York City, 1999–2015. Open Forum Infect. Dis. 2018, 5, ofy020. [Google Scholar] [CrossRef] [PubMed]
- Huang, C.Y.; Chang, L.; Liu, C.C.; Huang, Y.C.; Chang, L.Y.; Huang, Y.C.; Chiu, N.C.; Lin, H.C.; Ho, Y.H.; Chi, H.; et al. Risk factors of progressive community-acquired pneumonia in hospitalized children: A prospective study. J. Microbiol. Immunol. Infect. = Wei Mian Yu Gan Ran Za Zhi 2015, 48, 36–42. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Tessmer, A.; Welte, T.; Schmidt-Ott, R.; Eberle, S.; Barten, G.; Suttorp, N.; Schaberg, T. Influenza vaccination is associated with reduced severity of community-acquired pneumonia. Eur. Respir. J. 2011, 38, 147–153. [Google Scholar] [CrossRef]
- Shinjoh, M.; Sugaya, N.; Yamaguchi, Y.; Iibuchi, N.; Kamimaki, I.; Goto, A.; Kobayashi, H.; Kobayashi, Y.; Shibata, M.; Tamaoka, S.; et al. Inactivated influenza vaccine effectiveness and an analysis of repeated vaccination for children during the 2016/17 season. Vaccine 2018, 36, 5510–5518. [Google Scholar] [CrossRef]
- Zhang, X.; Zhang, J.; Chen, L.; Feng, L.; Yu, H.; Zhao, G.; Zhang, T. Pneumonia and influenza hospitalizations among children under 5 years of age in Suzhou, China, 2005–2011. Influenza Other Respir. Viruses 2017, 11, 15–22. [Google Scholar] [CrossRef] [PubMed]
- Almond, M.H.; McAuley, D.F.; Wise, M.P.; Griffiths, M.J. Influenza-related pneumonia. Clin. Med. 2012, 12, 67–70. [Google Scholar] [Green Version]
- Huang, H.H.; Chen, S.J.; Chao, T.F.; Liu, C.J.; Chen, T.J.; Chou, P.; Wang, F.D. Influenza vaccination and risk of respiratory failure in patients with chronic obstructive pulmonary disease: A nationwide population-based case-cohort study. J. Microbiol. Immunol. Infect. 2019, 52, 22–29. [Google Scholar] [CrossRef] [PubMed]
- Heo, J.Y.; Song, J.Y.; Noh, J.Y.; Choi, M.J.; Yoon, J.G.; Lee, S.N.; Cheong, H.J.; Kim, W.J. Effects of influenza immunization on pneumonia in the elderly. Hum. Vaccines Immunother. 2018, 14, 744–749. [Google Scholar] [CrossRef]
- Wang, I.K.; Lin, C.L.; Chang, Y.C.; Lin, P.C.; Liang, C.C.; Liu, Y.L.; Chang, C.T.; Yen, T.H.; Huang, C.C.; Sung, F.C. Effectiveness of influenza vaccination in elderly diabetic patients: A retrospective cohort study. Vaccine 2013, 31, 718–724. [Google Scholar] [CrossRef] [PubMed]
- Clar, C.; Oseni, Z.; Flowers, N.; Keshtkar-Jahromi, M.; Rees, K. Influenza vaccines for preventing cardiovascular disease. Cochrane Database Syst. Rev. 2015, CD005050. [Google Scholar] [CrossRef]
- Casado, I.; Dominguez, A.; Toledo, D.; Chamorro, J.; Astray, J.; Egurrola, M.; Fernandez-Sierra, M.A.; Martin, V.; Morales-Suarez-Varela, M.; Godoy, P.; et al. Repeated influenza vaccination for preventing severe and fatal influenza infection in older adults: A multicentre case-control study. Can. Med. Assoc. J. 2018, 190, E3–E12. [Google Scholar] [CrossRef]
- Chang, T.Y.; Chao, T.F.; Liu, C.J.; Chen, S.J.; Chung, F.P.; Liao, J.N.; Tuan, T.C.; Chen, T.J.; Chen, S.A. The association between influenza infection, vaccination, and atrial fibrillation: A nationwide case-control study. Heart Rhythm 2016, 13, 1189–1194. [Google Scholar] [CrossRef]
- Shih, C.H.; Lee, Y.J.; Chao, P.W.; Kuo, S.C.; Ou, S.M.; Huang, H.M.; Chen, Y.T. Association between influenza vaccination and the reduced risk of acute kidney injury among older people: A nested case-control study. Eur. J. Intern. Med. 2018, 54, 65–69. [Google Scholar] [CrossRef]
- Vardeny, O.; Udell, J.A.; Joseph, J.; Farkouh, M.E.; Hernandez, A.F.; McGeer, A.J.; Talbot, H.K.; Bhatt, D.L.; Cannon, C.P.; Goodman, S.G.; et al. High-dose influenza vaccine to reduce clinical outcomes in high-risk cardiovascular patients: Rationale and design of the invested trial. Am. Heart J. 2018, 202, 97–103. [Google Scholar] [CrossRef]
- Wong, K.; Campitelli, M.A.; Stukel, T.A.; Kwong, J.C. Estimating influenza vaccine effectiveness in community-dwelling elderly patients using the instrumental variable analysis method. Arch. Intern. Med. 2012, 172, 484–491. [Google Scholar] [CrossRef]
- Li, C.; Gubbins, P.O.; Chen, G.J. Prior pneumococcal and influenza vaccinations and in-hospital outcomes for community-acquired pneumonia in elderly veterans. J. Hosp. Med. 2015, 10, 287–293. [Google Scholar] [CrossRef] [Green Version]
- Demirdogen Cetinoglu, E.; Uzaslan, E.; Sayiner, A.; Cilli, A.; Kilinc, O.; Sakar Coskun, A.; Hazar, A.; Kokturk, N.; Filiz, A.; Polatli, M. Pneumococcal and influenza vaccination status of hospitalized adults with community acquired pneumonia and the effects of vaccination on clinical presentation. Hum. Vaccines Immunother. 2017, 13, 2072–2077. [Google Scholar] [CrossRef]
- Liu, J.C.; Hsu, Y.P.; Kao, P.F.; Hao, W.R.; Liu, S.H.; Lin, C.F.; Sung, L.C.; Wu, S.Y. Influenza vaccination reduces dementia risk in chronic kidney disease patients: A population-based cohort study. Medicine 2016, 95, e2868. [Google Scholar] [CrossRef]
- Cauley, L.S.; Vella, A.T. Why is coinfection with influenza virus and bacteria so difficult to control? Discov. Med. 2015, 19, 33–40. [Google Scholar] [PubMed]
- Joseph, C.; Togawa, Y.; Shindo, N. Bacterial and viral infections associated with influenza. Influenza Other Respir. Viruses 2013, 7 (Suppl. 2), 105–113. [Google Scholar] [CrossRef] [Green Version]
- Tsai, Y.H.; Hsieh, M.J.; Chang, C.J.; Wen, Y.W.; Hu, H.C.; Chao, Y.N.; Huang, Y.C.; Yang, C.T.; Huang, C.C. The 23-valent pneumococcal polysaccharide vaccine is effective in elderly adults over 75 years old—Taiwan’s PPV vaccination program. Vaccine 2015, 33, 2897–2902. [Google Scholar] [CrossRef]
- Chen, G.W.; Shih, S.R.; Hsiao, M.R.; Chang, S.C.; Lin, S.H.; Sun, C.F.; Tsao, K.C. Multiple genotypes of influenza b viruses cocirculated in taiwan in 2004 and 2005. J. Clin. Microbiol. 2007, 45, 1515–1522. [Google Scholar] [CrossRef] [PubMed]
- Alfelali, M.; Khandaker, G.; Booy, R.; Rashid, H. Mismatching between circulating strains and vaccine strains of influenza: Effect on hajj pilgrims from both hemispheres. Hum. Vaccines Immunother. 2016, 12, 709–715. [Google Scholar] [CrossRef]
- Noh, J.Y.; Choi, W.S.; Song, J.Y.; Lee, H.S.; Lim, S.; Lee, J.; Seo, Y.B.; Lee, J.S.; Wie, S.H.; Jeong, H.W.; et al. Significant circulation of influenza b viruses mismatching the recommended vaccine-lineage in South Korea, 2007–2014. Vaccine 2018, 36, 5304–5308. [Google Scholar] [CrossRef] [PubMed]


{kind=link}
| Variable | Pneumonia (N = 7565) | Non-Pneumonia (N = 7565) | p-Value | ||
|---|---|---|---|---|---|
| n | % | n | % | ||
| Vaccination | 0.026 * | ||||
| No | 5006 | 66.2 | 4876 | 64.5 | |
| Yes | 2559 | 33.8 | 2689 | 35.5 | |
| Age | 1 | ||||
| <40 | 1739 | 23.0 | 1739 | 23.0 | |
| 40–65 | 1383 | 18.3 | 1383 | 18.3 | |
| ≥65 | 4443 | 58.7 | 4443 | 58.7 | |
| Mean ± SD | 59.1 ± 29.1 | 59.1 ± 29.1 | 1 | ||
| Gender | 1 | ||||
| Female | 2991 | 39.5 | 2991 | 39.5 | |
| Male | 4574 | 60.5 | 4574 | 60.5 | |
| Hypertension | 3694 | 48.8 | 3173 | 41.9 | <0.001 ** |
| Diabetes | 1673 | 22.1 | 1116 | 14.8 | <0.001 ** |
| Cerebrovascular disease | 1425 | 18.8 | 693 | 9.2 | <0.001 ** |
| Renal disease | 591 | 7.8 | 301 | 4.0 | <0.001 ** |
| Liver disease | 385 | 5.1 | 298 | 3.9 | 0.001 ** |
| Ischemic heart disease | 1435 | 19.0 | 1111 | 14.7 | <0.001 ** |
| Dementia | 665 | 8.8 | 262 | 3.5 | <0.001 ** |
| Alcohol-related disorder | 58 | 0.8 | 15 | 0.2 | <0.001 ** |
| Malignancy | 1009 | 13.3 | 406 | 5.4 | <0.001 ** |
| Variable | Crude OR | 95% CI | Adjusted OR † | 95% CI |
|---|---|---|---|---|
| Vaccination | ||||
| No | 1 | 1 | ||
| Yes | 0.91 | ** 0.84–0.98 | 0.85 | ** 0.79–0.93 |
| Hypertension | 1.48 | ** 1.37–1.60 | 1.26 | ** 1.16–1.37 |
| Diabetes | 1.73 | ** 1.58–1.89 | 1.46 | ** 1.33–1.62 |
| Cerebrovascular disease | 2.48 | ** 2.24–2.76 | 2.15 | ** 1.92–2.41 |
| Renal disease | 2.06 | ** 1.78–2.38 | 1.64 | ** 1.41–1.92 |
| Liver disease | 1.31 | ** 1.12–1.54 | 1.11 | 0.94–1.32 |
| Ischemic heart disease | 1.40 | ** 1.28–1.53 | 1.35 | ** 1.22–1.49 |
| Dementia | 2.95 | ** 2.52–3.45 | 2.72 | ** 2.3–3.23 |
| Alcohol-related disorder | 4.07 | ** 2.27–7.31 | 3.68 | ** 1.99–6.82 |
| Malignancy | 2.88 | ** 2.54–3.27 | 3.10 | ** 2.71–3.55 |
| Variable | N | No. of Pneumonia | Crude OR | 95% C.I. | Adjusted OR † | 95% C.I. | |
|---|---|---|---|---|---|---|---|
| Vaccination | |||||||
| 1 yr | 2 yr | ||||||
| No | No | 9882 | 5006 | 1 | 1 | ||
| No | Yes | 1282 | 665 | 1.03 | 0.91–1.17 | 0.98 | 0.86–1.12 |
| Yes | No | 1817 | 908 | 0.96 | 0.86–1.07 | 0.87 * | 0.78–0.98 |
| Yes | Yes | 2149 | 986 | 0.79 ** | 0.71–0.88 | 0.75 ** | 0.67–0.85 |
| Vaccination | |||||||
| Never | 9243 | 4685 | 1 | 1 | |||
| Three consecutive years | 1096 | 475 | 0.64 ** | 0.53–0.77 | 0.56 ** | 0.45–0.69 | |
| Variable | Vaccination | Non-Vaccination | OR | 95% CI | ||
|---|---|---|---|---|---|---|
| N | No. of Pneumonia Event | N | No. of Pneumonia Event | |||
| Age a | ||||||
| <40 | 513 | 271 | 2965 | 1468 | 1.17 | 0.94–1.46 |
| 40–65 | 219 | 143 | 2547 | 1240 | 1.69 ** | 1.23–2.33 |
| ≥65 | 4516 | 2145 | 4370 | 2298 | 0.78 ** | 0.71–0.86 |
| Gender b | ||||||
| Female | 1869 | 943 | 4113 | 2048 | 0.99 | 0.87–1.13 |
| Male | 3379 | 1616 | 5769 | 2958 | 0.78 ** | 0.7–0.87 |
© 2019 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Yeh, L.-T.; Chan, C.-H.; Yang, S.-F.; Yeh, H.-W.; Yeh, Y.-T.; Wang, Y.-H.; Chou, M.-C.; Yeh, C.-B.; Teng, Y.-H. Association of Consecutive Influenza Vaccinations and Pneumonia: A Population-Based Case-Control Study. Int. J. Environ. Res. Public Health 2019, 16, 1078. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph16061078
Yeh L-T, Chan C-H, Yang S-F, Yeh H-W, Yeh Y-T, Wang Y-H, Chou M-C, Yeh C-B, Teng Y-H. Association of Consecutive Influenza Vaccinations and Pneumonia: A Population-Based Case-Control Study. International Journal of Environmental Research and Public Health. 2019; 16(6):1078. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph16061078
Chicago/Turabian StyleYeh, Liang-Tsai, Chi-Ho Chan, Shun-Fa Yang, Han-Wei Yeh, Ying-Tung Yeh, Yu-Hsun Wang, Ming-Chih Chou, Chao-Bin Yeh, and Ying-Hock Teng. 2019. "Association of Consecutive Influenza Vaccinations and Pneumonia: A Population-Based Case-Control Study" International Journal of Environmental Research and Public Health 16, no. 6: 1078. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph16061078