Evaluation of Implementing a Home-Based Fall Prevention Program among Community-Dwelling Older Adults

 ,
,
Abstract
:1. Introduction
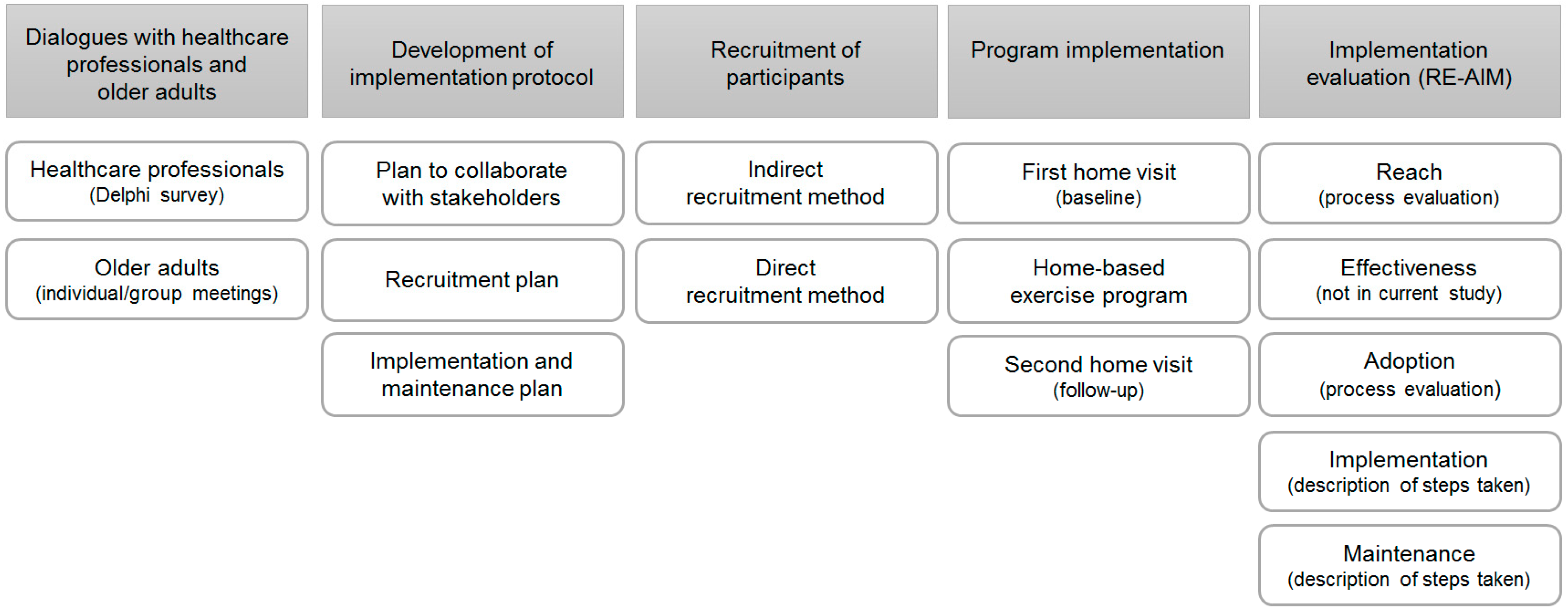
2. Materials and Methods
2.1. Study Design and Population
2.2. Dialogues with Heatlchare Professionals and Older Adults
2.2.1. Healthcare Professionals
2.2.2. Older Adults
2.3. Development of Implementation Protocol
2.4. Recruitment of Participants
2.5. Program Implementation
2.6. Implementation Evaluation
3. Results
3.1. Dialogues with Healthcare Professionals and Older Adults
3.1.1. Healthcare Professionals
3.1.2. Older Adults
3.2. Program Implementation
3.3. Implementation Evaluation
3.3.1. Reach
Indirect and Direct Methods
Barriers and Facilitators
3.3.2. Adoption
3.3.3. Implementation
Implemented as Planned
Program Satisfaction
3.3.4. Maintenance
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Conflicts of Interest
References
- Haagsma, J.A.; Graetz, N.; Bolliger, I.; Naghavi, M.; Higashi, H.; Mullany, E.C.; Abera, S.F.; Abraham, J.P.; Adofo, K.; Alsharif, U.; et al. The global burden of injury: Incidence, mortality, disability-adjusted life years and time trends from the Global Burden of Disease study 2013. Inj. Prev. 2016, 22, 3–18. [Google Scholar] [CrossRef] [PubMed]
- Orces, C.H.; Alamgir, H. Trends in fall-related injuries among older adults treated in emergency departments in the USA. Inj. Prev. 2014, 20, 421–423. [Google Scholar] [CrossRef]
- Davis, J.C.; Robertson, M.C.; Ashe, M.C.; Liu-Ambrose, T.; Khan, K.M.; Marra, C.A. International comparison of cost of falls in older adults living in the community: A systematic review. Osteoporos. Int. 2010, 21, 1295–1306. [Google Scholar] [CrossRef] [PubMed]
- Terroso, M.; Rosa, N.; Marques, A.T.; Simoes, R. Physical consequences of falls in the elderly: A literature review from 1995 to 2010. Eur. Rev. Aging Phys. Act. 2014, 11.1, 51. [Google Scholar] [CrossRef]
- Hopewell, S.; Adedire, O.; Copsey, B.J.; Boniface, G.J.; Sherrington, C.; Clemson, L.; Close, J.C.; Lamb, S.E. Multifactorial and multiple component interventions for preventing falls in older people living in the community. Cochrane Database Syst. Rev. 2018, 7. [Google Scholar] [CrossRef]
- Karlsson, M.K.; Magnusson, H.; von Schewelov, T.; Rosengren, B.E. Prevention of falls in the elderly—A review. Osteoporos. Int. 2013, 24, 747–762. [Google Scholar] [CrossRef]
- Sherrington, C.; Michaleff, Z.A.; Fairhall, N.; Paul, S.S.; Tiedemann, A.; Whitney, J.; Cumming, R.G.; Herbert, R.D.; Close, J.C.; Lord, S.R. Exercise to prevent falls in older adults: An updated systematic review and meta-analysis. Br. J. Sports Med. 2016, 51, 1750–1758. [Google Scholar] [CrossRef]
- Stubbs, B.; Brefka, S.; Denkinger, M. What works to prevent falls in community-dwelling older adults? An umbrella review of meta-analyses of randomized controlled trials. J. Am. Phys. Ther. Assoc. 2015, 95, 1095–1110. [Google Scholar] [CrossRef]
- Tricco, A.C.; Thomas, S.M.; Veroniki, A.A.; Hamid, J.S.; Cogo, E.; Strifler, L.; Khan, P.A.; Robson, R.; Sibley, K.M.; MacDonald, H.; et al. Comparisons of Interventions for Preventing Falls in Older Adults: A Systematic Review and Meta-analysis. JAMA 2017, 318, 1687–1699. [Google Scholar] [CrossRef] [PubMed]
- Yardley, L.; Kirby, S.; Ben-Shlomo, Y.; Gilbert, R.; Whitehead, S.; Todd, C. How likely are older people to take up different falls prevention activities? Prev. Med. 2008, 47, 554–558. [Google Scholar] [CrossRef] [PubMed]
- Yardley, L.; Bishop, F.; Beyer, N.; Hauer, K.; Kempen, G.; Pilot-Ziegler, C.; Tod, C.; Cuttelod, T.; Horne, M.; Lanta, K.; et al. Older people’s views of falls-prevention interventions in six european countries. Gerontologist 2006, 46, 650–660. [Google Scholar] [CrossRef] [PubMed]
- Child, S.; Goodwin, V.; Garside, R.; Jones-Hughes, T.; Boddy, K.; Stein, K. Factors influencing the implementation of fall-prevention programmes: A systematic review and synthesis of qualitative studies. Implement. Sci. 2012, 7, 91. [Google Scholar] [CrossRef] [PubMed]
- Casey, C.M.; Parker, E.M.; Winkler, G.; Liu, X.; Lambert, G.H.; Eckstrom, E. Lessons Learned From Implementing CDC’s STEADI Falls Prevention Algorithm in Primary Care. Gerontologist 2016, gnw074. [Google Scholar] [CrossRef] [PubMed]
- Li, F.; Harmer, P.; Fitzgerald, K.; Eckstrom, E.; Akers, L.; Chou, L.S.; Pidgeon, D.; Voit, J.; Winters-Stone, K. Effectiveness of a Therapeutic Tai Ji Quan Intervention vs a Multimodal Exercise Intervention to Prevent Falls Among Older Adults at High Risk of Falling: A Randomized Clinical Trial. JAMA Intern. Med. 2018, 178, 1301–1310. [Google Scholar] [CrossRef]
- Peel, N.M.; Travers, C.; Bell, R.A.; Smith, K. Evaluation of a health service delivery intervention to promote falls prevention in older people across the care continuum. J. Eval. Clin. Pract. 2010, 16, 1254–1261. [Google Scholar] [CrossRef] [PubMed]
- Roigk, P.; Becker, C.; Schulz, C.; Konig, H.H.; Rapp, K. Long-term evaluation of the implementation of a large fall and fracture prevention program in long-term care facilities. BMC Geriatr. 2018, 18, 233. [Google Scholar] [CrossRef] [PubMed]
- Coe, L.J.; St John, J.A.; Hariprasad, S.; Shankar, K.N.; MacCulloch, P.A.; Bettano, A.L.; Zotter, J. An Integrated Approach to Falls Prevention: A Model for Linking Clinical and Community Interventions through the Massachusetts Prevention and Wellness Trust Fund. Front. Public Health 2017, 5, 38. [Google Scholar] [CrossRef] [PubMed]
- Ory, M.G.; Smith, M.L.; Wade, A.; Mounce, C.; Wilson, A.; Parrish, R. Implementing and disseminating an evidence-based program to prevent falls in older adults, Texas, 2007–2009. Prev. Chronic Dis. 2010, 7, 6. [Google Scholar]
- Shubert, T.E.; Altpeter, M.; Busby-Whitehead, J. Using the RE-AIM framework to translate a research-based falls prevention intervention into a community-based program: Lessons learned. J. Saf. Res. 2011, 42, 509–516. [Google Scholar] [CrossRef] [PubMed]
- Durlak, J.A.; DuPre, E.P. Implementation matters: A review of research on the influence of implementation on program outcomes and the factors affecting implementation. Am. J. Community Psychol. 2008, 41, 327–350. [Google Scholar] [CrossRef] [PubMed]
- Glasgow, R.E.; Vogt, T.M.; Boles, S.M. Evaluating the Public Health Impact of Health Promotion Interventions: The RE-AIM Framework. Am. J. Public Health 1999, 89, 1322–1327. [Google Scholar] [CrossRef] [PubMed]
- Olij, B.F.; Erasmus, V.; Kuiper, J.I.; van Zoest, F.; van Beeck, E.F.; Polinder, S. Falls prevention activities among community-dwelling elderly in the Netherlands: A Delphi study. Injury 2017, 48, 2017–2021. [Google Scholar] [CrossRef] [PubMed]
- LimeSurvey Corporation. LimeSurvey User Manual; Carsten Schmitz: Hamburg, Germany, 2016. [Google Scholar]
- Bongers, K.; Schoon, Y.; Graauwmans, M.; Hoogsteen-Ossewaarde, M.; Olde Rikkert, M. Safety, feasibility and reliability of the maximal step length, gait speed and chair test measured by seniors themselves: The Senior Step Study. J. Aging Phys. Acc. 2015, 23, 438–443. [Google Scholar] [CrossRef]
- Campbell, A.J.; Robertson, M.C.; Gardner, M.M.; Norton, R.N.; Buchner, D.M. Falls prevention over 2 years: A randomized controlled trial in women 80 years and older. Age Ageing 1999, 28, 513–518. [Google Scholar] [CrossRef] [PubMed]
- Askari, M.; Eslami, S.; van Rijn, M.; Medlock, S.; Moll van Charante, E.P.; van der Velde, N.; de Rooij, S.E.; Abu-Hanna, A. Assessment of the quality of fall detection and management in primary care in the Netherlands based on the ACOVE quality indicators. Osteoporos. Int. 2016, 27, 569–576. [Google Scholar] [CrossRef] [PubMed]
- Bongers, K.T.J.; Schoon, Y.; Olde Rikkert, M.G.M. Self-management tasks to improve mobility and reduce fall risk are not leading to lower research participation in older adults. Arch. Gerontol Geriatr. 2018, 78, 14–17. [Google Scholar] [CrossRef] [PubMed]
- Van Dijk, H.M.; Cramm, J.M.; Nieboer, A.P. How To Build an Integrated Neighborhood Approach to Support Community-Dwelling Older People? Int. J. Integr. Care 2016, 16, 4. [Google Scholar]
- Brach, M.; Moschny, A.; Bucker, B.; Klaassen-Mielke, R.; Trampisch, M.; Wilm, S.; Platen, P.; Hinrichs, T. Recruiting hard-to-reach subjects for exercise interventions: A multi-centre and multi-stage approach targeting general practitioners and their community-dwelling and mobility-limited patients. Int. J. Environ. Res. Public Health 2013, 10, 6611–6629. [Google Scholar] [CrossRef] [PubMed]
- Grol, S.M.; Molleman, G.R.M.; Kuijpers, A.; van der Sande, R.; Fransen, G.A.J.; Assendelft, W.J.J.; Schers, H.J. The role of the general practitioner in multidisciplinary teams: A qualitative study in elderly care. BMC Fam. Pract. 2018, 19, 40. [Google Scholar] [CrossRef]
- Russell, K.; Taing, D.; Roy, J. Measurement of Fall Prevention Awareness and Behaviours among Older Adults at Home. Can. J. Aging 2017, 36, 522–535. [Google Scholar] [CrossRef] [PubMed]
- CBS Nederland. Population. 2017. Available online: http://www.cbs.nl/en-gb/society/population (accessed on 15 December 2018).
- Murthy, V.H.; Krumholz, H.M.; Gross, C.P. Participation in Cancer Clinical Trials: Race-, Sex-, and Age-Based Disparities. JAMA 2004, 291, 2720–2726. [Google Scholar] [CrossRef] [PubMed]
- Leake, A.R.; Bermudo, V.C.; Jacob, J.; Jacob, M.R.; Inouye, J. Health is wealth: Methods to improve attendance in a lifestyle intervention for a largely immigrant Filipino-American sample. J. Immigr. Minor. Health 2012, 14, 475–480. [Google Scholar] [CrossRef] [PubMed]
- Metayer, N.; Boulos, R.; Tovar, A.; Gervis, J.; Abreu, J.; Hval, E.; Kamins, C.L.; Tofuri, K.; Economos, C.D. Recruitment of New Immigrants Into a Randomized Controlled Prevention Trial: The Live Well Experience. J. Prim. Prev. 2018, 39, 453–468. [Google Scholar] [CrossRef] [PubMed]



{kind=link}
{kind=link}
| Dimension | Original Definition | Study Definition |
|---|---|---|
| Reach | Proportion of individuals that participated in the program | Proportion of individuals that enrolled in the study through indirect and direct methods; barriers and facilitators in recruitment |
| Effectiveness | Outcome effects of implementing the program as planned | Not discussed in current manuscript |
| Adoption | Proportion of practices and individuals that adopted the program | Activities executed to optimize collaboration with stakeholders |
| Implementation | Extent to which the program is implemented as planned | Extent to which the program was implemented as planned; program satisfaction of the participants |
| Maintenance | Extent to which a program is maintained over time | Activities executed to maintain the program locally |
| (n = 95) | |
|---|---|
| Barrier | (%) |
| Reaching older adults that are not in touch with healthcare professionals | 58 |
| Poor communication between different stakeholders | 53 |
| Absence of a neighborhood coordinator | 52 |
| Healthcare professionals that do not have enough knowledge on fall prevention | 47 |
| High costs | 36 |
| Lack of time | 31 |
| Lack of a central location in a large neighborhood | 15 |
| Facilitator | (%) |
| Good cooperation between different healthcare professionals | 60 |
| Taking into account the wishes and needs of older adults | 60 |
| Clear communication between different stakeholders | 48 |
| Shared vision on fall prevention in a community setting among stakeholders | 42 |
| Word of mouth | 31 |
| Providing good information about fall prevention to healthcare professionals | 28 |
| Neighborhood coordinator that takes control | 21 |
© 2019 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Olij, B.F.; Erasmus, V.; Barmentloo, L.M.; Burdorf, A.; Smilde, D.; Schoon, Y.; van der Velde, N.; Polinder, S. Evaluation of Implementing a Home-Based Fall Prevention Program among Community-Dwelling Older Adults. Int. J. Environ. Res. Public Health 2019, 16, 1079. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph16061079
Olij BF, Erasmus V, Barmentloo LM, Burdorf A, Smilde D, Schoon Y, van der Velde N, Polinder S. Evaluation of Implementing a Home-Based Fall Prevention Program among Community-Dwelling Older Adults. International Journal of Environmental Research and Public Health. 2019; 16(6):1079. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph16061079
Chicago/Turabian StyleOlij, Branko F., Vicki Erasmus, Lotte M. Barmentloo, Alex Burdorf, Dini Smilde, Yvonne Schoon, Nathalie van der Velde, and Suzanne Polinder. 2019. "Evaluation of Implementing a Home-Based Fall Prevention Program among Community-Dwelling Older Adults" International Journal of Environmental Research and Public Health 16, no. 6: 1079. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph16061079