The Association of Periodontal Treatment and Decreased Pneumonia: A Nationwide Population-Based Cohort Study


Abstract
:1. Introduction
2. Materials and Methods
2.1. Data Source
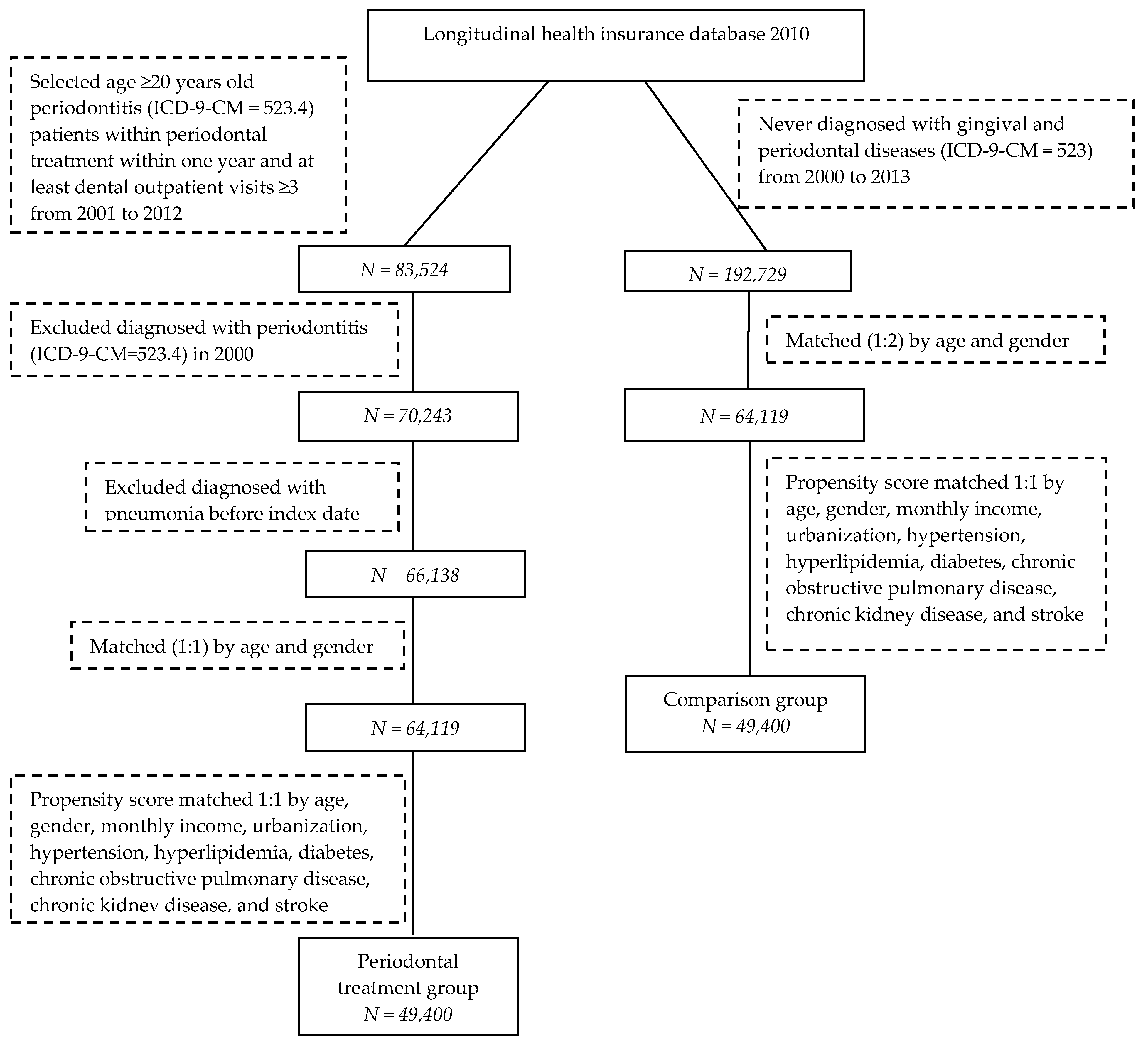
2.2. Study Sample
2.3. Covariates and Matching
2.4. Pneumonia Event
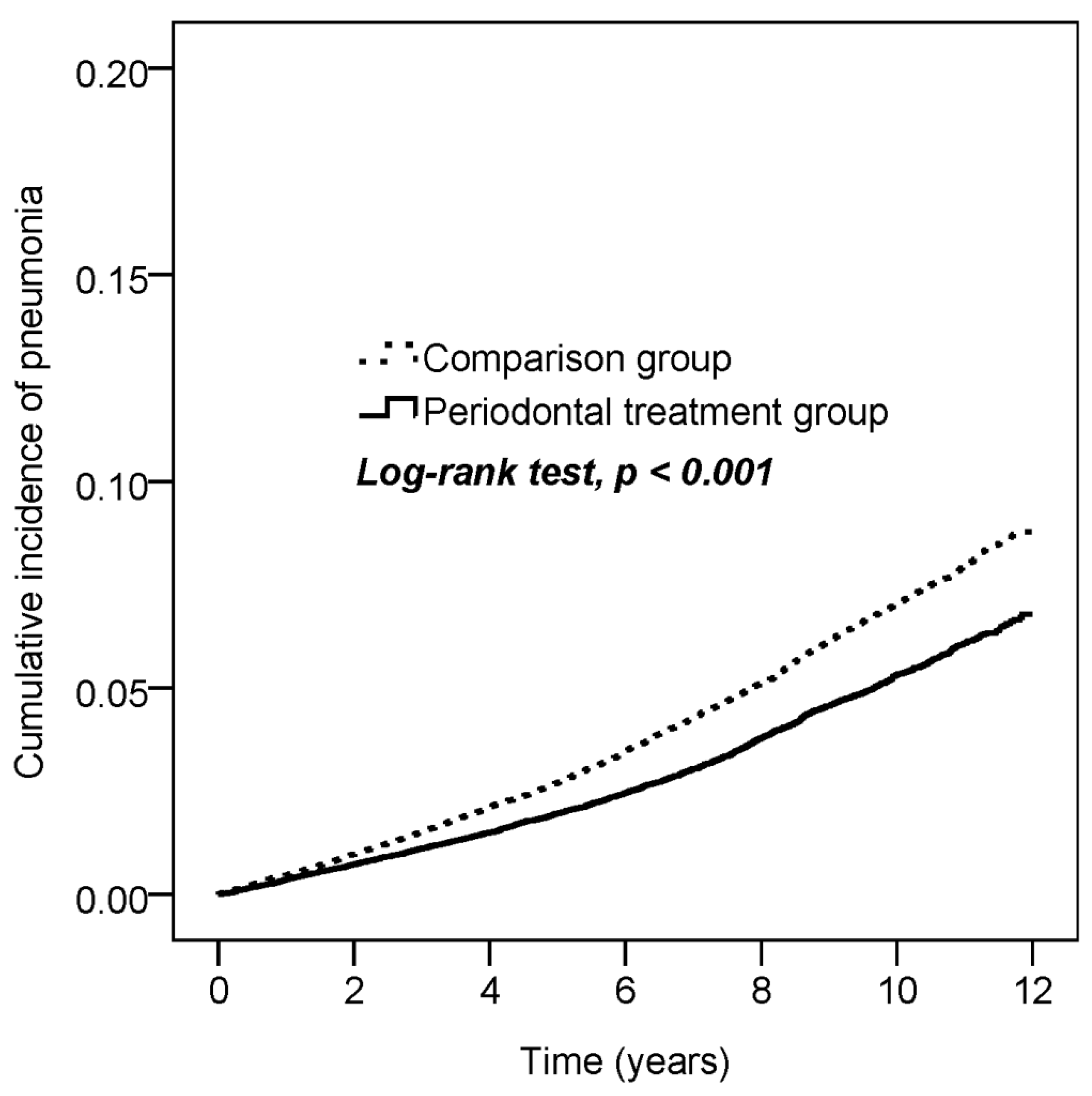
2.5. Statistical Analysis
3. Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Conflicts of Interest
References
- Reddy, M.S. Reaching a better understanding of non-oral disease and the implication of periodontal infections. Periodontol. 2000 2007, 44, 9–14. [Google Scholar] [CrossRef]
- Williams, R.C.; Offenbacher, S. Periodontal medicine: The emergence of a new branch of periodontology. Periodontol. 2000 2000, 23, 9–12. [Google Scholar] [CrossRef]
- Beck, J.; Garcia, R.; Heiss, G.; Vokonas, P.S.; Offenbacher, S. Periodontal disease and cardiovascular disease. J. Periodontol. 1996, 67, 1123–1137. [Google Scholar] [CrossRef]
- Polak, D.; Shapira, L. An update on the evidence for pathogenic mechanisms that may link periodontitis and diabetes. J. Clin. Periodontol. 2018, 45, 150–166. [Google Scholar] [CrossRef]
- Scannapieco, F.A.; Cantos, A. Oral inflammation and infection, and chronic medical diseases: Implications for the elderly. Periodontol. 2000. 2016, 72, 153–175. [Google Scholar] [CrossRef]
- World Health Organization. The Top 10 Causes of Death. Available online: http://www.who.int/mediacentre/factsheets/fs310/en/ (accessed on 13 October 2019).
- Ministry of Health and Welfare. Taiwan, R.O.C. The Top 10 Causes of Death 2018. Available online: https://www.mohw.gov.tw/cp-4256-48057-1.html (accessed on 13 October 2019).
- Raghavendran, K.; Mylotte, J.M.; Scannapieco, F.A. Nursing home-associated pneumonia, hospital-acquired pneumonia and ventilator-associated pneumonia: The contribution of dental biofilms and periodontal inflammation. Periodontol. 2000 2007, 44, 164–177. [Google Scholar] [CrossRef]
- Sumi, Y.; Miura, H.; Sunakawa, M.; Michiwaki, Y.; Sakagami, N. Colonization of denture plaque by respiratory pathogens in dependent elderly. Gerodontology 2002, 19, 25–29. [Google Scholar] [CrossRef] [PubMed]
- Sumi, Y.; Kagami, H.; Ohtsuka, Y.; Kakinoki, Y.; Haruguchi, Y.; Miyamoto, H. High correlation between the bacterial species in denture plaque and pharyngeal microflora. Gerodontology 2003, 20, 84–87. [Google Scholar] [CrossRef] [PubMed]
- National Health Insurance Administration. Ministry of Health and Welfare, Taiwan, R.O.C. National Health Insurance Annual Report 2014–2015. Available online: https://www.nhi.gov.tw/english/Content_List.aspx?n=D8ECF7F6C9D80FC1&topn=616B97F8DF2C3614 (accessed on 13 October 2019).
- Yu, H.C.; Chen, T.P.; Wei, C.Y.; Chang, Y.C. Association between peptic ulcer disease and periodontitis: A nationwide population-based case-control study in Taiwan. Int. J. Environ. Res. Public Health 2018, 15, 912. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Chen, C.K.; Huang, J.Y.; Wu, Y.T.; Chang, Y.C. Dental scaling decreases the risk of Parkinson’s disease: A nationwide population-based nested case-control study. Int. J. Environ. Res. Public Health 2018, 15, 1568. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Tong, C.; Wang, Y.H.; Chang, Y.C. Increased risk of carotid atherosclerosis in male patients with chronic periodontitis: A nationwide population-based retrospective cohort study. Int. J. Environ. Res. Public Health 2019, 16, 2635. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ministry of Labor, Taiwan, R.O.C. 2013. Available online: https://www.mol.gov.tw/topic/3067/5990/13171/19154/ (accessed on 19 December 2019).
- Liu, C.Y.; Hung, Y.T.; Chuang, Y.L.; Chen, Y.J.; Weng, W.S.; Liu, J.S.; Liang, K.Y. Incorporating development stratification of Taiwan townships into sampling design of large scale health interview survey. J. Health Manag. 2006, 4, 1–22. (In Chinese) [Google Scholar]
- Terpenning, M.S.; Taylor, G.W.; Lopatin, D.E.; Kerr, C.K.; Dominguez, B.L.; Loesche, W.J. Aspiration pneumonia: Dental and oral risk factors in an older veteran population. J. Am. Geriatr. Soc. 2001, 49, 557–563. [Google Scholar] [CrossRef] [PubMed]
- de Melo Neto, J.P.; Melo, M.S.; dos Santos-Pereira, S.A.; Martinez, E.F.; Okajima, L.S.; Saba-Chujfi, E. Periodontal infections and community-acquired pneumonia: A case-control study. Eur. J. Clin. Microbiol. Infect. Dis. 2013, 32, 27–32. [Google Scholar] [CrossRef] [PubMed]
- Gomes-Filho, I.S.; de Oliveira, T.F.; da Cruz, S.S.; Passos-Soares Jde, S.; Trindade, S.C.; Oliveira, M.T.; Souza-Machado, A.; Cruz, Á.A.; Barreto, M.L.; Seymour, G.J. Influence of periodontitis in the development of nosocomial pneumonia: A case-control study. J. Periodontol. 2014, 85, 82–90. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Yoneyama, T.; Yoshida, M.; Ohrui, T.; Mukaiyama, H.; Okamoto, H.; Hoshiba, K.; Ihara, S.; Yanagisawa, S.; Ariumi, S.; Morita, T.; et al. Oral care reduces pneumonia in older patients in nursing homes. J. Am. Geriatr. Soc. 2002, 50, 430–433. [Google Scholar] [CrossRef] [PubMed]
- Huang, S.T.; Lin, C.L.; Yu, T.M.; Wu, M.J.; Kao, C.H. Intensive periodontal treatment reduces risk of infection-related hospitalization in hemodialysis population: A nationwide population-based cohort study. Medicine 2015, 94, 1436. [Google Scholar] [CrossRef]
- Paju, S.; Scannapieco, F.A. Oral biofilms, periodontitis, and pulmonary infections. Oral Dis. 2007, 13, 508–512. [Google Scholar] [CrossRef] [Green Version]
- Scannapieco, F.A. Role of oral bacteria in respiratory infection. J. Periodontol. 1999, 70, 793–802. [Google Scholar] [CrossRef]
- Azarpazhooh, A.; Leake, J.L. Systematic review of the association between respiratory diseases and oral health. J. Periodontol. 2006, 77, 1465–1482. [Google Scholar] [CrossRef] [Green Version]
- Fourrier, F.; Cau-Pottier, E.; Boutigny, H.; Roussel-Delvallez, M.; Jourdain, M.; Chopin, C. Effects of dental plaque antiseptic decontamination on bacterial colonization and nosocomial infections in critically ill patients. Intensive Care Med. 2000, 26, 1239–1247. [Google Scholar] [CrossRef] [PubMed]
- Didilescu, A.C.; Skaug, N.; Marica, C.; Didilescu, C. Respiratory pathogens in dental plaque of hospitalized patients with chronic lung diseases. Clin. Oral Investig. 2005, 9, 141–147. [Google Scholar] [CrossRef] [PubMed]
- Sumi, Y.; Miura, H.; Michiwaki, Y.; Nagaosa, S.; Nagaya, M. Colonization of dental plaque by respiratory pathogens in dependent elderly. Arch. Gerontol. Geriatr. 2007, 44, 119–124. [Google Scholar] [CrossRef] [PubMed]
- Joshi, N.; O’Bryan, T.; Appelbaum, P.C. Pleuropulmonary infections caused by Eikenella corrodens. Rev. Infect. Dis. 1991, 13, 1207–1212. [Google Scholar] [CrossRef] [PubMed]
- Zijlstra, E.E.; Swart, G.R.; Godfroy, F.J.M.; Degener, J.E. Pericarditis, pneumonia and brain abscess due to a combined Actinomyces-Actinobacillus actinomycetemcomitans infection. J. Infect. 1992, 25, 83–87. [Google Scholar] [CrossRef]
- Abe, S.; Ishihara, K.; Adachi, M.; Okuda, K. Oral hygiene evaluation for effective oral care in preventing pneumonia in dentate elderly. Arch. Gerontol. Geriatr. 2006, 43, 53–64. [Google Scholar] [CrossRef] [PubMed]
- Russell, S.L.; Boylan, R.J.; Kaslick, R.S.; Scannapieco, F.A.; Katz, R.V. Respiratory pathogen colonization of the dental plaque of institutionalized elders. Spec. Care Dent. 1999, 19, 128–134. [Google Scholar] [CrossRef]



{kind=link}
{kind=link}
| Periodontal Treatment Group (N = 49,400) | Comparison Group (N = 49,400) | ||||
|---|---|---|---|---|---|
| n | % | n | % | p-Value | |
| Age | <0.001 | ||||
| 20–39 | 20,500 | 41.5 | 21,279 | 43.1 | |
| 40–64 | 23,838 | 48.3 | 23,295 | 47.2 | |
| ≥65 | 5062 | 10.2 | 4826 | 9.8 | |
| Mean ± SD | 44.25 ± 14.82 | 44.15 ± 14.5 | 0.283 | ||
| Gender | 0.049 | ||||
| Female | 26,242 | 53.1 | 26,551 | 53.7 | |
| Male | 23,158 | 46.9 | 22,849 | 46.3 | |
| Monthly income | 0.007 | ||||
| <NT $20,000 | 24,560 | 49.7 | 25,021 | 50.6 | |
| NT $20,000–NT $40,000 | 17,660 | 35.7 | 17,444 | 35.3 | |
| >NT $40,000 | 7180 | 14.5 | 6935 | 14.0 | |
| Urbanization | 0.797 | ||||
| Urban | 31,674 | 64.1 | 31,750 | 64.3 | |
| Suburban | 14,381 | 29.1 | 14,352 | 29.1 | |
| Rural | 3345 | 6.8 | 3298 | 6.7 | |
| Hypertension | 5761 | 11.7 | 5505 | 11.1 | 0.010 |
| Hyperlipidemia | 1997 | 4.0 | 1973 | 4.0 | 0.697 |
| Diabetes | 2651 | 5.4 | 2527 | 5.1 | 0.077 |
| Chronic obstructive pulmonary disease | 1367 | 2.8 | 1326 | 2.7 | 0.423 |
| Chronic kidney disease | 214 | 0.4 | 233 | 0.5 | 0.368 |
| Stroke | 887 | 1.8 | 872 | 1.8 | 0.718 |
| No. of Event | Observed Person-Years | ID | Crude HR | 95% CI | Adjusted HR † | 95% CI | |
|---|---|---|---|---|---|---|---|
| Group | |||||||
| Comparison | 2,504 | 366,251 | 6.8 | 1 | 1 | ||
| Periodontal treatment | 1922 | 378,522 | 5.1 | 0.74 | 0.70–0.78 | 0.69 | 0.65–0.73 |
| Age | |||||||
| 20–39 | 703 | 325,108 | 2.2 | 1 | 1 | ||
| 40–64 | 1889 | 351,970 | 5.4 | 2.51 | 2.30–2.73 | 2.28 | 2.09–2.50 |
| ≥65 | 1834 | 67,695 | 27.1 | 12.95 | 11.87–14.13 | 7.98 | 7.24–8.79 |
| Gender | |||||||
| Female | 1800 | 400,036 | 4.5 | 1 | 1 | ||
| Male | 2626 | 344,737 | 7.6 | 1.70 | 1.60–1.80 | 1.60 | 1.51–1.71 |
| Monthly income | |||||||
| <NT $20,000 | 2508 | 373,501 | 6.7 | 1 | 1 | ||
| NT $20,000–NT $40,000 | 1558 | 262,588 | 5.9 | 0.89 | 0.83–0.94 | 0.91 | 0.85–0.97 |
| >NT $40,000 | 360 | 108,685 | 3.3 | 0.49 | 0.44–0.55 | 0.65 | 0.58–0.73 |
| Urbanization | |||||||
| Urban | 2589 | 478,277 | 5.4 | 1 | 1 | ||
| Suburban | 1390 | 216,786 | 6.4 | 1.18 | 1.11–1.26 | 1.05 | 0.98–1.12 |
| Rural | 447 | 49,710 | 9.0 | 1.66 | 1.50–1.84 | 1.18 | 1.07–1.31 |
| Hypertension | 1403 | 76,450 | 18.4 | 4.18 | 3.93–4.46 | 1.42 | 1.31–1.53 |
| Hyperlipidemia | 360 | 25,386 | 14.2 | 2.63 | 2.36–2.92 | 0.95 | 0.85–1.07 |
| Diabetes | 729 | 34,065 | 21.4 | 4.27 | 3.94–4.62 | 1.78 | 1.63–1.94 |
| Chronic obstructive pulmonary disease | 431 | 19,815 | 21.8 | 3.95 | 3.57–4.36 | 1.77 | 1.6–1.96 |
| Chronic kidney disease | 103 | 2577 | 40.0 | 7.25 | 5.96–8.82 | 2.69 | 2.21–3.28 |
| Stroke | 361 | 11,462 | 31.5 | 5.88 | 5.28–6.55 | 1.74 | 1.55–1.95 |
| Periodontal Treatment Group (N = 49,400) | Comparison Group (N = 49,400) | p-Value | |
|---|---|---|---|
| Follow-up duration (years) | 7.66 ± 3.05 | 7.41 ± 3.14 | <0.001 |
| Time to event (years), N = 4426 | 5.34 ± 3.07 | 5.16 ± 3.01 | 0.057 |
| N | No. of Event | Crude HR | 95% CI | Adjusted HR † | 95% CI | |
|---|---|---|---|---|---|---|
| Periodontal treatment | ||||||
| None | 49,400 | 2504 | 1 | 1 | ||
| Scaling | 44,253 | 1783 | 0.74 | 0.7–0.79 | 0.70 | 0.66–0.75 |
| Root planing | 4380 | 128 | 0.76 | 0.64–0.91 | 0.58 | 0.48–0.69 |
| Flap surgery | 767 | 11 | 0.35 | 0.19–0.63 | 0.34 | 0.19–0.62 |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Yang, L.-C.; Suen, Y.-J.; Wang, Y.-H.; Lin, T.-C.; Yu, H.-C.; Chang, Y.-C. The Association of Periodontal Treatment and Decreased Pneumonia: A Nationwide Population-Based Cohort Study. Int. J. Environ. Res. Public Health 2020, 17, 356. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph17010356
Yang L-C, Suen Y-J, Wang Y-H, Lin T-C, Yu H-C, Chang Y-C. The Association of Periodontal Treatment and Decreased Pneumonia: A Nationwide Population-Based Cohort Study. International Journal of Environmental Research and Public Health. 2020; 17(1):356. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph17010356
Chicago/Turabian StyleYang, Li-Chiu, Yih-Jane Suen, Yu-Hsun Wang, Tai-Chen Lin, Hui-Chieh Yu, and Yu-Chao Chang. 2020. "The Association of Periodontal Treatment and Decreased Pneumonia: A Nationwide Population-Based Cohort Study" International Journal of Environmental Research and Public Health 17, no. 1: 356. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph17010356