Tripartite Data Analysis for Optimizing Telemedicine Operations: Evidence from Guizhou Province in China



Abstract
:1. Introduction
2. Literature Reviews
3. Methods
3.1. Game Theory in Health
3.2. Evolutionary Game Theory and ESS
3.3. Data Collection
4. Tripartite Evolutionary Game Model of Stakeholders in Telemedicine
4.1. The Hypothesis of the Tripartite Evolutionary Game Model
4.2. Payoff Matrix of the tripartite Evolutionary Game in Telemedicine
5. Analysis of the Tripartite Evolutionary Game Model in Telemedicine
5.1. Replicator Dynamics Equation of the Tripartite Evolutionary Game
5.2. Replicator Dynamic Analysis of the Tripartite Evolutionary Game
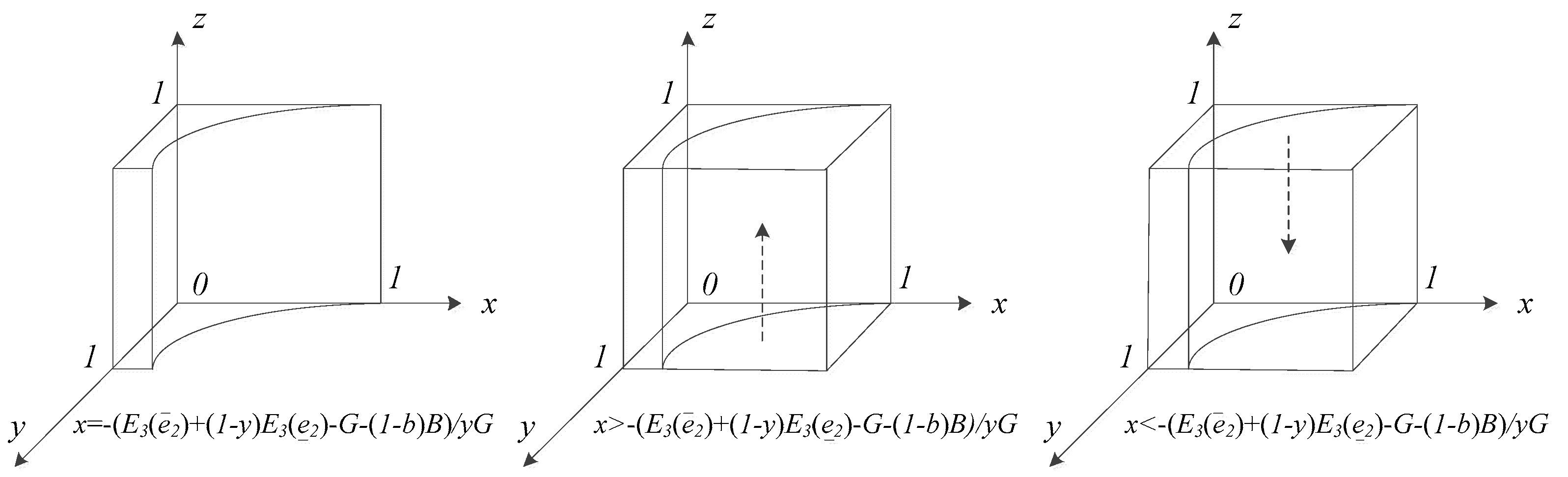
5.2.1. Replicator Dynamic Analysis of the Patient Group
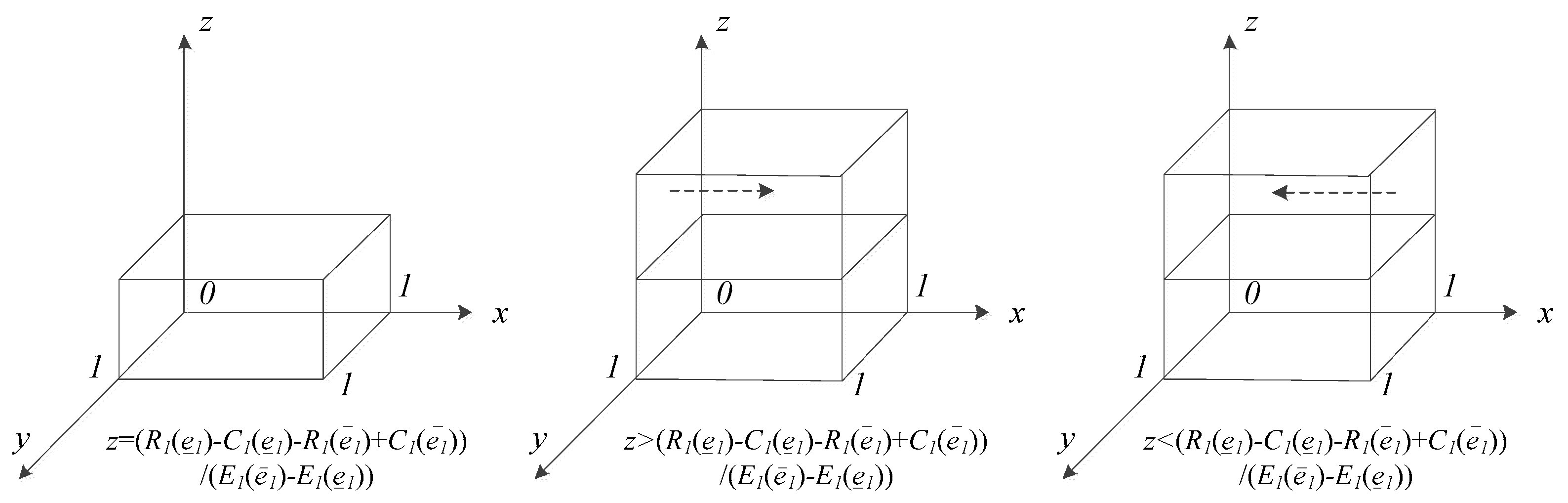
5.2.2. Replicator Dynamic Analysis of PMIs
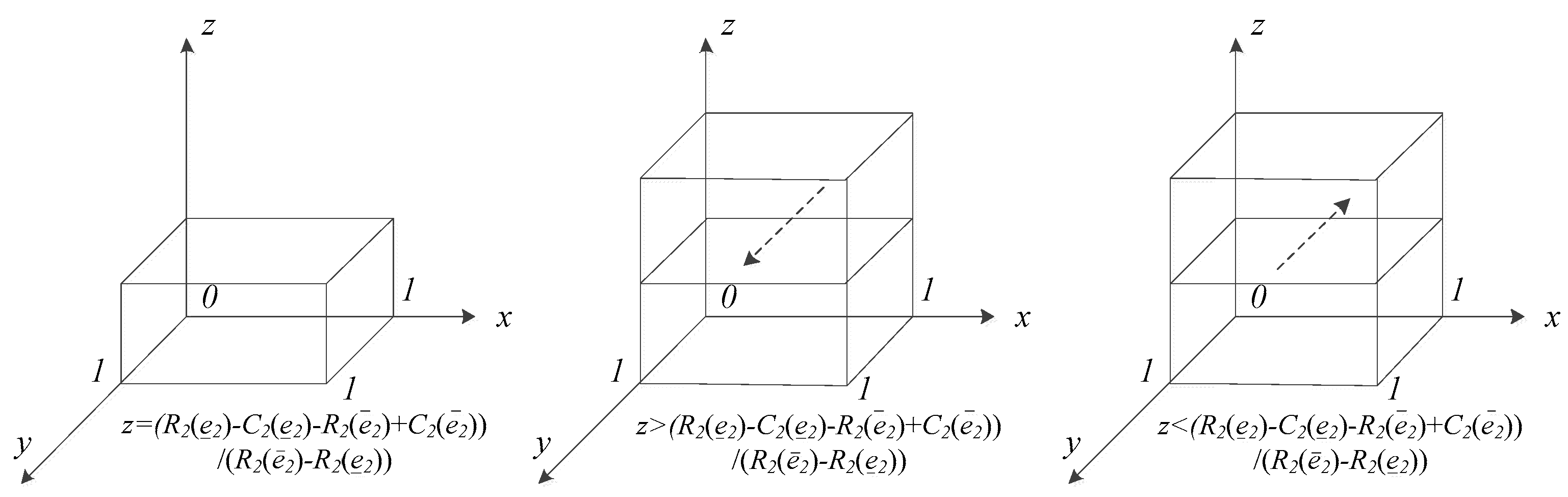
5.2.3. Replicator Dynamics Analysis of HMIs
5.3. Stability Analysis of the Local Equilibrium Points (EPs)
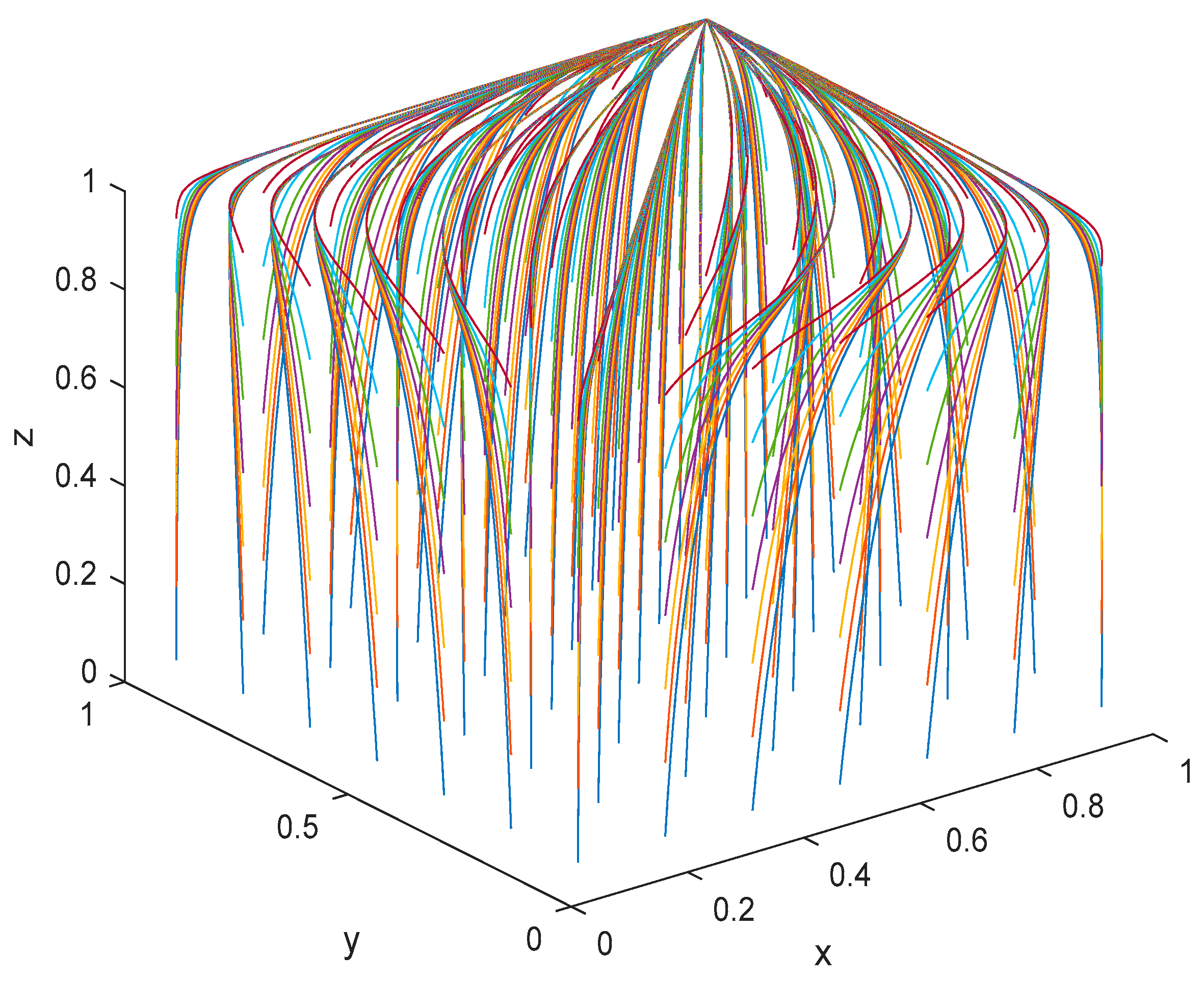
6. Simulation Analysis
6.1. Change in the Initial Intention of the Strategy Combination (‘HMI Efforts’, ‘PMI Efforts’, ‘Patients’ Acceptance’)
6.1.1. Scenario
6.1.2. Scenario
6.1.3. Scenario
6.2. Change in Telemedicine Fees for Patients
6.3. Change in the Reimbursement Ratio of Telemedicine Fees
6.3.1. Telemedicine Services Are Embedded in Social Medical Insurance Reimbursements
6.3.2. Telemedicine Services Are Not Embedded in Medical Insurance Reimbursements
7. The Telemedicine Service of Guizhou Province
7.1. The Price Reform of Telemedicine in Guizhou
7.2. The Reimbursement Ratio of Telemedicine in Guizhou
7.3. The Initial Probability of (‘HMI Efforts’, ‘PMI Efforts’, ‘Patients’ Acceptance’) in Guizhou
8. Discussion
9. Conclusions
Author Contributions
Funding
Conflicts of Interest
Abbreviations
| ESS | evolutionarily stability strategies |
| EP | equilibrium point |
| MI | medical institution |
| HMI | higher medical institution |
| PMI | primary medical institution |
| TAM | technology acceptance model |
| TPB | theory of planned behaviour |
References
- Wang, Z.; Gu, H. A review of telemedicine in China. J. Telemed. Telecare 2009, 15, 23–27. [Google Scholar] [CrossRef]
- AlDossary, S.; Martin-Khan, M.G.; Bradford, N.K.; Smith, A.C. A systematic review of the methodologies used to evaluate telemedicine service initiatives in hospital facilities. Int. J. Med. Inform. 2017, 97, 171–194. [Google Scholar] [CrossRef] [Green Version]
- Fatehi, F.; Wootton, R. Telemedicine, telehealth or e-health? A bibliometric analysis of the trends in the use of these terms. J. Telemed. Telsecare 2012, 18, 460–464. [Google Scholar] [CrossRef] [PubMed]
- Kvedar, J.; Coye, M.J.; Everett, W. Connected Health: A Review of Technologies and Strategies to Improve Patient Care with Telemedicine and Telehealth. Health Aff. 2014, 33, 194–199. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kiberu, V.M.; Scott, R.E.; Mars, M. Assessing core, e-learning, clinical and technology readiness to integrate telemedicine at public health facilities in Uganda: A health facility—based survey. BMC Health Serv. Res. 2019, 19, 266. [Google Scholar] [CrossRef]
- Mars, M. Telemedicine and Advances in Urban and Rural Healthcare Delivery in Africa. Prog. Cardiovasc. Dis. 2013, 56, 326–335. [Google Scholar] [CrossRef] [PubMed]
- Chau, P.Y.K.; Hu, P.J.-H. Investigating healthcare professionals’ decisions to accept telemedicine technology: An empirical test of competing theories. Inform. Manag. 2002, 39, 297–311. [Google Scholar] [CrossRef]
- Adenuga, K.L.; Iahad, N.A.; Miskon, S. Towards reinforcing telemedicine adoption amongst clinicians in Nigeria. Int. J. Med. Inform. 2017, 104, 84–96. [Google Scholar] [CrossRef] [PubMed]
- Adler-Milstein, J.; Kvedar, J.; Bates, D.W. Telehealth Among US Hospitals: Several Factors, Including State Reimbursement and Licensure Policies, Influence Adoption. Health Aff. 2014, 33, 207–215. [Google Scholar] [CrossRef]
- Greenhalgh, T.; Procter, R.; Wherton, J.; Sugarhood, P.; Hinder, S.; Rouncefield, M. What is quality in assisted living technology? The ARCHIE framework for effective telehealth and telecare services. BMC Med. 2015, 13, 91. [Google Scholar] [CrossRef] [Green Version]
- Liu, J.J. Pervasive Telemonitoring for Patients Living with Chronic Heart Failure: A Quantitative Study of Telemedicine; ProQuest LLC (UMI): Ann Arbor, MI, USA, 2009. [Google Scholar]
- Gorst, S.L.; Armitage, C.J.; Brownsell, S.; Hawley, M.S. Home telehealth uptake and continued use among heart failure and chronic obstructive pulmonary disease patients: A systematic review. Ann. Behav. Med. 2014, 48, 323–336. [Google Scholar] [CrossRef] [Green Version]
- Domingo, M.; Lupón, J.; González, B.; Crespo, E.; López, R.; Ramos, A.; Urrutia, A.; Pera, G.; Verdú, J.M.; Bayes-Genis, A. Evaluation of a telemedicine system for heart failure patients: Feasibility, acceptance rate, satisfaction and changes in patient behavior: Results from the CARME (CAtalan Remote Management Evaluation) study. Eur. J. Cardiovasc. Nurs. 2011, 11, 410–418. [Google Scholar] [CrossRef] [PubMed]
- Jue, J.; Spector, S.; Spector, S. Telemedicine broadening access to care for complex cases. J. Surg. Res. 2017, 220, 164–170. [Google Scholar] [CrossRef] [PubMed]
- Tarraga Marcos, M.L.; Panisello Royo, J.M.; Carbayo-Herencia, J.A.; Rosich Domenech, N.; Alins Presas, J.; Castell Panisello, E.; Tárraga López, P.J. Application of telemedicine in obesity management. Eur. Res. Telemed. 2017, 6, 3–12. [Google Scholar] [CrossRef]
- Sherwood, B.G.; Han, Y.; Nepple, K.G.; Erickson, B.A. Evaluating the Effectiveness, Efficiency and Safety of Telemedicine for Urological Care in the Male Prisoner Population. Urol. Pract. 2018, 5, 44–51. [Google Scholar] [CrossRef] [PubMed]
- Dullet, N.W.; Geraghty, E.M.; Kaufman, T.; Kissee, J.L.; King, J.; Dharmar, M.; Smith, A.C.; Marcin, J.P. Impact of a University-Based Outpatient Telemedicine Program on Time Savings, Travel Costs, and Environmental Pollutants. Value Health 2017, 20, 542–546. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Parajuli, R.; Doneys, P. Exploring the role of telemedicine in improving access to healthcare services by women and girls in rural Nepal. Telemat. Inform. 2017, 34, 1166–1176. [Google Scholar] [CrossRef]
- Henderson, C.; Knapp, M.; Fernández, J.-L.; Beecham, J.; Hirani, S.P.; Cartwright, M.; Rixon, L.; Beynon, M.; Rogers, A.; Bower, P.; et al. Cost effectiveness of telehealth for patients with long term conditions (Whole Systems Demonstrator telehealth questionnaire study): Nested economic evaluation in a pragmatic, cluster randomised controlled trial. BMJ Br. Med. J. 2013, 346, f1035. [Google Scholar] [CrossRef] [Green Version]
- Klaassen, B.; van Beijnum, B.J.F.; Hermens, H.J. Usability in telemedicine systems—A literature survey. Int. J. Med. Inform. 2016, 93, 57–69. [Google Scholar] [CrossRef]
- Tanimoto, J. Fundamentals of Evolutionary Game Theory and its Applications; Springer: Tokyo, Japan, 2015. [Google Scholar]
- Tarrant, C.; Stokes, T.; Colman, A.M. Models of the medical consultation: Opportunities and limitations of a game theory perspective. Qual. Saf. Health Care 2004, 13, 461–466. [Google Scholar] [CrossRef] [Green Version]
- Blake, A.; Carroll, B. Game theory and strategy in medical training. Med. Educ. 2016, 50, 1094–1106. [Google Scholar] [CrossRef] [PubMed]
- Dasgupta, A.; Buckingham, N.; Gračanin, D.; Handosa, M.; Tasooji, R. A Mixed Reality Based Social Interactions Testbed: A Game Theory Approach. In Virtual, Augmented and Mixed Reality: Applications in Health, Cultural Heritage, and Industry; Chen, J., Fragomeni, G., Eds.; VAMR 2018; Lecture Notes in Computer Science; Springer: Cham, Switzerland, 2018; Volume 10910. [Google Scholar]
- Kumar, K.; Jindal, A.; Rodrigues, J.J.P.C. Providing healthcare services on-the-fly using multi-player cooperation game theory in Internet of Vhiclees (IoV) environment. Digit. Commun. Netw. 2015, 1, 191–2013. [Google Scholar] [CrossRef] [Green Version]
- Weibull, J.W. Evolutionary Game Theory; MIT Press: Cambridge, MA, USA, 1995. [Google Scholar]
- Javarone, M.A. Statistical Physics and Computational Methods for Evolutionary Game Theory; Springer: Cham, Switzerland, 2018. [Google Scholar]
- Maynard Smith, J. Evolution and the theory of games: In situations characterized by conflict of interest, the best strategy to adopt depends on what others are doing. Am. Sci. 1976, 64, 41–45. [Google Scholar]
- Zeeman, E.C. Population dynamics from game theory. In Lecture Notes in Mathematics; Springer: Berlin, Germany, 1980; Volume 819. [Google Scholar]
- Friedman, D. On economic applications of evolutionary game theory. J. Evol. Econ. 1998, 8, 15–43. [Google Scholar] [CrossRef] [Green Version]
- Selten, R. A note on evolutionarily stable strategies in asymmetric animal conflicts. J. Theor. Biol. 1980, 84, 93–101. [Google Scholar] [CrossRef] [Green Version]
- Rho, M.J.; Kim, H.S.; Chung, K.; Choi, I.Y. Factors influencing the acceptance of telemedicine for diabetes management. Clust. Comput. 2015, 18, 321–331. [Google Scholar] [CrossRef]
- Kohnke, A.; Cole, M.; Bush, R.; Ellis, M.; Hagan, M.; Cruz, J. Incorporating UTAUT Predictors for Understanding Home Care Patients’ and Clinician’s Acceptance of Healthcare Telemedicine Equipment. J. Technol. Manag. Innov. 2014, 9, 29–41. [Google Scholar] [CrossRef] [Green Version]
- Hofmann-Wellenhof, R.; Salmhofer, W.; Binder, B.; Okcu, A.; Kerl, H.; Soyer, H.P. Feasibility and acceptance of telemedicine for wound care in patients with chronic leg ulcers. J. Telemed. Telecare 2006, 12, 15–17. [Google Scholar] [CrossRef]







{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| HMIs | ||||||
|---|---|---|---|---|---|---|
| PMIs | ||||||
| Patients | ||||||
| Acceptance () | ||||||
| Non-acceptance () | ||||||
| 0 | 0 | 0 | 0 | |||
| EP | Eigenvalue | ||
|---|---|---|---|
| EP | Scenario 1 Costs Are More Than Revenue | Scenario 2 Costs Are Less Than Revenue | ||
|---|---|---|---|---|
| Eigenvalue Symbol | Stability | Eigenvalue Symbol | Stability | |
| Stable point | Unstable point | |||
| Saddle point | Saddle point | |||
| Saddle point | Saddle point | |||
| Saddle point | Saddle point | |||
| Saddle point | Saddle point | |||
| Saddle point | Saddle point | |||
| Saddle point | Saddle point | |||
| Unstable point | Stable point | |||
| Items | Unit | Price Ceiling (Yuan) | ||
|---|---|---|---|---|
| National Level | Provincial Level | Municipal/City Level | ||
| Tele-consultation | Hour | 1550 | 700 | 595 |
| Traditional Chinese Medical (TCM) tele-diagnosis and tele-consultation | Hour | 1550 | 700 | 595 |
| Synchronized tele-pathological consultation | Per visit | 500 | 400 | 340 |
| Asynchronized tele-pathological consultation | Per visit | 400 | 300 | 255 |
| Remote imaging conference | Per visit | 400 | 200 | 170 |
| Items | Unit | Price Ceiling (Yuan) | ||
|---|---|---|---|---|
| National Level | Provincial Level | Municipal/City Level | ||
| Unidisciplinary tele-consultation | Per visit | Not exceed 100 per visit | 100 for chief physician | 100 for chief physician |
| Not exceed 80 per visit | 80 for associate chief physician | 80 for associate chief physician | ||
| Multidisciplinary tele-consultation | Hour | 1200 | 320 | 270 |
| TCM tele-diagnosis and tele-consultation | Hour | 1200 | 320 | 270 |
| Synchronized tele-pathological consultation | Per visit | 300 | 180 | 150 |
| Asynchronized tele-pathological consultation | Per visit | 300 | 140 | 120 |
| Remote electrocardiogram (ECG) diagnosis | Per visit | The price is charged according to the current medical price of the inviting party of the ECG project in Guizhou Province | ||
| Remote imaging diagnosis | Per visit | |||
| Remote laboratory diagnosis | Per visit | |||
| Telepathological diagnosis | Per visit | |||
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Yu, J.; Zhang, T.; Liu, Z.; Hatab, A.A.; Lan, J. Tripartite Data Analysis for Optimizing Telemedicine Operations: Evidence from Guizhou Province in China. Int. J. Environ. Res. Public Health 2020, 17, 375. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph17010375
Yu J, Zhang T, Liu Z, Hatab AA, Lan J. Tripartite Data Analysis for Optimizing Telemedicine Operations: Evidence from Guizhou Province in China. International Journal of Environmental Research and Public Health. 2020; 17(1):375. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph17010375
Chicago/Turabian StyleYu, Jinna, Tingting Zhang, Zhen Liu, Assem Abu Hatab, and Jing Lan. 2020. "Tripartite Data Analysis for Optimizing Telemedicine Operations: Evidence from Guizhou Province in China" International Journal of Environmental Research and Public Health 17, no. 1: 375. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph17010375