Exploring Doctors’ Willingness to Provide Online Counseling Services: The Roles of Motivations and Costs



Abstract
:1. Introduction
- (1)
- How do extrinsic and intrinsic motivations affect the desire to serve patients well?
- (2)
- How does the desire to serve patients well affect the willingness to offer free or paid online counseling services?
- (3)
- How do the number of consultations and the counseling time moderate the relationships between desire and willingness?
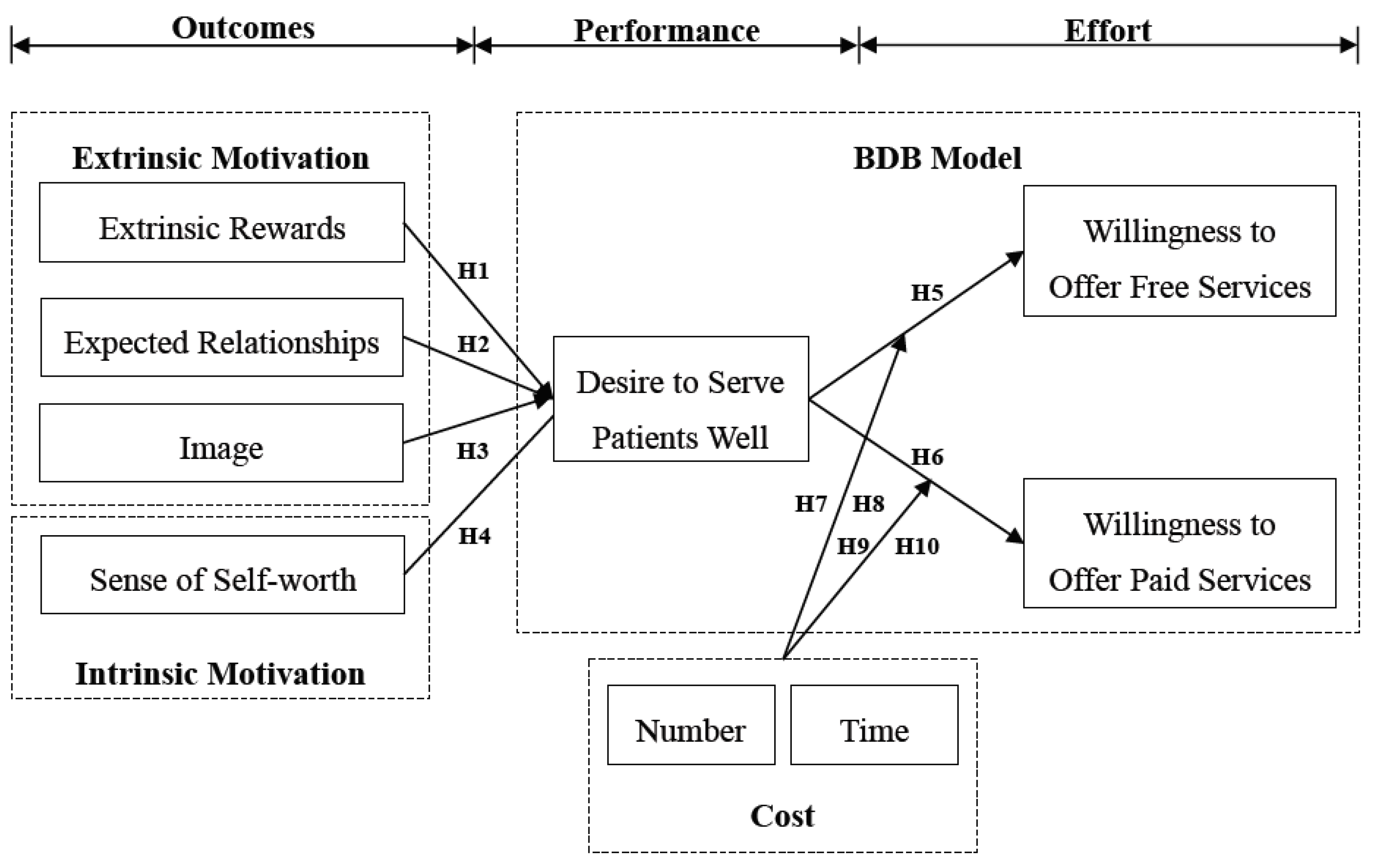
2. Research Hypotheses
2.1. Anticipated Outcomes
2.2. Performance Expectations and Effort Intentions
2.3. Costs
3. Research Methodology
3.1. Theoretical Foundation
3.1.1. Expectancy Theory
3.1.2. BDB Model
3.2. Ethics Statement
3.3. Participants and Procedures
3.4. Measures
4. Results
4.1. Demographic Characteristics
4.2. Measurement Model
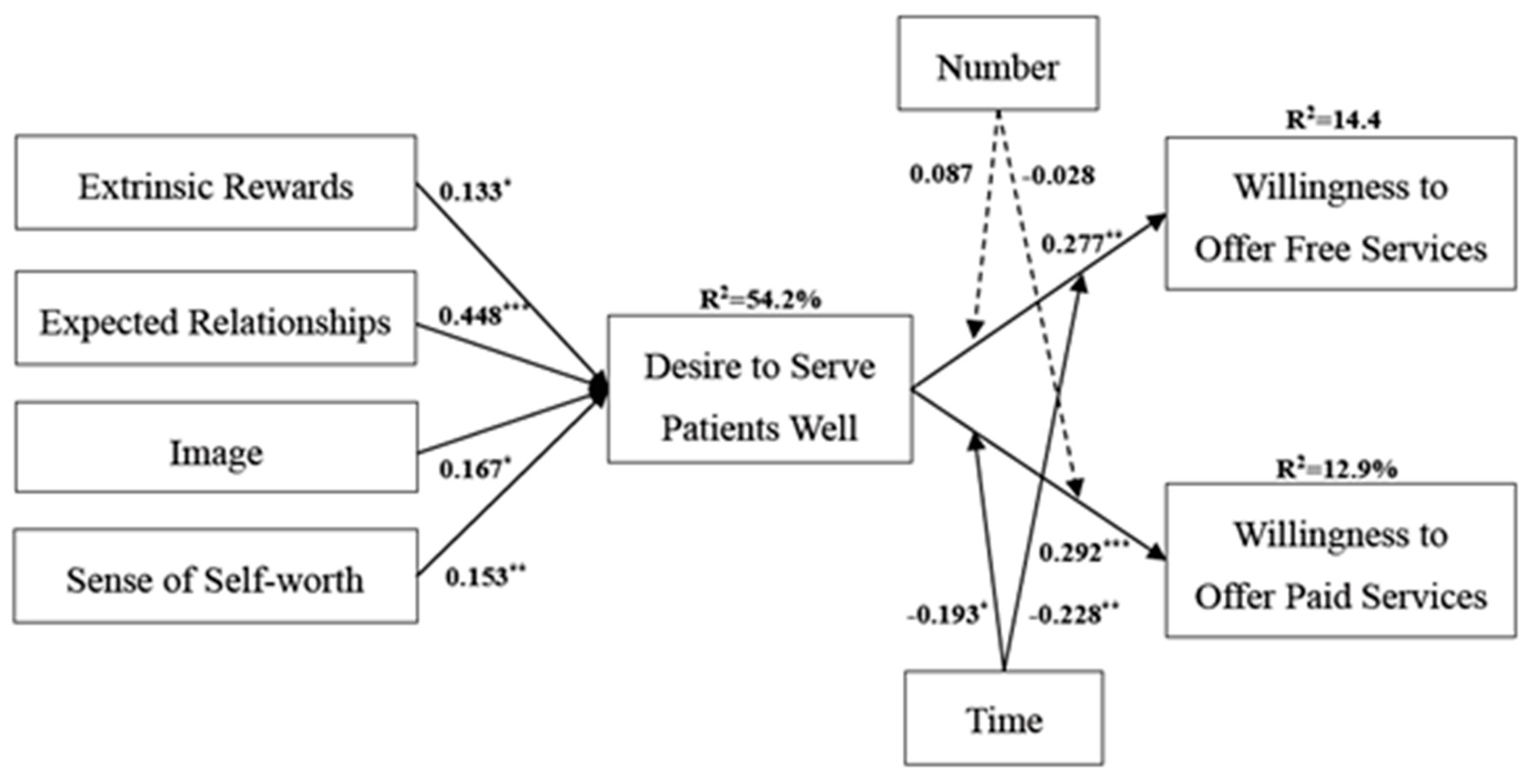
4.3. Structural Model and Discussion
5. Implications
5.1. Theoretical Implications
5.2. Practical Implications
6. Limitations
7. Conclusions
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
Appendix A

{kind=link}
{kind=link}
| Construct | Definition and Measures | Factor Loading | Source |
|---|---|---|---|
| Extrinsic Rewards | The extent to which a doctor expects that he/she can receive extrinsic returns from both online and offline channels when providing online counseling services | - | Bock et al. [12] |
| 1. The income acquired from patients’ visiting my hospital would increase because of my good online counseling services | 0.81 | ||
| 2. The quantity of online consultations would increase because of my good online counseling services | 0.83 | ||
| 3. The quantity of patients’ visiting in my hospital would increase because of my good online counseling services | 0.82 | ||
| Expected Relationships | The extent to which a doctor believes that he/she can foster mutual relationships with both online and offline patients when offering online counseling services | - | Bock et al. [12] |
| 1. Offering good online counseling services would strengthen the tie between me and my patients | 0.88 | ||
| 2. Offering good online counseling services would draw smooth relationships with my patients | 0.89 | ||
| 3. Offering good online counseling services would create strong relationships with my patients | 0.90 | ||
| Image | The extent to which a doctor’s online and offline reputation is increased through offering online counseling services | - | Kankanhalli et al. [17] |
| 1. Offering good online counseling services would improve my image on the online health platforms and in the hospitals | 0.86 | ||
| 2. Offering good online counseling services would improve others’ recognition of me | 0.87 | ||
| 3. Offering good online counseling services, the people I work with respect me | 0.77 | ||
| Sense of Self-worth | The extent of a doctor’s positive perception based on the feeling about his/her contribution to online and offline patients through online counseling services | - | Bock et al. [12] |
| 1. Offering good online counseling services would help my patients solve their health problems | 0.81 | ||
| 2. Offering good online counseling services would improve my service quality | 0.88 | ||
| 3. Offering good online counseling services would improve inquiry processes | 0.80 | ||
| 4. Offering good online counseling services would create chances to solve patients’ health problems. | 0.82 | ||
| Desire to Serve Patients Well | The strength of a doctor’s desire to serve patients well | - | Bagozzi et al. [21] |
| 1. I want to serve my patients well | 0.80 | ||
| 2. My overall wish is to serve my patients well | 0.88 | ||
| 3. I feel an urge or need to serve my patients well | 0.85 | ||
| Willingness to Offer Free Services | The strength of a doctor’s willingness to offer free services | - | Perugini and Bagozzi [37] |
| 1. I am planning to offer free online counseling services | 0.90 | ||
| 2. I will spend effort to offer free online counseling services | 0.94 | ||
| 3. I intend to offer free online counseling services | 0.93 | ||
| Willingness to Offer Paid Services | The strength of a doctor’s willingness to offer paid services | - | Perugini and Bagozzi [37] |
| 1. I am planning to offer paid online counseling services | 0.92 | ||
| 2. I will spend effort to offer paid online counseling services | 0.95 | ||
| 3. I intend to offer paid online counseling services | 0.93 |
Appendix B
| Measure | Item | Frequency | Percentage | Measure | Item | Frequency | Percentage |
|---|---|---|---|---|---|---|---|
| Gender | Male | 182 | 58.5 | Department | Internal medicine | 96 | 30.9 |
| Female | 129 | 41.5 | Stomatology | 59 | 19 | ||
| Age | 18–25 years | 10 | 3.2 | Traditional Chinese medicine | 42 | 13.5 | |
| 26–35 years | 117 | 37.6 | Bone surgery | 31 | 10 | ||
| 36–45 years | 128 | 41.2 | Gynecology and obstetrics | 25 | 8 | ||
| 46–55 years | 47 | 15.1 | Surgery | 21 | 6.7 | ||
| 56–65 years | 8 | 2.6 | Pediatrics | 9 | 2.9 | ||
| >65 years | 1 | 0.3 | Ophthalmology | 5 | 1.6 | ||
| Title | Assistant Doctor | 12 | 3.9 | Oncology | 4 | 1.3 | |
| Resident Doctor | 68 | 21.9 | Others | 19 | 6.1 | ||
| Attending Physician | 116 | 37.3 | Hospital | Hospital of Zhejiang University | 87 | 28.0 | |
| Associate Chief Physician | 77 | 24.8 | Zhejiang Provincial Hospital of Traditional Chinese Medicine | 66 | 21.2 | ||
| Chief Physician | 25 | 8 | Tongde Hospital of Zhejiang Province | 51 | 16.4 | ||
| Others | 13 | 4.2 | Wenzhou People’s Hospital | 38 | 12.2 | ||
| Career age | <1 year | 32 | 10.3 | Quzhou Hospital | 30 | 9.7 | |
| 1–2 years | 42 | 13.5 | Ningbo Hospital | 29 | 9.3 | ||
| 3–4 years | 38 | 12.2 | Hospital of Wenzhou Medical University | 10 | 3.2 | ||
| 5–6 years | 26 | 8.4 | |||||
| 7–8 years | 23 | 7.4 | |||||
| 9–10 years | 26 | 8.4 | |||||
| 11–12 years | 17 | 5.5 | |||||
| >12 years | 107 | 34.4 |
References
- Yan, Z.; Wang, T.; Chen, Y.; Zhang, H. Knowledge sharing in online health communities: A social exchange theory perspective. Inf. Manag. 2016, 53, 643–653. [Google Scholar] [CrossRef]
- Zhang, X.; Liu, S.; Chen, X.; Gong, Y. Social capital, motivations, and knowledge sharing intention in health Q & A communities. Manag. Decis. 2017, 55, 1536–1557. [Google Scholar]
- Sims, J.M. Communities of practice: Telemedicine and online medical communities. Technol. Forecast. Soc. Chang. 2018, 126, 53–63. [Google Scholar] [CrossRef]
- Chang, Y.W.; Hsu, P.Y.; Wang, Y.; Chang, P.Y. Integration of online and offline health services: The role of doctor-patient online interaction. Patient Educ. Couns. 2019, 102, 1905–1910. [Google Scholar] [CrossRef] [PubMed]
- Yang, H.; Zhang, X. Investigating the Effect of Paid and Free Feedback About Physicians’ Telemedicine Services on Patients’ and Physicians’ Behaviors: Panel Data Analysis. J. Med. Internet Res. 2019, 21, e12156. [Google Scholar] [CrossRef] [PubMed]
- Tang, Y.; Yang, Y.T.; Shao, Y.F. Acceptance of Online Medical Websites: An Empirical Study in China. Int. J. Environ. Res. Public Health 2019, 16, 943. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Le, W.; Chang, P.Y.; Chang, Y.W.; Chen, J. Why Do Patients Move from Online Health Platforms to Hospitals? The Perspectives of Fairness Theory and Brand Extension Theory. Int. J. Environ. Res. Public Health 2019, 16, 3755. [Google Scholar] [CrossRef] [Green Version]
- Deng, Z.; Liu, S. Understanding consumer health information-seeking behavior from the perspective of the risk perception attitude framework and social support in mobile social media websites. Int. J. Med. Inform. 2017, 105, 98–109. [Google Scholar] [CrossRef]
- Guo, S.; Guo, X.; Fang, Y.; Vogel, D. How doctors gain social and economic returns in online health-care communities: A professional capital perspective. J. Manag. Inf. Syst. 2017, 34, 487–519. [Google Scholar] [CrossRef]
- Oh, H.; Rizo, C.; Enkin, M.; Jadad, A. What is eHealth (3): A systematic review of published definitions. J. Med. Internet Res. 2005, 7, e1. [Google Scholar] [CrossRef]
- Liu, J.; Bian, Y.; Ye, Q.; Jing, D. Free for Caring? The Effect of Offering Free Online Medical-Consulting Services on Physician Performance in e-Health Care. Telemed. E Health 2019, 25, 979–986. [Google Scholar] [CrossRef] [PubMed]
- Bock, G.W.; Zmud, R.W.; Kim, Y.G.; Lee, J.N. Behavioral intention formation in knowledge sharing: Examining the roles of extrinsic motivators, social-psychological factors, and organizational climate. MIS Q. 2005, 29, 87–111. [Google Scholar] [CrossRef]
- Bock, G.W.; Kim, Y.G. Breaking the myths of rewards: An exploratory study of attitudes about knowledge sharing. Inf. Resour. Manag. J. 2002, 15, 14–21. [Google Scholar] [CrossRef] [Green Version]
- Chang, Y.W.; Hsu, P.Y.; Wu, Z.Y. Exploring managers’ intention to use business intelligence: The role of motivations. Behav. Inf. Technol. 2015, 34, 273–285. [Google Scholar] [CrossRef]
- Sedighi, M.; van Splunter, S.; Brazier, F.; van Beers, C.; Lukosch, S. Exploration of multi-layered knowledge sharing participation: The roles of perceived benefits and costs. J. Knowl. Manag. 2016, 20, 1247–1267. [Google Scholar] [CrossRef] [Green Version]
- Huang, Q.; Davison, R.M.; Gu, J. Impact of personal and cultural factors on knowledge sharing in China. Asia Pac. J. Manag. 2008, 25, 451–471. [Google Scholar] [CrossRef]
- Kankanhalli, A.; Tan, B.C.; Wei, K.K. Contributing knowledge to electronic knowledge repositories: An empirical investigation. MIS Q. 2005, 29, 113–143. [Google Scholar] [CrossRef] [Green Version]
- Tsai, M.T.; Chang, H.C.; Cheng, N.C.; Lien, C.C. Understanding IT professionals’ knowledge sharing intention through KMS: A social exchange perspective. Qual. Quant. 2013, 47, 2739–2753. [Google Scholar] [CrossRef]
- Lu, X.; Zhou, H.; Chen, S. Facilitate knowledge sharing by leading ethically: The role of organizational concern and impression management climate. J. Bus. Psychol. 2019, 34, 539–553. [Google Scholar] [CrossRef]
- Ding, G.; Liu, H.; Huang, Q.; Gu, J. Moderating effects of guanxi and face on the relationship between psychological motivation and knowledge-sharing in China. J. Knowl. Manag. 2017, 21, 1077–1097. [Google Scholar] [CrossRef]
- Bagozzi, R.P.; Dholakia, U.M.; Basuroy, S. How effortful decisions get enacted: The motivating role of decision processes, desires, and anticipated emotions. J. Behav. Decis. Mak. 2003, 16, 273–295. [Google Scholar] [CrossRef]
- Dholakia, U.M.; Bagozzi, R.P.; Gopinath, M. How formulating implementation plans and remembering past actions facilitate the enactment of effortful decisions. J. Behav. Decis. Mak. 2007, 20, 343–364. [Google Scholar] [CrossRef] [Green Version]
- Puspitasari, I.; Firdauzy, A. Characterizing Consumer Behavior in Leveraging Social Media for E-Patient and Health-Related Activities. Int. J. Environ. Res. Public Health 2019, 16, 3348. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Wang, M.Y.; Zhang, P.Z.; Zhou, C.Y.; Lai, N.Y. Effect of Emotion, Expectation, and Privacy on Purchase Intention in WeChat Health Product Consumption: The Mediating Role of Trust. Int. J. Environ. Res. Public Health 2019, 16, 3861. [Google Scholar] [CrossRef] [Green Version]
- Snead, K.C.; Harrell, A.M. An application of expectancy theory to explain a manager’s intention to use a decision support system. Decis. Sci. 1994, 25, 499–510. [Google Scholar] [CrossRef]
- Lin, C.P. Modeling corporate citizenship and turnover intention: Social identity and expectancy theories. Rev. Manag. Sci. 2017. [Google Scholar] [CrossRef]
- Rasch, R.H.; Tosi, H.L. Factors affecting software developers’ performance: An integrated approach. MIS Q. 1992, 16, 395–413. [Google Scholar] [CrossRef] [Green Version]
- Vroom, V.H. Work and Motivation; Wiley: New York, NY, USA, 1964; Volume 54. [Google Scholar]
- Chiang, C.F.; Jang, S.S. An expectancy theory model for hotel employee motivation. Int. J. Hosp. Manag. 2008, 27, 313–322. [Google Scholar] [CrossRef]
- Reinharth, L.; Wahba, M.A. Expectancy theory as a predictor of work motivation, effort expenditure, and job performance. Acad. Manag. J. 1975, 18, 520–537. [Google Scholar]
- Mullen, M.R. Diagnosing measurement equivalence in cross-national research. J. Int. Bus. Stud. 1995, 26, 573–596. [Google Scholar] [CrossRef]
- Fornell, C.; Larcker, D.F. Evaluating structural equation models with unobservable variables and measurement error. J. Mark. Res. 1981, 18, 39–50. [Google Scholar] [CrossRef]
- Hair, J.F.; Black, W.C.; Babin, B.J.; Anderson, R.E.; Tatham, R.L. Multivariate Data Analysis; Prentice Hall: Upper Saddle River, NJ, USA, 1998; Volume 5, pp. 207–219. [Google Scholar]
- Nunnally, J.C. Psychometric Methods, 2nd ed.; McGraw-Hill: New York, NY, USA, 1978. [Google Scholar]
- Cao, W.; Zhang, X.; Xu, K.; Wang, Y. Modeling online health information-seeking behavior in China: The roles of source characteristics, reward assessment, and internet self-efficacy. Health Commun. 2016, 31, 1105–1114. [Google Scholar] [CrossRef] [PubMed]
- Zhou, J.; Fan, T. Understanding the factors influencing patient E-health literacy in online health communities (OHCs): A social cognitive theory perspective. Int. J. Environ. Res. Public Health 2019, 16, 2455. [Google Scholar] [CrossRef] [Green Version]
- Perugini, M.; Bagozzi, R.P. The role of desires and anticipated emotions in goal-directed behaviours: Broadening and deepening the theory of planned behaviour. Br. J. Soc. Psychol. 2001, 40, 79–98. [Google Scholar] [CrossRef]

| Construct | Mean | S.D. | Cronbach’s α | CR | AVE | REW | REL | IMG | SSW | DES | WOF | WOP |
|---|---|---|---|---|---|---|---|---|---|---|---|---|
| REW | 4.61 | 0.83 | 0.76 | 0.86 | 0.67 | 0.82 | ||||||
| REL | 4.77 | 0.84 | 0.87 | 0.92 | 0.79 | 0.59 | 0.89 | |||||
| IMG | 4.77 | 0.89 | 0.78 | 0.87 | 0.70 | 0.63 | 0.69 | 0.83 | ||||
| SSW | 4.94 | 0.84 | 0.85 | 0.90 | 0.69 | 0.28 | 0.34 | 0.36 | 0.83 | |||
| DES | 4.78 | 0.76 | 0.80 | 0.88 | 0.72 | 0.55 | 0.69 | 0.61 | 0.40 | 0.85 | ||
| WOF | 4.14 | 1.11 | 0.92 | 0.95 | 0.86 | 0.20 | 0.25 | 0.15 | 0.06 | 0.26 | 0.93 | |
| WOP | 4.96 | 0.90 | 0.93 | 0.95 | 0.87 | 0.33 | 0.37 | 0.33 | 0.41 | 0.30 | −0.12 | 0.93 |
© 2019 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Chen, J.; Lan, Y.-C.; Chang, Y.-W.; Chang, P.-Y. Exploring Doctors’ Willingness to Provide Online Counseling Services: The Roles of Motivations and Costs. Int. J. Environ. Res. Public Health 2020, 17, 110. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph17010110
Chen J, Lan Y-C, Chang Y-W, Chang P-Y. Exploring Doctors’ Willingness to Provide Online Counseling Services: The Roles of Motivations and Costs. International Journal of Environmental Research and Public Health. 2020; 17(1):110. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph17010110
Chicago/Turabian StyleChen, Jiahe, Yi-Chen Lan, Yu-Wei Chang, and Po-Ya Chang. 2020. "Exploring Doctors’ Willingness to Provide Online Counseling Services: The Roles of Motivations and Costs" International Journal of Environmental Research and Public Health 17, no. 1: 110. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph17010110