Spatial Analysis of Built Environment Risk for Respiratory Health and Its Implication for Urban Planning: A Case Study of Shanghai

Abstract
:1. Introduction
2. Materials and Methods
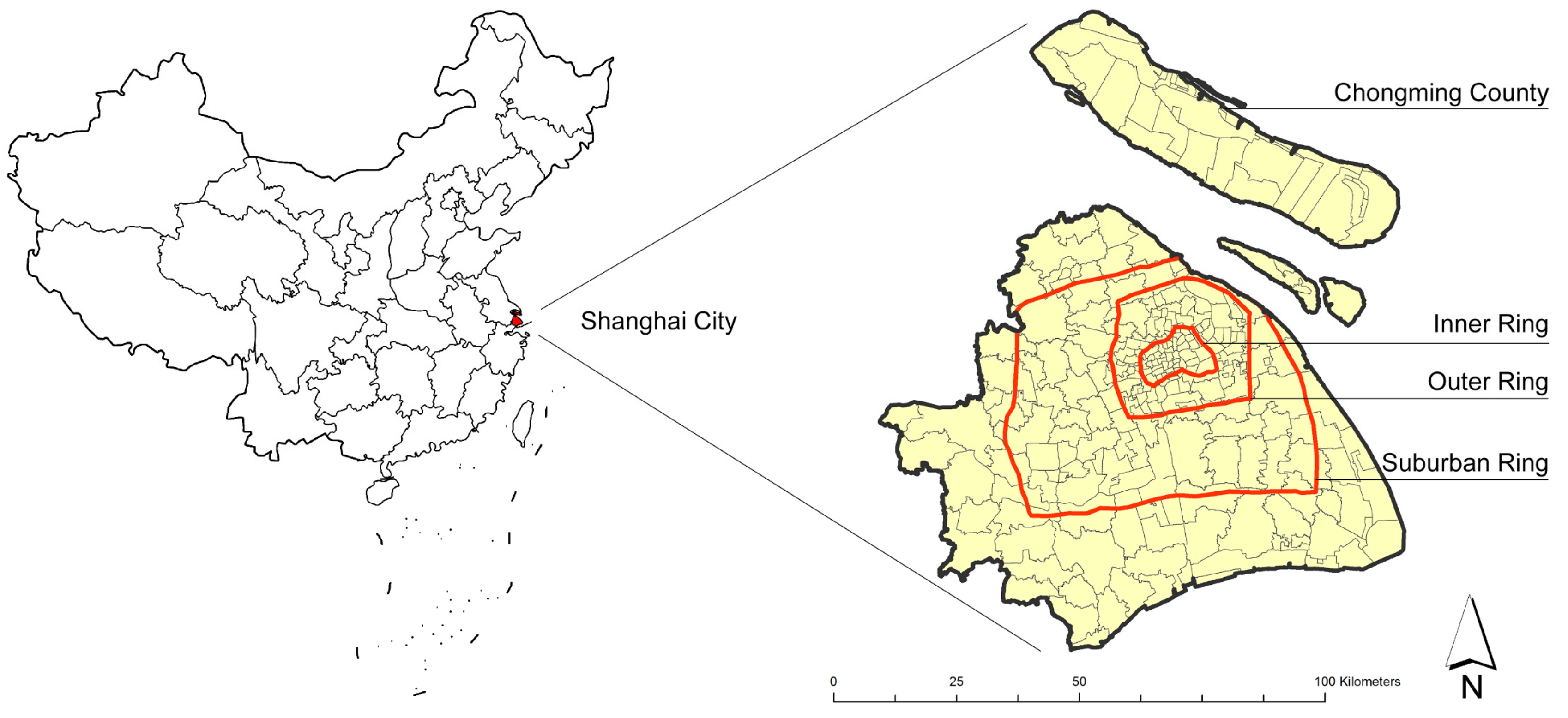
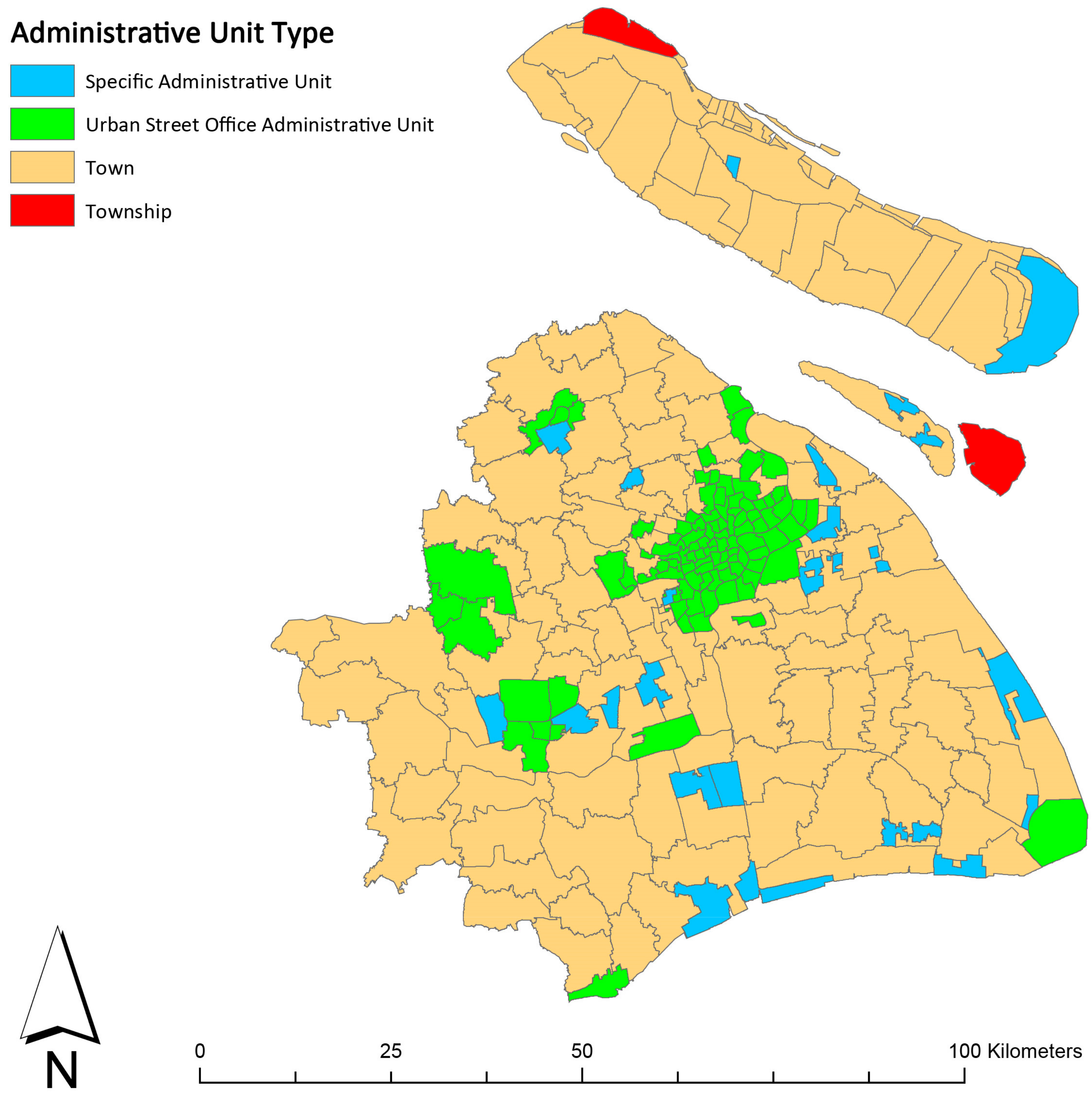
2.1. Study Site
2.2. Lung Cancer Data
2.3. Environmental Factors of Lung Cancer and Their Proxies
2.4. Analytical Methods
3. Results
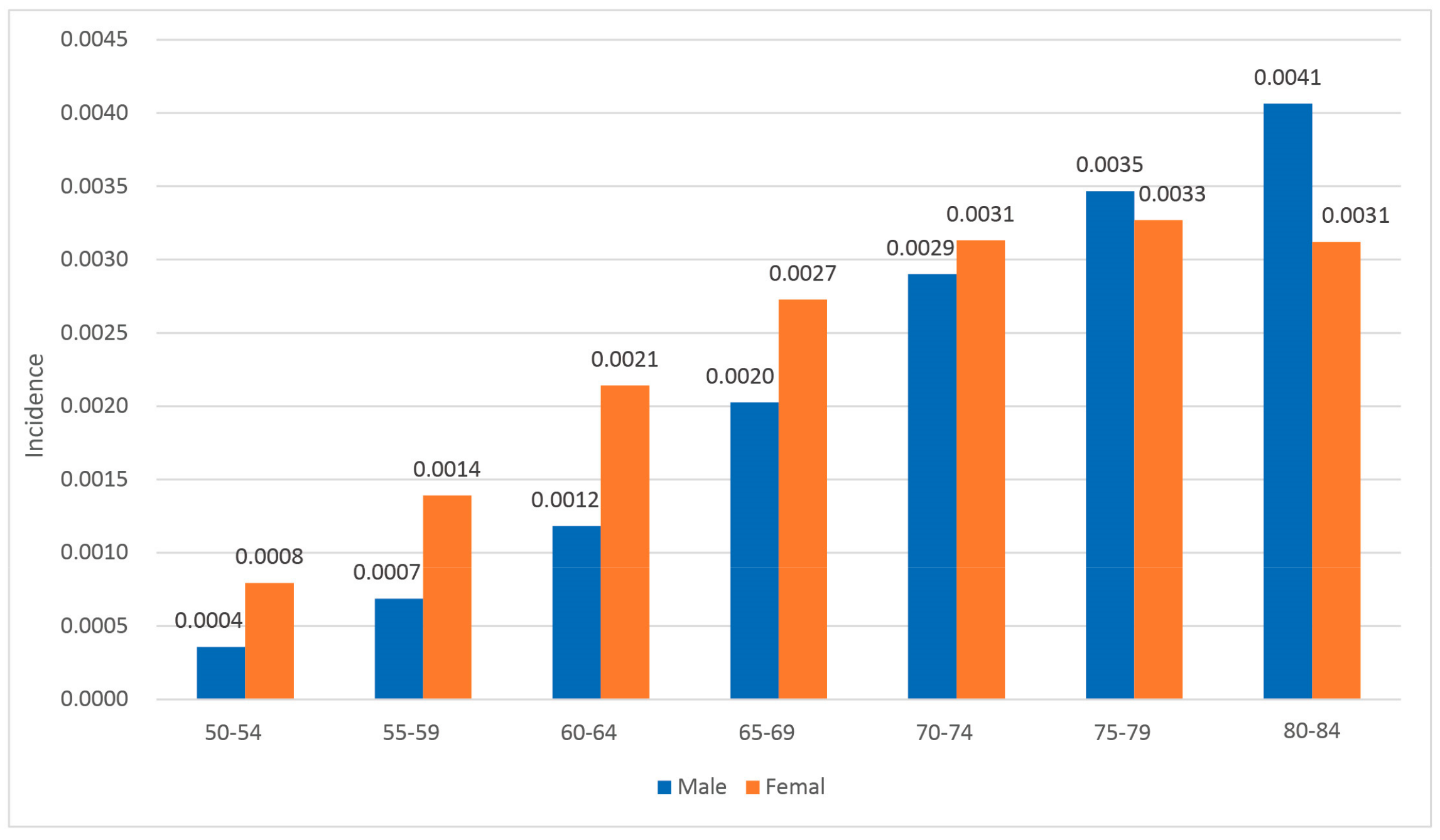
3.1. Descriptive Statistics of Lung Cancer Incidence and Built Environment Factors
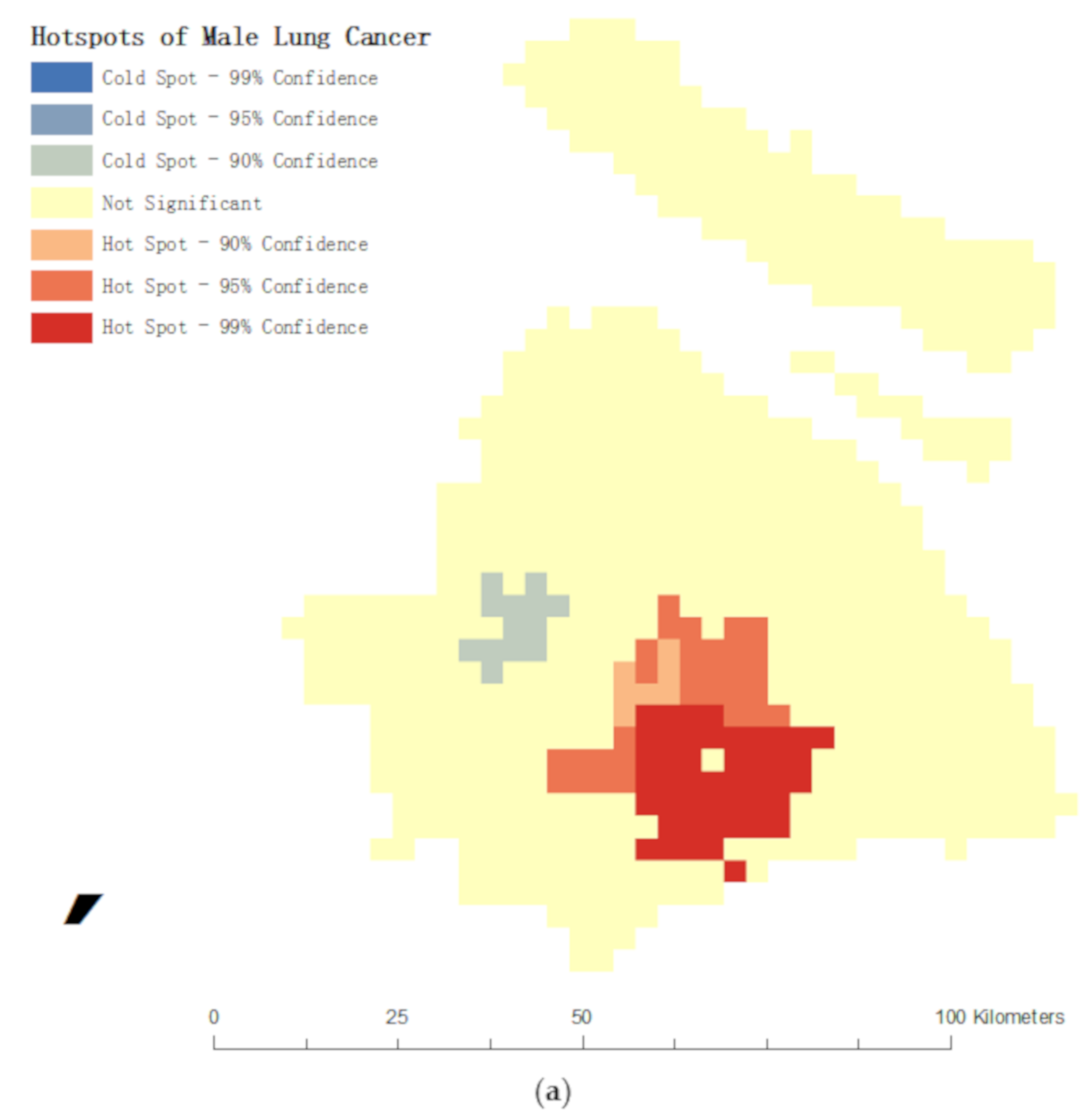
3.2. Spatial Clustering Characteristics of Lung Cancer Cases
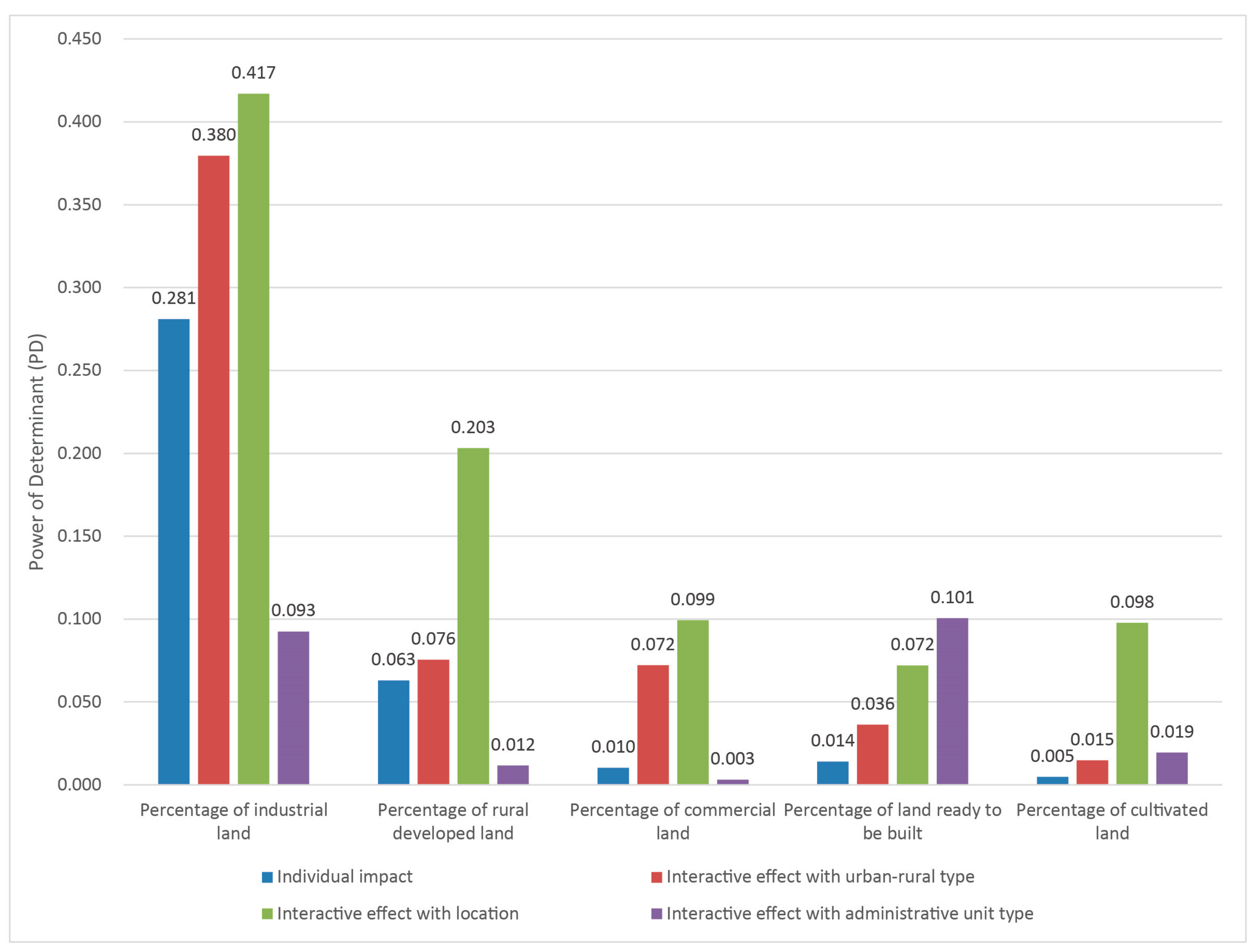
3.3. Spatial Stratified Heterogeneity of Lung Cancer Cases
4. Discussion
5. Conclusions
Author Contributions
Funding
Conflicts of Interest
References
- Bray, F.; Ferlay, J.; Soerjomataram, I.; Siegel, R.L.; Torre, L.A.; Jemal, A. Global cancer statistics 2018: GLOBOCAN estimates of incidence and mortality worldwide for 36 cancers in 185 countries. CA Cancer J. Clin. 2018, 68, 394–424. [Google Scholar] [CrossRef] [PubMed]
- Chen, W.; Sun, K.; Zheng, R.; Zeng, H.; Zhang, S.; Xia, C.; Yang, Z.; Li, H.; Zou, X.; He, J. Cancer incidence and mortality in China, 2014. Chin. J. Cancer Res. 2018, 30. [Google Scholar] [CrossRef]
- Wang, Y.-C.; Wei, L.-J.; Liu, J.-T.; Li, S.-X.; Wang, Q.-S. Comparison of cancer incidence between China and the USA. Cancer Biol. Med. 2012, 9, 128. [Google Scholar] [PubMed]
- Loomis, D.; Grosse, Y.; Lauby-Secretan, B.; Ghissassi, F.E.; Bouvard, V.; Benbrahim-Tallaa, L.; Guha, N.; Baan, R.; Mattock, H.; Straif, K. The carcinogenicity of outdoor air pollution. Lancet Oncol. 2013, 14, 1262–1263. [Google Scholar] [CrossRef]
- Pope, C.A. III; Burnett, R.T.; Thun, M.J.; Calle, E.E.; Daniel, K.; Kazuhiko, I.; Thurston, G.D. Lung cancer, cardiopulmonary mortality, and long-term exposure to fine particulate air pollution. JAMA 2002, 287, 1132–1141. [Google Scholar] [CrossRef]
- Perdue, W.C.; Stone, L.A.; Gostin, L.O. The built environment and its relationship to the public’s health: The legal framework. Am. J. Public Health 2003, 93, 1390–1394. [Google Scholar] [CrossRef]
- Evans, G.W. The built environment and mental health. J. Urban Health-Bull. N. Y. Acad. Med. 2003, 80, 536–555. [Google Scholar] [CrossRef] [PubMed]
- Srinivasan, S.; O’Fallon, L.A. Creating healthy communities, healthy homes, healthy people: Initiating a research agenda on the built environment and public health. Am. J. Public Health 2003, 93, 1446–1450. [Google Scholar] [CrossRef]
- Handy, S.L.; Boarnet, M.G.; Ewing, R.; Killingsworth, R.E. How the built environment affects physical activity: Views from urban planning. Am. J. Prev. Med. 2002, 23, 64–73. [Google Scholar] [CrossRef]
- Lan, W.; Shuwen, L.; Xiaojing, Z. Exploration of approaches and factors for healthy city planning. China City Planning Review 2018, 27, 24–31. [Google Scholar]
- Xu, H.; Bi, X.H.; Zheng, W.W.; Wu, J.H.; Feng, Y.C. Particulate matter mass and chemical component concentrations over four Chinese cities along the western Pacific coast. Environ. Sci. Pollut. Res. Int. 2015, 22, 1940–1953. [Google Scholar] [CrossRef] [PubMed]
- Weng, Q.; Yang, S. Urban air pollution patterns, land Use, and thermal landscape: An examination of the linkage using GIS. Environ. Monit. Assess. 2006, 117, 463–489. [Google Scholar] [CrossRef]
- Schweitzer, L.; Zhou, J. Neighborhood air quality, respiratory health, and vulnerable populations in compact and sprawled regions. J. Am. Plan. Assoc. 2010, 76, 363–371. [Google Scholar] [CrossRef]
- Durstine, J.L.; Gordon, B.; Wang, Z.; Luo, X. Chronic disease and the link to physical activity. J. Sport Health Sci. 2013, 2, 3–11. [Google Scholar] [CrossRef] [Green Version]
- Mackenbach, J.D.; Rutter, H.; Compernolle, S.; Glonti, K.; Oppert, J.M.; Charreire, H.; De, B.I.; Brug, J.; Nijpels, G.; Lakerveld, J. Obesogenic environments: A systematic review of the association between the physical environment and adult weight status, the SPOTLIGHT project. BMC Public Health 2014, 14, 233. [Google Scholar] [CrossRef] [PubMed]
- Edwards, R.; Plessmulloli, T.; Howel, D.; Chadwick, T.; Bhopal, R.; Harrison, R.; Gribbin, H. Does living near heavy industry cause lung cancer in women? A case-control study using life grid interviews. Thorax 2006, 61, 1076–1082. [Google Scholar] [CrossRef] [PubMed]
- Tang, X.; Liu, H.; Li, J.; Xie, Z.; Zhao, W. Response analysis of haze/particulate matter pollution to land use/cover in Beijing. China Environ. Sci. 2015, 35, 2561–2569. [Google Scholar]
- Xu, S.; Zou, B.; Pu, Q.; Guo, Y. Impact analysis of land use/cover on air pollution. J. Geo-Inf. Sci. 2015, 17, 290–299. [Google Scholar]
- Shi, Y.; Li, R.; Qiu, J.; Huang, D.; Wang, H. Spatial distribution simulation and underlying surface factors analysis of NO2 concentration based on land use regression spatial distribution simulation and underlying surface factors analysis of NO2 concentration based on land use regression. J. Geo-Inf. Sci. 2017, 19, 10–19. [Google Scholar]
- Cui, Y. Research of the Influence City Land Use Change on Air Environment Quality; Shandong Jianzhu University: Jinan, China, 2013. [Google Scholar]
- Gilescorti, B.; Vernezmoudon, A.; Reis, R.; Turrell, G.; Dannenberg, A.L.; Badland, H.; Foster, S.; Lowe, M.; Sallis, J.F.; Stevenson, M. City planning and population health: A global challenge. Lancet 2016, 388, 2912. [Google Scholar] [CrossRef]
- Zhu, Y.; Hinds, W.C.; Kim, S.; Sioutas, C. Concentration and size distribution of ultrafine particles near a major highway. J. Air Waste Manag. Assoc. 2002, 52, 1032–1042. [Google Scholar] [CrossRef] [PubMed]
- Chen, F.; Jackson, H.; Bina, W.F. Lung adenocarcinoma incidence rates and their relation to motor vehicle density. Cancer Epidemiol. Biomark Prev. 2009, 18, 760. [Google Scholar] [CrossRef]
- De, H.K.; Korek, M.; Vienneau, D.; Keuken, M.; Kukkonen, J.; Nieuwenhuijsen, M.J.; Badaloni, C.; Beelen, R.; Bolignano, A.; Cesaroni, G. Comparing land use regression and dispersion modelling to assess residential exposure to ambient air pollution for epidemiological studies. Environ. Int. 2014, 73, 382–392. [Google Scholar] [Green Version]
- Samet, J.M.; Avila-Tang, E.; Boffetta, P.; Hannan, L.M.; Olivo-Marston, S.; Thun, M.J.; Rudin, C.M. Lung cancer in never smokers: Clinical epidemiology and environmental risk factors. Clin. Cancer Res. 2009, 15, 5626–5645. [Google Scholar] [CrossRef] [PubMed]
- Thun, M.J.; Henley, S.J.; Burns, D.; Jemal, A.; Shanks, T.G.; Calle, E.E. Lung cancer death rates in lifelong nonsmokers. J. Natl. Cancer Inst. 2006, 98, 691–699. [Google Scholar] [CrossRef]
- Thun, M.J.; Henley, S.J.; Calle, E.E. Tobacco use and cancer: An epidemiologic perspective for geneticists. Oncogene 2002, 21, 7307. [Google Scholar] [CrossRef]
- Prescott, E.; Osler, M.; Hein, H.O.; Borchjohnsen, K.; Lange, P.; Schnohr, P.; Vestbo, J. Gender and smoking-related risk of lung cancer. The Copenhagen center for prospective population studies. Epidemiology 1998, 9, 79–83. [Google Scholar] [CrossRef]
- Boffetta, P.; Clark, S.; Min, S.; Gislefoss, R.; Peto, R.; Andersen, A. Serum cotinine level as predictor of lung cancer risk. Cancer Epidemiol. Biomark. Prev. 2006, 15, 1184–1188. [Google Scholar] [CrossRef]
- Wakelee, H.A.; Chang, E.T.; Gomez, S.L.; Keegan, T.H.; Feskanich, D.; Clarke, C.A.; Holmberg, L.; Yong, L.C.; Kolonel, L.N.; Gould, M.K. Lung cancer incidence in never smokers. J. Clin. Oncol. 2007, 25, 472–478. [Google Scholar] [CrossRef]
- Myers, R.; Brauer, M.; Ladhar, S.; Atkar-Khattra, S.; Yee, J.; Ho, C.; Mcguire, A.; Grant, K.; Lee, A.; Melosky, B. OA09. 07 Association between outdoor air pollution and lung cancer in female never smokers. J. Thoracic Oncol. 2018, 13, S342. [Google Scholar] [CrossRef]
- Booth, K.M.; Pinkston, M.M.; Poston, W.S.C. Obesity and the built environment. J. Am. Diet. Assoc. 2005, 105, 110–117. [Google Scholar] [CrossRef]
- Brownson, R.C.; Hoehner, C.M.; Day, K.; Forsyth, A.; Sallis, J.F. Measuring the built environment for physical activity: State of the science. Am. J. Prev. Med. 2009, 36, S99–S123. [Google Scholar] [CrossRef]
- Vandenbroucke, J.P. Is ‘The Causes of Cancer’ a Miasma theory for the end of the twentieth century? Int. J. Epidemiol. 1988, 17, 708–709. [Google Scholar] [CrossRef]
- Wu, S.; Powers, S.; Zhu, W.; Hannun, Y.A. Substantial contribution of extrinsic risk factors to cancer development. Nature 2016, 529, 43–47. [Google Scholar] [CrossRef] [PubMed]
- Sarkar, C.; Webster, C.; Gallacher, J. Healthy Cities: Public Health through Urban Planning; Edward Elgar Publishing: Cheltenham, UK, 2014. [Google Scholar]
- Mitchell, R.; Popham, F. Effect of exposure to natural environment on health inequalities: An observational population study. Lancet 2008, 372, 1655–1660. [Google Scholar] [CrossRef]
- Gazdar, A.F.; Zhou, C. 4 - Lung Cancer in Never-Smokers: A Different Disease. In IASLC Thoracic Oncology, 2nd ed.; Pass, H.I., Ball, D., Scagliotti, G.V., Eds.; Elsevier: Amsterdam, The Netherlands, 2018. [Google Scholar] [CrossRef]
- Wang, L.; Zhao, X.; Xu, W.; Tang, J.; Jiang, X. Correlation analysis of lung cancer and urban spatial factor: Based on survey in Shanghai. J. Thorac. Dis. 2016, 8, 2626. [Google Scholar] [CrossRef]
- Choe, S.-A.; Kauderer, S.; Eliot, M.N.; Glazer, K.B.; Kingsley, S.L.; Carlson, L.; Awad, Y.A.; Schwartz, J.D.; Savitz, D.A.; Wellenius, G.A. Air pollution, land use, and complications of pregnancy. Sci. Total Environ. 2018, 645, 1057–1064. [Google Scholar] [CrossRef]
- Son, Y.; Osornio-Vargas, Á.R.; O’Neill, M.S.; Hystad, P.; Texcalac-Sangrador, J.L.; Ohman-Strickland, P.; Meng, Q.; Schwander, S. Land use regression models to assess air pollution exposure in Mexico City using finer spatial and temporal input parameters. Sci. Total Environ. 2018, 639, 40–48. [Google Scholar] [CrossRef]
- Bertazzon, S.; Johnson, M.; Eccles, K.; Kaplan, G.G. Accounting for spatial effects in land use regression for urban air pollution modeling. Spat. Spatio-Temporal Epidemiol. 2015, 14-15, 9–21. [Google Scholar] [CrossRef] [PubMed]
- Habermann, M.; Billger, M.; Haeger-Eugensson, M. Land use regression as method to model air pollution. previous results for Gothenburg/Sweden. Procedia Eng. 2015, 115, 21–28. [Google Scholar] [CrossRef]
- Naughton, O.; Donnelly, A.; Nolan, P.; Pilla, F.; Misstear, B.D.; Broderick, B. A land use regression model for explaining spatial variation in air pollution levels using a wind sector based approach. Sci. Total Environ. 2018, 630, 1324–1334. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Li, C.; Wang, Z.; Li, B.; Peng, Z.-R.; Fu, Q. Investigating the relationship between air pollution variation and urban form. Build. Environ. 2018. [Google Scholar] [CrossRef]
- Shi, Y.; Xie, X.; Fung, J.C.-H.; Ng, E. Identifying critical building morphological design factors of street-level air pollution dispersion in high-density built environment using mobile monitoring. Build. Environ. 2018, 128, 248–259. [Google Scholar] [CrossRef]
- Coppel, G.; Wüstemann, H. The impact of urban green space on health in Berlin, Germany: Empirical findings and implications for urban planning. Landsc. Urban Plan 2017, 167, 410–418. [Google Scholar] [CrossRef]
- Wang, J.F.; Li, X.H.; Christakos, G.; Liao, Y.L.; Zhang, T.; Gu, X.; Zheng, X.Y. Geographical detectors-based health risk assessment and its application in the neural tube defects study of the Heshun Region, China. Int. J. Geogr. Inf. Sci. 2010, 24, 107–127. [Google Scholar] [CrossRef]
- Wang, J.-F.; Zhang, T.-L.; Fu, B.-J. A measure of spatial stratified heterogeneity. Ecol. Indic. 2016, 67, 250–256. [Google Scholar] [CrossRef] [Green Version]
- Liao, Y.; Wang, J.; Wu, J.; Driskell, L.; Wang, W.; Zhang, T.; Xue, G.; Zheng, X. Spatial analysis of neural tube defects in a rural coal mining area. Int. J. Environ. Health Res. 2010, 20, 439–450. [Google Scholar] [CrossRef] [PubMed]
- Huang, J.; Wang, J.; Bo, Y.; Xu, C.; Hu, M.; Huang, D. Identification of health risks of hand, foot and mouth disease in China using the geographical detector technique. Int. J. Environ. Res. Public Health 2014, 11, 3407–3423. [Google Scholar] [CrossRef] [PubMed]
- Elliott, P.; Wartenberg, D. Spatial epidemiology: Current approaches and future challenges. Environ. Health Perspect. 2004, 112, 998–1006. [Google Scholar] [CrossRef]
- Goovaerts, P.; Jacquez, G.M. Accounting for regional background and population size in the detection of spatial clusters and outliers using geostatistical filtering and spatial neutral models: The case of lung cancer in Long Island, New York. Int. J. Health Geogr. 2004, 3, 14. [Google Scholar] [CrossRef]
- Benedetti, M.; Lavarone, I.; Comba, P. Cancer risk associated with residential proximity to industrial sites: A review. Arch. Environ. Health 2001, 56, 342–349. [Google Scholar] [CrossRef] [PubMed]
- Chen, W.; Zheng, R.; Zeng, H.; Zhang, S. Epidemiology of lung cancer in China. Thorac. Cancer 2015, 6, 209–215. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Barbone, F.; Bovenzi, M.; Cavallieri, F.; Stanta, G. Air pollution and lung cancer in Trieste, Italy. Am. J. Epidemiol. 1995, 141, 1161–1169. [Google Scholar] [CrossRef] [PubMed]








{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Variables | Mean | Minimum | 25% | 50% | 75% | Maximum | |
|---|---|---|---|---|---|---|---|
| SIR 1 (new cases/10,000) | 7.86 | 0.00 | 4.56 | 6.63 | 8.90 | 104.5 | |
| Land use | Percentage of industrial land | 8.88 | 0.00 | 2.11 | 5.87 | 12.21 | 52.69 |
| Industrial parcel density (#/km2) | 113.02 | 0.00 | 34.79 | 53.73 | 99.51 | 1699.15 | |
| Percentage of high-quality residential land | 13.62 | 0.00 | 0.85 | 7.08 | 25.06 | 56.15 | |
| High-quality residential parcel density (#/km2) | 54.31 | 0.00 | 22.29 | 32.37 | 55.47 | 638.16 | |
| Percentage of Low-quality residential land | 1.52 | 0.00 | 0.05 | 0.46 | 1.23 | 21.37 | |
| Low-quality residential parcel density (#/km2) | 113.59 | 0.00 | 31.72 | 64.41 | 130.26 | 1276.32 | |
| Percentage of rural developed land | 4.52 | 0.00 | 0.00 | 1.63 | 8.33 | 20.83 | |
| Developed parcel density in rural area (#/km2) | 118.18 | 0.00 | 0.00 | 78.60 | 122.43 | 1215.28 | |
| Percentage of commercial land | 1.88 | 0.00 | 0.32 | 1.20 | 2.82 | 12.19 | |
| Commercial parcel density (#/km2) | 175.24 | 0.00 | 80.39 | 138.02 | 220.25 | 1391.98 | |
| Percentage of land ready to be built | 5.71 | 0.00 | 1.76 | 4.53 | 7.99 | 43.20 | |
| Density of parcel ready to be built (#/km2) | 74.80 | 0.00 | 35.35 | 55.44 | 95.33 | 431.22 | |
| Percentage of cultivated land | 24.36 | 0.00 | 0.00 | 12.16 | 49.39 | 86.23 | |
| Cultivated land density (#/km2) | 33.39 | 0.00 | 0.00 | 6.86 | 17.95 | 1755.62 | |
| Transportation system | Road density (#/km2) | 6.41 | 0.33 | 3.06 | 5.68 | 9.19 | 22.78 |
| Main road density (#/km2) | 0.41 | 0.00 | 0.11 | 0.28 | 0.59 | 2.11 | |
| Percentage of transportation land | 5.77 | 0.03 | 2.63 | 5.26 | 6.99 | 42.33 | |
| Green space | Percentage of green space | 2.79 | 0.00 | 0.57 | 1.65 | 3.60 | 70.92 |
| Green space density (#/km2) | 199.78 | 0.00 | 92.32 | 171.28 | 264.67 | 920.37 | |
| Variables | All Space Units Included | Industrial Parks Excluded | |||
|---|---|---|---|---|---|
| PD3 | p-Value | PD | p-Value | ||
| Land use | Administrative unit type 1 | 0.64 | 0.000 *** | 0.02 | 0.745 |
| Location 2 | 0.04 | 0.08 | 0.11 | 0.004 ** | |
| Percentage of industrial land | 0.28 | 0.000 *** | 0.04 | 0.978 | |
| Industrial parcel density (#/km2) | 0.01 | 0.909 | 0.07 | 0.263 | |
| Percentage of high-quality residential land | 0.01 | 0.263 | 0.02 | 0.556 | |
| High-quality residential parcel density (#/km2) | 0.00 | / | 0.05 | 0.622 | |
| Percentage of Low-quality residential land | 0.02 | 0.843 | 0.07 | 0.355 | |
| Low-quality residential parcel density (#/km2) | 0.00 | / | 0.00 | / | |
| Percentage of rural developed land | 0.01 | 0.362 | 0.02 | 0.471 | |
| Developed parcel density in rural area (#/km2) | 0.03 | 0.370 | 0.03 | 0.935 | |
| Percentage of commercial land | 0.01 | 0.666 | 0.02 | 0.988 | |
| Commercial parcel density (#/km2) | 0.01 | 0.489 | 0.02 | 0.915 | |
| Percentage of land ready to be built | 0.01 | 0.365 | 0.01 | 0.564 | |
| Density of parcel ready to be built (#/km2) | 0.02 | 0.548 | 0.01 | 0.976 | |
| Percentage of cultivated land | 0.06 | 0.03 * | 0.11 | 0.027 * | |
| Cultivated land density (#/km2) | 0.01 | 0.259 | 0.02 | 0.871 | |
| Transportation system | Road density (#/km2) | 0.01 | 0.547 | 0.01 | 0.987 |
| Main road density (#/km2) | 0.01 | 0.566 | 0.03 | 0.500 | |
| Percentage of transportation land | 0.02 | 0.261 | 0.01 | 0.986 | |
| With or without crossing expressway | 0.00 | / | 0.00 | / | |
| Green space | Percentage of green space | 0.05 | 0.037 * | 0.03 | 0.452 |
| Green space density (#/km2) | 0.01 | 0.573 | 0.11 | 0.318 | |
| Stratum | Street | Town | Township | Industrial Park |
|---|---|---|---|---|
| SIR (cases/10,000) | 7.29 | 6.86 | 4.21 | 63.52 |
| Stratum | <10% | 10–30% | >30% |
|---|---|---|---|
| SIR (cases/10,000) | 7.05 | 7.46 | 31.59 |
© 2019 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Wang, L.; Sun, W.; Zhou, K.; Zhang, M.; Bao, P. Spatial Analysis of Built Environment Risk for Respiratory Health and Its Implication for Urban Planning: A Case Study of Shanghai. Int. J. Environ. Res. Public Health 2019, 16, 1455. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph16081455
Wang L, Sun W, Zhou K, Zhang M, Bao P. Spatial Analysis of Built Environment Risk for Respiratory Health and Its Implication for Urban Planning: A Case Study of Shanghai. International Journal of Environmental Research and Public Health. 2019; 16(8):1455. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph16081455
Chicago/Turabian StyleWang, Lan, Wenyao Sun, Kaichen Zhou, Minlu Zhang, and Pingping Bao. 2019. "Spatial Analysis of Built Environment Risk for Respiratory Health and Its Implication for Urban Planning: A Case Study of Shanghai" International Journal of Environmental Research and Public Health 16, no. 8: 1455. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph16081455