Effect of a Comprehensive Health Care Program on Blood Pressure, Blood Glucose, Body Composition, and Depression in Older Adults Living Alone: A Quasi-Experimental Pretest–Posttest Study


Abstract
:1. Introduction
2. Materials and Methods
2.1. Design
2.2. Participants
2.3. Data Collection
2.3.1. Blood Pressure
2.3.2. Blood Glucose
2.3.3. Body Composition
2.3.4. Geriatric Depression Scale: Short Form
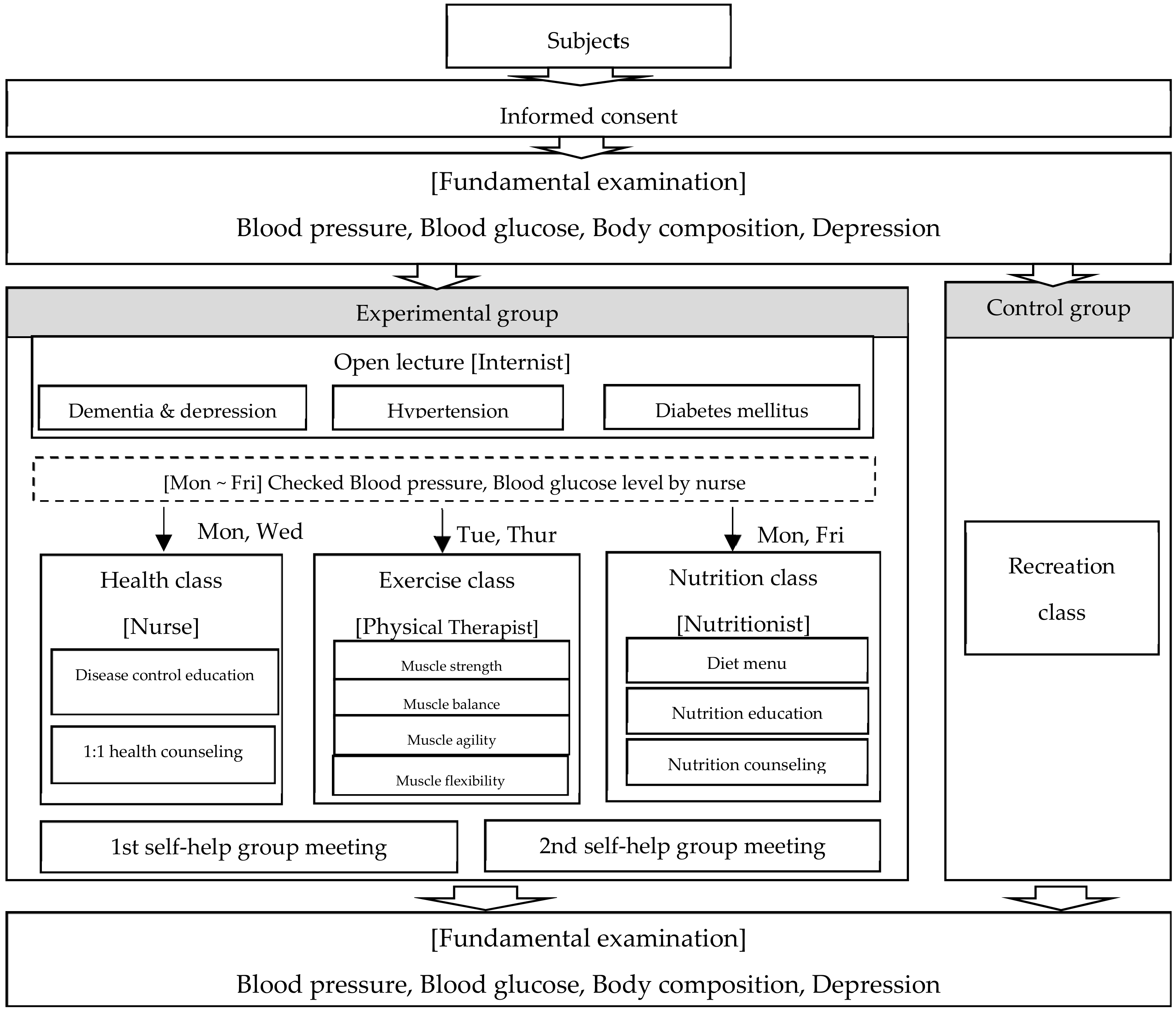
2.3.5. The CHCP Process
2.4. Data Analysis
2.5. Ethical Considerations
3. Results
3.1. Participant Characteristics
3.2. Comparison of Blood Pressure, Blood Glucose, Body Composition, and Depression before and after Participating in the CHCP
4. Discussion
5. Conclusions
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- National Statistical Office. Prospective Estimating Population and Household; National Statistical Office: Daejeon, Korea, 2019; Available online: http://kosis.kr/statisticsList/statisticsListIndex.do?menuId=M_01_01&vwcd=MT_ZTITLE&parmTabId=M_01_01#SelectStatsBoxDiv (accessed on 8 August 2019).
- Ministry of Health and Welfare. 2015 Analysis Report on the Situation of Older Adults Living Alone; The Ministry: Seoul, Korea, 2015; Available online: http://www.1661-2129.or.kr/upload/2015년독거노인현황조사결과분석보고서.pdf (accessed on 5 December 2018). (In Korean)
- Song, M.S.; Boo, S.J. Factors affecting the intention to participate in healthcare programs among elders living alone. J. Korean Acad. Community Health Nurs. 2016, 27. [Google Scholar] [CrossRef] [Green Version]
- Kim, Y.S. The study of the impact of the family type on the health promoting behavior and physical and mental health of elderly people. Health Soc. Welf. Rev. 2014, 34. [Google Scholar]
- Yoon, J.A.; Kang, J.S.; Bae, M.J.; Lee, N.Y.; Lee, C.M.; Jeon, W.J. Comparison of Psychological Well-Being, Self-Esteem and Satisfaction on Life between the Older Adults Living Alone and Older Adults Living with Other. J. Korea Aging Friendly Ind. Assoc. 2016, 8. [Google Scholar]
- Cederbom, S.; Soderlund, A.; Denison, E.; Wagert, P.V.H. Chronic pain among older women living alone: A study focusing on disability and morale. Eur. J. Physiother. 2014, 16. [Google Scholar]
- Korea Institute for Health and Social Affairs. Analysis of Determinants and Regional Differences of Suicide Risk and Regional Differences; The Institute: Seoul, Korea, 2014; Available online: https://www.kihasa.re.kr/web/publication/research/view.do?pageIndex=22&keyField=&key=&menuId=44&tid=71&bid=12&division=001&ano=1826 (accessed on 8 December 2018).
- Zebhauser, A.; Baumert, J.; Emeny, R.T.; Ronel, J.; Peters, A.; Ladwig, K.H. What prevents old people living alone from feeling lonely? Findings from the KORA-Age-study. Aging Ment. Health 2015, 19. [Google Scholar] [CrossRef] [PubMed]
- Chen, Y.; Hicks, A.; While, A.E. Loneliness and social support of older people living alone in a county of Shanghai China. Health Soc. Care Community 2014, 22, 429–438. [Google Scholar] [CrossRef] [PubMed]
- Kim, G.W.; Kim, Y.M. The Effects of Program Factors on the Quality of Life in the Senior Welfare Center: Focusing on social support parameters. J. Korean Policy Stud. 2016, 16, 37–52. [Google Scholar]
- Park, N.S.; Jang, Y.; Lee, B.S.; Chiriboga, D.A. The relation between living alone and depressive symptoms in older Korean Americans: Do feelings of loneliness mediate? Aging Ment. Health 2017, 21. [Google Scholar] [CrossRef]
- Faul, F.; Erdfelder, E.; Lang, A.-G.; Buchner, A. G*Power 3: A flexible statistical power analysis program for the social, behavioral, and biomedical sciences. Behav. Res. Methods 2007, 39, 175–191. [Google Scholar] [CrossRef]
- American Heart Association. Healthy and Unhealthy Blood Pressure Ranges. Texas (USA): The Association. 2019. Available online: http://www.heart.org/HEARTORG/Conditions/HighBloodPressure/AboutHighBloodPressure/Understanding-Blood-Pressure-Readings_UCM_301764_Article.jsp (accessed on 10 January 2019).
- Korean Diabetes Association. Diabetes Treatment and Control; The Association: Seoul, Korea, 2019; Available online: http://www.diabetes.or.kr/general/class/medical.php?mode=view&number=322&idx=6 (accessed on 8 November 2018).
- Yesavage, J.A.; Sheikh, J.I. Geriatric depression scale (GDS): Recent evidence and development of a shorter version. Clin. Geront. 1986, 5. [Google Scholar] [CrossRef]
- Kee, B.S. A preliminary study for the standardization of geriatric depression scale short form-Korea Version. J. Korean Neuropsychiatr. Assoc. 1996, 131, 298–307. [Google Scholar]
- Dorji, N.; Dunne, M.P.; Seib, C.; Deb, S. Quality of life among senior citizens in Bhutan: Associations with adverse life experiences, chronic diseases, spirituality, and social connectedness. Asia Pac. J. Pub. Health 2017, 29. [Google Scholar] [CrossRef] [PubMed]
- Yu, J.O.; Kim, J.S. Effects of a physical activity program using exergame with elderly women. J. Korean Acad. Nurs. 2015, 45. [Google Scholar] [CrossRef] [PubMed]
- Jang, S.J.; Park, H.J.; Kim, H.J.; Chang, S.J. Factors influencing physical activity among community-dwelling older adults with type 2 diabetes: A path analysis. J. Korean Acad. Nurs. 2015, 45. [Google Scholar] [CrossRef]
- Parry, S.; Chow, M.; Batchelor, F.; Fary, R.E. Physical activity and sedentary behavior in a residential aged care facility. Australas. J. Age. 2019, 38. [Google Scholar]
- Jefferis, B.J.; Merom, D.; Sartini, C.; Wannamethee, S.G.; Ash, S.; Lennon, L.T.; Lliffe, S.; Kendrick, D.; Whincup, P.H. Physical activity and falls in older men: The critical role of mobility limitation. Med. Sci. Sports Exerc. 2015, 47. [Google Scholar] [CrossRef] [Green Version]
- Jeon, M.Y.; Gu, M.O.; Yim, J.E. Comparison of walking, muscle strength, balance, and fear of falling between repeated fall group, one-time fall group, and nonfall group of the older adults receiving home care service. Asian Nurs. Res. 2017, 11. [Google Scholar] [CrossRef] [Green Version]
- Kim, H.J. Health promotion behaviors of rural elderly women living alone and their life satisfaction. J. Korean Acad. Community Health Nurs. 2016, 27. [Google Scholar] [CrossRef] [Green Version]
- Cho, S.H.; Lee, H.Y. A study on life satisfaction of low-income elderly people who living alone. J. Korea Acad. Indust. Coop. Soc. 2015, 16. [Google Scholar]
- Lee, H.S.; Kim, C. Structural equation modeling to assess discrimination, stress, social support, and depression among the elderly women in South Korea. Asian Nurs. Res. 2016, 10. [Google Scholar] [CrossRef] [Green Version]
- Lee, S.S.; Kim, S.H. A study on the living conditions and social welfare needs of the older adults who lives alone in the farming and fishing communities-focused on the province of Jeollanamdo. Korean Assoc. Reg. Dev. 2011, 11, 23–60. [Google Scholar]


{kind=link}
| Variables | Experimental Group (n = 30) | Control Group (n = 28) | t or χ2 | p-Value | ||
|---|---|---|---|---|---|---|
| n | % | n | % | |||
| Gender | ||||||
| Male | 11 | 36.7 | 17 | 60.7 | 3.35 | 0.058 |
| Female | 19 | 63.3 | 11 | 39.3 | ||
| Age | ||||||
| 65–69 | 1 | 3.3 | 3 | 10.7 | 1.30 | 0.521 |
| 70–79 | 15 | 50.0 | 12 | 42.9 | ||
| ≤80 | 14 | 46.7 | 13 | 46.4 | ||
| M ± SD | 78.17 ± 4.92 | 77.64 ± 6.45 | 0.35 | 0.728 | ||
| Disease | ||||||
| HT | 18 | 60.0 | 14 | 50.0 | 0.68 | 0.712 |
| DM | 2 | 6.7 | 3 | 10.7 | ||
| Both | 10 | 33.3 | 11 | 39.3 | ||
| Variables | Pretest | Posttest | t (p) | Differences | t (p) | ||
|---|---|---|---|---|---|---|---|
| BP | SBP | Experimental group | 139.91 ± 21.65 | 132.96 ± 12.83 | 1.26 (0.222) | −6.96 ± 26.56 | −2.53 (0.016) |
| Control group | 130.71 ± 14.98 | 139.88 ± 15.37 | −2.91 (0.008) | 9.17 ± 15.43 | |||
| t (p) | 1.69 (0.099) | −1.67 (0.102) | |||||
| DBP | Experimental group | 78.67 ± 17.42 | 81.47 ± 11.64 | −0.65 (0.520) | 2.800 ± 23.55 | 0.42 (0.674) | |
| Control group | 76.81 ± 13.27 | 77.44 ± 13.45 | −0.23 (0.824) | 0.63 ± 14.53 | |||
| t (p) | 0.45 (0.656) | 1.21 (0.231) | |||||
| BG | Experimental group | 132.04 ± 36.17 | 131.35 ± 39.47 | 0.12 (0.904) | −0.69 ± 28.93 | −3.09 (0.004) | |
| Control group | 126.50 ± 39.75 | 161.71 ± 59.47 | −3.68 (0.001) | 29.30 ± 37.79 | |||
| t (p) | 0.52 (0.608) | −2.37 (0.022) | |||||
| BC | MM | Experimental group | 21.59 ± 4.64 | 21.75 ± 4.72 | −0.47 (0.644) | 0.16 ± 1.87 | 1.44 (0.156) |
| Control group | 22.51 ± 4.20 | 22.03 ± 3.94 | 2.13 (0.046) | −0.48 ± 1.05 | |||
| t (p) | 0.69 (0.494) | −0.23 (0.820) | |||||
| BFM | Experimental group | 31.49 ± 8.92 | 32.34 ± 8.77 | −0.87 (0.395) | 0.85 ± 5.12 | 0.43 (0.670) | |
| Control group | 32.59 ± 8.32 | 32.90 ± 7.83 | −0.72 (0.479) | 0.31 ± 1.82 | |||
| t (p) | −0.30 (0.766) | −0.02 (0.987) | |||||
| Depression | Experimental group | 7.60 ± 4.00 | 5.80 ± 2.93 | 3.95 (0.000) | −1.80 ± 2.50 | −1.15 (0.255) | |
| Control group | 7.47 ± 4.75 | 6.41 ± 4.00 | 3.82 (0.002) | −1.06 ± 1.14 | |||
| t (p) | 0.10 (0.921) | −0.60 (0.550) |
© 2019 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Hwang, E.J.; Sim, I.O. Effect of a Comprehensive Health Care Program on Blood Pressure, Blood Glucose, Body Composition, and Depression in Older Adults Living Alone: A Quasi-Experimental Pretest–Posttest Study. Int. J. Environ. Res. Public Health 2020, 17, 220. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph17010220
Hwang EJ, Sim IO. Effect of a Comprehensive Health Care Program on Blood Pressure, Blood Glucose, Body Composition, and Depression in Older Adults Living Alone: A Quasi-Experimental Pretest–Posttest Study. International Journal of Environmental Research and Public Health. 2020; 17(1):220. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph17010220
Chicago/Turabian StyleHwang, Eun Jeong, and In Ok Sim. 2020. "Effect of a Comprehensive Health Care Program on Blood Pressure, Blood Glucose, Body Composition, and Depression in Older Adults Living Alone: A Quasi-Experimental Pretest–Posttest Study" International Journal of Environmental Research and Public Health 17, no. 1: 220. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph17010220