Modelling a Supplementary Vaccination Program of Rubella Using the 2012–2013 Epidemic Data in Japan



Abstract
:1. Introduction
2. Materials and Methods
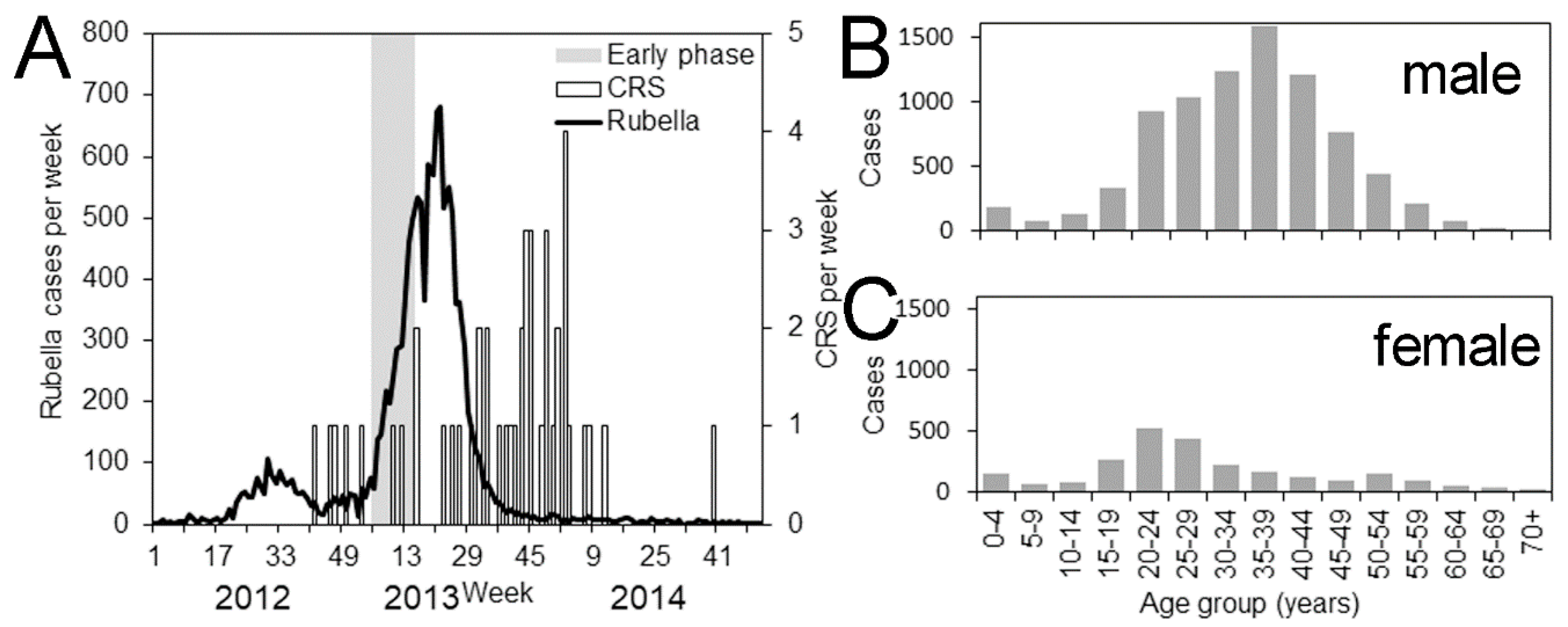
2.1. Epidemiological Data
2.2. Mathematical Models
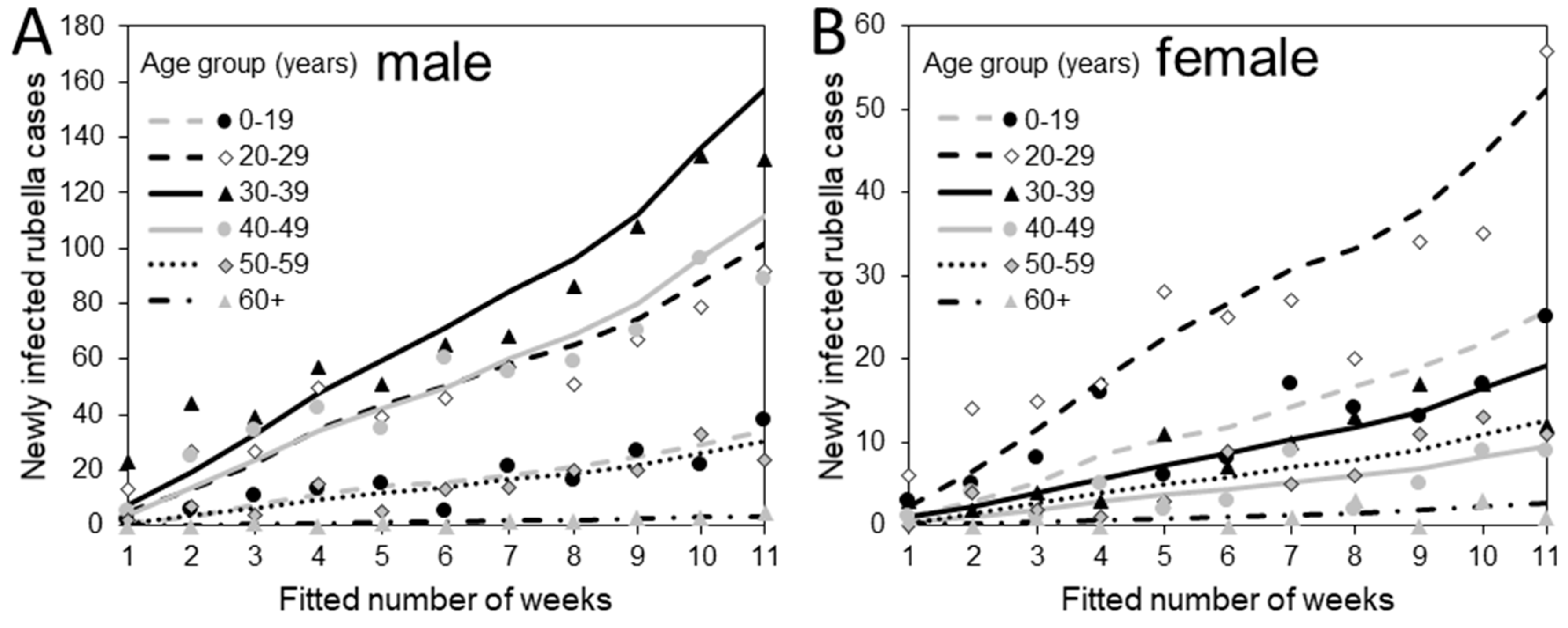
2.2.1. Transmission Model
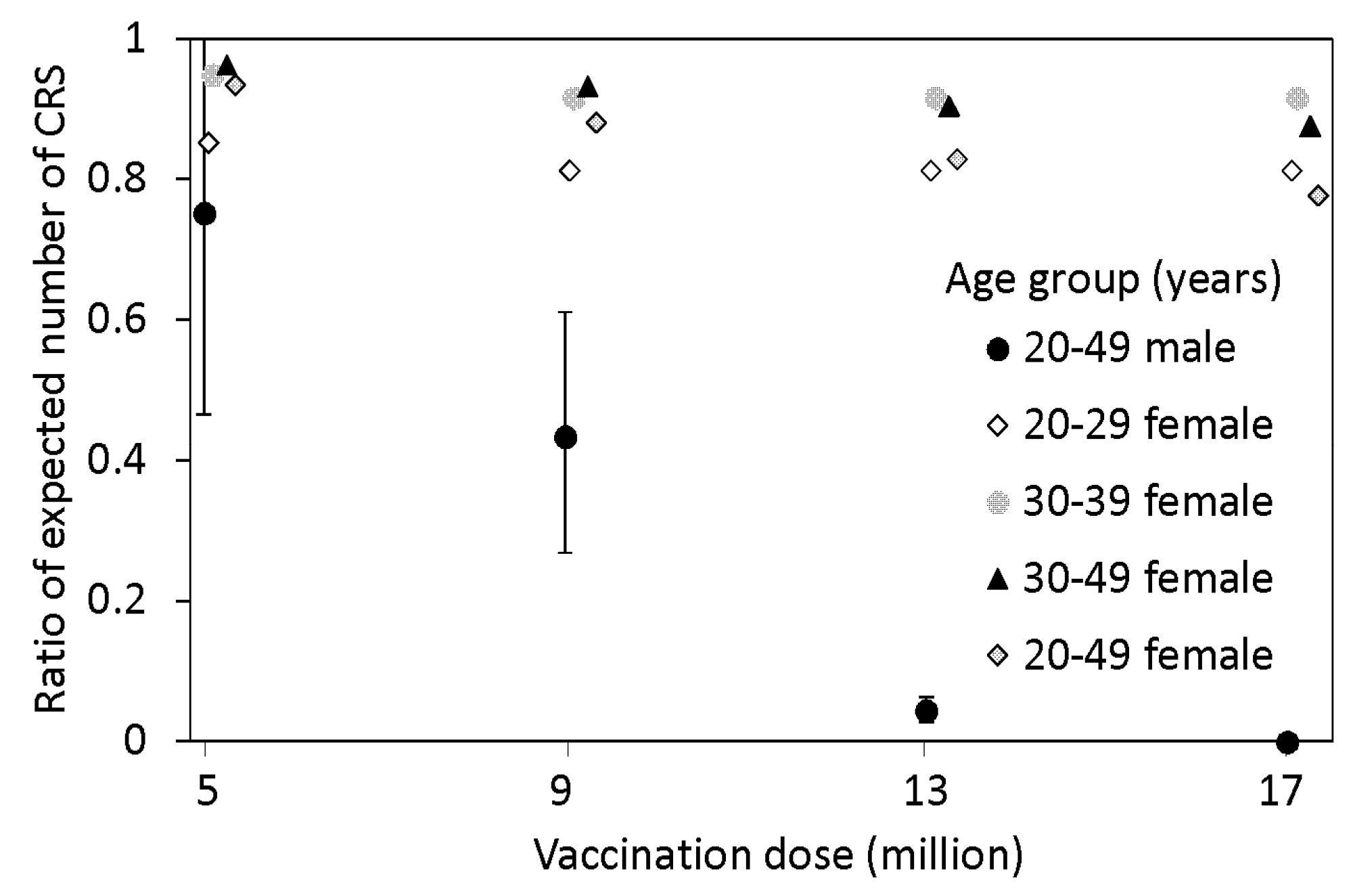
2.2.2. Prediction of Congenital Rubella Syndrome
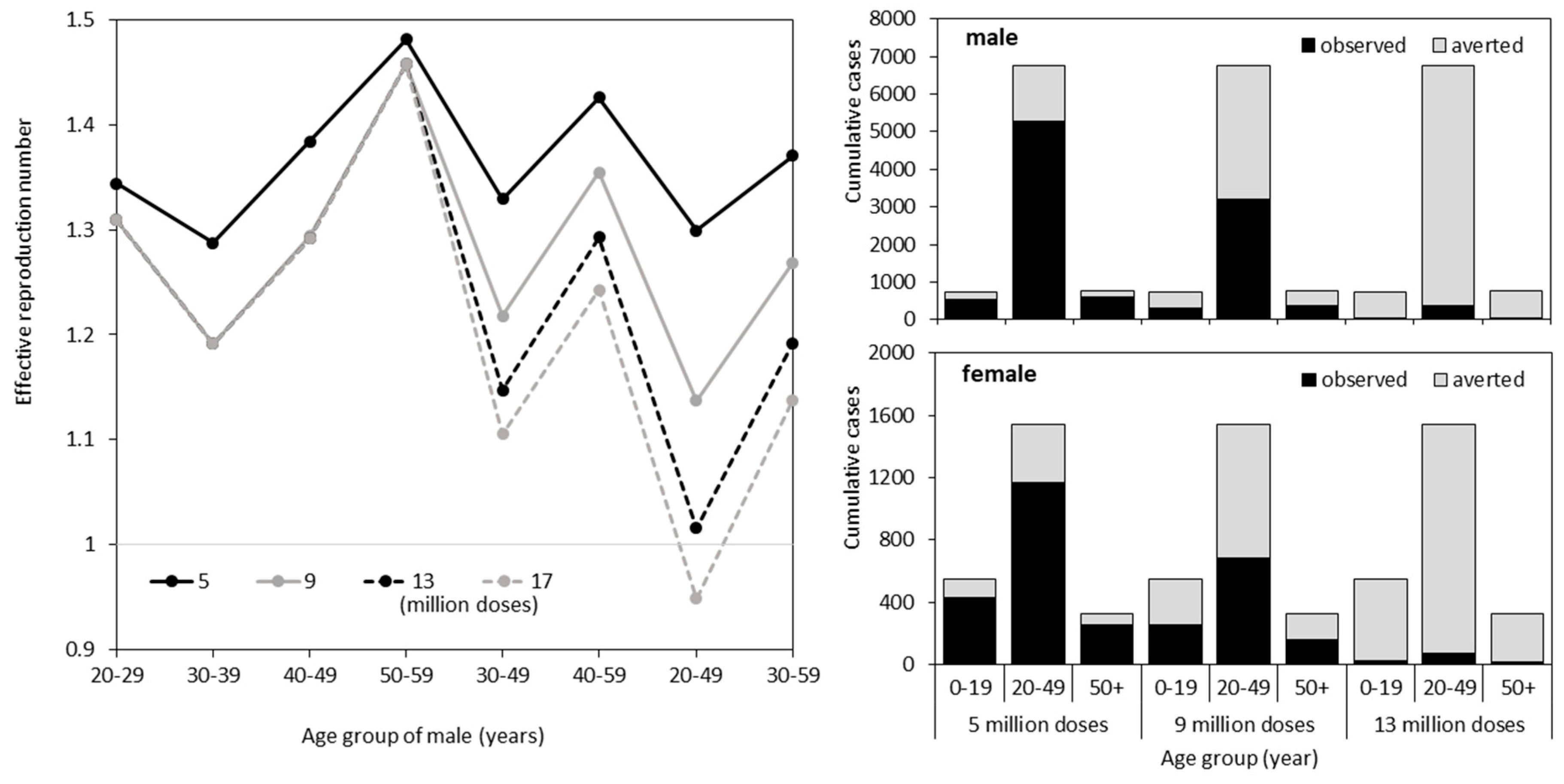
2.2.3. SIP Scenarios
2.3. Ethical Considerations
2.4. Data Sharing Policy
3. Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- Lambert, N.; Strebel, P.; Orenstein, W.; Icenogle, J.; Poland, G.A. Rubella. Lancet 2015, 385, 2297–2307. [Google Scholar] [CrossRef] [Green Version]
- Menser, M.; Forrest, J.; Bransby, R. Rubella infection and diabetes mellitus. Lancet 1978, 311, 57–60. [Google Scholar] [CrossRef]
- Tang, J.W.; Aarons, E.; Hesketh, L.M.; Strobel, S.; Schalasta, G.; Jauniaux, E.; Brink, S.; Enders, G. Prenatal diagnosis of congenital rubella infection in the second trimester of pregnancy. Prenatal Diag. 2003, 23, 509–512. [Google Scholar] [CrossRef] [PubMed]
- Banatvala, J.E.; Brown, D.W. Rubella. Lancet 2004, 363, 1127–1137. [Google Scholar] [CrossRef]
- Duszak, R.S. Congenital rubella syndrome—Major review. Optometry-J. Am. Opt. Assoc. 2009, 80, 36–43. [Google Scholar] [CrossRef] [PubMed]
- Anderson, R.M. The concept of herd immunity and the design of community-based immunization programmes. Vaccine 1992, 10, 928–935. [Google Scholar] [CrossRef]
- Wallinga, J.; Heijne, J.C.; Kretzschmar, M. A measles epidemic threshold in a highly vaccinated population. PLoS Med. 2005, 2. [Google Scholar] [CrossRef]
- Fine, P.; Eames, K.; Heymann, D.L. “Herd immunity”: A rough guide. Clin. Infect. Dis. 2011, 52, 911–916. [Google Scholar] [CrossRef]
- Kinoshita, R.; Nishiura, H. Assessing age-dependent susceptibility to measles in Japan. Vaccine 2017, 35, 3309–3317. [Google Scholar] [CrossRef]
- Jindai, K.; Funaki, T.; Nishijima, T.; Takakura, S.; Noda, H.; Miyake, K. Towards rubella elimination in Japan. Lancet Infect. Dis. 2018, 18, 713–714. [Google Scholar] [CrossRef]
- Terada, K. Rubella and congenital rubella syndrome in Japan: epidemiological problems. Japanese J. Infect. Dis. 2003, 56, 81–87. [Google Scholar]
- Mori, Y.; Miyoshi, M.; Kikuchi, M.; Sekine, M.; Umezawa, M.; Saikusa, M.; Matsushima, Y.; Itamochi, M.; Yasui, Y.; Kanbayashi, D.; et al. Molecular epidemiology of rubella virus strains detected around the time of the 2012–2013 epidemic in Japan. Front. Microbiol. 2017, 8. [Google Scholar] [CrossRef] [PubMed]
- National Institute of Infectious Diseases. Available online: https://www.niid.go.jp/niid/ja/diseases/ha/rubella.html (accessed on 21 February 2019).
- Anderson, R.M.; May, R.M. Vaccination against rubella and measles: quantitative investigations of different policies. Epidemiol. Infect. 1983, 90, 259–325. [Google Scholar] [CrossRef]
- Massad, E.; Azevedo-Neto, R.S.; Burattini, M.N.; Zanetta, D.M.T.; Coutinho, F.A.B.; Yang, H.M.; Moraes, J.C.; Pannuti, C.S.; Souza, V.A.U.F.; Silveira, A.S.B.; et al. Assessing the efficacy of a mixed vaccination strategy against rubella in São Paulo, Brazil. Int. J. Epidemiol. 1995, 24, 842–850. [Google Scholar] [CrossRef] [PubMed]
- Cutts, F.T.; Lessler, J.; Metcalf, C.J. Measles elimination: progress, challenges and implications for rubella control. Exp. Rev. Vaccines 2013, 12, 917–932. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Lee, H.; Kayano, T.; Nishiura, H. Predicting congenital rubella syndrome in Japan, 2018–2019. Int. J. Infect. Dis. 2019, in press. [Google Scholar] [CrossRef]
- Statistics Bureau, Ministry of Internal Affairs and Communication. Available online: http://www.stat.go.jp/data/jinsui/2.html (accessed on 21 February 2019).
- Panagiotopoulos, T.; Berger, A.; Valassi-Adam, E. Increase in congenital rubella occurrence after immunisation in Greece: retrospective survey and systematic review How does herd immunity work? BMJ 1999, 319, 1462–1467. [Google Scholar] [CrossRef] [Green Version]
- Metcalf, C.J.E.; Lessler, J.; Klepac, P.; Cutts, F.; Grenfell, B.T. Impact of birth rate, seasonality and transmission rate on minimum levels of coverage needed for rubella vaccination. Epidemiol. Infect. 2012, 140, 2290–2301. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Vink, M.A.; Bootsma, M.C.J.; Wallinga, J. Serial intervals of respiratory infectious diseases: A systematic review and analysis. Am. J. Epidemiol. 2014, 180, 865–875. [Google Scholar] [CrossRef]
- Munasinghe, L.; Asai, Y.; Nishiura, H. Quantifying heterogeneous contact patterns in Japan: A social contact survey. Theoret. Biol. Med. Model. 2019. conditionally accepted. [Google Scholar] [CrossRef] [PubMed]
- Infectious Diseases Weekly Report (IDWR), National Institute of Infectious Diseases. Available online: http://www.niid.go.jp/niid/ja/rubella-m-111/rubella-top/700-idsc/2131-rubella-doko.html (accessed on 22 February 2019).
- Nishiura, H.; Kinoshita, R.; Miyamatsu, Y.; Mizumoto, K. Investigating the immunizing effect of the rubella epidemic in Japan, 2012-14. Int. J. Infect. Dis. 2015, 38, 16–18. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Nishiura, H.; Chowell, G.; Safan, M.; Castillo-Chavez, C. Pros and cons of estimating the reproduction number from early epidemic growth rate of influenza A (H1N1) 2009. Theoret. Biol. Med. Model. 2010, 7. [Google Scholar] [CrossRef] [PubMed]
- Mizumoto, K.; Yamamoto, T.; Nishiura, H. Age-dependent estimates of the epidemiological impact of pandemic influenza (H1N1-2009) in Japan. Comp. Mat. Met. Med. 2013, 2013. [Google Scholar] [CrossRef]
- Castillo-Solórzano, C.; Marsigli, C.; Bravo-Alcántara, P.; Flannery, B.; Ruiz Matus, C.; Tambini, G.; Gross-Galiano, S.; Andrus, J.K. Elimination of rubella and congenital rubella syndrome in the Americas. J. Infect. Dis. 2011, 204, S571–S578. [Google Scholar] [CrossRef] [PubMed]
- Svensson, Å. A note on generation times in epidemic models. Mat. Biosci. 2007, 208, 300–311. [Google Scholar] [CrossRef] [Green Version]
- Cowling, B.J.; Fang, V.J.; Riley, S.; Peiris, J.M.; Leung, G.M. Estimation of the serial interval of influenza. Epidemiology 2009, 20, 344–347. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Orenstein, W.A.; Gay, N.J. The theory of measles elimination: implications for the design of elimination strategies. J. Infect. Dis. 2004, 189, S27–S35. [Google Scholar] [CrossRef] [PubMed]
- Winter, A.K.; Martinez, M.E.; Cutts, F.T.; Moss, W.J.; Ferrari, M.J.; McKee, A.; Lessler, J.; Hayford, K.; Wallinga, J.; Metcalf, C.J.E. Benefits and challenges in using seroprevalence data to inform models for measles and rubella elimination. J. Infect. Dis. 2018, 218, 355–364. [Google Scholar] [CrossRef] [PubMed]
- Vynnycky, E.; Adams, E.J.; Cutts, F.T.; Reef, S.E.; Navar, A.M.; Simons, E.; Yoshida, L.M.; Brown, D.W.; Jackson, C.; Strebel, P.M.; et al. Using seroprevalence and immunisation coverage data to estimate the global burden of congenital rubella syndrome. 1996–2010: A systematic review. PloS ONE 2016, 11. [Google Scholar] [CrossRef] [PubMed]
- Saito, M.M.; Nishiura, H.; Higuchi, T. Reconstructing the transmission dynamics of rubella in Japan, 2012–2013. PLoS ONE 2018, 13. [Google Scholar] [CrossRef]
- Giambi, C.; Bella, A.; Filia, A.; Del Manso, M.; Nacca, G.; Declich, S.; Rota, M.C. Underreporting of congenital rubella in Italy, 2010–2014. Eur. J. Pediat. 2017, 176, 955–962. [Google Scholar] [CrossRef] [PubMed]
- Saito, M.M.; Ejima, K.; Kinoshita, R.; Nishiura, H. Assessing the Effectiveness and Cost-Benefit of Test-and-Vaccinate Policy for Supplementary Vaccination against Rubella with Limited Doses. Int. J. Environ. Res. Public Health 2018, 15, 572. [Google Scholar] [CrossRef] [PubMed]






{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Age Group | Male | (95% CI a) | Female | (95% CI) |
|---|---|---|---|---|
| 0–4 | 0.286 | (0.207, 0.392) | 0.081 | (0.052, 0.127) |
| 5–9 | 0.085 | (0.055, 0.132) | 0.058 | (0.036, 0.092) |
| 10–14 | 0.134 | (0.098, 0.183) | 0.082 | (0.056, 0.121) |
| 15–19 | 0.196 | (0.158, 0.242) | 0.185 | (0.148, 0.232) |
| 20–24 | 0.419 | (0.371, 0.473) | 0.292 | (0.249, 0.341) |
| 25–29 | 0.441 | (0.393, 0.494) | 0.354 | (0.298, 0.420) |
| 30–34 | 0.524 | (0.473, 0.580) | 0.145 | (0.111, 0.190) |
| 35–39 | 0.606 | (0.553, 0.664) | 0.104 | (0.078, 0.138) |
| 40–44 | 0.486 | (0.439, 0.538) | 0.055 | (0.038, 0.080) |
| 45–49 | 0.297 | (0.259, 0.340) | 0.054 | (0.036, 0.081) |
| 50–54 | 0.170 | (0.140, 0.207) | 0.104 | (0.077, 0.140) |
| 55–59 | 0.116 | (0.090, 0.149) | 0.075 | (0.051, 0.112) |
| 60–64 | 0.030 | (0.017, 0.054) | 0.028 | (0.013, 0.059) |
| 65–69 | 0.023 | (0.010, 0.050) | 0.034 | (0.015, 0.079) |
| 70+ | 0.004 | (0.001, 0.026) | 0.005 | (0.001, 0.025) |
© 2019 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Kayano, T.; Lee, H.; Nishiura, H. Modelling a Supplementary Vaccination Program of Rubella Using the 2012–2013 Epidemic Data in Japan. Int. J. Environ. Res. Public Health 2019, 16, 1473. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph16081473
Kayano T, Lee H, Nishiura H. Modelling a Supplementary Vaccination Program of Rubella Using the 2012–2013 Epidemic Data in Japan. International Journal of Environmental Research and Public Health. 2019; 16(8):1473. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph16081473
Chicago/Turabian StyleKayano, Taishi, Hyojung Lee, and Hiroshi Nishiura. 2019. "Modelling a Supplementary Vaccination Program of Rubella Using the 2012–2013 Epidemic Data in Japan" International Journal of Environmental Research and Public Health 16, no. 8: 1473. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph16081473