Factors Correlating to the Development of Hepatitis C Virus Infection in Hemodialysis Patients—Findings Mainly from Asiatic Populations: A Systematic Review and Meta-Analysis

Abstract
:1. Introduction
2. Materials and Methods
2.1. Literature Search Strategy
2.2. Inclusion and Exclusion Criteria
2.3. Data Extraction
2.4. Sensitivity Analysis
2.5. Statistical Analysis
3. Results
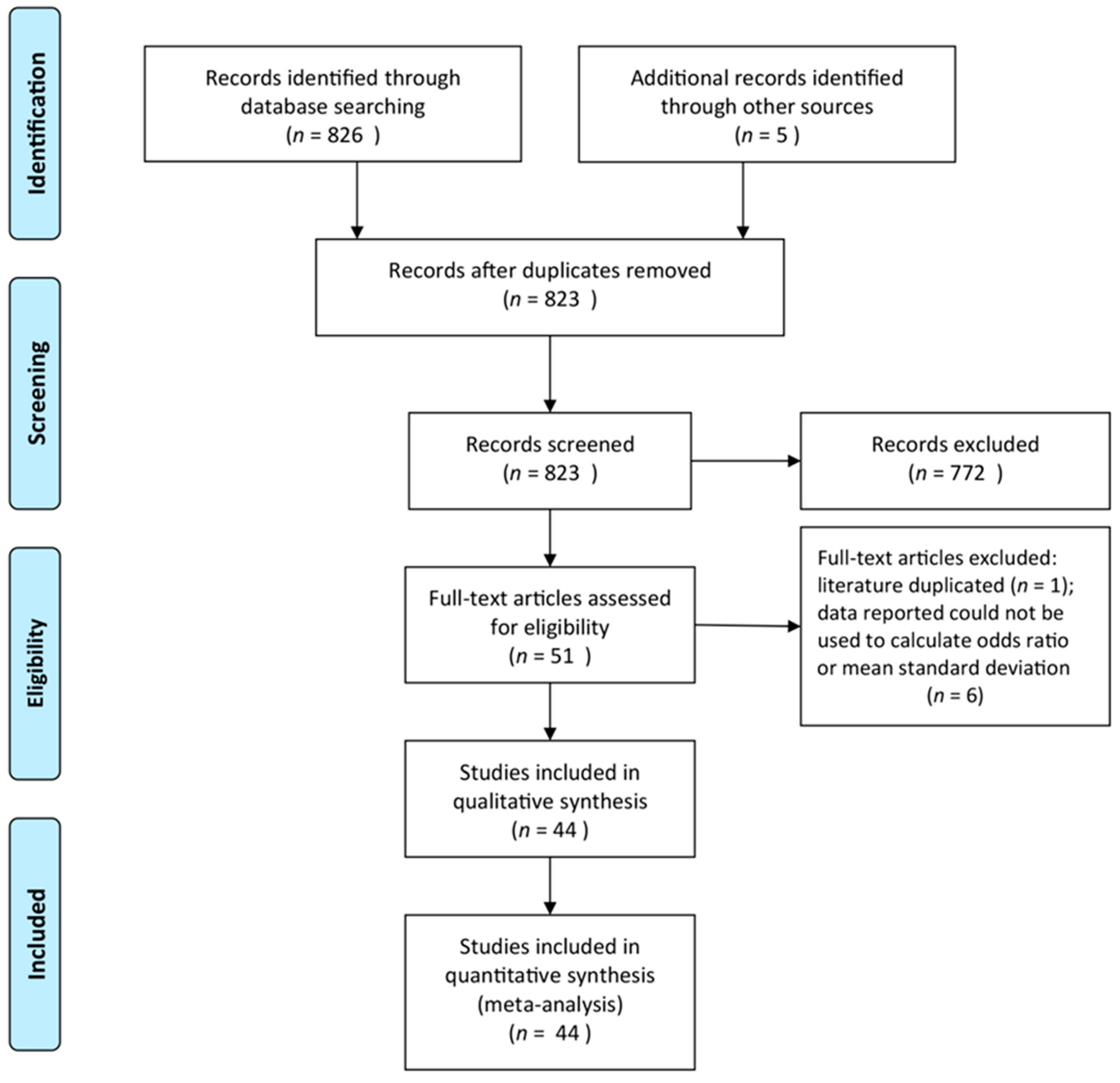
3.1. Literature Search
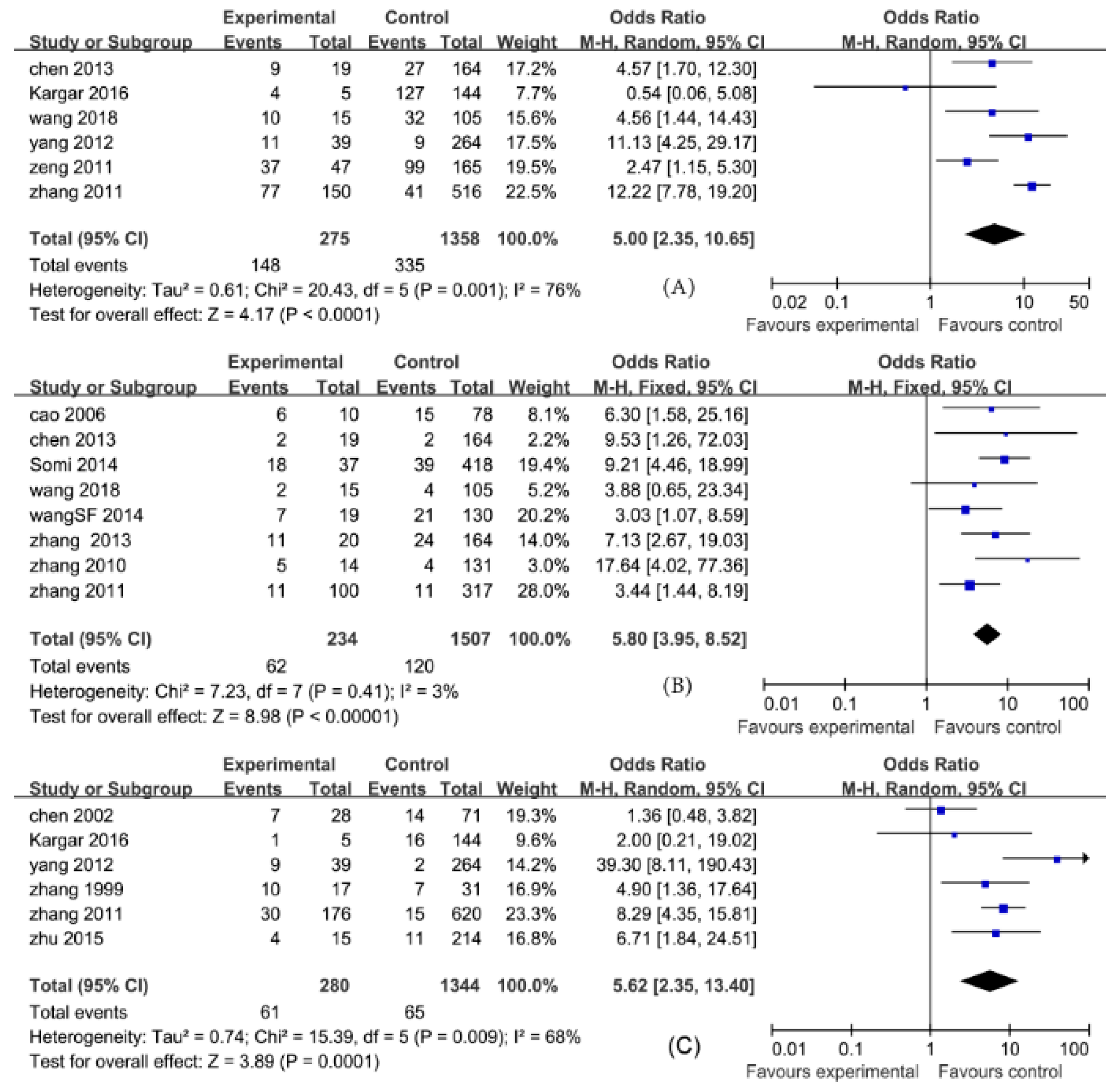
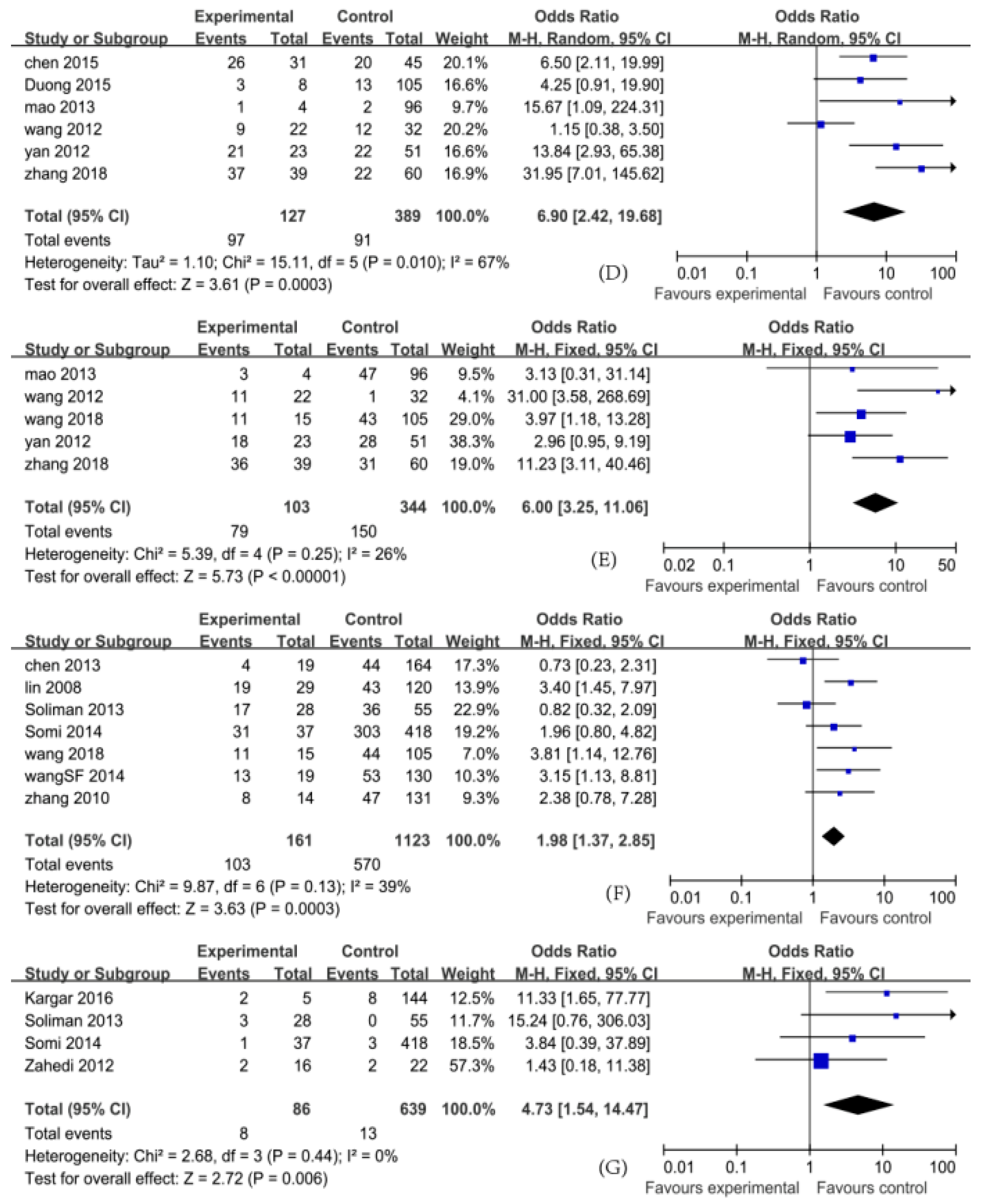
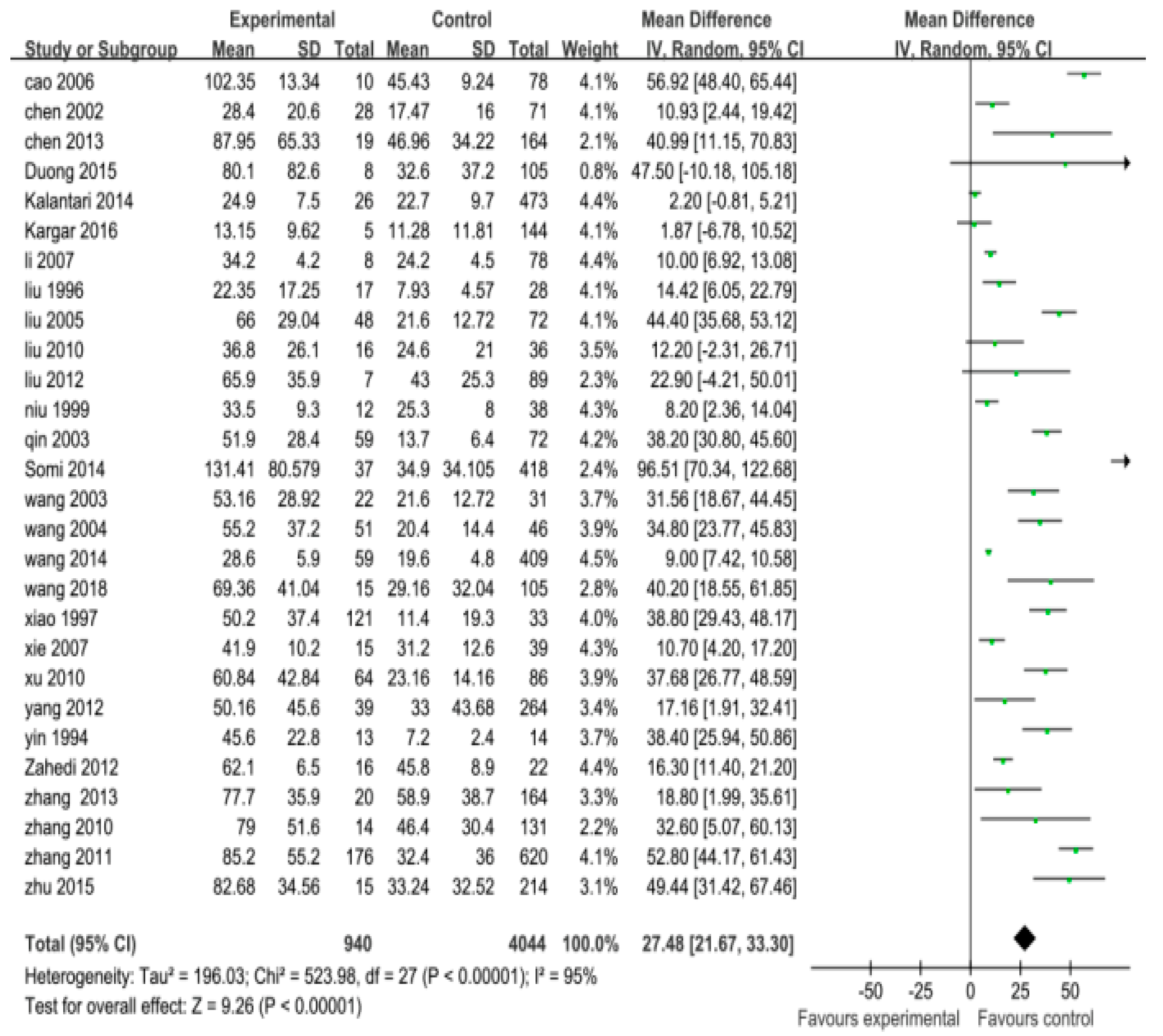
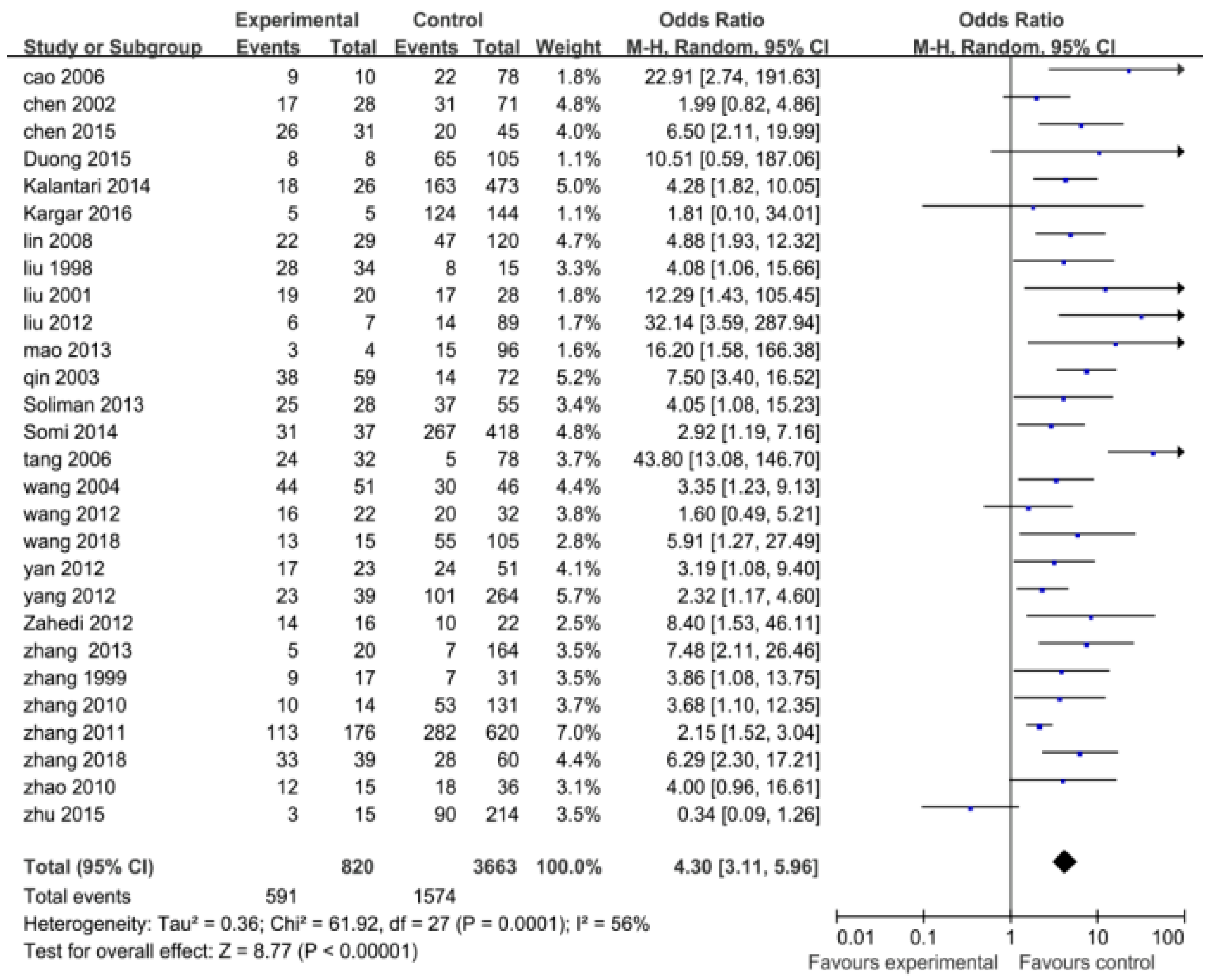
3.2. Results of Pooled ORs or MDs
3.3. Results of Rank Correlation Analysis
3.4. Results of Heterogeneity Evaluation
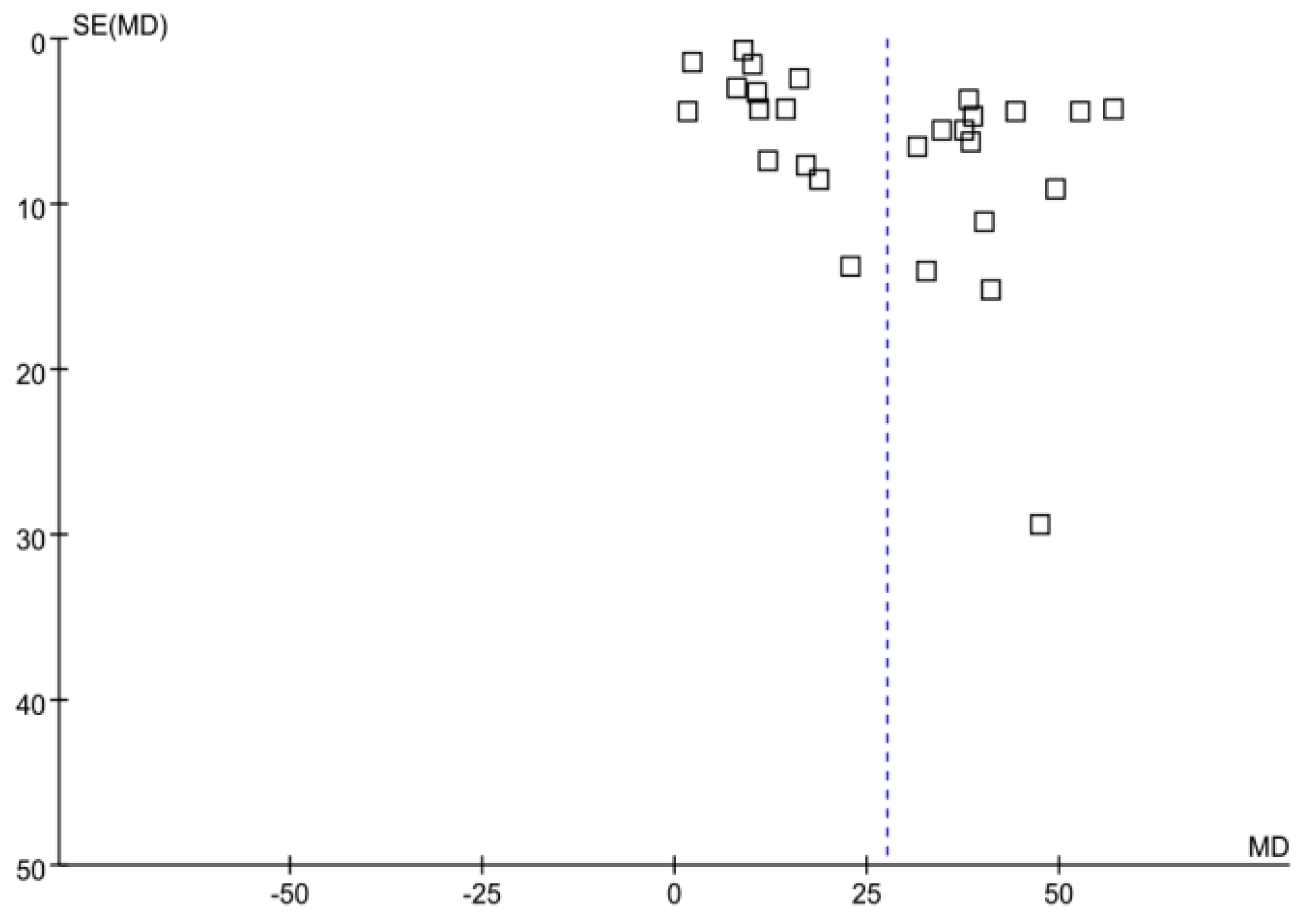
3.5. Publication Bias
3.6. Sensitivity Analysis
4. Discussion
5. Conclusions
Author Contributions
Conflicts of Interest
List of Abbreviations
| HBV | hepatitis B virus |
| HCV | hepatitis C virus |
| CI | confidence interval |
| MD | mean difference |
| OR | odds ratio |
| ALT | alanine aminotransferase |
References
- Fleming, G.M. Renal replacement review: Past, present and future. Organogenesis 2011, 7, 2–12. [Google Scholar] [CrossRef] [PubMed]
- Fresenius Medical Care. ESRD Patients in 2012: A Global Perspective; Fresenius Medical Care AG & Co. KGaA, Hof a.d. Saale: Bad Homburg, Germany, 2012. [Google Scholar]
- Santos, M.G.; Danguilan, R.A.; Que, E.T.; Balmaceda, R.P.; Padilla, B.S. Prevalence of hepatitis B and hepatitis C in hemodialysis patients. Nephrology 1998, 4, 101–104. [Google Scholar] [CrossRef]
- Zahedi, M.J.; Moghaddam, S.D.; Alavian, S.M.; Dalili, M. Seroprevalence of Hepatitis Viruses B, C, D and HIV Infection Among Hemodialysis Patients in Kerman Province, SouthEast Iran. Hepat. Mon. 2012, 12, 339. [Google Scholar] [CrossRef] [PubMed]
- Al-Jamal, M.; Al-Qudah, A.; Al-Shishi, K.F.; Al-Sarayreh, A.; Al-Quraan, L. Hepatitis C virus (HCV) infection in hemodialysis patients in the south of Jordan. Saudi J. Kidney Dis. Transpl. 2009, 20, 488. [Google Scholar] [PubMed]
- Hinrichsen, H.; Leimenstoll, G.; Stegen, G.; Schrader, H.; Fölsch, U.R.; Schmidt, W.E. Prevalence and risk factors of hepatitis C virus infection in haemodialysis patients: A multicentre study in 2796 patients. Gut 2002, 52, 429–433. [Google Scholar] [CrossRef]
- Zhuang, H. Current situation and objective of hepatitis b prevention and treatment in China. Chin. J. Pract. Med. 2008, 47, 793–795. [Google Scholar]
- Sun, J.; Yu, R.; Zhu, B.; Wu, J.; Larsen, S.; Zhao, W. Hepatitis C infection and related factors in hemodialysis patients in China: Systematic review and meta-analysis. Ren. Fail 2009, 31, 610–620. [Google Scholar] [CrossRef] [PubMed]
- World Health Organization, Expanded Programme on Immunization, Global Advisory Group. Meeting (14th: 1991: Antalya, Turkey) & WHO Expanded Programme on Immunization. (1992). Expanded Programme on Immunization: Report of the 14th Global Advisory Group, 14–18 October 1991, Antalya, Turkey. Available online: http://apps.who.int/iris/handle/10665/61561 (accessed on 16 May 2018).
- Zanetti, A.R.; Mariano, A.; Romanò, L.; D’Amelio, R.; Chironna, M.; Coppola, R.C.; Cuccia, M.; Mangione, R.; Marrone, F.; Negrone, F.S.; et al. Long-term immunogenicity of hepatitis B vaccination and policy for booster: An Italian multicentre study. Lancet 2005, 366, 1379–1384. [Google Scholar] [CrossRef]
- Liang, X.; Bi, S.; Yang, W.; Wang, L.; Cui, G.; Cui, F.; Zhang, Y.; Liu, J.; Gong, X.; Chen, Y.; et al. Epidemiological serosurvey of hepatitis B in China declining HBV prevalence due to hepatitis B vaccination. Vaccine 2009, 27, 6550–6557. [Google Scholar] [CrossRef] [PubMed]
- Liang, X.; Bi, S.; Yang, W.; Wang, L.; Cui, G.; Cui, F.; Zhang, Y.; Liu, J.; Gong, X.; Chen, Y.; et al. Evaluation of the impact of hepatitis B vaccination among children born during 1992–2005 in China. J. Infect. Dis. 2009, 200, 39–47. [Google Scholar] [CrossRef]
- Kumagai, J.; Komiya, Y.; Tanaka, J.; Katayama, K.; Tatsukawa, Y.; Yorioka, N.; Miyakawa, Y.; Yoshizawa, H. Hepatitis C virus infection in 2744 hemodialysis patients followed regularly at nine centers in Hiroshima during November 1999 through February 2003. J. Med. Virol. 2005, 76, 498–502. [Google Scholar] [CrossRef]
- Abdulkarim, A.S.; Zein, N.N.; Germer, J.J.; Kolbert, C.P.; Kabbani, L.O.; Krajnik, K.L.; Hola, A.L.; Agha, M.N.; Tourogman, M.O.; Persing, D.H. Hepatitis C virus genotypes and hepatitis G virus in hemodialysis patients from Syria: Identification of two novel hepatitis C virus subtypes. Am. J. Trop. Med. Hyg. 1998, 59, 571–576. [Google Scholar] [CrossRef]
- Tanaka, J.; Katayama, K.; Matsuo, J.; Akita, T.; Asao, T.; Ohisa, M.; Tsuchiya, S.; Yorioka, N. The Association of Hepatitis C Virus Infection with the Prognosis of Chronic Hemodialysis Patients: A Retrospective Study of 3064 Patients Between 1999 and 2010. J. Med. Virol. 2015, 87, 1558–1564. [Google Scholar] [CrossRef]
- Alter, M.J.; Favero, M.S.; Maynard, J.E. Impact of infection control strategics on the incidence of dialysis associated hepatitis in the United States. J. Infect. Dis. 1998, 153, 1149–1151. [Google Scholar] [CrossRef]
- Improving Global Outcomes (KDIGO) Transplant Work Group. KDIGO Clinical practice guideline for the care of kidney transplant recipients. Am. J. Transpl. 2009, 9, 155–158. [Google Scholar]
- Wang, N.S.; Zhu, Y.G.; Zhou, S.S.; Tang, L.Q.; Liao, L.T. Logisic Analysis of Risk Factors of Hepatitis C Virus in Patients with Maintenance Hemodialysis. Chin. J. Hosp. Infect. 2002, 12, 169–171. [Google Scholar]
- Zhang, Y.Z.; Shang, Y.Q.; Su, W.; Zhao, X.Y. Clinical analysis of HCV infection in hemodialysis patients. Jilin Med. 2012, 33, 476–479. [Google Scholar]
- Chen, X.J.; He, Y.C.; Wan, Q.J. The risk factors of hepatitis C virus infection in maintenance hemodialysis patients. Chin. J. Blood Purif. 2013, 12, 617–4620. [Google Scholar]
- Edey, M.; Barraclough, K.; Johnson, D.W. Review article: Hepatitis B and dialysis. Nephrology 2010, 15, 9. [Google Scholar] [CrossRef] [PubMed]
- Kheirabad, A.K.; Kargar, F.B.; Ghasemzadeh, I. Hepatitis C and G Virus Infection Prevalence Among Hemodialysis Patients and Associated Risk Factors in the Hormozgan Province of Southern Iran. Hepat. Mon. 2016, 16, e40375. [Google Scholar] [CrossRef]
- Zhang, X.L.; Fu, W.L. Evaluation of the prevalence HCV infection in hemodialysis patients and its infective risk factors. Chin. J. Nosocomiol. 1999, 9, 77–79. [Google Scholar]
- Cao, Y.L.; Wang, S.X.; Guo, P.; Liu, H. Hepatitis C virus infection in maintenance hemodialysis patients. Chin. J. Blood Purif. 2006, 5, 430–432. [Google Scholar]
- Chen, L.; Xuewang, L.I.; Peng, L. Hepatitis B and C virus infection in uremia patients on chronic hemodialysis. Chin. J. Pract. Med. 2002, 22, 407–409. [Google Scholar]
- Liu, G.; Fu, B.Y.; Wei, J.R.; Sun, B.; Zhang, Q.S. Study on HCV infection in hemodialysis patients. Chin. J. Metall. Ind. Med. 1996, 13, 77–79. [Google Scholar]
- Liu, H.L.; Li, G.G.; Duan, X.F.; Cai, Q. Clinical Characteristics of hepatitis B and C viral infection in hemodialysis patients. Chin. J. Intern. Med. 1998, 37, 758–4761. [Google Scholar]
- Liu, J.M. Clinical study on 120 patients with maintenance hemodialysis complicated with viral hepatitis. J. Nongken Med. 2005, 27, 194–196. [Google Scholar]
- Wang, L.; Hu, C.Y.; Li, X.Y. Clinical investigation of the maintenance hemodialysis patients complicated with viral hepatitis. Chin. J. Blood Purif. 2003, 2, 24–26. [Google Scholar]
- Wang, Z.H.; Chen, N.; Zhu, P.; Qing, Y.; Shen, P.Y.; Wang, G.Y. Prevalence of hepatitis B and C viral infection in uremia patients treated by chronic hemodialysis. J. Diagn. Concepts Pr. 2004, 3, 9–11. [Google Scholar]
- Xiao, G.Q.; Ji, D.X.; Chen, C.H.; Huan, H.D.; Xie, H.L.; Liu, Y.; Liu, Z.H.; Li, L.S. Study on HCV infection in hemodialysis patients and dialysis center staff. J. Nephrol. Dialy Transpl. 1997, 6, 525–530. [Google Scholar]
- Zhao, H.; Chang, M.; Xing, S.Q. Analysis of hepatitis virus infection in hemodialysis patients. Chin. J. Blood Purif. 2008, 7, 207–209. [Google Scholar]
- Lin, Y.Y.; Yu, Y.; Sun, S.Q.; Hong, J.P.; Chen, J. Analysis of hepatitis virus infection in hemodialysis patients. J. Clin. Nephrol. 2008, 8, 60–62. [Google Scholar]
- Qin, F.Q.; Li, P. A comprehensive analysis of 135 hemodialysis patients with viral hepatitis b and c infection. Chin. J. Blood Purif. 2003, 2, 267–268. [Google Scholar]
- Tong, Q.; Wu, B.B.; Zhang, L.M. Hepatitis virus infection in maintenance hemodialysis patients. Shanghai Med. 2006, 29, 838–840. [Google Scholar]
- Liu, G.L.; Xu, W.L.; Wei, J.F.; Wang, X.L. Investigation of HBV infection in hemodialysis patients. Prev. Med. Lit. Inf. 2001, 7, 1–3. [Google Scholar]
- Niu, A.N.; Yang, L.M. Analysis of infection status and related factors of HBV- HCV in hemodialysis patients. Shenzhen Med. 1999, 12, 17–18. [Google Scholar]
- Yin, L.F.; Huang, D.S. Observation of hepatitis virus infection in hemodialysis patients. Railw. Med. 1994, 22, 27–28. [Google Scholar]
- Xie, M.X.; Chen, Y.F. Comparison of positivity rates of anti-HCV in patients under dialysis. China Trop. Med. 2007, 7, 548–550. [Google Scholar]
- Li, Z.H.; Wu, Q.Z.; Wang, Z.H. Analysis of hepatitis B, C infection in maintenance hemodialysis patients. Int. Med. Health Guid. News 2007, 13, 37–38. [Google Scholar]
- Liu, J.C. Detection and analysis of hepatitis virus infection in hemodialysis patients. Chin. Folk Med. 2010, 16, 89–90. [Google Scholar]
- Liu, Q.; Yao, L.; Liu, X.D.; Liu, X.D.; Zhu, X.W.; Geng, Y.; Fen, M.L.; Wang, L.N. Analysis of viral hepatitis infection in hemodialysis patients. Chin. Blood Purif. 2012, 8, 417–420. [Google Scholar]
- Mao, W.J.; Li, X.Q.; Zhen, T.T. Investigation and analysis of HCV infection in hemodialysis patients. Chin. J. Hosp. Infect. 2013, 5, 1002–1003. [Google Scholar]
- Wang, H. Analysis of HCV infection related factors in maintenance hemodialysis patients in a primary hospital. Chin. J. Infect. Control 2012, 5, 376–378. [Google Scholar]
- Ling, L.; Wang, S.F.; Qian, Y.M. Analysis of HCV infection in hemodialysis patients and its influencing factors. Anhui Med. 2014, 8, 1045–1048. [Google Scholar]
- Wang, Q.; Pang, Y.S.; Li, L. Analysis of hepatitis c infection and influencing factors in 120 dialysis patients with type 2 diabetes mellitus and renal failure. Pract. Prev. Med. 2018, 1, 96–98. [Google Scholar]
- Wang, L.F.; Ma, L.B. Analysis of related factors of hemodialysis hepatitis b and hepatitis c infection and discussion of preventive measures. Pract. Prev. Med. 2014, 5, 598–599. [Google Scholar]
- Xu, X.Y.; Liu, F.J.Z. Clinical study of viral hepatitis in 150 patients with maintenance hemodialysis. Contemp. Med 2010, 20, 21–22. [Google Scholar]
- Yan, S.P.; Pan, H.Q.; Li, L.C.; Li, X.L.; Li, M.L.; Zhou, M. Risk factors of HCV infection in hemodialysis patients in a hospital in Changsha. Chin. J. Infect. Control 2012, 2, 112–114. [Google Scholar]
- Yang, M.; Wang, J.S.; Zhu, J.T.; Zhang, X.L.; Zhu, B. A multicenter clinical study of HCV infection in hemodialysis patients. J. Nanjing Med. Univ. 2012, 6, 852–854. [Google Scholar]
- Zeng, S.Y.; Xue, S.Q.; Lou, G.P. Risk factors and prevention of HCV nosocomial infection in hemodialysis patients. Chin. J. Integr. Nephrop. 2011, 4, 318–320. [Google Scholar]
- Zhang, W.C.; Li, H.; Yu, L.; Wang, S.X. Serological changes and risk factors of HCV infection in hemodialysis patients: Follow-up data for three years attached. Chin. J. Clin. 2013, 1, 125–127. [Google Scholar]
- Zhang, T.; Sun, X.F.; Chen, X.M.; Wang, Y.D. The occurrence and cause of hepatitis virus infection in hemodialysis patients. Chin. Blood Purif. 2010, 10, 577–579. [Google Scholar]
- Zhu, B.; Wang, Y.F.; Zhou, Y.F.; Bao, Z.Y.; Zhao, W.H. Clinical study on HCV infection in hemodialysis patients in changshu district. Chin. Blood Purif. 2015, 4, 213–215. [Google Scholar]
- Zhang, H.L. Analysis of the correlation between hemodialysis and hepatitis c virus infection in patients with type 2 diabetic renal failure. Med. Clin. Res. 2018, 35, 377–378. [Google Scholar]
- Chen, B.L.; Yao, P.; Tan, Q.L.; Zhang, H.; Yao, M.C. Analysis of related factors of hemodialysis hepatitis c virus infection in patients with type 2 diabetic renal failure. Chin. J. Hosp. Infect. 2015, 25, 171–173. [Google Scholar]
- Zhang, X.L.; Zhu, B.; Yu, R.B.; Zhao, W.H. A multicenter clinical study of HCV infection in hemodialysis patients. Chin. Blood Purif. 2011, 10, 429–432. [Google Scholar]
- Zhao, B.; Yang, W.; Ni, X.Y.; Zhang, L.G. Investigation of hepatitis c infection in hospital maintenance hemodialysis patients (2008–2009). J. Pract. Med. 2010, 27, 555–556. [Google Scholar]
- Duong, C.M.; Olszyna, D.P.; McLaws, M.L. Hepatitis B and C virus infections among patients with end stage renal disease in a low-resourced hemodialysis center in Vietnam: A cross-sectional study. BMC Public Health 2015, 15, 192–199. [Google Scholar] [CrossRef]
- Somi, M.H.; Etemadi, J.; Ghojazadeh, M.; Farhang, S.; Faramarzi, M.; Foroutan, S.; Soleimanpour, M. Risk factors of HCV seroconversion in hemodialysis patients in Tabriz, Iran. Hepat. Mon. 2014, 14, e17417. [Google Scholar] [CrossRef]
- Kalantari, H.; Ebadi, S.; Yaran, M.; Maracy, M.; Shahshahan, Z. Prevalence and risk factors of hepatitis B and C viruses among hemodialysis patients in Isfahan, Iran. Adv. Biomed. Res. 2014, 3, 73. [Google Scholar] [PubMed]
- Chang, J.M.; Huang, C.F.; Chen, S.C.; Dai, C.Y.; Yeh, M.L.; Huang, J.F.; Kuo, H.T.; Chuang, W.L.; Yu, M.L.; Hwang, S.J.; et al. Discrepancy between serological and virological analysis of viral hepatitis in hemodialysis patients. Int. J. Med. Sci. 2014, 11, 436. [Google Scholar] [CrossRef]
- Soliman, A.R.; MomtazAbdElaziz, M.; ElLawindi, M.I. Evaluation of an isolation program of hepatitis C virus infected hemodialysis patients in some hemodialysis centers in Egypt. Nephrology 2013, 2013, 395467. [Google Scholar] [CrossRef]
- National Health and Family Planning Commission of The People’s Republic of China. WS 213-018 Diagnosis for hepatitis C. J. Clin. Hepatol. 2018, 34, 3–5. [Google Scholar]
- Ebrahim, S.; Clarke, M. STROBE: New standards for reporting observational epidemiology, a chance to improve. Internat. J. Epidemiol. 2007, 36, 946–948. [Google Scholar] [CrossRef] [PubMed]
- Strobe Statement: Strengthening the Reporting of Observational Studies in Epidemiology [EB /OL]. Available online: http: //www.strobe-statement.org /index.php? id = strobe-translations (accessed on 1 May 2013).
- Ades, A.E.; Lu, G.; Higgins, J.P. The interpretation of random-effects meta-analysis in decision models. Med. Decis. Mak. 2005, 25, 646–654. [Google Scholar] [CrossRef]
- Schaefer, M.; Mauss, S. Hepatitis C treatment in patients with drug addiction: Clinical management of interferon-alpha-associated psychiatric side effects. Curr. Drug Abus. Rev. 2008, 1, 177–187. [Google Scholar] [CrossRef]
- Dolan, K.A.; Shearer, J.; White, B.; Zhou, J.; Kaldor, J.; Wodak, A.D. Four-year follow-up of imprisoned male heroin users and methadone treatment:mortality, re-incarceration and hepatitis C infection. Addiction 2005, 100, 820–828. [Google Scholar] [CrossRef] [PubMed]
- Alfurayh, O.; Sabeel, A.; Al Ahdal, M.N.; Almeshari, K.; Kessie, G.; Hamid, M.; Cruz, D.D. Hand contamination with hepatitis C virus in staff looking after hepatitis C-positive hemodialysis patients. Am. J. Nephrol. 2000, 20, 103–106. [Google Scholar] [CrossRef] [PubMed]
- Girndt, M.; Kohler, H.; Schiedhelm-Weick, E. T-cell activation defect in HD patients: Evidence for a role of tlle B7/CD28 pathway. Kidney Int. 1933, 44, 359–365. [Google Scholar] [CrossRef]
- Huraib, S.O. Hepatitis C in dialysis patients. Saudi J. Kidney Dis. Transpl. 2003, 14, 442–450. [Google Scholar]
- Zeldis, J.B.; Depner, T.A.; Kuramoto, I.K.; Gish, R.G.; Holland, P.V. The prevalence of hepatitis C virus antibodies among hemodialysis patients. Ann. Intern. Med. 1990, 112, 958–960. [Google Scholar] [CrossRef]
- Marinaki, S.; Boletis, J.N.; Sakellariou, S.; Delladetsima, I.K. Hepatitis C in hemodialysis patients. World J. Hepatol. 2015, 7, 548–558. [Google Scholar] [CrossRef] [PubMed]







{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Reference Number | Author and Year of Publication | Regions | Study Type | Participants Category (Case/Control) | Sample Size (Case/Control) | Male/Female | Age (Years) * |
|---|---|---|---|---|---|---|---|
| 4 | Zahedi 2012 | Iran, Kerman | observational study | HCV-infected hemodialysis patients/non-HCV-infected hemodialysis patients | 16/22 | 24/14 | 51 ± 9 |
| 20 | Chen 2013 | Guangdong, Shenzhen | observational study | HCV-infected hemodialysis patients/non-HCV-infected hemodialysis patients | 19/164 | 117/66 | 47.14 ± 15.196 |
| 22 | Kargar 2016 | Iran, Hormozgan | observational study | HCV-infected hemodialysis patients/non-HCV-infected hemodialysis patients | 5/144 | 92/57 | 56.23 ± 12.35 |
| 23 | Zhang 1999 | China, Chongqing | observational study | HCV-infected hemodialysis patients/non-HCV-infected hemodialysis patients | 17/31 | 30/18 | 50.5 ± 13.5 |
| 59 | Duong 2015 | Australia, Sydney | observational study | HCV-infected hemodialysis patients/non-HCV-infected hemodialysis patients | 8/105 | 59/54 | 53 ± 16 |
| 60 | Somi 2014 | Iran, Tabriz | observational study | HCV-infected hemodialysis patients/non-HCV-infected hemodialysis patients | 37/418 | 275/180 | 55.98 ± 15.6 |
| 61 | Kalantari 2014 | Iran, Isfahan | observational study | HCV-infected hemodialysis patients/non-HCV-infected hemodialysis patients | 26/473 | 303/196 | 52.3 ± 12.8 |
| 62 | Chang 2014 | Taiwan, Kaohsiung | observational study | HCV-infected hemodialysis patients/non-HCV-infected hemodialysis patients | 290/1391 | 824/857 | 62.2 ± 12.9 |
| 63 | Soliman 2013 | Egypt, Cairo | observational study | HCV-infected hemodialysis patients/non-HCV-infected hemodialysis patients | 28/55 | 47/36 | 52.29 ± 12.10; 49.47 ± 15.5 |
| 24 | Cao 2006 | China, Beijing | observational study | HCV-infected hemodialysis patients/non-HCV-infected hemodialysis patients | 10/78 | 42/88 | 52.33 ± 12.55; 57.45 ± 12.16 |
| 25 | Chen 2002 | China, Beijing | observational study | HCV-infected hemodialysis patients/non-HCV-infected hemodialysis patients | 28/71 | 57/42 | 58.1 ± 13.2; 57.7 ± 12.9 1) |
| 26 | Liu 1996 | China, Shenyang | observational study | HCV-infected hemodialysis patients/non-HCV-infected hemodialysis patients | 17/28 | 33/12 | 23–62 |
| 27 | Liu 1998 | China, Beijing | observational study | HCV-infected hemodialysis patients/non-HCV-infected hemodialysis patients | 34/15 | 21/28 | 53.1 ± 11.2 |
| 28 | Liu 2005 | Xinjiang, Shihe | observational study | HCV-infected hemodialysis patients/non-HCV-infected hemodialysis patients | 48/72 | 80/40 | 19–81 |
| 29 | Wang 2003 | Anhui, Benyang | observational study | HCV-infected hemodialysis patients/non-HCV-infected hemodialysis patients | 22/31 | 40/11 | 46.68 ± 10.18; 47.50 ± 13.44 |
| 30 | Wang 2004 | China, Shanahai | observational study | HCV-infected hemodialysis patients/non-HCV-infected hemodialysis patients | 51/97 | 57/91 | 51 ± 14 |
| 31 | Xiao 1997 | Jiangsu, Nanji | observational study | HCV-infected hemodialysis patients/non-HCV-infected hemodialysis patients | 121/33 | 110/44 | 46.0 ± 12.8 |
| 32 | Zhao 2008 | China, Dalin | observational study | HCV-infected hemodialysis patients/non-HCV-infected hemodialysis patients | 124/583 | _ | 60.25 ± 13.95; 63.51 ± 17.52 |
| 33 | Li 2008 | Fujian, Fuzhou | observational study | HCV-infected hemodialysis patients/non-HCV-infected hemodialysis patients | 29/120 | 101/48 | 13–82 |
| 34 | Qin 2003 | China, Dalin | observational study | HCV-infected hemodialysis patients/non-HCV-infected hemodialysis patients | 59/135 | 77/117 | 49.7 ± 16.4 |
| 35 | Tang 2006 | China, Shanahai | observational study | HCV-infected hemodialysis patients/non-HCV-infected hemodialysis patients | 32/78 | 59/51 | 49.2 ± 14.3 |
| 36 | Liu 2001 | Shandong, Liaocheng | observational study | HCV-infected hemodialysis patients/non-HCV-infected hemodialysis patients | 20/28 | 36/12 | 17–76 |
| 37 | Niu 1999 | Guangdong, Shenzhen | observational study | HCV-infected hemodialysis patients/non-HCV-infected hemodialysis patients | 12/38 | 27/23 | 48.5 + 12.8; 49.4 + 16.8 |
| 38 | Yin 1994 | Jiangsu, Nanji | observational study | HCV-infected hemodialysis patients/non-HCV-infected hemodialysis patients | 14/13 | 17/10 | 21–69 |
| 39 | Xie 2007 | Haikou, Hainan | observational study | HCV-infected hemodialysis patients/non-HCV-infected hemodialysis patients | 15/39 | 36/18 | 48.4 |
| 40 | Li 2007 | Guangdong, Zhanjiang | observational study | HCV-infected hemodialysis patients/non-HCV-infected hemodialysis patients | 8/78 | 46/40 | 49.3 (25–71) |
| 41 | Liu 2010 | Jilin, Songyuan | observational study | HCV-infected hemodialysis patients/non-HCV-infected hemodialysis patients | 16/36 | 32/20 | 48.7 ± 2.1 |
| 42 | Liu 2012 | Liaoning, Shenyang | observational study | HCV-infected hemodialysis patients/non-HCV-infected hemodialysis patients | 7/89 | 42/54 | 52.8 ± 15.4 |
| 43 | Mao 2013 | Zhejiang, Taizhou | observational study | HCV-infected hemodialysis patients/non-HCV-infected hemodialysis patients | 4/96 | 57/43 | 50.8 (25–72) |
| 44 | Wang 2012 | Hunan, Zhuzhou | observational study | HCV-infected hemodialysis patients/non-HCV-infected hemodialysis patients | 22/32 | 35/19 | 51.88 ± 13.10 |
| 45 | Wang, S.F. 2014 | Anhui, Hefei | observational study | HCV-infected hemodialysis patients/non-HCV-infected hemodialysis patients | 19/130 | 1.33/1 | 52.6 ± 11.3 |
| 46 | Wang 2018 | China, Chongqing | observational study | HCV-infected hemodialysis patients/non-HCV-infected hemodialysis patients | 15/105 | 69/51 | 57.86 ± 7.85 |
| 47 | Wang, L.F. 2014 | Zhejiang, Qunan | observational study | HCV-infected hemodialysis patients/non-HCV-infected hemodialysis patients | 59/409 | 249/219 | 21–78 |
| 48 | Xu 2010 | Guangdong, Zhanjiang | observational study | HCV-infected hemodialysis patients/non-HCV-infected hemodialysis patients | 64/86 | 80/70 | 17–84 |
| 49 | Yan 2012 | Hunan, Changsha | observational study | HCV-infected hemodialysis patients/non-HCV-infected hemodialysis patients | 23/51 | 47/27 | 47.72 ± 18.93 |
| 50 | Yang 2012 | Jiangsu, Yangzhou | observational study | HCV-infected hemodialysis patients/non-HCV-infected hemodialysis patients | 39/264 | 194/109 | 48.49 ± 11.45; 50.08 ± 12.95 |
| 51 | Zeng 2011 | Guangdong, Qingyuan | observational study | HCV-infected hemodialysis patients/non-HCV-infected hemodialysis patients | 47/165 | 116/96 | 16–76 |
| 52 | Zhang 2013 | China, Beijing | observational study | HCV-infected hemodialysis patients/non-HCV-infected hemodialysis patients | 20/164 | 97/87 | 55.0 ± 15.6 |
| 53 | Zhang 2010 | China, Beijing | observational study | HCV-infected hemodialysis patients/non-HCV-infected hemodialysis patients | 14/131 | _ | _ |
| 54 | Zhu 2015 | Jiangsu, Changzhou | observational study | HCV-infected hemodialysis patients/non-HCV-infected hemodialysis patients | 15/214 | 134/95 | 56.25 ± 13.38; 51.04 ± 13.20 |
| 55 | Zhang 2018 | Hebei, Shijiazhuang | observational study | HCV-infected hemodialysis patients/non-HCV-infected hemodialysis patients | 39/60 | 74/25 | 54.58 ± 11.88 |
| 56 | Chen 2015 | Hubei, Enshi | observational study | HCV-infected hemodialysis patients/non-HCV-infected hemodialysis patients | 31/45 | 43/33 | 53.21 ± 10.61 |
| 57 | Zhang 2011 | Jiangsu, Nanji | observational study | HCV-infected hemodialysis patients/non-HCV-infected hemodialysis patients | 176/620 | 492/304 | 53 ± 12; 52 ± 14 |
| 58 | Zhao 2010 | Shandong, Weifang | observational study | HCV-infected hemodialysis patients/non-HCV-infected hemodialysis patients | 15/36 | 27/24 | l9–78 |
| Subgroup Analyses by Study Factors | OR or MD(95% CI) before Reference Omitted | OR or MD (95% CI) after Reference Omitted | Reversal of OR or MD (95% CI) after Reference Omitted Compared with that before Reference Omitted | Reference Omitted |
|---|---|---|---|---|
| The studies with wide interval of 95% CI for OR values | ||||
| Histories of blood transfusion | 4.30 (3.11–5.96) | 5.13 (3.43–7.68) | No | 42 |
| Shared hemodialysis devices | 5.00 (2.35–10.65) | 4.10 (1.66–10.16) | No | 50 |
| Hemodialysis units > 2 | 6.90 (2.42–19.68) | 6.35 (2.01–20.08) | No | 43 |
| Serum alanine aminotransferase levels | 5.62 (2.35–13.40) | 4.17 (1.89–9.23) | No | 50 |
| The studies with wide interval of 95% CI for MD values | ||||
| Duration of hemodialysis (months) | 28.96 (22.11–35.80) | 23.38 (18.17–28.59) | No | 59 |
| The studies with maximum value of weight (OR) | ||||
| Histories of blood transfusion | 4.30 (3.11–5.96) | 4.45 (3.26–6.09) | No | 57 |
| Shared hemodialysis devices | 5.00 (2.35–10.65) | 3.97 (1.89–8.32) | No | 57 |
| Hemodialysis units > 2 | 6.90 (2.42–19.68) | 10.16 (4.95–20.85) | No | 44 |
| Serum alanine aminotransferase levels | 5.62 (2.35–13.40) | 5.06 (1.60–15.98) | No | 57 |
| The studies with maximum value of weight (MD) | ||||
| Duration of hemodialysis (months) | 28.96 (22.11–35.80) | 26.36 (19.53–33.19) | No | 61,47 |
© 2019 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Cai, G.; Zheng, H.; Luo, L.; Wang, Z.; Jiang, Z.; Xu, S.; Lv, H.; Chen, Y.; Zhou, B.; Hu, C. Factors Correlating to the Development of Hepatitis C Virus Infection in Hemodialysis Patients—Findings Mainly from Asiatic Populations: A Systematic Review and Meta-Analysis. Int. J. Environ. Res. Public Health 2019, 16, 1453. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph16081453
Cai G, Zheng H, Luo L, Wang Z, Jiang Z, Xu S, Lv H, Chen Y, Zhou B, Hu C. Factors Correlating to the Development of Hepatitis C Virus Infection in Hemodialysis Patients—Findings Mainly from Asiatic Populations: A Systematic Review and Meta-Analysis. International Journal of Environmental Research and Public Health. 2019; 16(8):1453. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph16081453
Chicago/Turabian StyleCai, Gaofeng, Hongjie Zheng, Lan Luo, Zhengting Wang, Zhenggang Jiang, Shuangfei Xu, Huakun Lv, Yongdi Chen, Biao Zhou, and Chonggao Hu. 2019. "Factors Correlating to the Development of Hepatitis C Virus Infection in Hemodialysis Patients—Findings Mainly from Asiatic Populations: A Systematic Review and Meta-Analysis" International Journal of Environmental Research and Public Health 16, no. 8: 1453. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph16081453