Associations between Facial Emotion Recognition and Mental Health in Early Adolescence

 ,
, 
Abstract
:1. Introduction
2. Materials and Methods
2.1. Participants
2.2. Mental Health
2.3. Emotion Recognition (ER)
2.4. Statistical Analyses
3. Results
3.1. Mental Health
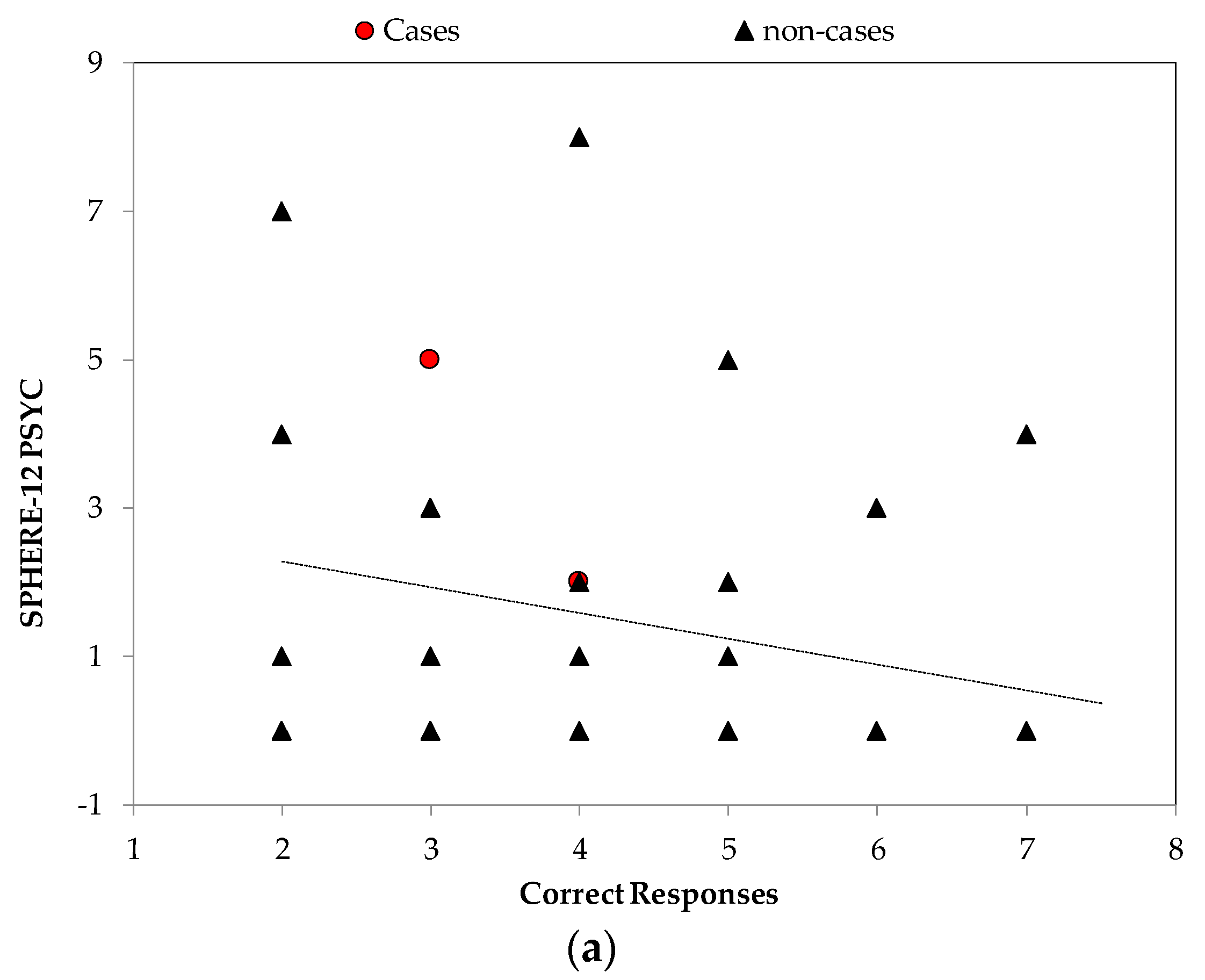
3.2. Mental Health and ER: Anger
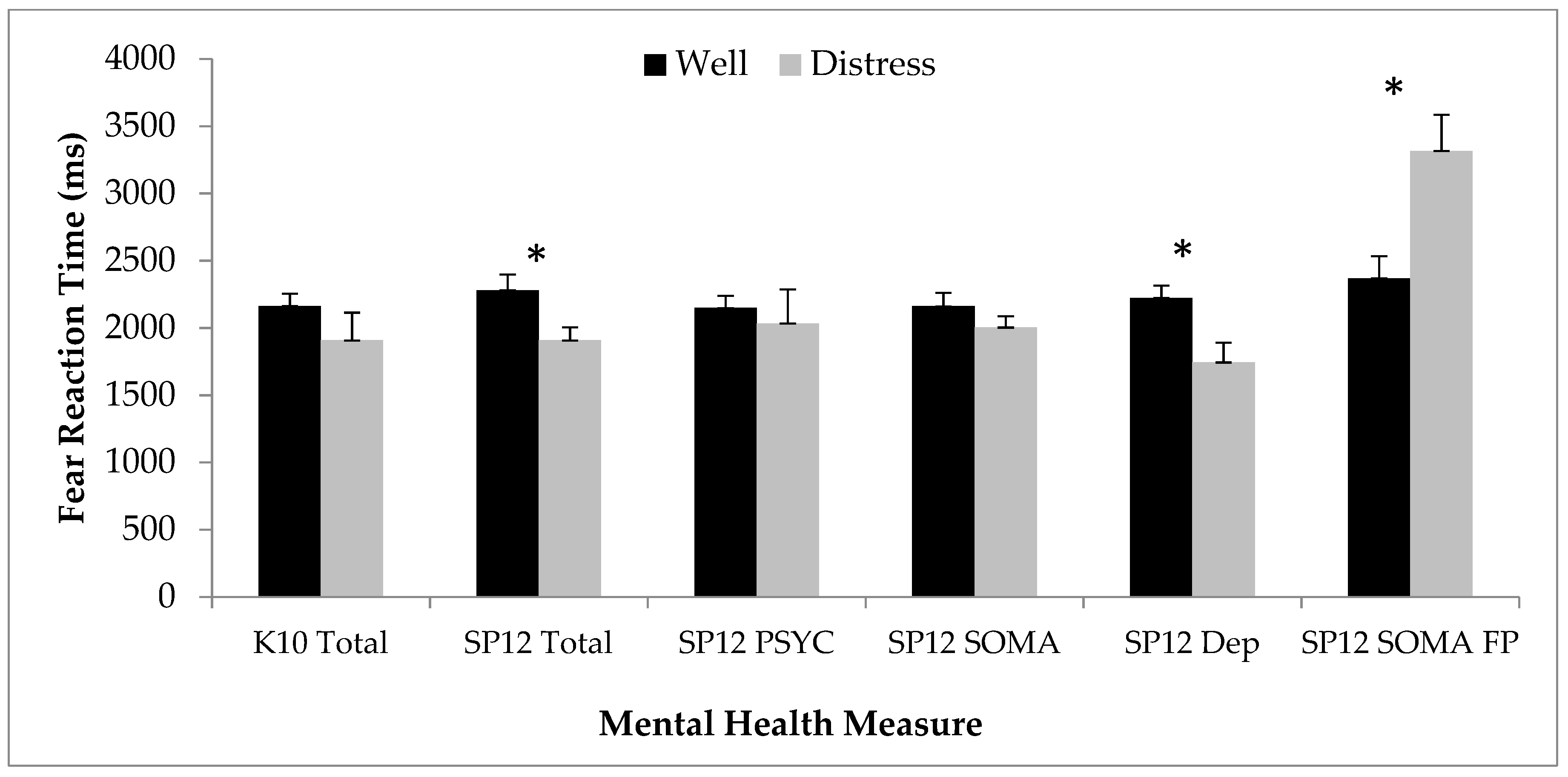
3.3. Mental Health and ER: Fear
3.4. Mental Health and ER: Neutral
3.5. Mental Health and ER: Happy and Sad
4. Discussion
5. Conclusions
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- Lawrence, K.; Campbell, R.; Skuse, D. Age, gender, and puberty influence the development of facial emotion recognition. Front. Psychol. 2015, 6, 761. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Serrano, J.M.; Iglesias, J.; Loeches, A. Visual discrimination and recognition of facial expressions of anger, fear, and surprise in 4- to 6-month-old infants. Dev. Psychobiol. 1992, 25, 411–425. [Google Scholar] [CrossRef] [PubMed]
- McClure, E.B. A meta-analytic review of sex differences in facial expression processing and their development in infants, children, and adolescents. Psychol. Bull. 2000, 126, 424–453. [Google Scholar] [CrossRef] [PubMed]
- Herba, C.; Phillips, M. Annotation: Development of facial expression recognition from childhood to adolescence: Behavioural and neurological perspectives. J. Child Psychol. Psychiatry 2004, 45, 1185–1198. [Google Scholar] [CrossRef] [PubMed]
- Ekman, P.; Friesen, W.V. Constants across cultures in the face and emotion. J. Personal. Soc. Psychol. 1971, 17, 124–129. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Demenescu, L.R.; Kortekaas, R.; den Boer, J.A.; Aleman, A. Impaired attribution of emotion to facial expressions in anxiety and major depression. PLoS ONE 2010, 5, e15058. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Keltner, D. Expression and the course of life: Studies of emotion, personality, and psychopathology from a social-functional perspective. Ann. N. Y. Acad. Sci. 2003, 1000, 222–243. [Google Scholar] [CrossRef]
- Tse, W.S.; Bond, A.J. The impact of depression on social skills. J. Nerv. Ment. Dis. 2004, 192, 260–268. [Google Scholar] [CrossRef]
- McClure, E.B.; Pope, K.; Hoberman, A.J.; Pine, D.S.; Leibenluft, E. Facial expression recognition in adolescents with mood and anxiety disorders. Am. J. Psychiatry 2003, 160, 1172–1174. [Google Scholar] [CrossRef] [Green Version]
- Masten, C.L.; Guyer, A.E.; Hodgdon, H.B.; McClure, E.B.; Charney, D.S.; Ernst, M.; Kaufman, J.; Pine, D.S.; Monk, C.S. Recognition of facial emotions among maltreated children with high rates of post-traumatic stress disorder. Child Abus. Negl. 2008, 32, 139–153. [Google Scholar] [CrossRef] [Green Version]
- Berg, H.E.; Ballard, E.D.; Luckenbaugh, D.A.; Nugent, A.C.; Inonescu, D.F.; Zarate, C.A.J. Recognition of emotional facial expressions in anxious and nonanxious depression. Compr. Psychiatry 2016, 70, 1–8. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Brotman, M.A.; Rich, B.A.; Schmajuk, M.; Reising, M.M.; Monk, C.S.; Dickstein, D.P.; Mogg, K.; Bradley, B.P.; Pine, D.S.; Leibenluft, E. Attention bias to threat faces in children with bipolar disorder and comorbid lifetime anxiety disorders. Biol. Psychiatry 2007, 61, 819–821. [Google Scholar] [CrossRef] [PubMed]
- Waters, A.M.; Henry, J.; Mogg, K.; Bradley, B.P.; Pine, D.S. Attentional bias towards angry faces in childhood anxiety disorders. J. Behav. Ther. Exp. Psychiatry 2010, 41, 158–164. [Google Scholar] [CrossRef] [PubMed]
- Lenti, C.; Giacobbe, A.; Pegna, C. Recognition of emotional facial expressions in depressed children and adolescents. Percept. Mot. Skills 2000, 91, 227–236. [Google Scholar] [CrossRef] [PubMed]
- Jarros, R.B.; Salum, G.A.; Belem da Silva, C.T.; Toazza, R.; de Abreu Costa, M.; Fumagalli de Salles, J.; Manfro, G.G. Anxiety disorders in adolescence are associated with impaired facial expression recognition to negative valence. J. Psychiatr. Res. 2012, 46, 147–151. [Google Scholar] [CrossRef] [PubMed]
- Schepman, K.; Taylor, E.; Collishaw, S.; Fombonne, D. Face emotion processing in depressed children and adolescents with and without comorbid conduct disorder. J. Child Psychol. 2012, 40, 583–593. [Google Scholar] [CrossRef]
- Blair, R.J.R.; Colledge, E.; Murray, L.; Mitchell, D.G.V. A selectivei mpairment in the processing of sad and fearful expressions in children with psychopathic tendencies. J. Child Psychol. 2001, 29, 491–498. [Google Scholar]
- Lopez-Duran, N.L.; Kuhlman, K.R.; George, C.; Kavacs, M. Facial expression recognition by children at familial risk for depression: High-risk boys are oversensitive to sadness. J. Child Psychol. Psychiatry 2013, 54, 565–574. [Google Scholar] [CrossRef] [Green Version]
- Kessler, R.C.; Berglund, P.; Demler, O.; Jin, R.; Merikangas, K.R.; Walters, E.E. Lifetime prevalence and age-of-Onset Distributions of DSM-IV Disorders in the National Comorbidity Survey Replication. Arch. Gen. Psychiatry 2005, 62, 593–602. [Google Scholar] [CrossRef] [Green Version]
- Lawrence, D.; Johnson, S.; Hafekost, J.; Boterhoven de Haan, K.; Sawyer, M.; Ainle, J.; Zubrick, S.R. The Mental Health of Children and Adolescents. Report on the Second Australian Child and Adolescent Survey of Mental Health and Wellbeing; Department of Health: Canberra, Australia, 2015.
- Kessler, R.C.; Avenevoli, S.; Ries Merikangas, K. Mood disorders in children and adolescents: An epidemiologic perspective. Biol. Psychiatry 2001, 49, 1002–1014. [Google Scholar] [CrossRef]
- Kessler, R.C.; Andrews, G.; Colpe, L.J.; Hiripi, E.; Mroczek, D.K.; Normand, S.L.; Walters, E.E.; Zaslavsky, A.M. Short screening scales to monitor population prevalences and trends in non-specific psychological distress. Psychol. Med. 2002, 32, 959–976. [Google Scholar] [CrossRef] [PubMed]
- Chan, S.M.; Tong Fung, T.C. Reliability and validity of K10 and K6 in screening depressive symptoms in Hong Kong adolescents. Vulnerable Child. Youth Stud. 2014, 9, 75–85. [Google Scholar] [CrossRef]
- Hickie, I.B.; Davenport, T.A.; Naismith, S.L.; Scott, E.M. SPHERE: A national depression project. SPHERE National Secretariat. Med. J. Aust. 2001, 175, S4–S5. [Google Scholar] [CrossRef] [PubMed]
- Scott, J.; Davenport, T.A.; Parker, R.; Hermens, D.F.; Lind, P.A.; Meland, S.E.; Wright, M.J.; Martin, N.G.; Gillespie, N.A.; Hickie, I.B. Pathways to depression by age 16 years: Examining trajectories for self-reported psychological and somatic phenotypes across adolescence. J. Affect. Disord. 2018, 230, 1–6. [Google Scholar] [CrossRef] [Green Version]
- Gur, R.C.; Ragland, J.D.; Moberg, P.J.; Turner, T.H.; Bilker, W.B.; Kohler, C.G.; Seigel, S.J.; Gur, R.E. Computerized neurocognitive scanning: I. Methodology and validation in healthy people. Neuropsychopharmacol. Off. Publ. Am. Coll. Neuropsychopharmacol. 2001, 25, 766–776. [Google Scholar] [CrossRef] [Green Version]
- Roddy, S.; Tiedt, L.; Kelleher, I.; Clarke, M.C.; Murphy, J.; Rawdon, C.; Roche, R.A.; Calkins, M.E.; Richard, J.A.; Kohler, C.G.; et al. Facial emotion recognition in adolescents with psychotic-like experiences: A school-based sample from the general population. Psychol. Med. 2012, 42, 2157–2166. [Google Scholar] [CrossRef] [Green Version]
- Taylor, S.F.; McDonald, A.W., III. Brain mapping biomarkers of socio-emotional processing in schizophrenia. Schizophr. Bull. 2012, 38, 73–80. [Google Scholar] [CrossRef] [Green Version]
- Keyes, C.L. The mental health continuum: From languishing to flourishing in life. J. Health Soc. Behav. 2002, 43, 207–222. [Google Scholar] [CrossRef] [Green Version]
- Keyes, C.L. Mental illness and/or mental health? Investigating axioms of the complete state model of health. J. Consult. Clin. Psychol. 2005, 73, 539–548. [Google Scholar] [CrossRef] [Green Version]
- Keyes, C.L. Mental health in adolescence: Is America’s youth flourishing? Am. J. Orthopsychiatry 2006, 76, 395–402. [Google Scholar] [CrossRef]
- Han, G.; KiLimer-Dougan, B.; Jespen, S.; Barllard, K.; Nelson, M.; Houri, A.; Kumra, S.; Cullen, K. Selective neurocognitive impairments in adolescents with major depressive disorder. J. Adolesc. 2012, 35, 11–20. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Bozorg, B.; Tehrain-Doost, M.; Sharhrivar, Z.; Fata, L.; Mohamadzadeh, A. Facial emotion recognition in adolescents with bipolar disorder. Iran J. Psychiatry 2014, 9, 20–24. [Google Scholar] [PubMed]
- Blair, R.J.R.; Morris, J.S.; Frith, C.D.; Perrett, D.I.; Dolan, R.J. Dissociable neural responses to facial expressions of sadness and anger. Brain 1999, 122, 883–893. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Penton-Voak, I.; Bate, H.; Lewis, G.; Munafo, M.R. Effects of emotion perception training on mood in undergraduate students: Randomised controlled trial. Br. J. Psychiatry 2012, 20, 71–72. [Google Scholar] [CrossRef] [PubMed]
- Rawdon, D.; Murphy, D.; Motyer, G.; Munafo, M.R.; Penton-Voak, I.; Fitxgerald, A. An investigation of emotion recognition training to reduce symptoms of social anxiety in adolescence. Psychiatry Res. 2018, 263, 257–267. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Melfsen, S.; Florin, I. Do socially anxious children show deficits in classifying facial expressions of emotions? J. Nonverbal Behav. 2002, 26, 109–126. [Google Scholar] [CrossRef]
- Sheehan, D.V.; Lecrubier, Y.; Sheehan, K.H.; Amorim, P.; Janavs, J.; Weiller, E.; Hergueta, T.; Baker, R.; Dunbar, G.C. The Mini-International Neuropsychiatric Interview (M.I.N.I.): The development and validation of a structured diagnostic psychiatric interview for DSM-IV and ICD-10. J. Clin. Psychiatry 1998, 59 (Suppl. 20), 22–33. [Google Scholar]
- Broadhouse, K.M.; Boyes, A.; Winks, N.; Dokonal, T.; McLoughlin, L.; Parker, M.; Beaudequin, D.; Simcock, G.; Lagopoulos, J.; Hermens, D.F. Subcortical volume correlates of psychological distress in early adolescence. Dev. Neurosci. 2019. [Google Scholar] [CrossRef]
- Broadhouse, K.M.; Winks, N.; McLoughlin, L.; Parker, M.; Beaudequin, D.; Simcock, G. Resting-state functional neurobiological signatures associated with psychological distress in early adolescence. Eur. J. Child Adolesc. Psychol. under review.




{kind=link}
{kind=link}
{kind=link}
| Mental Health | K10 | S 12 Total | SP12 PSYCH | SP12 SOMA | Mean (SD) | Possible Mental Disorder N (%) |
|---|---|---|---|---|---|---|
| K10 | 15.13 (4.45) | 5 (12.5) | ||||
| SP12 Total | 0.61 ** | 4.08 (3.75) | 16 (40) | |||
| SP12 PSYC | 0.51 ** | 0.79 ** | 1.43 (2.02) | 4 (10) | ||
| SP12 SOMA | 0.57 ** | 0.91 ** | 0.52 ** | 2.65 (2.51) | 7 (17.5) | |
| SP12 Depression | 0.37 * | 0.65 ** | 0.65 ** | 0.46 ** | 0.18 (0.38) | 7 (17.5) |
| Facial Expressions | |||||
|---|---|---|---|---|---|
| Mental Health | Anger | Fear | Happy | Neutral | Sad |
| Correct Responses (CR) | |||||
| K10 | −0.07 | 0.12 | −0.08 | 0.10 | −0.16 |
| SP12 Total | −0.15 | 0.01 | 0.06 | 0.35 * | −0.17 |
| SP12 PSYC | −0.32 * | 0.03 | −0.02 | 0.32 * | −0.21 |
| SP12 SOMA | −0.06 | −0.03 | 0.07 | 0.26 | −0.18 |
| SP12 Depression | −0.16 | −0.06 | 0.15 | 0.40 * | −0.04 |
| False Positives (FP) | |||||
| K10 | −0.11 | −0.12 | −0.10 | 0.11 | −0.10 |
| SP12 Total | −0.28 * | 0.10 | −0.22 | 0.07 | −0.06 |
| SP12 PSYC | −0.42 ** | 0.23 | −0.11 | 0.17 | −0.07 |
| SP12 SOMA | −0.17 | −0.05 | −0.18 | 0.18 | −0.09 |
| SP12 Depression | −0.15 | 0.15 | −0.09 | −0.01 | 0.01 |
| Reaction Time for CR | |||||
| K10 | −0.07 | −0.36 * | 0.001 | 0.29 | 0.13 |
| SP12 Total | −0.003 | −0.40 * | 0.02 | 0.13 | −0.06 |
| SP12 PSYC | −0.02 | −0.31 | 0.01 | 0.04 | −0.13 |
| SP12 SOMA | −0.20 | −0.41 ** | 0.06 | 0.16 | −0.04 |
| SP12 Depression | −0.01 | −0.12 | 0.01 | 0.05 | −0.21 |
| Reaction Time for FP | |||||
| K10 | 0.68 * | −0.10 | −0.12 | −0.03 | 0.02 |
| SP12 Total | 0.50 | −0.02 | −0.04 | −0.24 | 0.10 |
| SP12 PSYC | 0.54 | −0.18 | −0.09 | −0.23 | 0.01 |
| SP12 SOMA | 0.50 | 0.11 | 0.07 | −0.22 | 0.11 |
| SP12 Depression | 0.50 | −0.22 | −0.10 | −0.16 | −0.05 |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Simcock, G.; McLoughlin, L.T.; De Regt, T.; Broadhouse, K.M.; Beaudequin, D.; Lagopoulos, J.; Hermens, D.F. Associations between Facial Emotion Recognition and Mental Health in Early Adolescence. Int. J. Environ. Res. Public Health 2020, 17, 330. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph17010330
Simcock G, McLoughlin LT, De Regt T, Broadhouse KM, Beaudequin D, Lagopoulos J, Hermens DF. Associations between Facial Emotion Recognition and Mental Health in Early Adolescence. International Journal of Environmental Research and Public Health. 2020; 17(1):330. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph17010330
Chicago/Turabian StyleSimcock, Gabrielle, Larisa T. McLoughlin, Tamara De Regt, Kathryn M. Broadhouse, Denise Beaudequin, Jim Lagopoulos, and Daniel F. Hermens. 2020. "Associations between Facial Emotion Recognition and Mental Health in Early Adolescence" International Journal of Environmental Research and Public Health 17, no. 1: 330. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph17010330