Community-Based Participatory Research and Drug Utilization Research to Improve Childhood Diarrhea Case Management in Ujjain, India: A Cross-Sectional Survey


Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Design and Setting
2.2. Sample Size Calculation
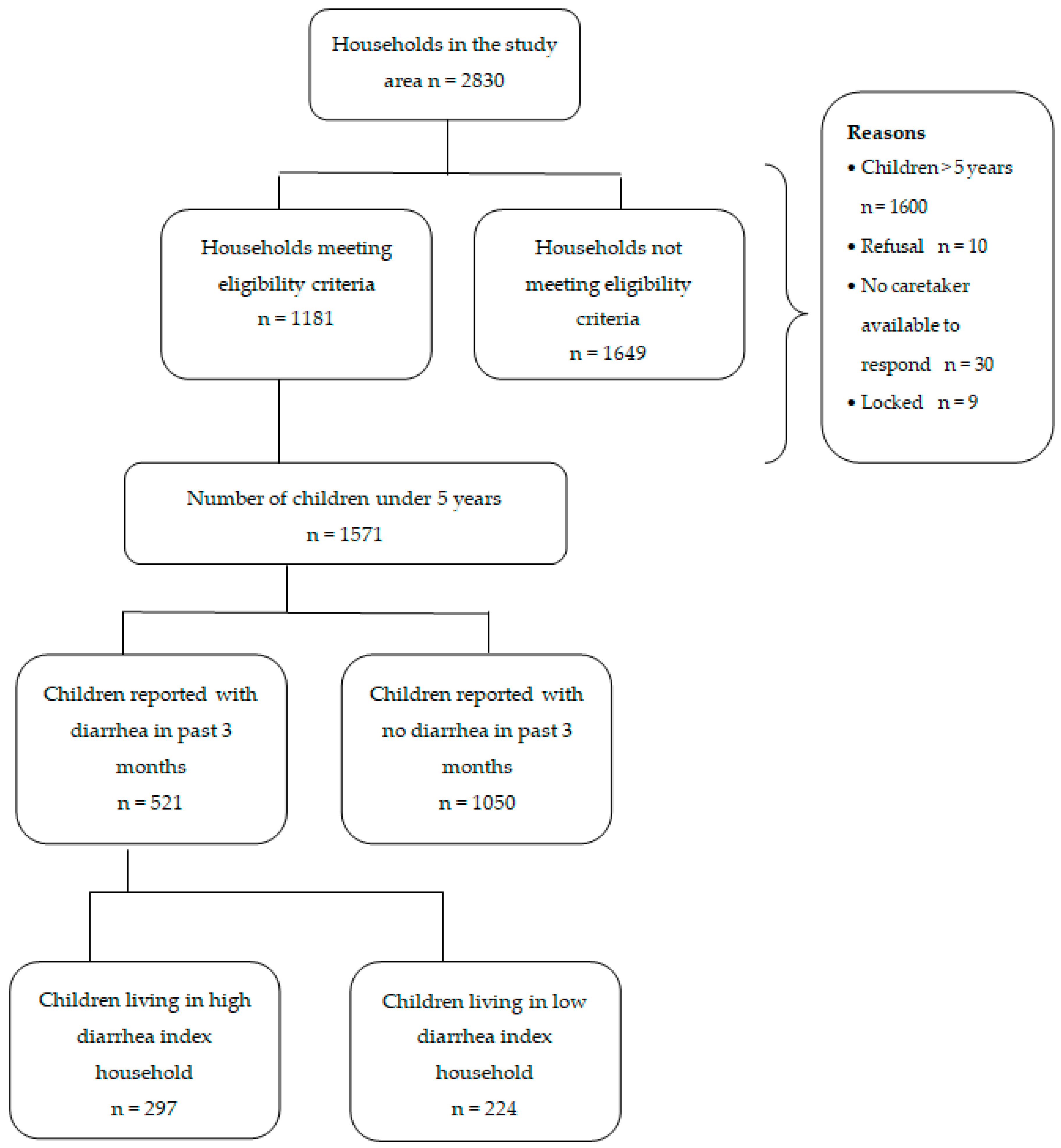
2.3. Sampling Frame and Data Collection Tools and Methods
- 1.
- an = number of episodes of diarrhea in the past three months in the first child living in the same household.
- 2.
- bn = number of episodes of diarrhea in past three months in the second child living in the same household as a.
- 3.
- cn = number of episodes of diarrhea in the past three months in the third child living in the same household as a and b.
- 4.
- dn = Number of episodes of diarrhea in the past three months in the fourth child living in the same household as a, b, and c
- 5.
- y = Number of children aged less than five years living in the same household
2.4. Data Management and Data Analysis
2.5. Ethical Consideration
2.6. Availability of Data and Materials
3. Results
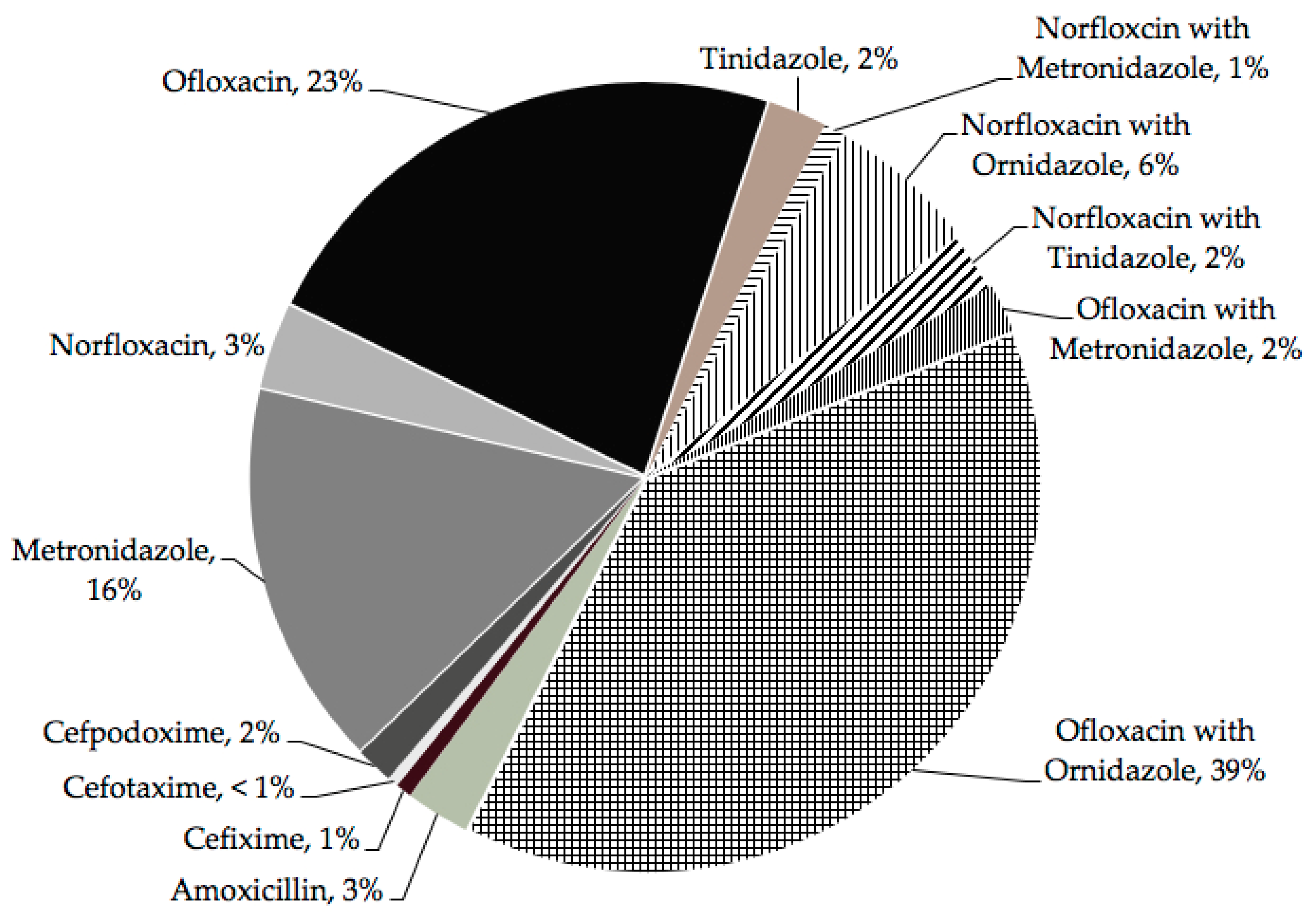
Treatment Given to Children for the Last Episode of Diarrhea
4. Discussion
Methodological Considerations
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- UNICEF; WHO. End Preventable Deaths: Global Action Plan for Prevention and Control of Pneumonia and Diarrhoea; World Health Organization: Lyon, France, 2013; Available online: http://apps.who.int/iris/bitstream/handle/10665/79200/9789241505239_eng.pdf;jsessionid=837AEC1288C76D2368F1E8F8DAB86B55?sequence=1 (accessed on 29 December 2018).
- Global Burden of Disease Collaborators. Estimates of the global, regional, and national morbidity, mortality, and aetiologies of diarrhoea in 195 countries: A systematic analysis for the global burden of disease study 2016. Lancet Infect. Dis. 2018, 18, 1211–1228. [Google Scholar] [CrossRef]
- Ganguly, E.; Sharma, P.K.; Bunker, C.H. Prevalence and risk factors of diarrhea morbidity among under-five children in India: A systematic review and meta-analysis. Indian J. Child Health 2015, 2, 152–160. [Google Scholar]
- Ram, U.; Jha, P.; Ram, F.; Kumar, S.; Awasthi, S.; Shet, A.; Padera, J.; Nansukusa, S.; Kumar, R. Neonatal, 1–59 month, and under-5 mortality in 597 Indian districts, 2001 to 2012: Estimates from national demographic and mortality surveys. Lancet Glob. Health 2013, 1, e219–e226. [Google Scholar] [CrossRef]
- Walker, C.L.; Rudan, I.; Liu, L.; Nair, H.; Theodoratou, E.; Bhutta, Z.A.; O’Brien, K.L.; Campbell, H.; Black, R.E. Global burden of childhood pneumonia and diarrhoea. Lancet 2013, 381, 1405–1416. [Google Scholar] [CrossRef]
- Pathak, D.; Pathak, A.; Marrone, G.; Diwan, V.; Lundborg, C.S. Adherence to treatment guidelines for acute diarrhoea in children up to 12 years in Ujjain, India—A cross-sectional prescription analysis. BMC Infect. Dis. 2011, 11, 32. [Google Scholar] [CrossRef]
- Lakshminarayanan, S.; Jayalakshmy, R. Diarrheal diseases among children in India: Current scenario and future perspectives. J. Nat. Sci. Biol. Med. 2015, 6, 24–28. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Bhutta, Z.A.; Das, J.K.; Walker, N.; Rizvi, A.; Campbell, H.; Rudan, I.; Black, R.E.; Lancet, D.; Pneumonia Interventions Study Group. Interventions to address deaths from childhood pneumonia and diarrhoea equitably: What works and at what cost? Lancet 2013, 381, 1417–1429. [Google Scholar] [CrossRef]
- Kadam, D.M.; Hadaye, R.; Pandit, D. Knowledge and practices regarding oral rehydration therapy among mothers in rural area of Vasind, India. Nepal. Med. Coll. J. 2013, 15, 110–112. [Google Scholar] [PubMed]
- Bhatia, V.; Swami, H.M.; Bhatia, M.; Bhatia, S.P. Attitude and practices regarding diarrhoea in rural community in Chandigarh. Indian J. Pediatr. 1999, 66, 499–503. [Google Scholar] [CrossRef] [PubMed]
- Datta, V.; John, R.; Singh, V.P.; Chaturvedi, P. Maternal knowledge, attitude and practices towards diarrhea and oral rehydration therapy in rural Maharashtra. Indian J. Pediatr. 2001, 68, 1035–1037. [Google Scholar] [CrossRef]
- Ujjain district. Office of the Registrar General and Census Commissioner, Ministry of Home Affairs, Government of India, New Delhi, 2011. Available online: http://www.censusindia.gov.in/2011census/dchb/DCHB_A/23/2318_PART_A_DCHB_UJJAIN.pdf (accessed on 29 December 2018).
- National Family Health Survey-4 (NFHS 4). District Fact Sheet, Ujjain, Madhya Pradesh, Ministry of Health and Family Welfare; Ministry of Health and Family Welfare, Government of India: New Delhi, India, 2016; pp. 105–116. Available online: http://rchiips.org/NFHS/FCTS/MP/MP_FactSheet_435_Ujjain.pdf (accessed on 29 December 2018).
- Rowe, A.K.; Lama, M.; Onikpo, F.; Deming, M.S. Design effects and intraclass correlation coefficients from a health facility cluster survey in Benin. Int. J. Qual. Health Care 2002, 14, 521–523. [Google Scholar] [CrossRef] [Green Version]
- Rattray, J.; Jones, M.C. Essential elements of questionnaire design and development. J. Clin. Nurs. 2007, 16, 234–243. [Google Scholar] [CrossRef] [Green Version]
- El Bushra, H.A.; Tigerman, N.S.; El Tom, A.R. Perceived causes and traditional treatment of diarrhoea by mothers in eastern Sudan. Ann. Trop. Paediatr. 1988, 8, 135–140. [Google Scholar] [CrossRef]
- Bella, H.; Ai-Freihi, H.; El-Mousan, M.; Danso, K.T.; Sohaibani, M.; Khazindar, M.S. Knowledge, attitudes and practices related to diarrhoea in eastern province, Saudi Arabia. J. Fam. Community Med. 1994, 1, 40–44. [Google Scholar]
- Stapleton, M.C. Diarrhoeal diseases: Perceptions and practices in Nepal. Soc. Sci. Med. 1989, 28, 593–604. [Google Scholar] [CrossRef]
- Gladstone, B.P.; Das, A.R.; Rehman, A.M.; Jaffar, S.; Estes, M.K.; Muliyil, J.; Kang, G.; Bose, A. Burden of illness in the first 3 years of life in an indian slum. J. Trop. Pediatr. 2010, 56, 221–226. [Google Scholar] [CrossRef]
- Sarkar, R.; Kang, G.; Naumova, E.N. Rotavirus seasonality and age effects in a birth cohort study of southern India. PLoS ONE 2013, 8, e71616. [Google Scholar] [CrossRef]
- WHO/UNICEF Core Questions on Drinking Water and Sanitation for Household Surveys. World Health Organization and United Nations Children’s Fund: Geneva, Switzerland; New York, NY, USA, 2004; Available online: https://www.who.int/mediacentre/news/releases/2017/launch-version-report-jmp-water-sanitation-hygiene.pdf (accessed on 29 December 2018).
- Huq, A.; Yunus, M.; Sohel, S.S.; Bhuiya, A.; Emch, M.; Luby, S.P.; Russek-Cohen, E.; Nair, G.B.; Sack, R.B.; Colwell, R.R. Simple sari cloth filtration of water is sustainable and continues to protect villagers from cholera in Matlab, Bangladesh. MBio 2010, 1, e00034-10. [Google Scholar] [CrossRef]
- Bain, R.; Cronk, R.; Hossain, R.; Bonjour, S.; Onda, K.; Wright, J.; Yang, H.; Slaymaker, T.; Hunter, P.; Pruss-Ustun, A.; et al. Global assessment of exposure to faecal contamination through drinking water based on a systematic review. Trop. Med. Int. Health 2014, 19, 917–927. [Google Scholar] [CrossRef] [Green Version]
- Kundu, A.; Smith, W.A.; Harvey, D.; Wuertz, S. Drinking water safety: Role of hand hygiene, sanitation facility, and water system in semi-urban areas of India. Am. J. Trop. Med. Hyg. 2018, 99, 889–898. [Google Scholar] [CrossRef]
- Sinha, A.; Nagel, C.L.; Schmidt, W.P.; Torondel, B.; Boisson, S.; Routray, P.; Clasen, T.F. Assessing patterns and determinants of latrine use in rural settings: A longitudinal study in Odisha, India. Int. J. Hyg. Environ. Health 2017, 220, 906–915. [Google Scholar] [CrossRef] [PubMed]
- Biran, A.; Jenkins, M.W.; Dabrase, P.; Bhagwat, I. Patterns and determinants of communal latrine usage in urban poverty pockets in Bhopal, India. Trop. Med. Int. Health 2011, 16, 854–862. [Google Scholar] [CrossRef] [Green Version]
- Akter, T.; Ali, A.R.; Dey, N.C. Transition overtime in household latrine use in rural Bangladesh: A longitudinal cohort study. BMC Public Health 2014, 14, 721. [Google Scholar] [CrossRef]
- Thys, S.; Mwape, K.E.; Lefevre, P.; Dorny, P.; Marcotty, T.; Phiri, A.M.; Phiri, I.K.; Gabriel, S. Why latrines are not used: Communities’ perceptions and practices regarding latrines in a Taenia solium endemic rural area in eastern Zambia. PLoS Negl. Trop. Dis. 2015, 9, e0003570. [Google Scholar] [CrossRef]
- Awoke, W.; Muche, S. A cross sectional study: Latrine coverage and associated factors among rural communities in the district of Bahir Dar Zuria, Ethiopia. BMC Public Health 2013, 13, 99. [Google Scholar] [CrossRef]
- Zwisler, G.; Simpson, E.; Moodley, M. Treatment of diarrhea in young children: Results from surveys on the perception and use of oral rehydration solutions, antibiotics, and other therapies in India and Kenya. J. Glob. Health 2013, 3, 010403. [Google Scholar] [CrossRef]
- Shah, M.S.; Ahmad, A.; Khalique, N.; Afzal, S.; Ansari, M.A.; Khan, Z. Home-based management of acute diarrhoeal disease in an urban slum of Aligarh, India. J. Infect. Dev. Ctries. 2012, 6, 137–142. [Google Scholar] [CrossRef]
- Joseph, N.; Suvarna, P.; Hariharan Bharadwaj, S.; Dhanush, K.S.; Raeesa, F.; Mohamed Jasir, K.K.; Joseph, N.; Kotian, S.M.; Rai, S. Prevalence, risk factors and treatment practices in diarrhoeal diseases in south India. Environ. Health Prev. Med. 2016, 21, 248–257. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Rabbani, G.H.; Larson, C.P.; Islam, R.; Saha, U.R.; Kabir, A. Green banana-supplemented diet in the home management of acute and prolonged diarrhoea in children: A community-based trial in rural Bangladesh. Trop. Med. Int. Health 2010, 15, 1132–1139. [Google Scholar] [CrossRef]




{kind=link}
{kind=link}
{kind=link}
| Socio-demographic characteristics. | Mean | SD |
|---|---|---|
| Continuous variables | ||
| Age of the children (years) | 2.08 | 1.18 |
| Family size (number) | 7.20 | 3.24 |
| Age of mother (years) | 25.11 | 4.67 |
| Categorical variables | n = 1181 households | % |
| Location | ||
| Rural | 660 | 56 |
| Urban | 521 | 44 |
| Education status of mother | ||
| Uneducated | 240 | 20 |
| Primary | 629 | 53 |
| Secondary or more | 312 | 27 |
| Caste | ||
| General | 151 | 13 |
| Scheduled castes * | 166 | 14 |
| Scheduled tribes * | 815 | 69 |
| Other backward class * | 49 | 4 |
| Religion | ||
| Hindu | 695 | 59 |
| Muslim | 460 | 39 |
| Others | 26 | 2 |
| Type of home | ||
| Self-owned | 1091 | 92 |
| Rented | 90 | 8 |
| Number of household members | ||
| ≤4 | 254 | 21 |
| 5–8 | 586 | 50 |
| ≥9 | 341 | 29 |
| Water Sanitation and Hygiene Related Characteristics | n = 1181 | % |
|---|---|---|
| Water treatment | ||
| Drinking water source * | ||
| Hand-pump | 709 | 60 |
| Bore well | 683 | 58 |
| Tap (municipal supply) | 294 | 25 |
| Storage practices * | ||
| Roof-top storage | 242 | 20 |
| Ground storage | 1181 | 100 |
| Drinking water storage containers * | ||
| Earthenware pot (Matka/Ghada) | 1181 | 100 |
| Buckets | 557 | 47 |
| Plastic cans | 298 | 25 |
| Frequency of cleaning ground water containers | ||
| Daily | 779 | 66 |
| Every 2nd–3rd day | 250 | 21 |
| Weekly or more | 154 | 13 |
| Do you treat water before drinking? | ||
| No | 283 | 24 |
| Yes | 898 | 76 |
| Filtration using cloth | 839 | 71 |
| Coagulation, flocculation, and sedimentation (by alum) | 43 | 4.4 |
| Boiling for 20 min | 16 | 1.6 |
| Sanitation | ||
| Toilet constructed in household | ||
| Yes | 1100 | 93 |
| Toilet used by adults | 1080 | 91 |
| Toilet used by children | 276 | 23 |
| Household waste | ||
| Thrown on streets | 1050 | 89 |
| Burnt | 83 | 7 |
| Collected and disposed (municipal facility) | 48 | 4 |
| Hand washing done by mothers/caregivers | ||
| After cleaning child’s feces | 1155 | 98 |
| After toilet | 1153 | 98 |
| After cooking | 960 | 81 |
| After cleaning child’s urine | 675 | 77 |
| Before feeding child | 603 | 51 |
| To clean visible dirt | 558 | 47 |
| Before cooking | 352 | 30 |
| After cleaning nose/mouth | 319 | 27 |
| Categorical Variables | n = 521 | % |
|---|---|---|
| Feeding Practices * | ||
| Continued breastfeeding | 249 | 48 |
| Top milk | 270 | 52 |
| Tea | 230 | 44 |
| Homemade diet | 314 | 60 |
| Mashed food/fruit | 224 | 43 |
| Heard about ORS | 173 | 33 |
| Where to get ORS? | ||
| Health care workers | 388 | 74 |
| Pharmacy store | 29 | 6 |
| Don’t know | 104 | 20 |
| Heard about zinc | 62 | 12 |
| Where to get zinc? | ||
| Health care workers | 177 | 34 |
| Pharmacy store | 29 | 6 |
| Don’t know | 315 | 60 |
| Treatment practices | ||
| No treatment | 11 | 2 |
| Self-treatment only | 155 | 30 |
| Self-treatment with ORS | 28 | 18 |
| Self-treatment with left over medicines | 123 | 79 |
| Zinc tablet/ syrup | 6 | 4 |
| Homemade solutions | 34 | 22 |
| Treatment at healthcare facility | 485 | 93 |
| Government setting | 83 | 17 |
| Private setting | 339 | 70 |
| Formal health care provider | 106 | 31 |
| Informal healthcare provider | 233 | 69 |
| Medical store | 63 | 13 |
| Both self and healthcare facility | 130 | 25 |
| Received any treatment | 510 | 98 |
| Received an antibiotic | 423 | 83 |
| Received ORS | 150 | 29 |
| Received zinc tablets/syrups | 54 | 11 |
© 2019 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Mathur, A.; Baghel, D.; Jaat, J.; Diwan, V.; Pathak, A. Community-Based Participatory Research and Drug Utilization Research to Improve Childhood Diarrhea Case Management in Ujjain, India: A Cross-Sectional Survey. Int. J. Environ. Res. Public Health 2019, 16, 1646. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph16091646
Mathur A, Baghel D, Jaat J, Diwan V, Pathak A. Community-Based Participatory Research and Drug Utilization Research to Improve Childhood Diarrhea Case Management in Ujjain, India: A Cross-Sectional Survey. International Journal of Environmental Research and Public Health. 2019; 16(9):1646. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph16091646
Chicago/Turabian StyleMathur, Aditya, Devendra Baghel, Jitendra Jaat, Vishal Diwan, and Ashish Pathak. 2019. "Community-Based Participatory Research and Drug Utilization Research to Improve Childhood Diarrhea Case Management in Ujjain, India: A Cross-Sectional Survey" International Journal of Environmental Research and Public Health 16, no. 9: 1646. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph16091646