Difference in Long-Term Trends in COPD Mortality between China and the U.S., 1992–2017: An Age–Period–Cohort Analysis

 and
and
Abstract
:1. Introduction
2. Materials and Methods
2.1. Data Sources
2.2. Statistical Analysis
3. Results
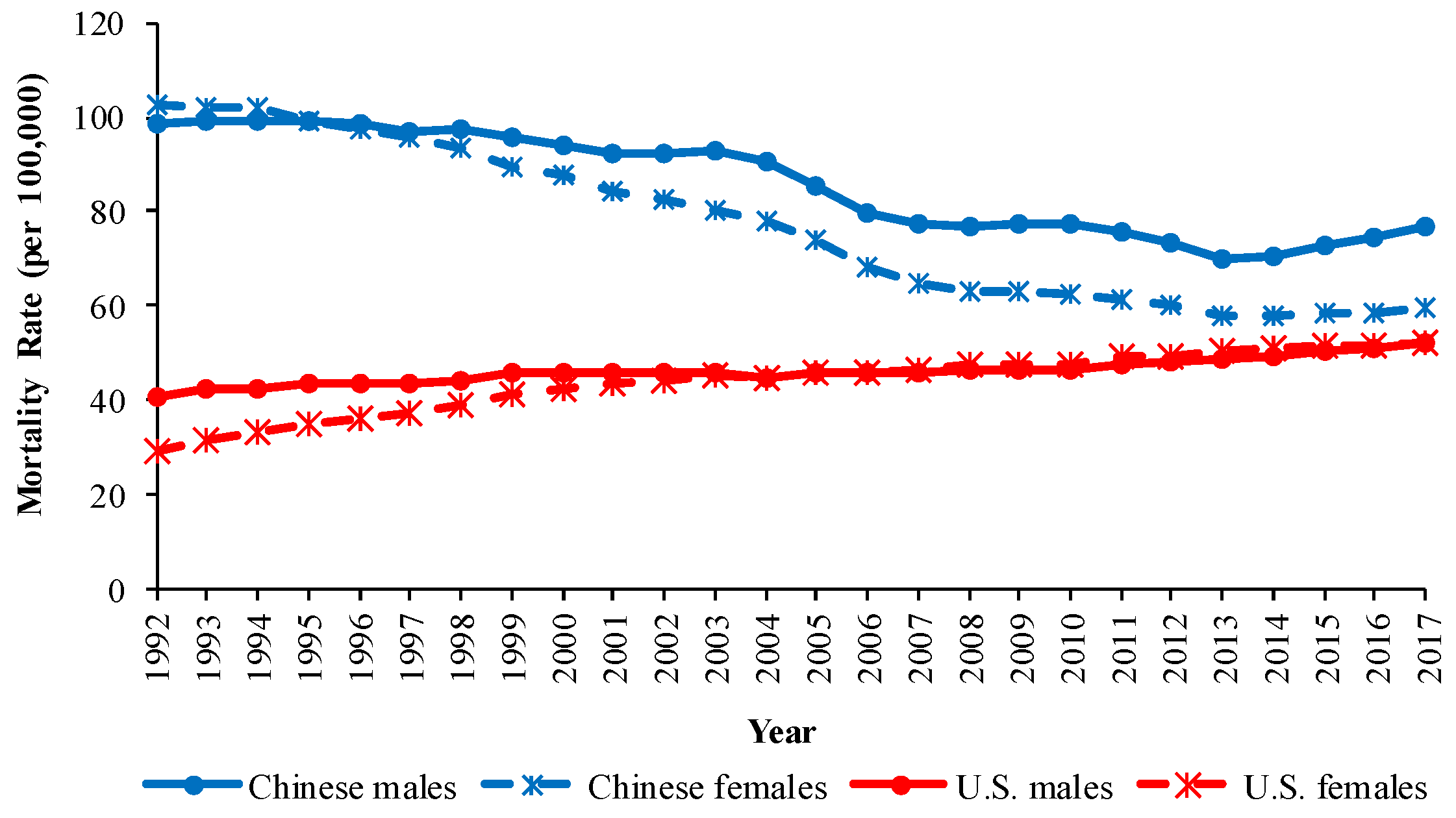
3.1. The Overall Trends in COPD Mortality in China and the U.S.
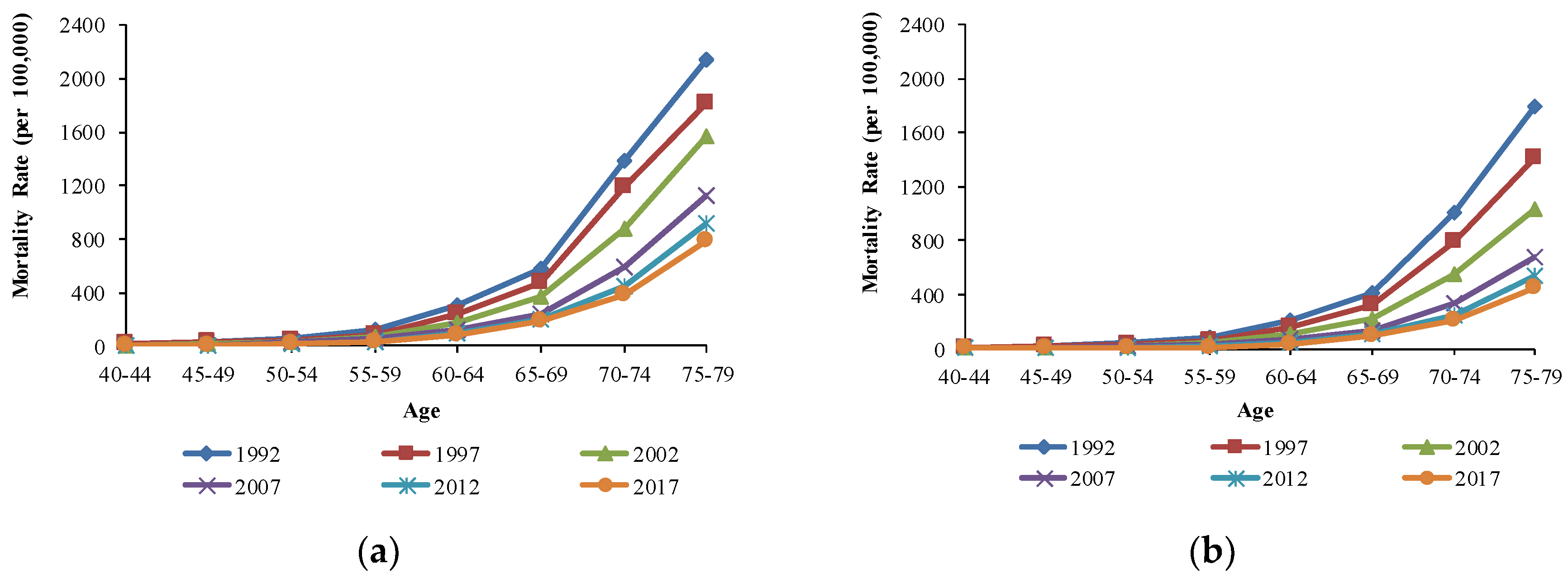
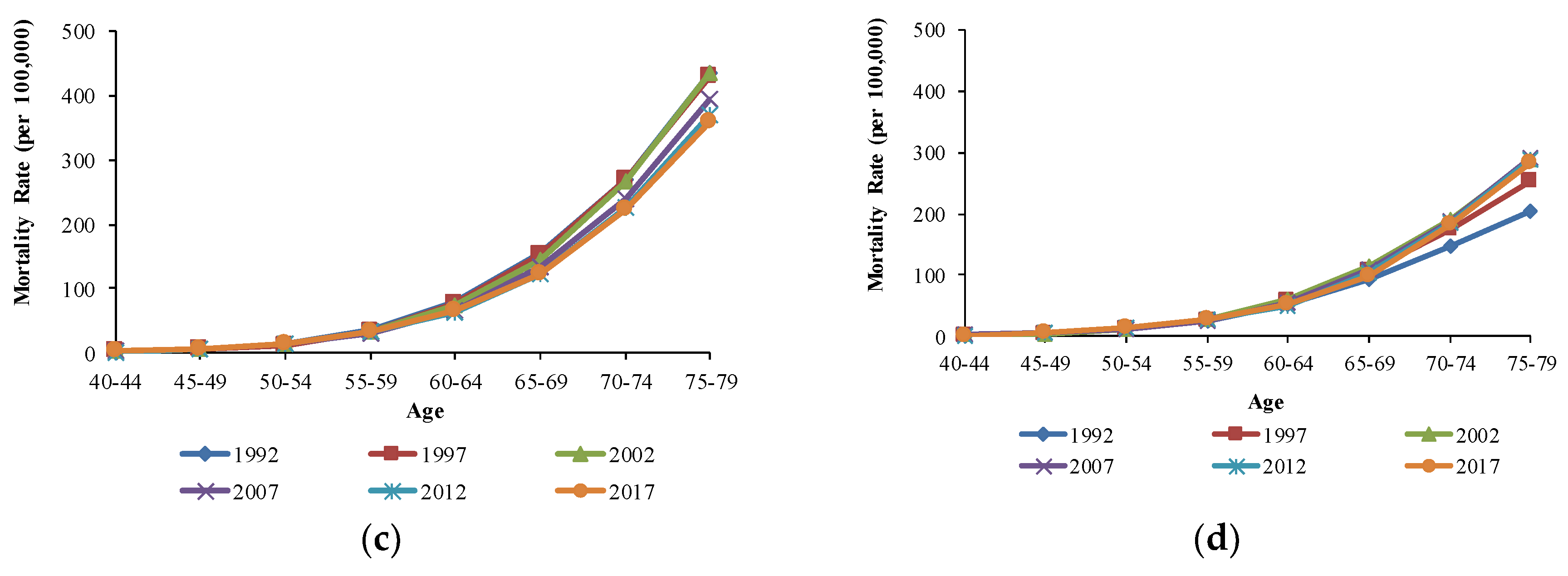
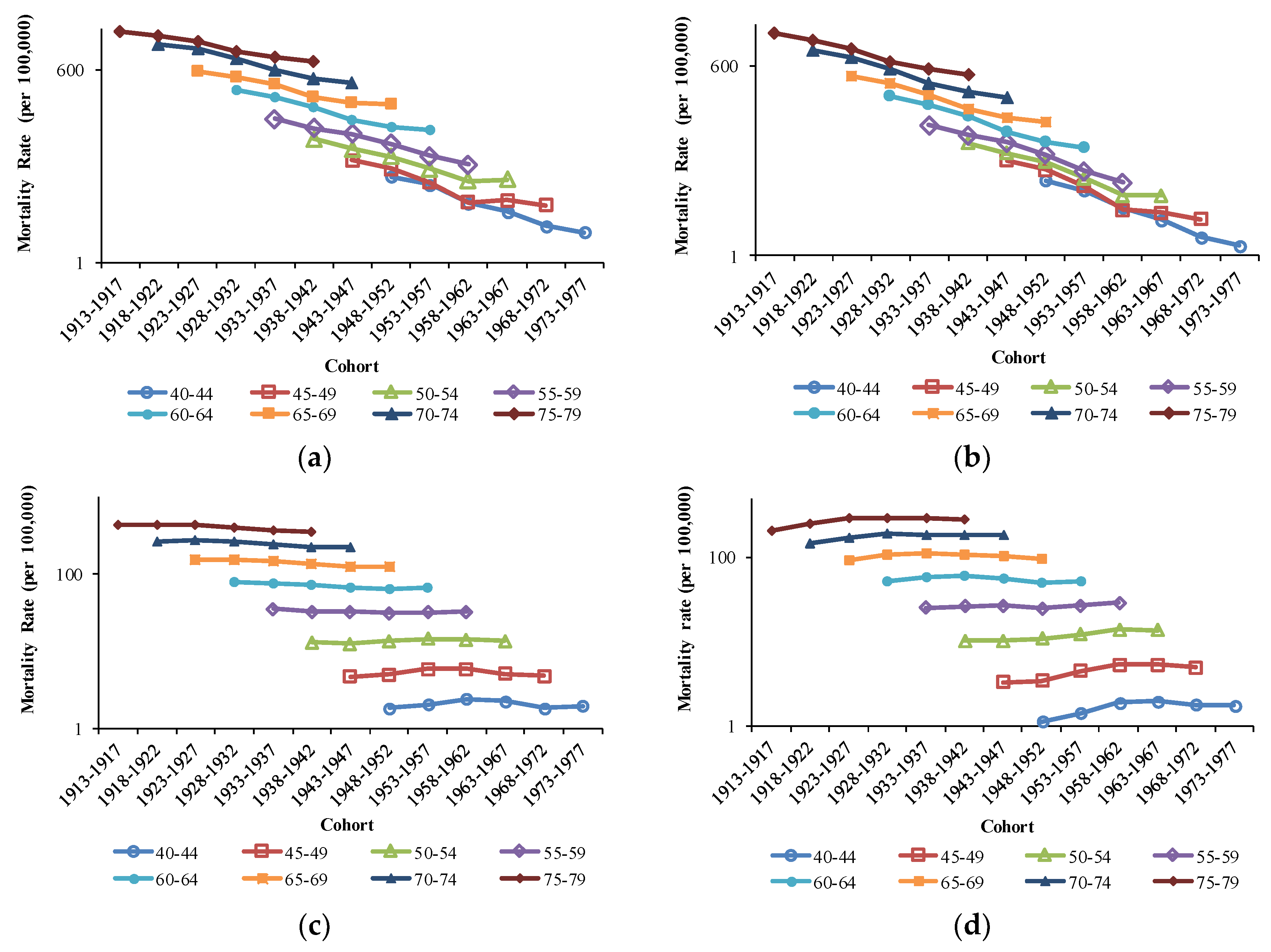
3.2. The Variation in Age, Period, and Cohort on COPD Mortality
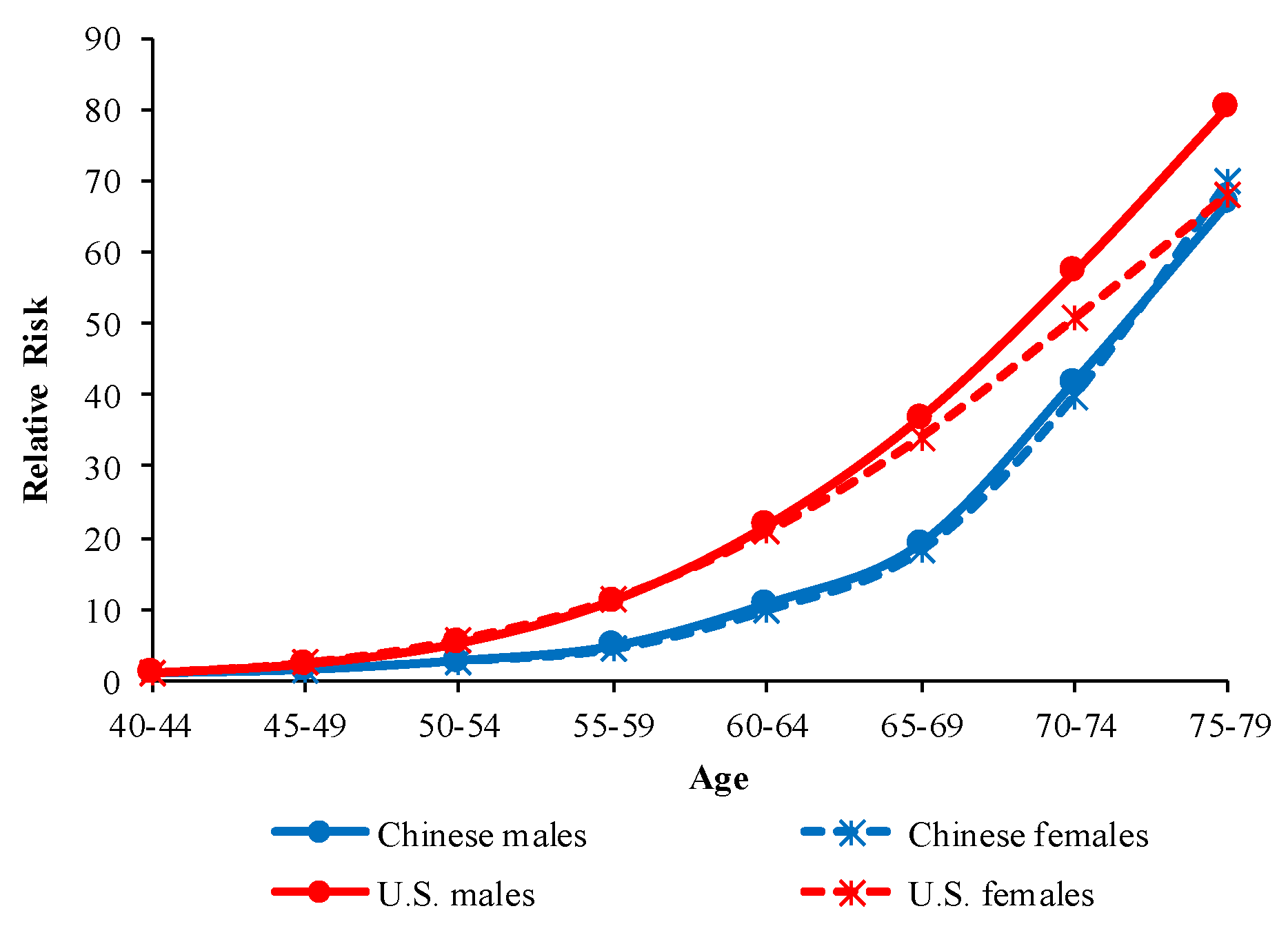
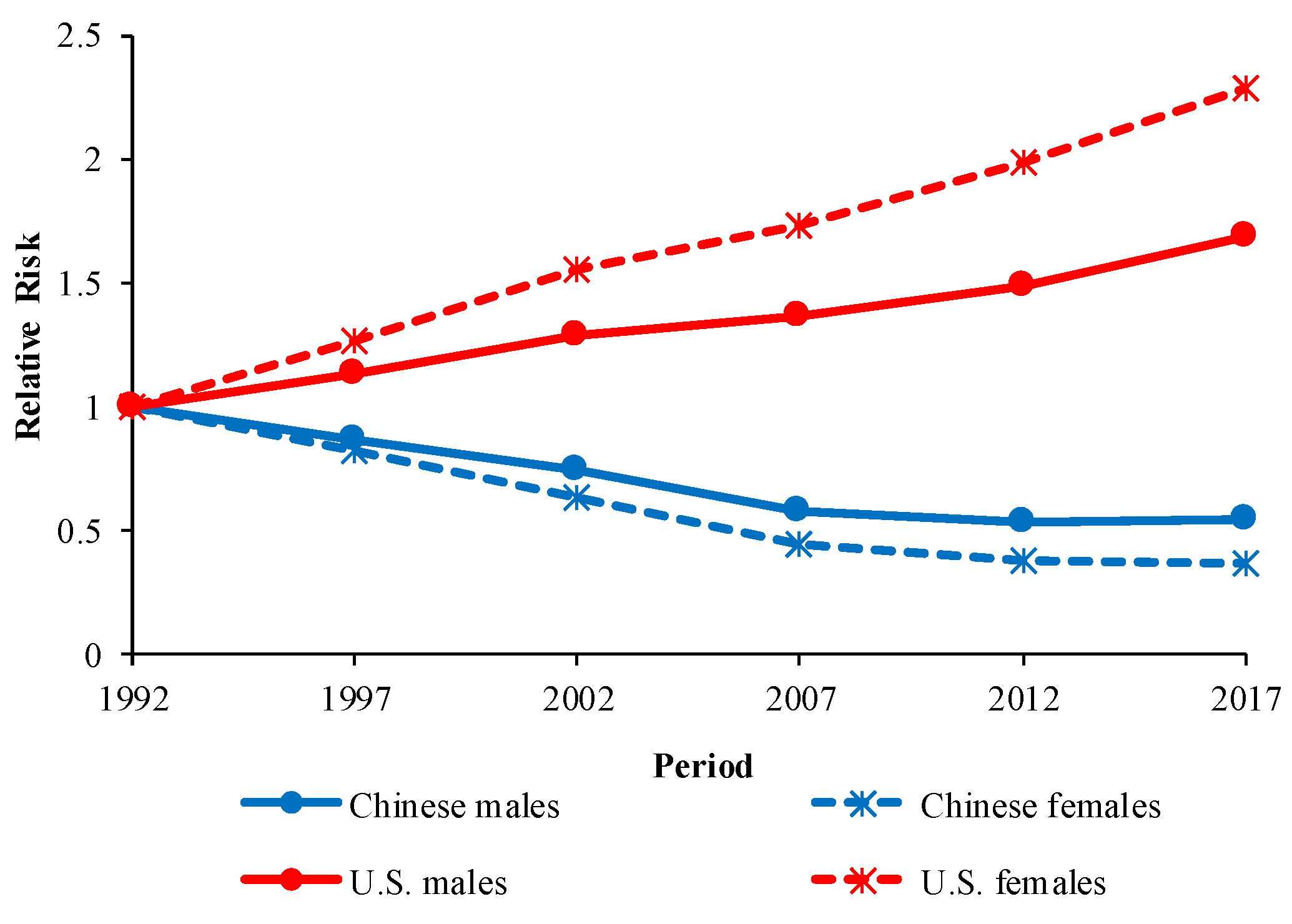
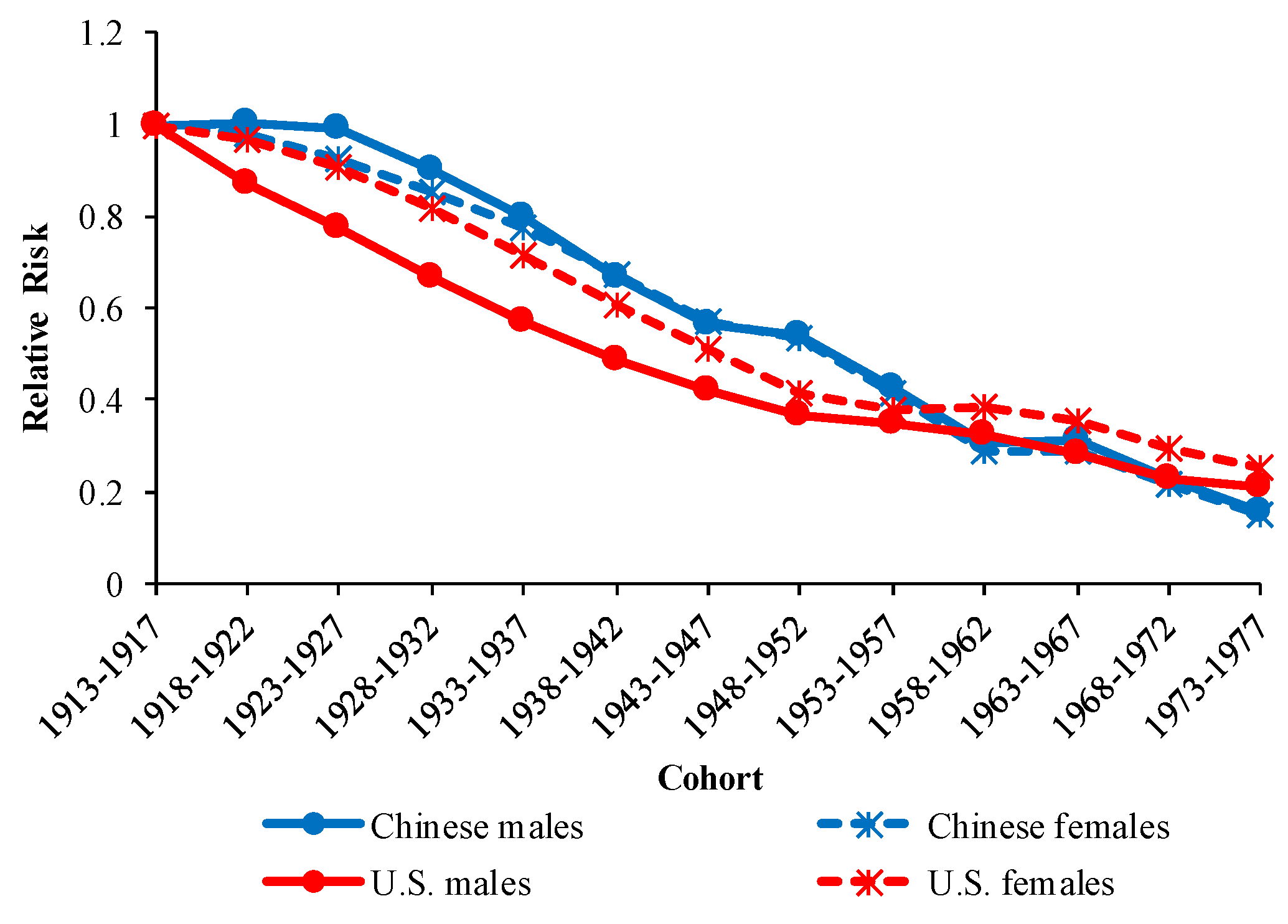
3.3. The Age, Period, and Cohort Effects on COPD Mortality
4. Discussion
5. Conclusions
Author Contributions
Funding
Conflicts of Interest
Appendix A

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Variables | Male | Female | ||||
|---|---|---|---|---|---|---|
| Coef (95%CI) | RR (95%CI) | p | Coef (95%CI) | RR (95%CI) | p | |
| Intercept | 4.47 (4.36, 4.58) | 0.00 | 3.99 (3.84, 4.15) | 0.00 | ||
| Age | ||||||
| 40–44 | −2.03 (−2.27, −1.79) | 1.00 | 0.00 | −2.01 (−2.30, −1.72) | 1.00 | 0.00 |
| 45–49 | −1.62 (−1.81, −1.44) | 1.50 (1.58, 1.42) | 0.00 | −1.52 (−1.74, −1.30) | 1.63 (1.75, 1.52) | 0.00 |
| 50–54 | −1.01 (−1.16, −0.87) | 2.76 (3.04, 2.50) | 0.00 | −1.02 (−1.19, −0.85) | 2.69 (3.03, 2.39) | 0.00 |
| 55–59 | −0.46 (−0.57, −0.36) | 4.80 (5.48, 4.20) | 0.00 | −0.53 (−0.66, −0.40) | 4.39 (5.15, 3.75) | 0.00 |
| 60–64 | 0.34 (0.26, 0.41) | 10.68 (12.60, 9.04) | 0.00 | 0.27 (0.18, 0.37) | 9.78 (11.99, 8.05) | 0.00 |
| 65–69 | 0.92 (0.86, 0.98) | 19.11 (22.86, 15.98) | 0.00 | 0.89 (0.81, 0.97) | 18.17 (22.48, 14.66) | 0.00 |
| 70–74 | 1.70 (1.64, 1.76) | 41.75 (49.88, 34.95) | 0.00 | 1.68 (1.59, 1.76) | 40.04 (49.11, 32.39) | 0.00 |
| 75–79 | 2.17 (2.09, 2.25) | 66.79 (78.54, 56.79) | 0.00 | 2.24 (2.13, 2.35) | 70.09 (84.28, 58.23) | 0.00 |
| Period | ||||||
| 1992 | 0.38 (0.30, 0.45) | 1.00 | 0.00 | 0.57 (0.48, 0.67) | 1.00 | 0.00 |
| 1997 | 0.23 (0.18, 0.28) | 0.87 (0.89, 0.85) | 0.00 | 0.37 (0.31, 0.44) | 0.82 (0.84, 0.79) | 0.00 |
| 2002 | 0.07 (0.03, 0.11) | 0.74 (0.76, 0.71) | 0.00 | 0.11 (0.07, 0.16) | 0.63 (0.66, 0.60) | 0.00 |
| 2007 | −0.18 (−0.22, −0.13) | 0.57 (0.59, 0.56) | 0.00 | −0.24 (−0.30, −0.18) | 0.44 (0.46, 0.43) | 0.00 |
| 2012 | −0.26 (−0.32, −0.21) | 0.53 (0.53, 0.52) | 0.00 | −0.39 (−0.47, −0.31) | 0.38 (0.39, 0.37) | 0.00 |
| 2017 | −0.24 (−0.32, −0.16) | 0.54 (0.54, 0.54) | 0.00 | −0.42 (−0.53, −0.32) | 0.37 (0.37, 0.37) | 0.00 |
| Cohort | ||||||
| 1913–1917 | 0.65 (0.53, 0.77) | 1.00 | 0.00 | 0.68 (0.52, 0.84) | 1.00 | 0.00 |
| 1918–1922 | 0.65 (0.55, 0.75) | 1.00 (1.02, 0.98) | 0.00 | 0.66 (0.52, 0.79) | 0.98 (1.00, 0.95) | 0.00 |
| 1923–1927 | 0.64 (0.55, 0.74) | 0.99 (1.02, 0.97) | 0.00 | 0.60 (0.48, 0.73) | 0.92 (0.95, 0.89) | 0.00 |
| 1928–1932 | 0.54 (0.45, 0.64) | 0.90 (0.92, 0.87) | 0.00 | 0.53 (0.40, 0.65) | 0.86 (0.88, 0.83) | 0.00 |
| 1933–1937 | 0.43 (0.32, 0.53) | 0.80 (0.82, 0.79) | 0.00 | 0.43 (0.29, 0.57) | 0.78 (0.79, 0.76) | 0.00 |
| 1938–1942 | 0.25 (0.13, 0.36) | 0.67 (0.67, 0.66) | 0.00 | 0.29 (0.13, 0.44) | 0.68 (0.68, 0.67) | 0.00 |
| 1943–1947 | 0.08 (−0.06, 0.22) | 0.57 (0.56, 0.57) | 0.26 | 0.13 (−0.06, 0.31) | 0.58 (0.56, 0.59) | 0.18 |
| 1948–1952 | 0.04 (−0.13, 0.20) | 0.54 (0.52, 0.57) | 0.65 | 0.06 (−0.16, 0.28) | 0.54 (0.51, 0.57) | 0.59 |
| 1953–1957 | −0.20 (−0.40, 0.01) | 0.43 (0.39, 0.47) | 0.06 | −0.19 (−0.47, 0.08) | 0.42 (0.37, 0.47) | 0.17 |
| 1958–1962 | −0.54 (−0.82, −0.26) | 0.30 (0.26, 0.36) | 0.00 | −0.56 (−0.94, −0.18) | 0.29 (0.23, 0.36) | 0.00 |
| 1963–1967 | −0.51 (−0.86, −0.16) | 0.31 (0.25, 0.40) | 0.00 | −0.55 (−1.03, −0.08) | 0.29 (0.21, 0.40) | 0.02 |
| 1968–1972 | −0.82 (−1.32, −0.31) | 0.23 (0.16, 0.34) | 0.00 | −0.86 (−1.55, −0.17) | 0.21 (0.13, 0.36) | 0.02 |
| 1973–1977 | −1.22 (−2.34, −0.10) | 0.15 (0.06, 0.42) | 0.03 | −1.20 (−2.73, 0.32) | 0.15 (0.04, 0.60) | 0.12 |
| AIC | 7.67 | 7.04 | ||||
| BIC | −78.85 | −86.69 | ||||
| Deviance | 14.06 | 6.21 | ||||
| Variables | Male | Female | ||||
|---|---|---|---|---|---|---|
| Coef (95%CI) | RR (95%CI) | p | Coef (95%CI) | RR (95%CI) | p | |
| Intercept | 3.66 (3.52,3.79) | 0.00 | 3.39 (3.25,3.53) | 0.00 | ||
| Age | ||||||
| 40–44 | −2.50 (−3.00, −2.00) | 1.00 | 0.00 | −2.47 (−3.04, −1.91) | 1.00 | 0.00 |
| 45–49 | −1.68 (−1.99, −1.36) | 2.27 (2.75, 1.90) | 0.00 | −1.59 (−1.94, −1.24) | 2.42 (1.95, 3.00) | 0.00 |
| 50–54 | −0.85 (−1.08, −0.62) | 5.21 (6.82, 3.97) | 0.00 | −0.73 (−0.99, −0.48) | 5.68 (4.18, 7.77) | 0.00 |
| 55–59 | −0.09 (−0.26, 0.09) | 11.13 (15.49, 8.08) | 0.32 | −0.04 (−0.23, 0.16) | 11.40 (7.92,16.61) | 0.71 |
| 60–64 | 0.58 (0.44, 0.71) | 21.76 (31.19, 15.03) | 0.00 | 0.57 (0.42, 0.71) | 20.82 (13.74, 31.82) | 0.00 |
| 65–69 | 1.11 (1.00, 1.21) | 36.97 (54.60, 24.78) | 0.00 | 1.06 (0.94, 1.17) | 34.08 (21.76, 53.52) | 0.00 |
| 70–74 | 1.55 (1.45, 1.64) | 57.40 (85.63, 38.09) | 0.00 | 1.46 (1.36, 1.56) | 50.73 (32.14, 81.45) | 0.00 |
| 75–79 | 1.89 (1.79, 1.99) | 80.64 (120.3, 54.05) | 0.00 | 1.75 (1.65, 1.85) | 68.07 (42.95, 108.85) | 0.00 |
| Period | ||||||
| 1992 | −0.27 (−0.39, −0.15) | 1.00 | 0.00 | −0.46 (−0.59, −0.32) | 1.00 | 0.00 |
| 1997 | −0.15 (−0.23, −0.06) | 1.13 (1.17, 1.09) | 0.00 | −0.22 (−0.32, −0.12) | 1.26 (1.22, 1.31) | 0.00 |
| 2002 | −0.02 (−0.08, 0.05) | 1.28 (1.36, 1.22) | 0.64 | −0.02 (−0.10, 0.06) | 1.55 (1.46, 1.63) | 0.65 |
| 2007 | 0.04 (−0.03, 0.11) | 1.36 (1.43, 1.30) | 0.26 | 0.09 (0.01, 0.17) | 1.73 (1.63, 1.82) | 0.02 |
| 2012 | 0.13 (0.04, 0.22) | 1.49 (1.54, 1.45) | 0.00 | 0.23 (0.13, 0.32) | 1.98 (1.90, 2.05) | 0.00 |
| 2017 | 0.26 (0.15, 0.37) | 1.70 (1.72, 1.68) | 0.00 | 0.37 (0.25, 0.49) | 2.29 (2.25, 2.32) | 0.00 |
| Cohort | ||||||
| 1913–1917 | 0.80 (0.62, 0.98) | 1.00 | 0.00 | 0.64 (0.43, 0.84) | 1.00 | 0.00 |
| 1918–1922 | 0.66 (0.52, 0.81) | 0.87 (0.90, 0.84) | 0.00 | 0.61 (0.44, 0.77) | 0.97 (0.93, 1.01) | 0.00 |
| 1923–1927 | 0.55 (0.42, 0.67) | 0.78 (0.82, 0.73) | 0.00 | 0.54 (0.39, 0.68) | 0.90 (0.85, 0.96) | 0.00 |
| 1928–1932 | 0.40 (0.28, 0.53) | 0.67 (0.71, 0.64) | 0.00 | 0.43 (0.30, 0.57) | 0.82 (0.76, 0.88) | 0.00 |
| 1933–1937 | 0.24 (0.10, 0.37) | 0.57 (0.59, 0.54) | 0.00 | 0.30 (0.15, 0.45) | 0.72 (0.68, 0.76) | 0.00 |
| 1938–1942 | 0.08 (−0.06, 0.23) | 0.49 (0.51, 0.47) | 0.27 | 0.14 (−0.02, 0.30) | 0.61 (0.58, 0.64) | 0.09 |
| 1943–1947 | −0.07 (−0.25, 0.11) | 0.42 (0.42, 0.42) | 0.48 | −0.03 (−0.23, 0.16) | 0.51 (0.51, 0.52) | 0.75 |
| 1948–952 | −0.21 (−0.43, 0.01) | 0.36 (0.35, 0.38) | 0.06 | −0.25 (−0.49, −0.01) | 0.41 (0.43, 0.40) | 0.04 |
| 1953−1957 | −0.26 (−0.52, 0.01) | 0.35 (0.32, 0.38) | 0.06 | −0.34 (−0.62, −0.05) | 0.38 (0.41, 0.35) | 0.02 |
| 1958−1962 | −0.32 (−0.64, 0.01) | 0.33 (0.28, 0.38) | 0.06 | −0.32 (−0.66, 0.02) | 0.38 (0.44, 0.34) | 0.07 |
| 1963−1967 | −0.46 (−0.88, −0.03) | 0.28 (0.22, 0.36) | 0.04 | −0.39 (−0.83, 0.04) | 0.36 (0.45, 0.28) | 0.08 |
| 1968−1972 | −0.67 (−1.31, −0.04) | 0.23 (0.15, 0.36) | 0.04 | −0.58 (−1.22, 0.06) | 0.30 (0.46, 0.19) | 0.08 |
| 1973−1977 | −0.76 (−2.14, 0.62) | 0.21 (0.06, 0.70) | 0.28 | −0.74 (−2.21, 0.72) | 0.25 (0.89, 0.07) | 0.32 |
| AIC | 6.51 | 6.26 | ||||
| BIC | −92.21 | −92.00 | ||||
| Deviance | 0.70 | 0.91 | ||||
References
- Kim, Y.S. Definition and Epidemiology of COPD. In COPD: Heterogeneity and Personalized Treatment; Springer: Berlin, Germany, 2017; pp. 3–7. [Google Scholar]
- Lopez-Campos, J.L.; Tan, W.; Soriano, J.B. Global burden of COPD. Respirology 2016, 21, 14–23. [Google Scholar] [CrossRef]
- Yang, G.; Wang, Y.; Zeng, Y.; Gao, G.F.; Liang, X.; Zhou, M.; Wan, X.; Yu, S.; Jiang, Y.; Naghavi, M.; et al. Rapid health transition in China, 1990–2010: Findings from the Global Burden of Disease Study 2010. Lancet 2013, 381, 1987–2015. [Google Scholar] [CrossRef]
- Centers for Disease Control and Prevention. Chronic obstructive pulmonary disease among adults—United States, 2011. MMWR. Morb. Mortal. Wkly. Rep. 2012, 61, 938. [Google Scholar]
- Rawla, P.; Sunkara, T.; Gaduputi, V. Epidemiology of Pancreatic Cancer: Global Trends, Etiology and Risk Factors. World J. Oncol. 2019, 10, 10–27. [Google Scholar] [CrossRef]
- Rawla, P.; Sunkara, T.; Muralidharan, P.; Raj, J.P. Update in global trends and aetiology of hepatocellular carcinoma. Contemp. Oncol. 2018, 22, 141–150. [Google Scholar] [CrossRef]
- Rawla, P.; Barsouk, A. Epidemiology of gastric cancer: Global trends, risk factors and prevention. Prz. Gastroenterol. 2019, 14, 26–38. [Google Scholar] [CrossRef] [PubMed]
- Ren, Y.; Zhang, M.; Luo, X.; Zhao, J.; Yin, L.; Pang, C.; Feng, T.; Wang, S.; Wang, B.; Zhang, H.; et al. Secular trend of the leading causes of death in China from 2003 to 2013. Afr. Health Sci. 2017, 17, 532–537. [Google Scholar] [CrossRef] [Green Version]
- Institute for Health Metrics and Evaluation. GBD Results Tool 2017. Available online: http://ghdx.healthdata.org/gbd-results-tool (accessed on 8 November 2018).
- Ford, E.S.; Croft, J.B.; Mannino, D.M.; Wheaton, A.G.; Zhang, X.Y.; Giles, W.H. COPD Surveillance-United States, 1999–2011. Chest 2013, 144, 284–305. [Google Scholar] [CrossRef] [PubMed]
- Wang, C.; Xu, J.; Yang, L.; Xu, Y.; Zhang, X.; Bai, C.; Kang, J.; Ran, P.; Shen, H.; Wen, F.; et al. Prevalence and risk factors of chronic obstructive pulmonary disease in China (the China Pulmonary Health [CPH] study): A national cross-sectional study. Lancet 2018, 391, 1706–1717. [Google Scholar] [CrossRef]
- Reilly, K.H.; Gu, D.; Duan, X.; Wu, X.; Chen, C.S.; Huang, J.; Kelly, T.N.; Chen, J.; Liu, X.; Yu, L.; et al. Risk factors for chronic obstructive pulmonary disease mortality in Chinese adults. Am. J. Epidemiol. 2008, 167, 998–1004. [Google Scholar] [CrossRef]
- Qiu, H.; Tan, K.; Long, F.Y.; Wang, L.Y.; Yu, H.Y.; Deng, R.; Long, H.; Zhang, Y.L.; Pan, J.P. The Burden of COPD Morbidity Attributable to the Interaction between Ambient Air Pollution and Temperature in Chengdu, China. Int. J. Environ. Res. Public Health 2018, 15, 492. [Google Scholar] [CrossRef]
- Brown, D.W.; Croft, J.B.; Greenlund, K.J.; Giles, W.H. Trends in Hospitalization with Chronic Obstructive Pulmonary Disease—United States, 1990—2005. COPD 2010, 7, 59–62. [Google Scholar] [CrossRef]
- Yin, P.; Wang, H.; Vos, T.; Li, Y.; Liu, S.; Liu, Y.; Liu, J.; Wang, L.; Naghavi, M.; Murray, C.J.; et al. A Subnational Analysis of Mortality and Prevalence of COPD in China from 1990 to 2013: Findings from the Global Burden of Disease Study 2013. Chest 2016, 150, 1269–1280. [Google Scholar] [CrossRef]
- Ford, E.S. Trends in Mortality from COPD among Adults in the United States. Chest 2015, 148, 962–970. [Google Scholar] [CrossRef]
- GBD 2017 Mortality Collaborators. Global, regional, and national age-sex-specific mortality for 282 causes of death in 195 countries and territories, 1980–2017: A systematic analysis for the Global Burden of Disease Study 2017. Lancet 2018, 392, 1736–1788. [Google Scholar] [CrossRef]
- Zhou, M.; Wang, H.; Zhu, J.; Chen, W.; Wang, L.; Liu, S.; Li, Y.; Wang, L.; Liu, Y.; Yin, P.; et al. Cause-specific mortality for 240 causes in China during 1990–2013: A systematic subnational analysis for the Global Burden of Disease Study 2013. Lancet 2016, 387, 251–272. [Google Scholar] [CrossRef]
- GBD 2015 Chronic Respiratory Disease Collaborators. Global, regional, and national deaths, prevalence, disability-adjusted life years, and years lived with disability for chronic obstructive pulmonary disease and asthma, 1990–2015: A systematic analysis for the Global Burden of Disease Study 2015. Lancet Respir. Med. 2017, 5, 691–706. [Google Scholar] [CrossRef]
- Yang, Y. Trends in US adult chronic disease mortality, 1960–1999: Age, period, and cohort variations. Demography 2008, 45, 387–416. [Google Scholar] [CrossRef]
- Yang, Y.; Land, K.C. Age-Period-Cohort Analysis: New Models, Methods, and Empirical Applications; Chapman and Hall/CRC: London, UK, 2016. [Google Scholar]
- Mason, K.O.; Mason, W.M.; Winsborough, H.H.; Poole, W.K. Some methodological issues in cohort analysis of archival data. Am. Sociol. Rev. 1973, 38, 242–258. [Google Scholar] [CrossRef]
- Yang, Y.; Schulhofer-Wohl, S.; Fu, W.J.J.; Land, K.C. The intrinsic estimator for age-period-cohort analysis: What it is and how to use it. Am. J. Sociol. 2008, 113, 1697–1736. [Google Scholar] [CrossRef]
- Yang, Y.; Fu, W.J.J.; Land, K.C. A methodological comparison of age-period-cohort models: The intrinsic estimator and conventional generalized linear models. Sociol. Methodol. 2004, 34, 75–110. [Google Scholar] [CrossRef]
- Luo, L. Assessing validity and application scope of the intrinsic estimator approach to the age-period-cohort problem. Demography 2013, 50, 1945–1967. [Google Scholar] [CrossRef]
- Tantucci, C.; Modina, D. Lung function decline in COPD. Int. J. Chronic Obstr. Pulm. Dis. 2012, 7, 95–99. [Google Scholar] [CrossRef] [Green Version]
- Makris, D.; Moschandreas, J.; Damianaki, A.; Ntaoukakis, E.; Siafakas, N.M.; Emili, J.M.; Tzanakis, N. Exacerbations and lung function decline in COPD: New insights in current and ex-smokers. Respir. Med. 2007, 101, 1305–1312. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Stanojevic, S.; Wade, A.; Stocks, J.; Hankinson, J.; Coates, A.L.; Pan, H.; Rosenthal, M.; Corey, M.; Lebecque, P.; Cole, T.J. Reference ranges for spirometry across all ages—A new approach. Am. J. Respir. Crit. Care 2008, 177, 253–260. [Google Scholar] [CrossRef] [PubMed]
- Sharma, G.; Hanania, N.A.; Shim, Y.; Shim, M. The aging immune system and its relationship to the development of chronic obstructive pulmonary disease. Proc. Am. Thorac. Soc. 2009, 6, 573–580. [Google Scholar] [CrossRef]
- Lin, H.H.; Murray, M.; Cohen, T.; Colijn, C.; Ezzati, M. Effects of smoking and solid-fuel use on COPD, lung cancer, and tuberculosis in China: A time-based, multiple risk factor, modelling study. Lancet 2008, 372, 1473–1483. [Google Scholar] [CrossRef]
- Lam, K.B.H.; Yin, P.; Jiang, C.Q.; Zhang, W.S.; Adab, P.; Miller, M.R.; Thomas, G.N.; Ayres, J.G.; Lam, T.H.; Cheng, K.K. Past dust and GAS/FUME exposure and COPD in Chinese: The Guangzhou Biobank Cohort Study. Respir. Med. 2012, 106, 1421–1428. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- United Nations Department of Economic and Social Affairs. Interactive Data—Profiles of Ageing 2017. Available online: https://population.un.org/ProfilesOfAgeing2017/index.html (accessed on 12 December 2018).
- Anderson, R.N.; Miniño, A.M.; Hoyert, D.L.; Rosenberg, H.M. Comparability of cause of death between ICD-9 and ICD-10: Preliminary estimates. Natl. Vital Stat. Rep. 2001, 49, 1–32. [Google Scholar]
- Mannino, D.M.; Homa, D.M.; Akinbami, L.J.; Ford, E.S.; Redd, S.C.J. Chronic obstructive pulmonary disease surveillance-United States, 1971–2000. Respir. Care 2002, 47, 1184–1199. [Google Scholar]
- Centers for Disease Control and Prevention. Tobacco use—United States, 1900–1999. MMWR. Morb. Mortal. Wkly. Rep. 1999, 48, 986. [Google Scholar]
- Giovino, G.A.; Schooley, M.W.; Zhu, B.P.; Chrismon, J.H.; Tomar, S.L.; Peddicord, J.P.; Merritt, R.K.; Husten, C.G.; Eriksen, M.P. Surveillance for selected tobacco-use behaviors—United States, 1900–1994. MMWR CDC Surveill Summ 1994, 43, 1–43. [Google Scholar] [PubMed]
- Kazerouni, N.; Alverson, C.J.; Redd, S.C.; Mott, J.A.; Mannino, D.M. Sex differences in COPD and lung cancer mortality trends—United States, 1968–1999. J. Women’s Health 2004, 13, 17–23. [Google Scholar] [CrossRef] [PubMed]
- Ma, J.; Ward, E.M.; Siegel, R.L.; Jemal, A. Temporal Trends in Mortality in the United States, 1969–2013. JAMA 2015, 314, 1731–1739. [Google Scholar] [CrossRef]
- Wellmann, K.F. Smoking and Health. On the Report of the Advisory Committee to the Surgeon General of the Public Health Service. Dtsch. Med. Wochenschr. 1964, 89, 1085–1086. [Google Scholar] [PubMed]
- Wang, T.W.; Asman, K.; Gentzke, A.S.; Cullen, K.A.; Holder-Hayes, E.; Reyes-Guzman, C.; Jamal, A.; Neff, L.; King, B.A. Tobacco Product Use Among Adults—United States, 2017. MMWR. Morb. Mortal. Wkly. Rep. 2018, 67, 1225–1232. [Google Scholar] [CrossRef]
- Weng, X.Z.; Hong, Z.G.; Chen, D.Y. Smoking prevalence in Chinese aged 15 and above. Chin. Med. J. 1987, 100, 886–892. [Google Scholar]
- Yang, G.; Fan, L.; Tan, J.; Qi, G.; Zhang, Y.; Samet, J.M.; Taylor, C.E.; Becker, K.; Xu, J. Smoking in China: Findings of the 1996 National Prevalence Survey. JAMA 1999, 282, 1247–1253. [Google Scholar] [CrossRef]
- Wang, M.; Luo, X.; Xu, S.; Liu, W.; Ding, F.; Zhang, X.; Wang, L.; Liu, J.; Hu, J.; Wang, W. Trends in smoking prevalence and implication for chronic diseases in China: Serial national cross-sectional surveys from 2003 to 2013. Lancet Respir. Med. 2019, 7, 35–45. [Google Scholar] [CrossRef]
- Qian, J.; Cai, M.; Gao, J.; Tang, S.; Xu, L.; Critchley, J.A. Trends in smoking and quitting in China from 1993 to 2003: National Health Service Survey data. Bull. World Health Organ. 2010, 88, 769–776. [Google Scholar] [CrossRef]
- The World Bank Database, Smoking Prevalence, Total (Ages 15+). Available online: https://data.worldbank.org/indicator/SH.PRV.SMOK?year_low_desc=true (accessed on 10 March 2019).
- Sun, Y.L.; Sin, D.D. Crisis of COPD in China: The future is now. Lancet Respir. Med. 2018, 6, 404–405. [Google Scholar] [CrossRef]
- Zhou, Y.; Wang, C.; Yao, W.; Chen, P.; Kang, J.; Huang, S.; Chen, B.; Ni, D.; Wang, X.; Wang, D.J. COPD in Chinese nonsmokers. Eur. Respir. J. 2009, 33, 509–518. [Google Scholar] [CrossRef] [Green Version]
- Syamlal, G.; Mazurek, J.M. Chronic Obstructive Pulmonary Disease Prevalence Among Adults Who Have Never Smoked, by Industry and Occupation—United States, 2013–2017. MMWR. Morb. Mortal. Wkly. Rep. 2019, 68, 303–307. [Google Scholar] [CrossRef]
- Mannino, D.M.; Gagnon, R.C.; Petty, T.L.; Lydick, E.J. Obstructive lung disease and low lung function in adults in the United States: Data from the National Health and Nutrition Examination Survey, 1988–1994. Arch. Intern. Med. 2000, 160, 1683–1689. [Google Scholar] [CrossRef]
- Celli, B.R.; Halbert, R.J.; Isonaka, S.; Schau, B. Population impact of different definitions of airway obstruction. Eur. Respir. J. 2003, 22, 268–273. [Google Scholar] [CrossRef] [Green Version]
- Gómez, F.P.; Rodriguez-Roisin, R.J. Global Initiative for Chronic Obstructive Lung Disease (GOLD) guidelines for chronic obstructive pulmonary disease. Curr. Opin. Pulm. Med. 2002, 8, 81–86. [Google Scholar] [CrossRef]
- Martinez, C.H.; Mannino, D.M.; Jaimes, F.A.; Curtis, J.L.; Han, M.K.; Hansel, N.N.; Diaz, A.A. Undiagnosed Obstructive Lung Disease in the United States Associated Factors and Long-term Mortality. Ann. Am. Thorac. Soc. 2015, 12, 1788–1795. [Google Scholar] [CrossRef]
- Halbert, R.J.; Natoli, J.L.; Gano, A.; Badamgarav, E.; Buist, A.S.; Mannino, D.M. Global burden of COPD: Systematic review and meta-analysis. Eur. Respir. J. 2006, 28, 523–532. [Google Scholar] [CrossRef]
- Zielinski, J.; Bednarek, M.; Know the Age of Your Lung Study Group. Early detection of COPD in a high-risk population using spirometric screening. Chest 2001, 119, 731–736. [Google Scholar] [CrossRef]
- Zhong, N.; Wang, C.; Yao, W.; Chen, P.; Kang, J.; Huang, S.; Chen, B.; Wang, C.; Ni, D.; Zhou, Y.; et al. Prevalence of chronic obstructive pulmonary disease in China—A large, population-based survey. Am. J. Respir. Crit. Care 2007, 176, 753–760. [Google Scholar] [CrossRef]
- Zheng, J.; Yang, J.; Zhou, X.; Zhao, L.; Hui, F.; Wang, H.; Bai, C.; Chen, P.; Li, H.; Kang, J.; et al. Roflumilast for the treatment of COPD in an Asian population: A randomized, double-blind, parallel-group study. Chest 2014, 145, 44–52. [Google Scholar] [CrossRef]
- Zheng, J.P.; Yang, L.; Wu, Y.M.; Chen, P.; Wen, Z.G.; Huang, W.J.; Shi, Y.; Wang, C.Z.; Huang, S.G.; Sun, T.Y.; et al. The efficacy and safety of combination salmeterol (50 μg)/fluticasone propionate (500 μg) inhalation twice daily via Accuhaler in Chinese patients with COPD. Chest 2007, 132, 1756–1763. [Google Scholar] [CrossRef] [PubMed]
- Wang, H.J. A dilemma of Chinese healthcare reform: How to re-define government roles? China Econ. Rev. 2009, 20, 598–604. [Google Scholar] [CrossRef]
- Wang, H.; Gusmano, M.K.; Cao, Q.J. An evaluation of the policy on community health organizations in China: Will the priority of new healthcare reform in China be a success? Health Policy 2011, 99, 37–43. [Google Scholar] [CrossRef]
- Xu, D.; Sun, B.; Wan, X.; Ke, Y. Reformation of medical education in China. Lancet 2010, 375, 1502–1504. [Google Scholar] [CrossRef]
- Zhang, C.G.; Lin, Y. Panel estimation for urbanization, energy consumption and CO2 emissions: A regional analysis in China. Energy Policy 2012, 49, 488–498. [Google Scholar] [CrossRef]
- Guan, W.-J.; Zheng, X.-Y.; Chung, K.F.; Zhong, N. Impact of air pollution on the burden of chronic respiratory diseases in China: time for urgent action. Lancet 2016, 388, 1939–1951. [Google Scholar] [CrossRef]
- Song, Q.K.; Christiani, D.C.; Wang, X.R.; Ren, J. The Global Contribution of Outdoor Air Pollution to the Incidence, Prevalence, Mortality and Hospital Admission for Chronic Obstructive Pulmonary Disease: A Systematic Review and Meta-Analysis. Int. J. Environ. Res. Public Health 2014, 11, 11822–11832. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Salvi, S.; Barnes, P.J. Is Exposure to Biomass Smoke the Biggest Risk Factor for COPD Globally? Chest 2010, 138, 3–6. [Google Scholar] [CrossRef]
- Shuhua, G.; Kun, H.; Daixong, Q.; Smith, K.R. One hundred million improved cookstoves in China: How was it done. World Dev. 1993, 21, 941–961. [Google Scholar]
- Mestl, H.E.; Aunan, K.; Seip, H.M.; Wang, S.; Zhao, Y.; Zhang, D. Urban and rural exposure to indoor air pollution from domestic biomass and coal burning across China. Sci. Total Environ. 2007, 377, 12–26. [Google Scholar] [CrossRef] [PubMed]
- Aunan, K.; Wang, S.J. Internal migration and urbanization in China: Impacts on population exposure to household air pollution (2000–2010). Sci. Total Environ. 2014, 481, 186–195. [Google Scholar] [CrossRef] [Green Version]
- Zhao, B.; Zheng, H.T.; Wang, S.X.; Smith, K.R.; Lu, X.; Aunan, K.; Gu, Y.; Wang, Y.; Ding, D.; Xing, J.; et al. Change in household fuels dominates the decrease in PM2.5 exposure and premature mortality in China in 2005–2015. Proc. Natl. Acad. Sci. USA 2018, 115, 12401–12406. [Google Scholar] [CrossRef]
- Shen, G.F. Changes from traditional solid fuels to clean household energies—Opportunities in emission reduction of primary PM2.5 from residential cookstoves in China. Biomass Bioenergy 2016, 86, 28–35. [Google Scholar] [CrossRef]
- Lei, Y.; Zhang, Q.; He, K.B.; Streets, D.G. Primary anthropogenic aerosol emission trends for China, 1990–2005. Atmos. Chem. Phys. 2011, 11, 931–954. [Google Scholar] [CrossRef] [Green Version]
- Wang, S.X.; Hao, J.M. Air quality management in China: Issues, challenges, and options. J. Environ. Sci. China 2012, 24, 2–13. [Google Scholar] [CrossRef]
- Cheng, Z.; Jiang, J.K.; Fajardo, O.; Wang, S.X.; Hao, J.M. Characteristics and health impacts of particulate matter pollution in China (2001–2011). Atmos. Environ. 2013, 65, 186–194. [Google Scholar] [CrossRef]
- Chen, B.; Hong, C.; Kan, H. Exposures and health outcomes from outdoor air pollutants in China. Toxicology 2004, 198, 291–300. [Google Scholar] [CrossRef]
- Liu, M.; Huang, Y.; Ma, Z.; Jin, Z.; Liu, X.; Wang, H.; Liu, Y.; Wang, J.; Jantunen, M.; Bi, J.; et al. Spatial and temporal trends in the mortality burden of air pollution in China: 2004–2012. Environ. Int. 2017, 98, 75–81. [Google Scholar] [CrossRef]
- Zhang, Q.; Geng, G.N.; Wang, S.W.; Richter, A.; He, K.B. Satellite remote sensing of changes in NOx emissions over China during 1996–2010. Chin. Sci. Bull. 2012, 57, 2857–2864. [Google Scholar] [CrossRef]
- Hand, J.L.; Schichtel, B.A.; Malm, W.C.; Pitchford, M.L. Particulate sulfate ion concentration and SO2 emission trends in the United States from the early 1990s through 2010. Atmos. Chem. Phys. 2012, 12, 10353–10365. [Google Scholar] [CrossRef]
- Hart, J.E.; Yanosky, J.D.; Puett, R.C.; Ryan, L.; Dockery, D.W.; Smith, T.J.; Garshick, E.; Laden, F. Spatial Modeling of PM10 and NO2 in the Continental United States, 1985–2000. Environ. Health Perspect. 2009, 117, 1690–1696. [Google Scholar] [CrossRef] [PubMed]
- Postma, D.S.; Bush, A.; van den Berge, M.J. Risk factors and early origins of chronic obstructive pulmonary disease. Lancet 2015, 385, 899–909. [Google Scholar] [CrossRef]
- Wedzicha, J.A.; Seemungal, T.A. COPD exacerbations: Defining their cause and prevention. Lancet 2007, 370, 786–796. [Google Scholar] [CrossRef]
- Yin, P.; Zhang, M.; Li, Y.; Jiang, Y.; Zhao, W.J. Prevalence of COPD and its association with socioeconomic status in China: Findings from China Chronic Disease Risk Factor Surveillance 2007. BMC Public Health 2011, 11, 586. [Google Scholar] [CrossRef] [PubMed]
- Tsang, M.C.J. Education and national development in China since 1949: Oscillating policies and enduring dilemmas. China Rev. 2000, 2000, 579–618. [Google Scholar]








© 2019 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Wen, H.; Xie, C.; Wang, L.; Wang, F.; Wang, Y.; Liu, X.; Yu, C. Difference in Long-Term Trends in COPD Mortality between China and the U.S., 1992–2017: An Age–Period–Cohort Analysis. Int. J. Environ. Res. Public Health 2019, 16, 1529. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph16091529
Wen H, Xie C, Wang L, Wang F, Wang Y, Liu X, Yu C. Difference in Long-Term Trends in COPD Mortality between China and the U.S., 1992–2017: An Age–Period–Cohort Analysis. International Journal of Environmental Research and Public Health. 2019; 16(9):1529. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph16091529
Chicago/Turabian StyleWen, Haoyu, Cong Xie, Lu Wang, Fang Wang, Yafeng Wang, Xiaoxue Liu, and Chuanhua Yu. 2019. "Difference in Long-Term Trends in COPD Mortality between China and the U.S., 1992–2017: An Age–Period–Cohort Analysis" International Journal of Environmental Research and Public Health 16, no. 9: 1529. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph16091529