The Development of Keratopathy after Surgery-Indicated Chronic Rhinosinusitis: A Population-Based Cohort Study

 , , ,
, , , 
Abstract
:1. Introduction
2. Materials and Methods
2.1. Data Source
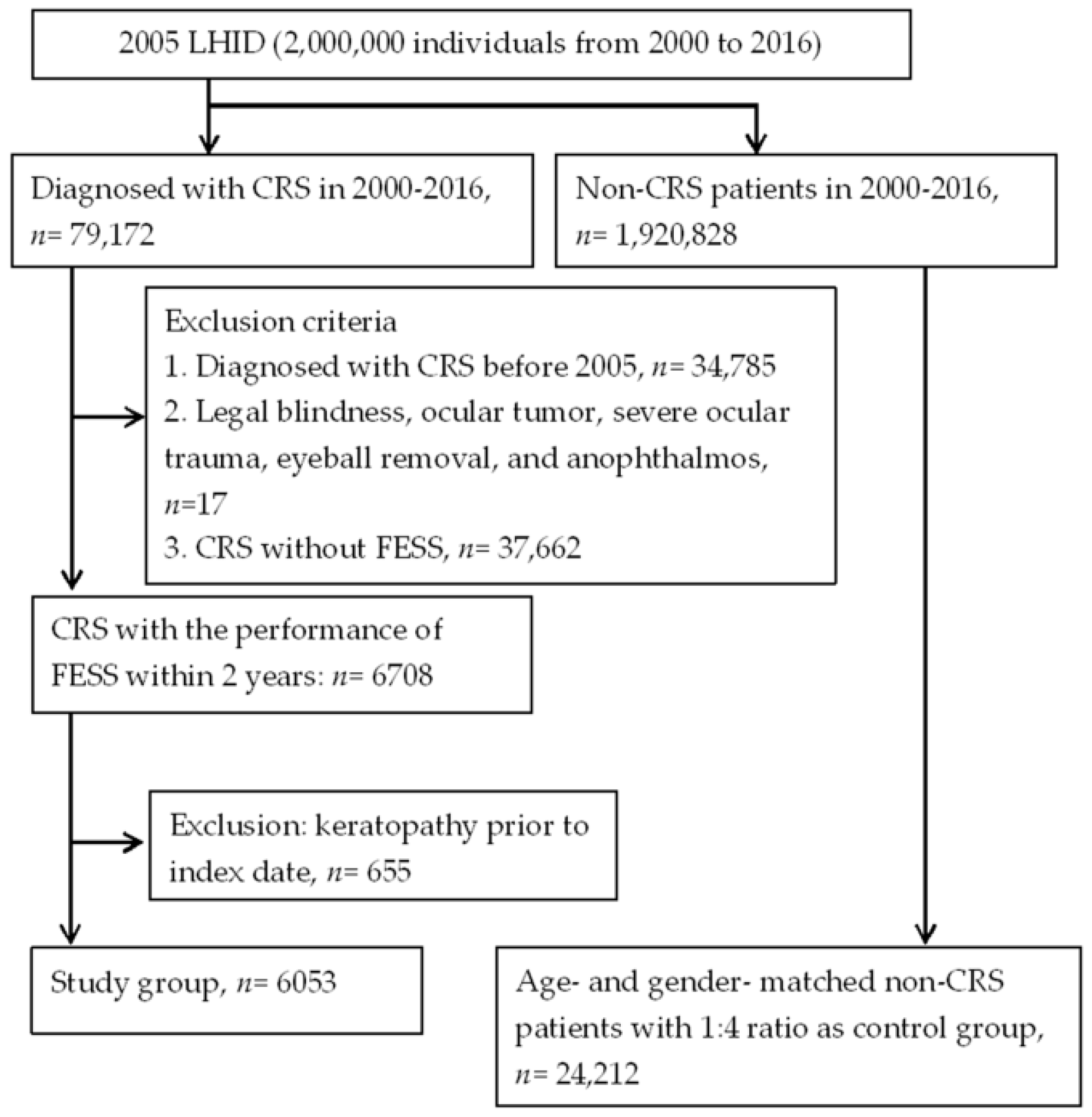
2.2. Patient Selection
2.3. Main Outcome Measurement
2.4. Demographic Variables and Co-Morbidities
2.5. Statistical Analysis
3. Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Conflicts of Interest
References
- Siedek, V.; Stelter, K.; Betz, C.S.; Berghaus, A.; Leunig, A. Functional endoscopic sinus surgery—A retrospective analysis of 115 children and adolescents with chronic rhinosinusitis. Int. J. Pediatr. Otorhinolaryngol. 2009, 73, 741–745. [Google Scholar] [CrossRef]
- Gulati, S.P.; Chaudhry, D.; Kalra, V.; Wadhera, R.; Garg, A. The role of functional endoscopic sinus surgery (fess) in patients with asthma with chronic sinusitis. Indian J. Otolaryngol. Head Neck Surg. 2008, 60, 152–155. [Google Scholar] [CrossRef] [PubMed]
- Anselmo-Lima, W.T.; Ferreira, M.D.; Valera, F.C.; Rossato, M.; de Mello, V.R.; Demarco, R.C. Histological evaluation of maxillary sinus mucosa after functional endoscopic sinus surgery. Am. J. Rhinol. 2007, 21, 719–724. [Google Scholar] [CrossRef] [PubMed]
- Poletti, S.C.; Cuevas, M.; Weile, S.; Hummel, T. Trigeminal sensitivity in chronic rhinosinusitis: Topographical differences and the effect of surgery. Rhinology 2017, 55, 70–74. [Google Scholar] [CrossRef] [PubMed]
- Saliba, J.; Fnais, N.; Tomaszewski, M.; Carriere, J.S.; Frenkiel, S.; Frasnelli, J.; Tewfik, M.A. The role of trigeminal function in the sensation of nasal obstruction in chronic rhinosinusitis. Laryngoscope 2016, 126, E174–E178. [Google Scholar] [CrossRef] [PubMed]
- Constantin, F.; Niculescu, P.A.; Petre, O.; Balasa, D.; Tunas, A.; Rusu, I.; Lupascu, M.; Orodel, C. Orbital cellulitis and brain abscess—Rare complications of maxillo-spheno-ethmoidal rhinosinusitis. Rom. J. Ophthalmol. 2017, 61, 133–136. [Google Scholar] [CrossRef] [PubMed]
- Fokkens, W.J.; Lund, V.J.; Mullol, J.; Bachert, C.; Alobid, I.; Baroody, F.; Cohen, N.; Cervin, A.; Douglas, R.; Gevaert, P.; et al. EPOS 2012: European position paper on rhinosinusitis and nasal polyps 2012. A summary for otorhinolaryngologists. Rhinology 2012, 50, 1–12. [Google Scholar] [CrossRef] [PubMed]
- Tan, B.K.; Lane, A.P. Endoscopic sinus surgery in the management of nasal obstruction. Otolaryngol. Clin. North Am. 2009, 42, 227–240. [Google Scholar] [CrossRef] [PubMed]
- Ramakrishnan, V.R.; Kennedy, D.W. Advances in the surgical management of chronic sinusitis and nasal polyps. Curr. Allergy Asthma Rep. 2011, 11, 220–229. [Google Scholar] [CrossRef] [PubMed]
- Welch, K.C.; Stankiewicz, J.A. A contemporary review of endoscopic sinus surgery: Techniques, tools, and outcomes. Laryngoscope 2009, 119, 2258–2268. [Google Scholar] [CrossRef]
- Barac, A.; Pekmezovic, M.; Spiric, V.T.; Trivic, A.; Marinkovic, J.; Pekic, S.; Arsenijevic, V.A. Chronic rhinosinusitis: Association of recalcitrant nasal polyposis and fungal finding in polyp’s single-cell suspension. Euro. Arch. Otorhinolaryngol. 2015, 272, 3727–3734. [Google Scholar] [CrossRef] [PubMed]
- Brooks, S.G.; Trope, M.; Blasetti, M.; Doghramji, L.; Parasher, A.; Glicksman, J.T.; Kennedy, D.W.; Thaler, E.R.; Cohen, N.A.; Palmer, J.N.; et al. Preoperative lund-mackay computed tomography score is associated with preoperative symptom severity and predicts quality-of-life outcome trajectories after sinus surgery. Int. Forum Allergy Rhinol. 2018, 8, 668–675. [Google Scholar] [CrossRef] [PubMed]
- Chang, Y.S.; Chen, P.L.; Hung, J.H.; Chen, H.Y.; Lai, C.C.; Ou, C.Y.; Chang, C.M.; Wang, C.K.; Cheng, H.C.; Tseng, S.H. Orbital complications of paranasal sinusitis in Taiwan, 1988 through 2015: Acute ophthalmological manifestations, diagnosis, and management. PLoS ONE 2017, 12, e0184477. [Google Scholar] [CrossRef] [PubMed]
- Cazzavillan, A.; Gaini, R.M.; Pignataro, L.; Piacentini, E.; Leo, G. Treatment of rhinosinusitis: The role of surgery. Int. J. Immunopathol. Pharmacol. 2010, 23, 74–77. [Google Scholar] [PubMed]
- Rossi, P.; Urbani, C.; Donelli, G.; Pozio, E. Resolution of microsporidial sinusitis and keratoconjunctivitis by itraconazole treatment. Am. J. ophthalmol. 1999, 127, 210–212. [Google Scholar] [CrossRef]
- Cao, Y.; Zhang, W.; Wu, J.; Zhang, H.; Zhou, H. Peripheral ulcerative keratitis associated with autoimmune disease: Pathogenesis and treatment. J. Ophthalmol. 2017, 2017, 7298026. [Google Scholar] [CrossRef] [PubMed]
- Maertzdorf, J.; Osterhaus, A.D.; Verjans, G.M. Il-17 expression in human herpetic stromal keratitis: Modulatory effects on chemokine production by corneal fibroblasts. J. Immunol. 2002, 169, 5897–5903. [Google Scholar] [CrossRef] [PubMed]
- Ramakrishnan, V.R.; Gonzalez, J.R.; Cooper, S.E.; Barham, H.P.; Anderson, C.B.; Larson, E.D.; Cool, C.D.; Diller, J.D.; Jones, K.; Kinnamon, S.C. Rna sequencing and pathway analysis identify tumor necrosis factor alpha driven small proline-rich protein dysregulation in chronic rhinosinusitis. Am. J. Rhinol. Allergy 2017, 31, 283–288. [Google Scholar] [CrossRef] [PubMed]
- Olcott, C.M.; Han, J.K.; Cunningham, T.D.; Franzese, C.B. Interleukin-9 and interleukin-17c in chronic rhinosinusitis. Int. Forum Allergy Rhinol. 2016, 6, 841–847. [Google Scholar] [CrossRef] [PubMed]
- Lee, B.; Cai, C.X.; Srikumaran, D.; Woreta, F.A. Severe achromobacter xylosoxidans keratitis with deep corneal involvement. Am. J. Ophthalmol. Case Rep. 2018, 11, 128–130. [Google Scholar] [CrossRef] [PubMed]
- Wang, J.Y.; Wang, D.Q.; Qi, X.L.; Cheng, J.; Xie, L.X. Modified ulcer debridement in the treatment of the superficial fungal infection of the cornea. Int. J. Ophthalmol. 2018, 11, 223–229. [Google Scholar] [PubMed]
- Djalilian, A.R.; Smith, J.A.; Walsh, T.J.; Malech, H.L.; Robinson, M.R. Keratitis caused by candida glabrata in a patient with chronic granulomatous disease. Am. J. Ophthalmol. 2001, 132, 782–783. [Google Scholar] [CrossRef]
- Clark, J.D.; Fernandez de Castro, J.P.; Compton, C.; Lee, H.; Nunery, W. Orbital cellulitis and corneal ulcer due to cedecea: First reported case and review of the literature. Orbit 2016, 35, 140–143. [Google Scholar] [CrossRef] [PubMed]
- Drago, L.; Pignataro, L.; Torretta, S. Microbiological aspects of acute and chronic pediatric rhinosinusitis. J. Clin. Med. 2019, 8, 149. [Google Scholar] [CrossRef] [PubMed]
- Biswas, J.; Babu, K.; Gopal, L.; Krishnakumar, S.; Suresh, S.; Ramakrishnan, S. Ocular manifestations of wegener’s granulomatosis. Analysis of nine cases. Indian J. Ophthalmol. 2003, 51, 217–223. [Google Scholar] [PubMed]
- Tsubota, K.; Yokoi, N.; Shimazaki, J.; Watanabe, H.; Dogru, M.; Yamada, M.; Kinoshita, S.; Kim, H.M.; Tchah, H.W.; Hyon, J.Y.; et al. New perspectives on dry eye definition and diagnosis: A consensus report by the asia dry eye society. Ocul. Surf. 2017, 15, 65–76. [Google Scholar] [CrossRef] [PubMed]
- Milner, M.S.; Beckman, K.A.; Luchs, J.I.; Allen, Q.B.; Awdeh, R.M.; Berdahl, J.; Boland, T.S.; Buznego, C.; Gira, J.P.; Goldberg, D.F.; et al. Dysfunctional tear syndrome: Dry eye disease and associated tear film disorders—New strategies for diagnosis and treatment. Curr. Opin. Ophthalmol. 2017, 27 (Suppl. 1), 3–47. [Google Scholar] [CrossRef]
- Krontz, D.P.; Wood, T.O. Corneal decompensation following acute angle-closure glaucoma. Ophthalmic Surg. 1988, 19, 334–338. [Google Scholar] [PubMed]
- Inoue, K.; Okugawa, K.; Kato, S.; Inoue, Y.; Tomita, G.; Oshika, T.; Amano, S. Ocular factors relevant to anti-glaucomatous eyedrop-related keratoepitheliopathy. J. Glaucoma 2003, 12, 480–485. [Google Scholar] [CrossRef] [PubMed]
- Wensing, B.; Mochizuki, M.; De Boer, J.H. Clinical characteristics of herpes simplex virus associated anterior uveitis. Ocular Immunol. Inflamm. 2018, 26, 333–337. [Google Scholar] [CrossRef] [PubMed]
- Chan, N.S.; Chee, S.P.; Caspers, L.; Bodaghi, B. Clinical features of cmv-associated anterior uveitis. Ocular Immunol. Inflamm. 2018, 26, 107–115. [Google Scholar] [CrossRef] [PubMed]



{kind=link}
{kind=link}
| Baseline Characteristics | Study, n = 6053 | Control, n = 24,212 | p Value |
|---|---|---|---|
| Age | 1.0000 | ||
| <40 | 2177 (35.97%) | 8708 (35.97%) | |
| 40–59 | 2643 (43.66%) | 10,572 (43.66%) | |
| 60–79 | 1168 (19.3%) | 4672 (19.3%) | |
| ≥80 | 65 (1.07%) | 260 (1.07%) | |
| Sex | 1.0000 | ||
| Male | 3812 (62.98%) | 15,248 (62.98%) | |
| Female | 2241 (37.02%) | 8964 (37.02%) | |
| Co-morbidities | |||
| Hypertension | 1662 (27.46%) | 5654 (23.35%) | <0.0001 |
| Diabetes mellitus | 823 (13.6%) | 2838 (11.72%) | 0.0047 |
| Ischemic heart diseases | 634 (10.47%) | 1901 (7.85%) | <0.0001 |
| Hyperlipidemia | 1466 (24.22%) | 4736 (19.56%) | <0.0001 |
| Heart failure | 223 (3.68%) | 675 (2.79%) | 0.0002 |
| Peripheral vascular disease | 165 (2.73%) | 554 (2.29%) | 0.0454 |
| Cerebrovascular disease | 432 (7.14%) | 1408 (5.82%) | 0.0001 |
| Dementia | 37 (0.61%) | 167 (0.69%) | 0.5045 |
| Chronic pulmonary diseases | 1701 (28.1%) | 3920 (16.19%) | <0.0001 |
| Rheumatic disease | 154 (2.54%) | 414 (1.71%) | <0.0001 |
| Peptic ulcer disease | 1839 (30.38%) | 5352 (22.1%) | <0.0001 |
| DED | 401 (6.62%) | 1024 (4.23%) | <0.0001 |
| Uveitis | 54 (0.89%) | 179 (0.74%) | 0.2237 |
| Glaucoma | 161 (2.66%) | 386 (1.59%) | <0.0001 |
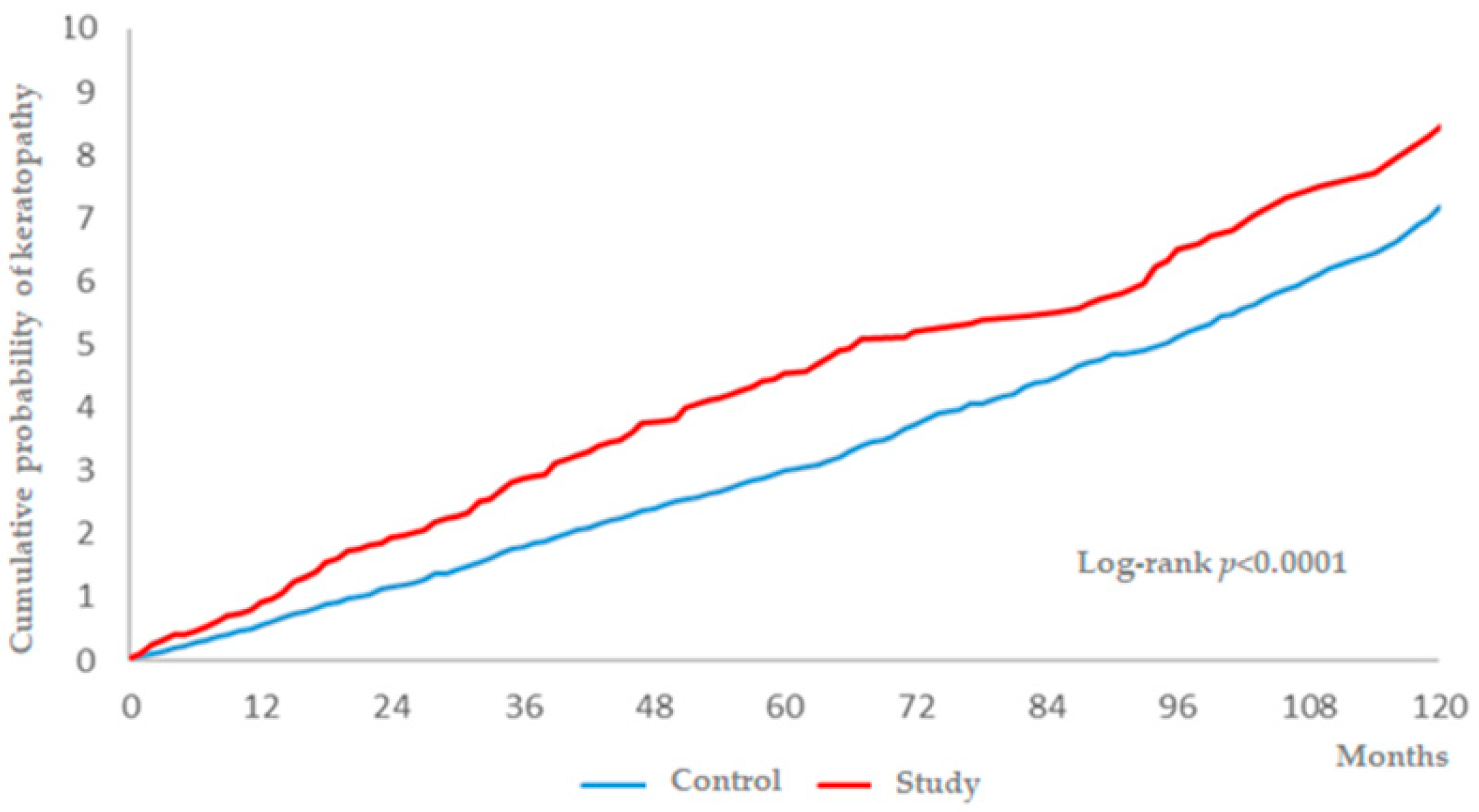
| Incidence | Study, n = 6053 | Control, n = 24,212 |
|---|---|---|
| Follow-up person months | 310,709 | 1,258,744 |
| New keratopathy events | 231 | 695 |
| Incidence rate * (95% CI) | 74.35 (65.35–84.58) | 55.21 (51.26–59.48) |
| Crude Relative risk (95% CI) | 1.345 (1.159–1.561) | Reference |
| Variable | aHR (95% CI) |
|---|---|
| Surgery-indicated CRS | 1.208 (1.038–1.406) |
| Age (Reference: 40–59) | |
| <40 | 1.044 (0.885–1.231) |
| 60–79 | 1.487 (1.249–1.77) |
| ≥80 | 1.06 (0.535–2.099) |
| Sex (Reference: Female) | |
| Male | 0.648 (0.568–0.739) |
| Co-morbidities | |
| Hypertension | 1.235 (1.034–1.475) |
| Diabetes mellitus | 0.946 (0.771–1.161) |
| Ischemic heart diseases | 0.983 (0.783–1.235) |
| Hyperlipidemia | 1.085 (0.906–1.300) |
| Heart failure | 0.852 (0.595–1.219) |
| Peripheral vascular disease | 1.297 (0.921–1.827) |
| Cerebrovascular disease | 0.953 (0.732–1.241) |
| Dementia | 0.874 (0.427–1.792) |
| Chronic pulmonary diseases | 1.335 (1.142–1.561) |
| Rheumatic disease | 1.261 (0.874–1.821) |
| Peptic ulcer disease | 1.105 (0.946–1.292) |
| DED | 2.085 (1.668–2.607) |
| Uveitis | 1.414 (0.792–2.524) |
| Glaucoma | 1.334 (0.93–1.914) |
| Subgroups | Incidence Rate (95% CI) of Keratopathy | aHR (95% CI) | |
|---|---|---|---|
| Study | Control | ||
| Sex subgroups | |||
| Male | 55.88 (46.39–67.3) | 44.87 (40.47–49.76) | 1.14 (0.919–1.415) |
| Female | 107.09 (89.54–128.07) | 73.39 (65.94–81.69) | 1.287 (1.038–1.595) |
| p for interaction | 0.5209 | ||
| Age subgroups (at index date) | |||
| <40 | 52.03 (40.56–66.74) | 44.56 (38.97–50.94) | 1.117 (0.838–1.488) |
| 40–59 | 72.26 (59.34–87.99) | 48.89 (43.42–55.04) | 1.295 (1.024–1.637) |
| 60–79 | 125.9 (98.91–160.26) | 96.41 (84.02–110.63) | 1.148 (0.862–1.527) |
| ≥80 | 189.49 (71.12–504.88) | 53.07 (22.09–127.49) | 12.006 (1.004–143.496) |
| p for interaction | 0.4097 | ||
© 2019 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Hsu, H.-J.; Lee, C.-Y.; Yang, K.-L.; Chen, H.-C.; Sun, C.-C.; Huang, J.-Y.; Lin, H.-Y.; Yang, S.-F. The Development of Keratopathy after Surgery-Indicated Chronic Rhinosinusitis: A Population-Based Cohort Study. Int. J. Environ. Res. Public Health 2019, 16, 1218. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph16071218
Hsu H-J, Lee C-Y, Yang K-L, Chen H-C, Sun C-C, Huang J-Y, Lin H-Y, Yang S-F. The Development of Keratopathy after Surgery-Indicated Chronic Rhinosinusitis: A Population-Based Cohort Study. International Journal of Environmental Research and Public Health. 2019; 16(7):1218. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph16071218
Chicago/Turabian StyleHsu, Hung-Jui, Chia-Yi Lee, Kun-Lin Yang, Hung-Chi Chen, Chi-Chin Sun, Jing-Yang Huang, Hung-Yu Lin, and Shun-Fa Yang. 2019. "The Development of Keratopathy after Surgery-Indicated Chronic Rhinosinusitis: A Population-Based Cohort Study" International Journal of Environmental Research and Public Health 16, no. 7: 1218. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph16071218