The Association of Black Cardiologists (ABC) Cardiovascular Implementation Study (CVIS): A Research Registry Integrating Social Determinants to Support Care for Underserved Patients

 ,
,  , , , , ,
, , , , , {kind=link}
{kind=link}
Abstract
:1. Introduction
1.1. Importance of the Problem and Critical Barrier to Progress on Health Disparities
1.2. Realizing the Full Potential of Precision Medicine in Health and Healthcare-Can We Avoid Widening Disparities?
1.3. Increasing Costs and Complexity of Drug Discovery and Development
1.4. Knowledge Gap
2. Materials and Methods
2.1. Research Hypothesis
2.2. Approach- Collaborating Partners
2.2.1. The Association of Black Cardiologists
2.2.2. Morehouse School of Medicine (MSM)
2.2.3. The Georgia Clinical and Translational Science Alliance (GaCTSA)
2.2.4. Clinical Research Center
2.2.5. Mobile Clinical Research Vehicle
2.3. RCMI Translational Research Network
2.4. Duke Clinical Research Institute (DCRI)
2.5. Informatics Infrastructure Support for the Registry
2.5.1. Informatics for Integrating Biology and the Bedside (i2b2) and SHRINE (Shared Health Research Informatics Network)
2.5.2. Medidata Rave Electronic Data Capture (EDC)
2.5.3. Health 360x-A Mobile and Web based Patient Engagement Platform
2.5.4. Substitutable Medical Applications and Reusable Technologies (SMART)
2.5.5. SMART on Fast Health Interoperable Resources (FHIR)
2.6. Vanguard Site Principal Investigators
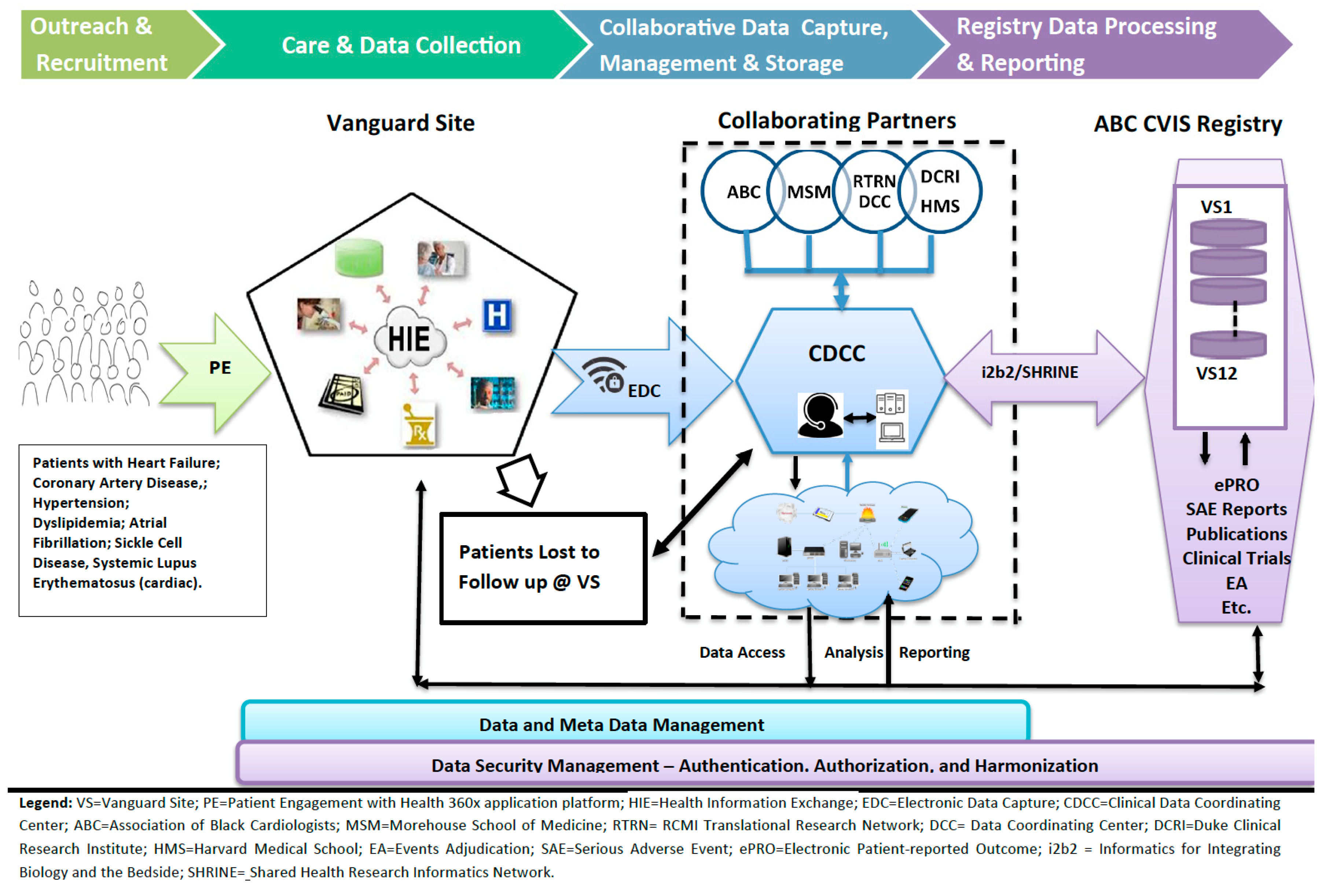
2.7. Study (Registry) Design
Informed Consent and Enrollment
Data Collection Process
Long Term Follow up
End of Study or Withdrawal
Data and Meta Data Management
Roles of Collaborating Institutions and Organizations
Patient Reported Outcomes (PROs) Data Collection
Training Sessions and Procedures
Analysis Plan
Statistical Design
3. Discussion
4. Conclusions
Author Contributions
Funding
Acknowledgments
In Memoriam
Conflicts of Interest
References
- IOM (Institute of Medicine). Public Engagement and Clinical Trials: New Models and Disruptive Technologies: Workshop Summary; The National Academies Press: Washington, DC, USA, 2012. [Google Scholar]
- IOM. Transforming Clinical Research in the United States: Challenges and Opportunities: Workshop summary; The National Academies Press: Washington, DC, USA, 2010. [Google Scholar]
- Dzau, V.J.; Ginsburg, G.S.; Chopra, A.; Goldman, D.; Green, E.D.; Leonard, D.G.B.; McClellan, M.; Plump, A.; Terry, S.F.; Yamamoto, K.R. Realizing the Full Potential of Precision Medicine in Health and Health Care; Vital Directions for Health and Health Care Series; Discussion Paper; National Academy of Medicine: Washington, DC, USA, 2016. [Google Scholar] [CrossRef]
- The White House. FACT SHEET: President Obama’s Precision Medicine Initiative. 2015. Available online: https://www.whitehouse.gov/the-press-office/2015/01/30/fact-sheet-president-obama-s-precision-medicine-initiative Office of Science (accessed on 14 June 2016).
- NIH. About the Precision Medicine Initiative Cohort Program. 2016. Available online: Ttps://www.nih.gov/precision-medicine-initiative-cohort-program (accessed on 14 June 2016).
- Toward Precision Medicine: Building a Knowledge Network for Biomedical Research and a New Taxonomy of Disease, National Academies Press. Committee on A Framework for Developing a New Taxonomy of Disease Board on Life Sciences Division on Earth and Life Studies; National Research Council of the National Academies: Washington, DC, USA, 2011. [Google Scholar]
- Baker, D.; Might, M.; O’Rourke, P.; Rodriguez, L.L.; Simoncelli, T.; Wilbanks, J. Participant Engagement, Data Privacy, and Novel Ways of Returning Information to Participants; Precision Medicine Initiative Research Cohort: Newtown, PA, USA, 2015. [Google Scholar]
- Rollins, L.; Sy, A.; Crowell, N.; Rivers, D.; Miller, A.; Cooper, P.; Teague, D.; Jackson, C.; Henry Akintobi, T.; Ofili, E. Learning and Action in Community Health: Using the Health Belief Model to Assess and Educate African American Community Residents about Participation in Clinical Research. Int. J. Environ. Res. Public Health 2018, 15, 1862. [Google Scholar] [CrossRef] [PubMed]
- National Center for Advancing Translational Science. Strategic Plan; National Center for Advancing Translational Science: Bethesda, MD, USA, 2016.
- DeVol, R.C.; Bedroussian, A.; Yeo, B. The Global Biomedical Industry: Preserving U.S. Leadership; The Milken Institute: Santa Monica, CA, USA, 2011; Available online: http://www.milkeninstitute.org/publications/ (accessed on 16 March 2019).
- Tufts Center for the Study of Drug Development. Briefing: Cost of Developing a New Drug; Tufts Center for the Study of Drug Development & Tufts School of Medicine: Boston, MA, USA, 2014. [Google Scholar]
- Getz, K.A.; Campo, R.A.; Kaitin, K.I. Variability in Protocol Design Complexity by Phase and Therapeutic Area. Drug Inf. J. 2011, 45, 413–420. [Google Scholar] [CrossRef]
- Califf, R.M.; Harrington, R.A. American industry and the U.S cardiovascular clinical research enterprise: An appropriate analogy? J. Am. Coll. Cardiol. 2011, 58, 677–680. [Google Scholar] [CrossRef] [PubMed]
- Kim, E.S.; Carrigan, T.P.; Menon, V. International participation in cardiovascular randomized controlled trials sponsored by the NHLBI. J. Am. Coll. Cardiol. 2011, 58, 671–676. [Google Scholar] [CrossRef] [PubMed]
- IOM (Institute of Medicine). Roundtable on the Promotion of Health Equity and the Elimination of Health Disparities: Strategies for Ensuring Diversity, Inclusion, and Meaningful Participation in Clinical Trials; Institute of Medicine: Washington, DC, USA, 2012. [Google Scholar]
- FDAct. The Food and Drug Administration Safety and Innovation Act (FDASIA); Siskiyou: Siskiyou, CA, USA, 2012.
- FDA Guidance Collection of Race and Ethnicity Data in Clinical Trials. Available online: http://www.fda.gov/ForIndustry/FDABasicsforIndustry/ucm234622.htm (accessed on 16 March 2019).
- Sacubitril in Congestive Heart Failure. Center for Drug Evaluation and Research Application Number: 207620Orig1s000. 2015. Available online: https://www.accessdata.fda.gov/drugsatfda_docs/nda/2015/207620Orig1s000Approv.pdf (accessed on 16 March 2019).
- Scharff, D.P.; Mathews, K.J.; Jackson, P.; Hoffsuemmer, J.; Martin, E.; Edwards, D. More than Tuskegee: Understanding mistrust about research participation. J. Health Care Poor Unders. 2010, 21, 87997. [Google Scholar]
- Shaw, M.G.; Morrell, D.S.; Corbie Smith, G.M.; Lowell, A.; Goldsmith, L.A. Perceptions of pediatric clinical research among African American and Caucasian parents. J. Natl. Med. Assoc. 2009, 101, 900907. [Google Scholar] [CrossRef]
- Braunstein, J.B.; Sherber, N.S.; Schulman, S.P.; Ding, E.L.; Powe, N.R. Race, medical researcher distrust, perceived harm, and willingness to participate in cardiovascular prevention trials. Medicine 2008, 87, 19. [Google Scholar] [CrossRef]
- Gadegbeku, C.A.; Stillman, P.K.; Huffman, M.D.; Jackson, J.S.; Kusek, J.W.; Jamerson, K.A. Factors associated with enrollment of African Americans into a clinical trial: Results from the African American study of kidney disease and hypertension. Contemp. Clin. Trials 2008, 29, 83742. [Google Scholar] [CrossRef]
- Paskett, E.D.; Reeves, K.W.; McLaughlin, J.M.; Katz, M.L.; McAlearney, A.S.; Ruffin, M.T.; Halbert, C.H.; Merete, C.; Davis, F.; Gehlert, S. Recruitment of minority and underserved populations in the United States: The Centers for Population Health and Health Disparities experience. Contemp. Clin. Trials 2008, 29, 84761. [Google Scholar] [CrossRef]
- Durant, R.W.; Davis, R.B.; St George, D.M.; Williams, I.C.; Blumenthal, C.; Corbie Smith, G.M. Participation in research studies: Factors associated with failing to meet minority recruitment goals. Ann. Epidemiol. 2007, 17, 63442. [Google Scholar] [CrossRef]
- Powell, J.H.; Fleming, Y.; WalkerMcGill, C.L.; Lenoir, M. The project IMPACT experience to date: Increasing minority participation and awareness of clinical trials. J. Natl. Med. Assoc. 2008, 100, 17887. [Google Scholar] [CrossRef]
- Corbie Smith, G.; Williams, I.C.; Blumenthal, C.; Dorrance, J.; Estroff, S.E.; Henderson, G. Relationships and communication in minority participation in research: Multidimensional and multidirectional. J. Natl. Med. Assoc. 2007, 99, 48998. [Google Scholar]
- Garber, M.; Hanusa, B.H.; Switzer, G.E.; Mellors, J.; Arnold, R.M. HIVinfected African Americans are willing to participate in HIV treatment trials. J. Gen. Intern. Med. 2007, 22, 1742. [Google Scholar] [CrossRef]
- Howerton, M.W.; Gibbons, M.C.; Baffi, C.R.; Gary, T.L.; Lai, G.Y.; Bolen, S.; Tilburt, J.; Tanpitukpongse, T.P.; Wilson, R.F.; Powe, N.R.; et al. Provider roles in the recruitment of underrepresented populations to cancer clinical trials. Cancer 2007, 109, 46576. [Google Scholar] [CrossRef]
- Lawsin, C.R.; Borrayo, E.A.; Edwards, R.; Belloso, C. Community readiness to promote Latinas’ participation in breast cancer prevention clinical trials. Health Soc. Care Commun. 2007, 15, 36978. [Google Scholar] [CrossRef]
- Movsas, B.; Moughan, J.; Owen, J.; Coia, L.R.; Zelefsky, M.J.; Hanks, G.; Wilson, J.F. Who enrolls onto clinical oncology trials? A radiation Patterns of Care Study analysis. Int. J. Radiat Oncol. Biol. Phys. 2007, 68, 114550. [Google Scholar] [CrossRef]
- Cultural Competence in Research Annotated Bibliography Program for Cultural Competence in Research Harvard Catalyst Program for Faculty Development & Diversity. Created: September 2009 Updated: October 2010. Available online: catalyst.harvard.edu/pdf/diversity/CCR-annotated (accessed on 16 March 2019).
- Betancourt, R.J.; Green, A.R.; Ananeth-Firempong, O., II. Defining cultural competence: A practical framework for addressing racial/ethnic disparities in health and health care. Public Health Rep. 2003, 118, 293–302. [Google Scholar] [CrossRef]
- O’Brien, R.L.; KosokoLasaki, O.; Cook, C.T.; Kissell, J.; Peak, F.; Williams, E.H. Self-assessment of cultural attitudes and competence of clinical investigators to enhance recruitment and participation of minority populations in research. J. Natl. Med. Assoc. 2006, 98, 674–682. [Google Scholar]
- Otado, J.; Kwagyan, J.; Edwards, D.; Ukaegbu, A.; Rockcliffe, F.; Nana Osafo, N. Culturally Competent Strategies for Recruitment and Retention of African-American Populations into Clinical Trials. Clin. Transl. Sci. 2015, 8, 460–466. [Google Scholar] [CrossRef]
- Association of Black Cardiologists. Morehouse School of Medicine, American Heart Association. New Cardiovascular Disease Registry to Support Care for Underserved; Release Press: Dallas, TX, USA, 2016. [Google Scholar]
- Stephens, D.S.; West, A.C.; Ofili, E.O.; Boyan, B.D.; Blumberg, H.M. The Atlanta Clinical and Translational Science Institute: Clinical and translational science education and training partnership. Clin. Transl. Sci. 2011, 4, 143–145. [Google Scholar] [CrossRef]
- Ofili, E.O.; Fair, A.; Norris, K.; Verbalis, J.G.; Poland, R.; Bernard, B.; Stephens, D.S.; Dubinett, S.M.; Imperato-McGinley, J.; Dottin, R.P.; et al. Models of Interinstitutional Partnerships between Research Intensive Universities and Minority Serving Institutions (MSI) across the Clinical Translational Science Award (CTSA) Consortium. Clin. Transl. Sci. 2013, 6, 435–443. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Murphy, F.; Jackson, P.; Johnson, P.; Ofili, E.O.; Cashmire, N.; Quarshie, A. Informing and Consenting Disadvantaged Populations for Clinical and Community Research. Am. J. Health Stud. 2005, 19, 246–253. [Google Scholar]
- Ofili, E.O.; Igho-Pemu, P.; Lapu-Bula, R.; Quarshie, A.; Obialo, C.; Thomas, C.; Onwuanyi, A.; Oduwole, A.; Ojutalayo, F.; Johnson, P.; et al. The Community Physicians’ Network (CPN©): An Academic-Community Partnership to Eliminate Healthcare Disparities. Ethn. Dis. 2005, 15, 124–127. [Google Scholar]
- Egan, B.; Lackland, D.; Igho-Pemu, P.; Hendrix, K.; Basile, J.; Rehman, S.; Okonofua, E.; Quarshie, A.; Oduwole, A.; Onwuanyi, A.; et al. Cardiovascular Risk Factor Control in Communities—The ASH Carolinas-Georgia Chapter, the Hypertension Initiative, and the Community Physicians’ Network. J. Clin. Hypertens. 2006, 8, 879–886. [Google Scholar] [CrossRef]
- Ofili, E.O.; Tchounwou, P.B.; Fernandez-Repollet, E.; Yanagihara, R.M.D.; Akintobi, T.H.; Lee, J.E.; Malouhi, M.; Garner, S.T.; Hayes, T.T.; Baker, A.R.; et al. The research centers in minority institutions (RCMI) Translational Research Network: Building and Sustaining Capacity for Multi-site Basic Biomedical, Clinical and Behavioral Research (Networks and Partnerships to Advance Health Equity). Ethn. Dis. 2019, 29, 135–144. [Google Scholar] [CrossRef] [PubMed]
- Fleming, E.S.; Perkins, J.; Easa, D.; Conde, J.G.; Baker, R.S.; Southerland, W.M.; Dottin, R.; Benabe, J.E.; Ofili, E.O.; Bond, V.C.; et al. Addressing health disparities through multi-institutional multidisciplinary collaboratories. Ethn. Dis. 2008, 18, S2-161-7. [Google Scholar] [PubMed]
- Fleming, E.S.; Perkins, J.; Easa, D.; Conde, J.G.; Baker, R.S.; Southerland, W.M.; Dottin, R.; Benabe, J.E.; Ofili, E.O.; Bond, V.C.; et al. The role of translational research in addressing health disparities: A conceptual framework. Ethn. Dis. 2008, 18, S2-155-60. [Google Scholar]
- RCMI Translational Science 2017: Innovate, Translate, Collaborate, Engage—Community 30 October 2017. Available online: http://www.RCMI2017conf.com|#RCMIconf (accessed on 19 December 2018).
- CARRA. Available online: https://carragroup.org (accessed on 16 March 2019).
- Lionetti, G.; Kimura, Y.; Schanberg, L.E.; Beukelman, T.; Wallace, C.A.; Ilowite, N.T.; Winsor, J.; Kathleen, F.; Natter, M.; Sundy, J.S. Using Registries to Identify Adverse Events in Rheumatic Diseases. Pediatrics 2013, 132, e1384–e1394. [Google Scholar] [CrossRef] [Green Version]
- Natter, M.D.; Quan, J.; Ortiz, D.M.; Bousvaros, A.; Ilowite, N.T.; Inman, C.J.; Marsolo, K.; McMurry, A.J.; Sandborg, C.I.; Schanberg, L.E.; et al. An i2b2-based, generalizable, open source, self-scaling chronic disease registry. J. Am. Med. Inf. Assoc. 2013, 20, 172–179. [Google Scholar] [CrossRef] [Green Version]
- Schanberg, L.E.; Ilowite, N.T.; Sandborg, C.I.; Wallace, C.A. CARRA: Accelerating Toward an Evidence Based Culture in Pediatric Rheumatology (1RC2AR058934-01). Available online: https://projectreporter.nih.gov/project_info_description. cfm?aid=7855553 (accessed on 11 April 2017).
- Weber, G.M.; Murphy, S.N.; McMurry, A.J.; MacFadden, D.; Nigrin, D.J.; Churchill, S.; Kohane, I.S. The Shared Health Research Information Network (SHRINE): A prototype federated query tool for clinical data repositories. J. Am. Med. Inf. Assoc. 2009, 16, 624–630. [Google Scholar] [CrossRef]
- Murphy, S.N.; Weber, G.; Mendis, M.; Gainer, V.; Chueh, H.C.; Churchill, S.; Kohane, I. Serving the enterprise and beyond with informatics for integrating biology and the bedside (i2b2). J. Am. Med. Inf. Assoc. 2010, 17, 124–130. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Goryachev, S.; Sordo, M.; Zeng, Q.T. A suite of natural language processing tools developed for the I2B2 project. In Proceedings of the AMIA Annual Symposium Proceedings, Washington, DC, USA, 11–15 November 2006. [Google Scholar]
- Murphy, S.N.; Gainer, V.; Mendis, M.; Churchill, S.; Kohane, I. Strategies for maintaining patient privacy in i2b2. J. Am. Med. Inf. Assoc. 2011, 18 (Suppl. 1), i103–i108. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Murphy, S.N.; Avillach, P.; Bellazzi, R.; Phillips, L.; Gabetta, M.; Eran, A.; McDuffie, M.T.; Kohane, I.S. Combining clinical and genomics queries using i2b2—Three methods. PLoS ONE 2017, 12, e0172187. [Google Scholar] [CrossRef] [PubMed]
- Medidata Rave Electronic Data Capture. Available online: https://www.mdsol.com/en (accessed on 16 March 2019).
- Ofili, E.O.; Pemu, P.E.; Quarshie, A.; Alema Mensah, E.; Rollins, L.; Ojutalayo, F.; McCaslin, A.; Saint Clair, B. Democratizing discovery health with me. Trans. Am. Clin. Climatol. Assoc. 2018, 129, 215–234. [Google Scholar] [PubMed]
- Ofili, E.O.; Pemu, P.I.; Quarshie, A.; Johnson, P.; Linn, L.J.; Kaur, D.; Ali, J. A System and Method for Chronic Illness Care. US Patent 8,234,131B2, 31 July 2012. [Google Scholar]
- Pemu, P.E.; Quarshie, A.Q.; Josiah-Willock, R.; Ojutalayo, F.O.; Alema-Mensah, E.; Ofili, E.O. Socio-demographic psychosocial and clinical characteristics of participants in e-HealthyStrides©: An interactive ehealth program to improve diabetes self-management skills. J. Health Care Poor Unders. 2011, 22 (Suppl. 4), 146–164. [Google Scholar] [CrossRef] [PubMed]
- Morehouse School of Medicine Offers Health Coaching Program for Diabetics. Available online: http://www.myfoxatlanta.com/video?clipId=8674166&autostart=true47 (accessed on 24 June 2015).
- Atlanta Journal Atlanta Journal-Constitution. 13 March 2013. Available online: http://www.ajc.com/news/news/atlanta-workers-team-up-with-morehouse-medical-to-/nWq3Y/ (accessed on 16 March 2019).
- Mandl, K.D.; Mandel, J.C.; Murphy, S.N.; Elmer Victor Bernstam, E.V.; Ramoni, R.L.; Kreda, D.A.; McCoy, J.M.; Ben Adida, B.; Kohane, I.S. The SMART Platform: Early experience enabling substitutable applications for electronic health records. J. Am. Med. Inf. Assoc. 2012, 19, 597–603. [Google Scholar] [CrossRef]
- Mandel, J.C.; Kreda, D.A.; Mandl, K.D.; Kohane, I.S.; Ramoni, R.B. SMART on FHIR: A standards-based, interoperable apps platform for electronic health records. J. Am. Med. Inf. Assoc. 2016, 1–10. [Google Scholar] [CrossRef] [PubMed]
- FDA Grant U24FD006543, Expanding HL7 FHIR to Support Post-Marketing Research and Surveillance within Multi-Source, Chronic Disease Registries. Natter, Marc D (PI). Available online: https://projectreporter.nih.gov/project_info_description.cfm?aid=9720434&icde=43219705 (accessed on 16 March 2019).
- Teresi, J.A.; Jones, R.N. Methodological issues in examining measurement equivalence in patient reported outcomes measures: Methods overview to the two-part series, Measurement equivalence of the Patient Reported Outcomes Measurement Information System® (PROMIS®) short forms. Psychol. Test Assess. Model. 2016, 58, 37–78. [Google Scholar]
- Wee, C.C.; Davis, R.B.; Hamel, M.B. Comparing the SF-12 and SF-36 health status questionnaires in patients with and without obesity. Health Qual. Life Outcomes 2008, 6, 11. [Google Scholar] [CrossRef]
- Tzelepis, F.; Rose, S.K.; Sanson-Fisher, R.W.; Clinton-McHarg, T.; Carey, M.L.; Paul, C.L. Are we missing the Institute of Medicine’s mark? A systematic review of patient-reported outcome measures assessing quality of patient-centered cancer care. BMC Cancer 2014, 14, 41. [Google Scholar] [CrossRef]
- Health Level 7. Open Source FHIR Implementations. 2015. Available online: http://wiki.hl7. org/index.php?title.Open_Source_FHIR_implementations (accessed on 22 June 2015).
- Guidelines for Good Pharmacoepidemiology Practices (GPP). Initially Issued: 1996; Revision 1: August 2004; Revision 2: April 2007 Revision 3: June 2015. Available online: https://www.pharmacoepi.org/resources/policies/guidelines-08027/ (accessed on 19 December 2018).
- FDA Office of Minority Health Hosts. Ensuring Diversity, Inclusion and Meaningful Participation in Clinical Trials: The Model of the ABC Cardiovascular Study (A CME Program); FDA Office of Minority Health Hosts: Atlanta, GA, USA, 2017.


© 2019 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Ofili, E.O.; Schanberg, L.E.; Hutchinson, B.; Sogade, F.; Fergus, I.; Duncan, P.; Hargrove, J.; Artis, A.; Onyekwere, O.; Batchelor, W.; et al. The Association of Black Cardiologists (ABC) Cardiovascular Implementation Study (CVIS): A Research Registry Integrating Social Determinants to Support Care for Underserved Patients. Int. J. Environ. Res. Public Health 2019, 16, 1631. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph16091631
Ofili EO, Schanberg LE, Hutchinson B, Sogade F, Fergus I, Duncan P, Hargrove J, Artis A, Onyekwere O, Batchelor W, et al. The Association of Black Cardiologists (ABC) Cardiovascular Implementation Study (CVIS): A Research Registry Integrating Social Determinants to Support Care for Underserved Patients. International Journal of Environmental Research and Public Health. 2019; 16(9):1631. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph16091631
Chicago/Turabian StyleOfili, Elizabeth O., Laura E. Schanberg, Barbara Hutchinson, Felix Sogade, Icilma Fergus, Phillip Duncan, Joe Hargrove, Andre Artis, Osita Onyekwere, Wayne Batchelor, and et al. 2019. "The Association of Black Cardiologists (ABC) Cardiovascular Implementation Study (CVIS): A Research Registry Integrating Social Determinants to Support Care for Underserved Patients" International Journal of Environmental Research and Public Health 16, no. 9: 1631. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph16091631