Dealing with Ethical Concerns in Suicide Research: A Survey of Australian Researchers

 , , , , and
, , , , and
Abstract
:1. Introduction
2. Materials and Methods
2.1. Survey
2.2. Sampling
2.3. Analyses
3. Results
3.1. Characteristics of the Sample
3.2. Characteristics of Specific Ethics Applications
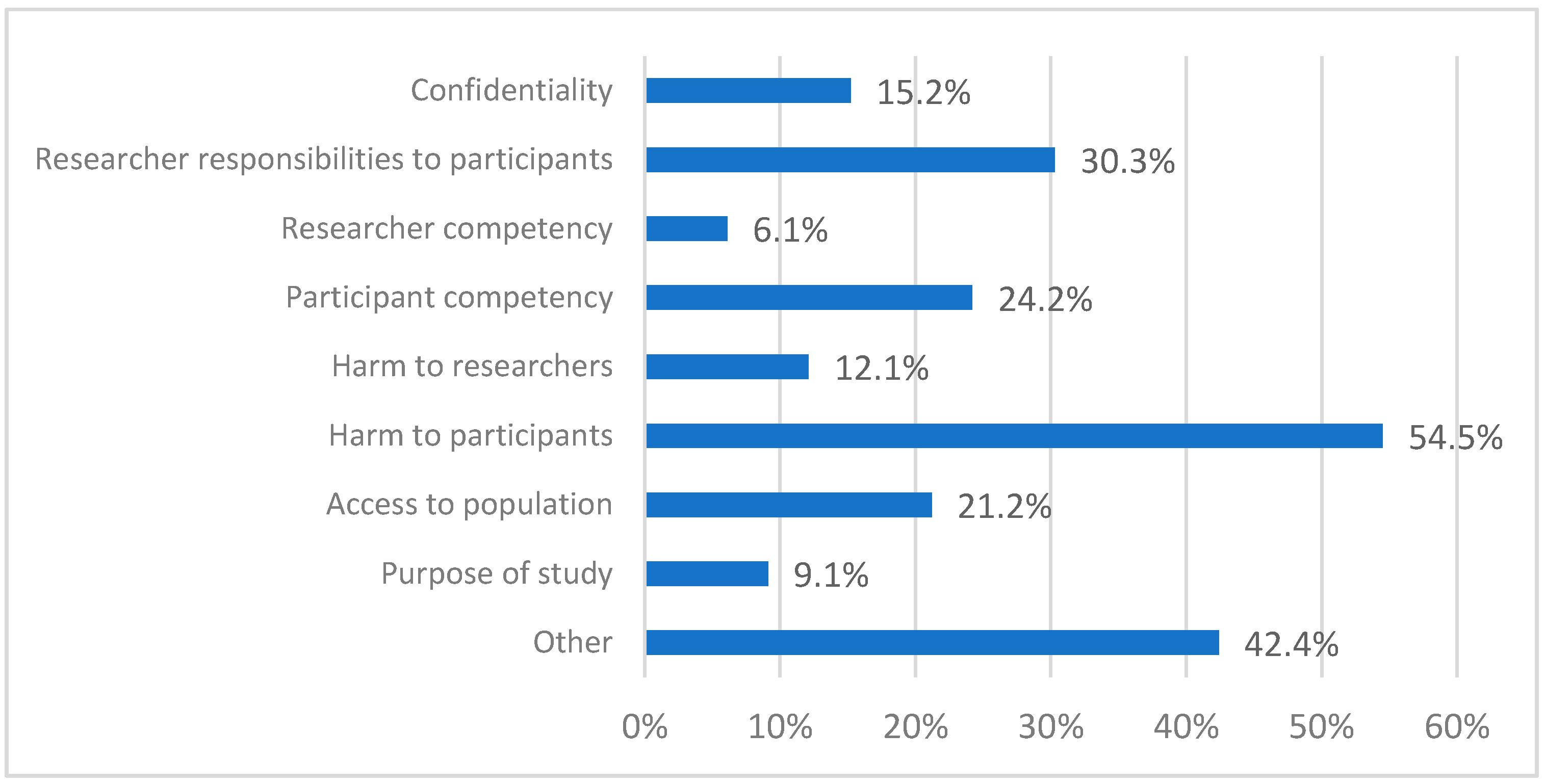
3.3. Concerns Received by Respondents from Their Ethics Committees
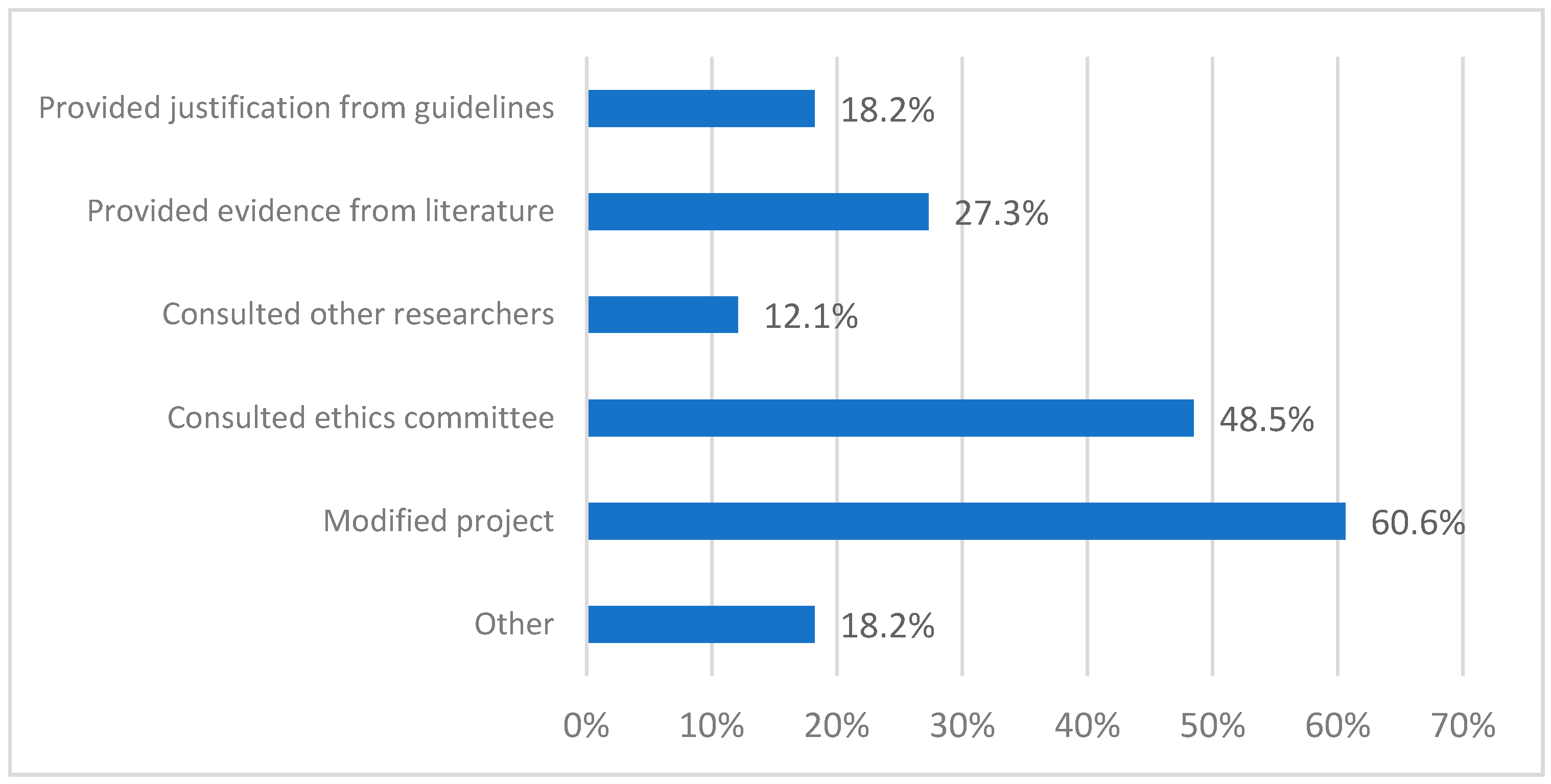
3.4. Researchers’ Responses to the Concerns
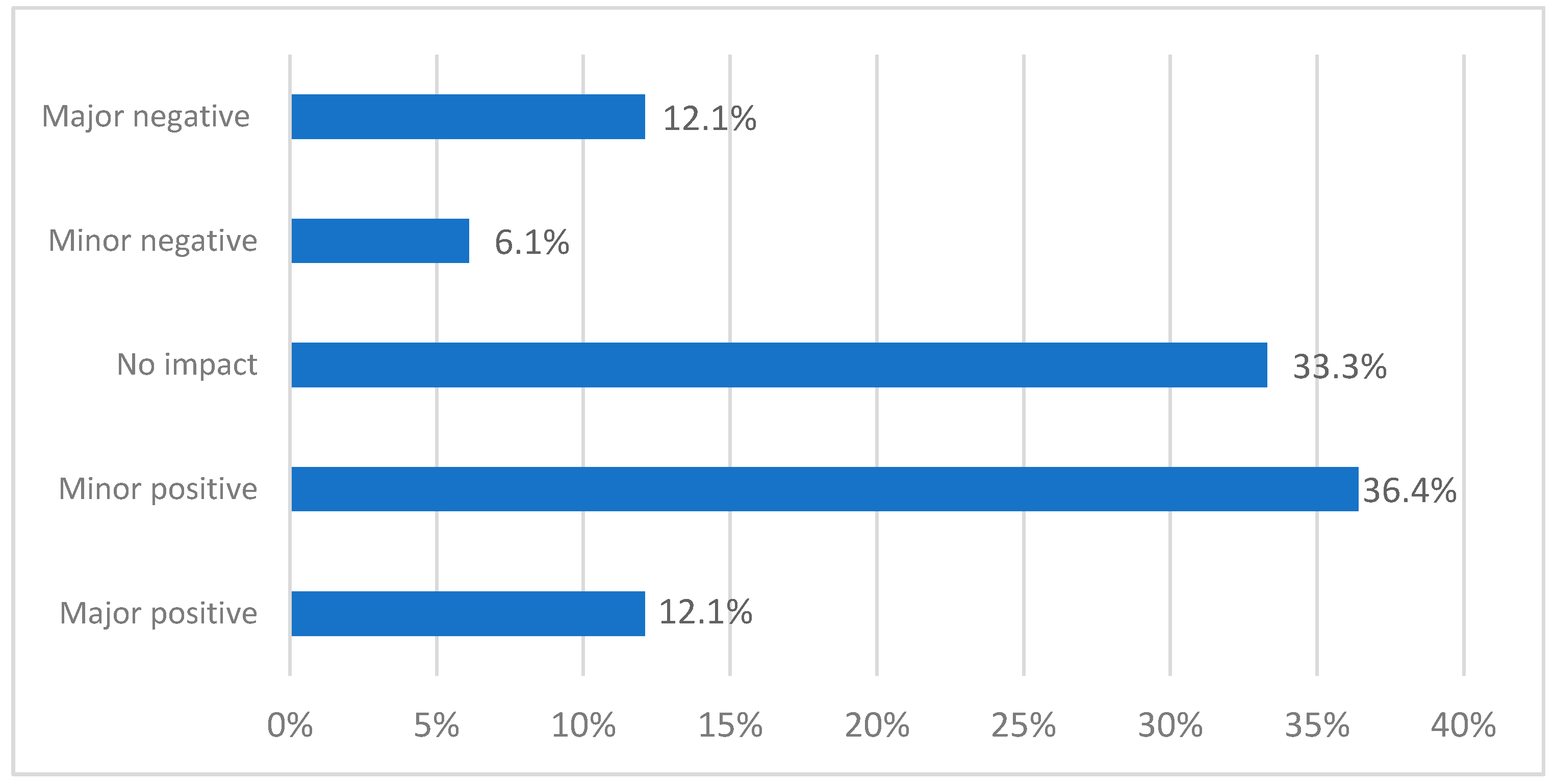
3.5. Impact of the Concerns on the Applications
4. Discussion
Limitations
5. Conclusions
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
Appendix A

{kind=link}
{kind=link}
{kind=link}
| Assessment of Suicide Risk | Group Support after a Suicide Attempt | Feasibility of Online Intervention for Suicidal Ideation | |
|---|---|---|---|
| Description | To develop a scale to assess suicide risk, recovery and psychosocial functioning of adults who recently had attempted suicide. Mixed-methods study including focus groups, an online survey providing item set with individuals with lifetime experience of suicide attempt, and testing the scale with individuals with recent and with lifetime history of attempted suicide | Efficacy of a support group for adult persons who had attempted suicide. Mixed-methods study aiming to examine the participants’ suicidality, mood and hopelessness using validated scales, pre and post-test the support group program, and to collect qualitative data from participants and group facilitators. | Single-group pre- and post-test study evaluating an online social-networking-based intervention for young people aged 16–24, who experience suicidal ideation, and who were clients of a tertiary-level mental health service. Mixed-methods study to examine feasibility, safety and acceptability of the intervention, and exploring potential clinical efficacy. |
| Concerns raised | Potential harm to participants: Asking participants about the relevance of scale items might be distressing or trigger suicidal behaviour. Participant competency: The participant information sheet should draw participants’ attention to their capacity to cope with research participation. Researchers’ responsibilities: Clinicians should actively monitor the focus groups and be available for distressed participants. Confidentiality: Focus group participants might know each other, how to avoid personal disclosures. | Potential harm to participants: Safety of participants exposed to discussions on suicidality and mental health issues. Potential harm to researchers: Impact on researchers conducting detailed interviews with suicidal persons. Participant competency: Whether participants were vulnerable and able to give consent in an objective way. Researchers’ responsibilities: Protocols for responding to participants who seem suicidal or distressed during research participation. | Other concerns: Significance of measuring clinical efficacy in small sample size with no control. |
| Researchers’ response to concerns | Modified ethics application: Clarified project aims and information about capacity to participate in participant information sheets. Provided additional clinical support for focus groups. Provided evidence from literature: Emphasized extensive literature on low risk of distress from being asked about suicide or mental health in vulnerable populations. | Modified ethics application: Clarified suicide safety and referral protocols. Made consent processes clearer and more explicit. Provided justification: Referred to the body of knowledge on value of lived experience perspectives to research on suicide prevention. | Consulted with ethics committee: Argued that the information would be useful and emphasized that the researchers would not over-interpret the data. |
| Study proceeded | Yes | Yes | Yes |
| Impact of concerns | Overall: No impact Negative impacts: greater resourcing requirements, changes in wording and lengthier participant information sheet potentially stigmatizing to participants, and time taken to address comments that were based on misunderstandings. Positive impacts: minor clarifications to participants of nature, risks and study aims. | Minor positive impact. The ethics committee responses focused researchers’ attention on protocols and consent practices, but did not raise issues that they were not already considering. Researchers helped ethics committee to understand that their views of suicidal people were stigmatizing. Duration of ethics process delayed the start of the study. | No impact No changes were needed, only information to justify the design. |
| Duration of ethics approval process | 1–2 months | 5–6 months | 5–6 months |
| Advice to other researchers | Cite the literature on distress regarding asking about suicide or mental health. Expect that the ethics committee provide evidence for their assertions. Allow enough time and resources, expect that it will take a while. Push back against stigmatizing responses, educate the committee if possible. Be open to compromise: concessions that do not harm the quality of the research might result in a more favourable outcome. | Provide ethics committees with the rationale and knowledge available on the use of lived experience in research on suicide prevention. Prepare to answer questions around duty of care and consent but reinforce to the ethics committee the importance of not discounting lived experience in research simply because it is somewhat risk laden or difficult to undertake. | Experience, a strong research team and ensuring the study protocol is as thorough as possible. Talk to others who have had success in this area before. Our team has a lot of experience with this kind of projects and was able to pre-empt many of the possible ethical concerns (e.g., around monitoring and managing risk). The team has a good track record of conducting similar research, which definitely helps. |
References
- ABS. Causes of Death, Australia, 2017; Australian Bureau of Statistics: Canberra, Australia, 2018. Available online: http://tinyurl.com/y2fxq4q8 (accessed on 5 March 2019).
- World Health Organization. Suicide Rates (per 100,000 Population). 2016. Available online: http://www.who.int/gho/mental_health/suicide_rates/en/ (accessed on 5 March 2019).
- Andriessen, K.; Rahman, B.; Draper, B.; Dudley, M.; Mitchell, P.B. Prevalence of exposure to suicide: A meta-analysis of population-based studies. J. Psychiatr. Res. 2017, 88, 113–120. [Google Scholar] [CrossRef] [PubMed]
- Slade, T.; Johnston, A.; Teesson, M.; Whiteford, H.; Burgess, P.; Pirkis, J.; Saw, S. The Mental Health of Australians 2. Report on the 2007 National Survey of Mental Health and Wellbeing; Department of Health and Ageing: Canberra, Australia, 2009; ISBN 1-74186-903-X. Available online: http://tinyurl.com/y2jlhm8o (accessed on 5 March 2019).
- O’Connor, R.C.; Pirkis, J. (Eds.) The International Handbook of Suicide Prevention, 2nd ed.; Wiley-Blackwell: Chichester, UK, 2016; ISBN 978-1-118-90327-8. [Google Scholar] [CrossRef]
- Large, M.; Kaneson, M.; Myles, N.; Myles, H.; Gunaratne, P.; Ryan, C. Meta-analysis of longitudinal cohort studies of suicide risk assessment among psychiatric patients: Heterogeneity in results and lack of improvement over time. PLoS ONE 2016, 11, e0156322. [Google Scholar] [CrossRef] [PubMed]
- Fisher, C.B.; Pearson, J.L.; Kim, S.; Reynolds, C.F. Ethical issues in including suicidal individuals in clinical research. IRB 2002, 24, 9–14. [Google Scholar] [CrossRef] [PubMed]
- Hom, M.A.; Podlogar, M.C.; Stanley, I.H.; Joiner, T.E., Jr. Ethical issues and practical challenges in suicide research. Crisis 2017, 38, 107–114. [Google Scholar] [CrossRef] [PubMed]
- Andriessen, K.; Krysinska, K.; Draper, B.; Dudley, M.; Mitchell, P.B. Harmful or helpful? A systematic review of how those bereaved through suicide experience research participation. Crisis 2018, 39, 364–376. [Google Scholar] [CrossRef] [PubMed]
- Blades, C.A.; Stritzke, W.G.; Page, A.C.; Brown, J.D. The benefits and risks of asking research participants about suicide: A meta-analysis of the impact of exposure to suicide-related content. Clin. Psychol. Rev. 2018, 64, 1–12. [Google Scholar] [CrossRef] [PubMed]
- Mishara, B.L.; Weisstub, D.N. Ethical and legal issues in suicide research. Int. J. Law. Psychiatry 2005, 28, 23–41. [Google Scholar] [CrossRef] [PubMed]
- Commonwealth of Australia. National Statement on Ethical Conduct in Human Research 2007 (Updated 2018); The National Health and Medical Research Council, the Australian Research Council and Universities Australia: Canberra, Australia, 2018; Available online: http://tinyurl.com/y6jfgwn2 (accessed on 5 March 2019).
- Lakeman, R.; Fitzgerald, M. Ethical suicide research: A survey of researchers. Int. J. Ment. Health. Nurs. 2009, 18, 10–17. [Google Scholar] [CrossRef] [PubMed]
- Lakeman, R.; FitzGerald, M. The ethics of suicide research: The views of ethics committee members. Crisis 2009, 30, 13–19. [Google Scholar] [CrossRef] [PubMed]
- Australian Government. The National Suicide Prevention Leadership & Support. Program, 2017. Available online: http://tinyurl.com/yxo2euwb (accessed on 5 March 2019).
- Reifels, L.; Ftanou, M.; Krysinska, K.; Machlin, A.; Robinson, J.; Pirkis, J. Research priorities in suicide prevention: Review of Australian research from 2010–2017 highlights continued need for intervention research. Int. J. Environ. Res. Public. Health 2018, 15, 807. [Google Scholar] [CrossRef] [PubMed]
- IBM Corp. IBM SPSS Statistics for Windows, Version 24.0 [Computer Software]; IBM Corp.: Armonk, NY, USA, 2016. [Google Scholar]
- Bryman, A. Social Research Methods, 4th ed.; Oxford University Press: Oxford, UK, 2012; ISBN 978-0199588053. [Google Scholar]



| Variable | Categories or Range | n (%) Respondents | Median or M, SD |
|---|---|---|---|
| Gender | Female | 19 (57.6%) | - |
| Male | 14 (42.4%) | ||
| Other | 0 (0%) | ||
| Years of experience | <5 | 11 (33.4%) | 5–10 years |
| 5–10 | 15 (45.5%) | ||
| >10 | 7 (21.3%) | ||
| Ethics applications submitted last 5 years (n = 180) | Range: 1–25 | 33 | 2 5.45 (6.41) |
| Ethics applications submitted as Principal Investigator last 5 years (n = 88) | Range: 1–20 | 33 | 1 2.67 (4.02) |
| Outcomes experienced of all applications submitted last 5 years (n = 180) 1 | Approved | 4 (12.1%) | - |
| Minor revision | 24 (72.7%) | ||
| Major revision | 18 (54.5%) | ||
| Not approved | 3 (9.1%) |
| Variable | Categories | n (%) Respondents 1 |
|---|---|---|
| Research type | Social | 4 (12.1%) |
| Biological | 0 (0.0%) | |
| Evaluation | 10 (30.3%) | |
| Intervention | 10 (30.3%) | |
| Epidemiological | 8 (24.2%) | |
| Assessment | 7 (21.2%) | |
| Other | 7 (21.2%) | |
| Focus of the research project | Current or ex-military | 1 (3.0%) |
| Women | 2 (6.1%) | |
| Men | 2 (6.1%) | |
| Offenders | 1 (3.0%) | |
| People who have attempted suicide | 7 (21.2%) | |
| People with substance use problems | 1 (3.0%) | |
| People with physical health problems | 2 (6.1%) | |
| People with mental health problems | 6 (18.2%) | |
| GLBT+ people | 1 (3.0%) | |
| People bereaved by suicide | 6 (18.2%) | |
| People in rural areas | 3 (9.1%) | |
| Culturally and linguistically diverse people | 1 (3.0%) | |
| Indigenous people | 3 (9.1%) | |
| Older adults | 1 (3.0%) | |
| Adults | 10 (30.3%) | |
| Young people | 15 (45.5%) | |
| Children | 0 (0.0%) | |
| None of these groups | 3 (9.1%) | |
| Other | 3 (9.1%) | |
| Setting of the research project | Online | 2 (6.1%) |
| Mental health service | 12 (36.4%) | |
| Emergency department | 1 (3.0%) | |
| Primary care (e.g., general practice) | 2 (6.1%) | |
| Other health service | 3 (9.1%) | |
| Workplace | 0 (0.0%) | |
| Prison | 0 (0.0%) | |
| Tertiary institution | 3 (9.1%) | |
| School | 3 (9.1%) | |
| Community | 12 (36.4%) | |
| No specific type of setting | 5 (15.2%) | |
| Other | 2 (6.1%) |
© 2019 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Andriessen, K.; Reifels, L.; Krysinska, K.; Robinson, J.; Dempster, G.; Pirkis, J. Dealing with Ethical Concerns in Suicide Research: A Survey of Australian Researchers. Int. J. Environ. Res. Public Health 2019, 16, 1094. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph16071094
Andriessen K, Reifels L, Krysinska K, Robinson J, Dempster G, Pirkis J. Dealing with Ethical Concerns in Suicide Research: A Survey of Australian Researchers. International Journal of Environmental Research and Public Health. 2019; 16(7):1094. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph16071094
Chicago/Turabian StyleAndriessen, Karl, Lennart Reifels, Karolina Krysinska, Jo Robinson, Georgia Dempster, and Jane Pirkis. 2019. "Dealing with Ethical Concerns in Suicide Research: A Survey of Australian Researchers" International Journal of Environmental Research and Public Health 16, no. 7: 1094. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph16071094