The Impact of the Chronic Disease Self-Management Program on Health Literacy: A Pre-Post Study Using a Multi-Dimensional Health Literacy Instrument

 , ,
, ,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Setting
2.2. Intervention
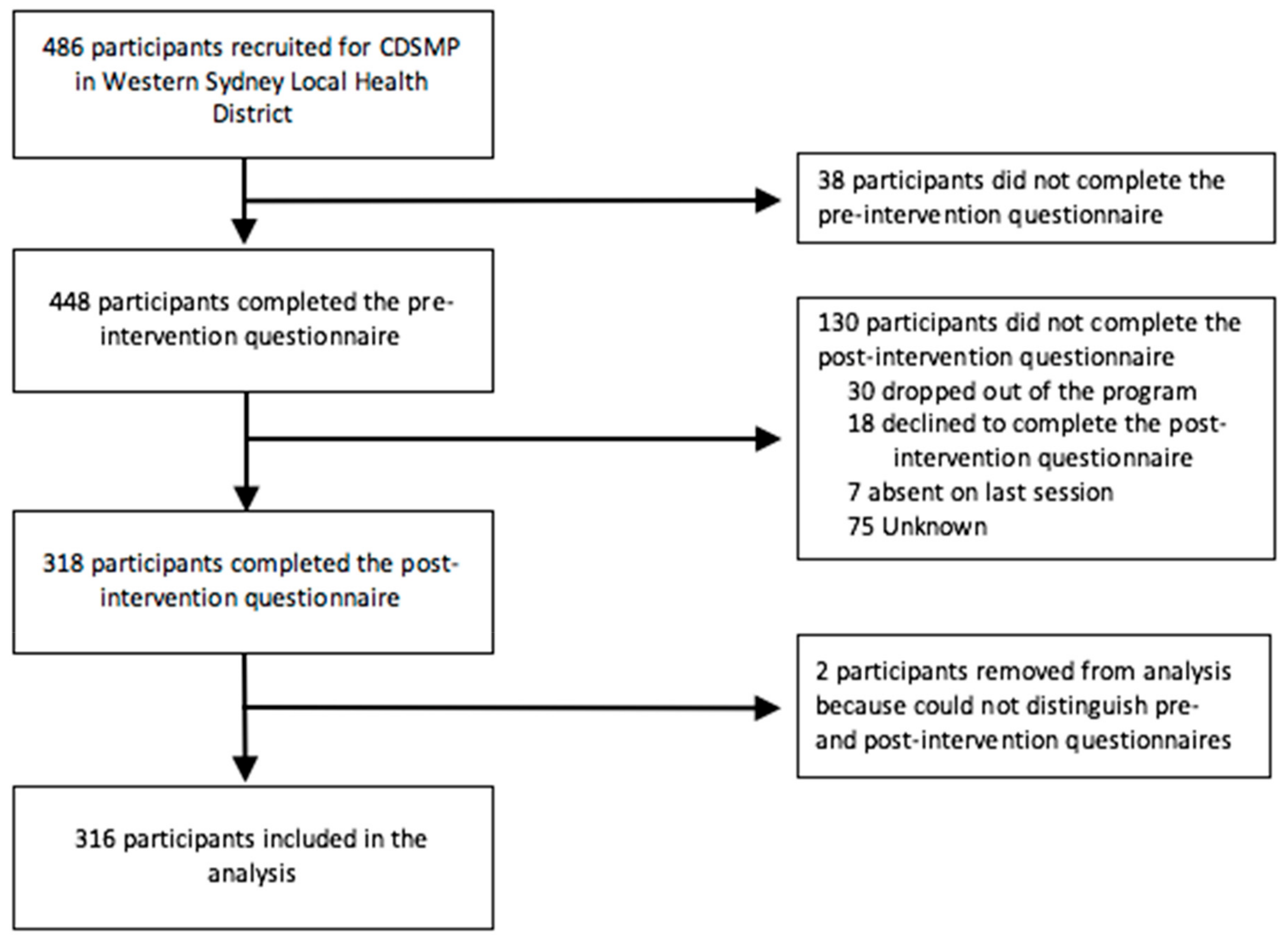
2.3. Participants and Recruitment
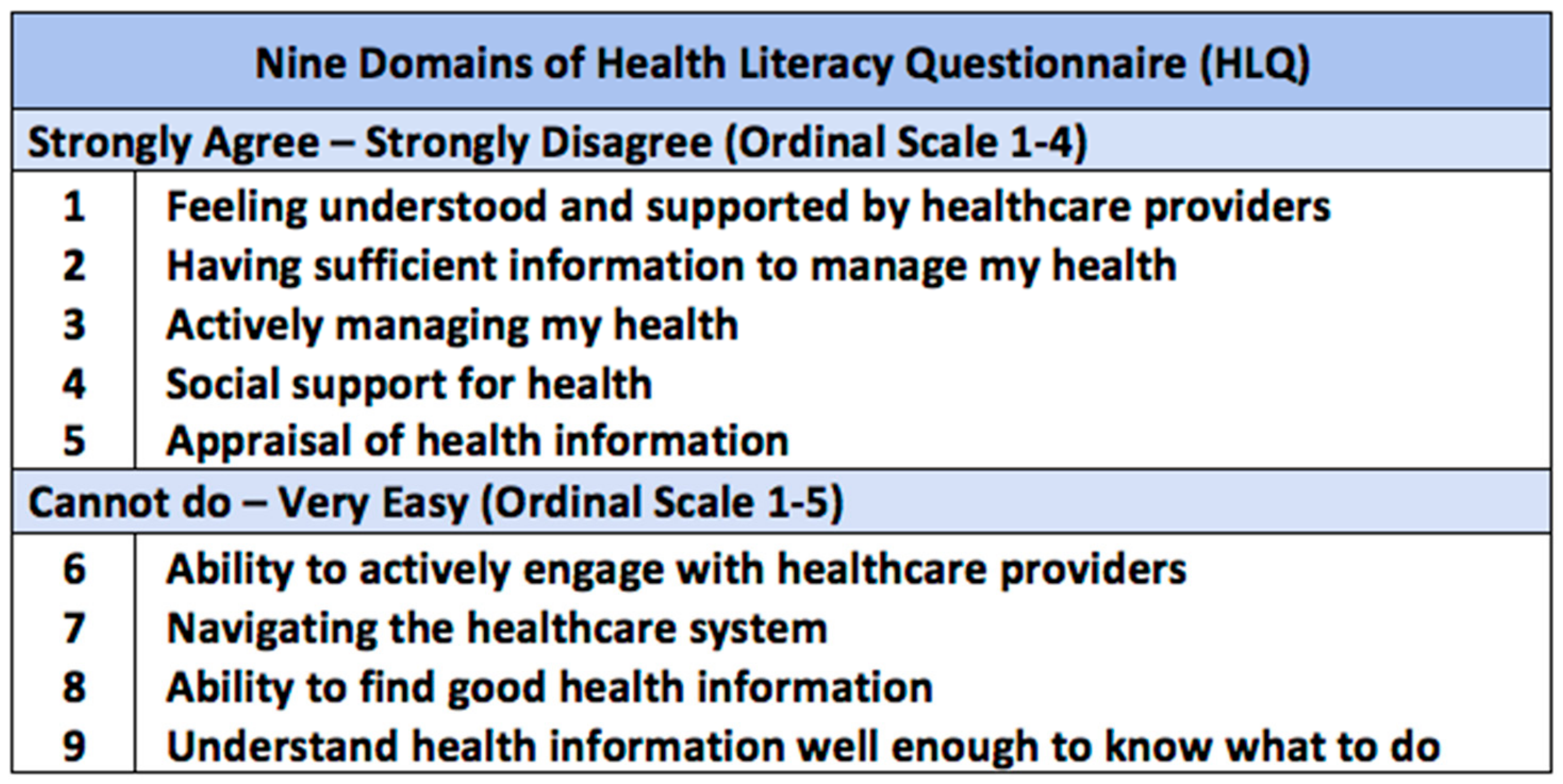
2.4. Outcome Measures
2.5. Statistical Analysis
2.6. Ethics
3. Results
3.1. Demographic Characteristics
3.2. Health Literacy
4. Discussion
5. Conclusions
Author Contributions
Funding
Conflicts of Interest
Appendix A

{kind=link}
{kind=link}
{kind=link}
| Characteristics | Completed n (%) | Not Completed n (%) | Χ2 (P) |
|---|---|---|---|
| Number of participants | 316 | 132 | |
| Age (years) | |||
| <50 | 12 (3.8%) | 11 (8.3%) | 6.97 (0.14) |
| 50–59 | 39 (12.3%) | 15 (11.4%) | |
| 60–69 | 123 (38.9%) | 46 (34.8%) | |
| 70–79 | 104 (32.9%) | 34 (25.8%) | |
| ≥80 | 29 (9.1%) | 17 (12.9%) | |
| Gender | |||
| Female | 196 (62.0%) | 84 (63.6%) | 0.09 (0.76) |
| Male | 115 (36.4%) | 45 (34.1%) | |
| Live Alone | |||
| Yes | 56 (17.7%) | 27 (20.5%) | 0.28 (0.59) |
| No | 235 (74.4%) | 95 (72.0%) | |
| Country of Birth | |||
| Australia | 51 (16.1%) | 36 (27.3%) | 54.85 (<0.001) |
| Mainland China | 78 (24.7%) | 40 (30.3%) | |
| India | 71 (22.5%) | 21 (15.9%) | |
| Hong Kong | 34 (10.8%) | 1 (0.8%) | |
| Turkey | 33 (10.4%) | 1 (0.8%) | |
| Sri Lanka | 25 (7.9%) | 3 (2.3%) | |
| Other | 19 (6.0 %) | 26 (19.7%) | |
| English Spoken at Home | |||
| Yes | 88 (27.8%) | 63 (47.7%) | 17.01 (<0.001) |
| No | 222 (70.3%) | 64 (48.5%) | |
| Education Level | |||
| Primary School or Less | 32 (10.1%) | 15 (11.4%) | 11.03 (0.05) |
| High School (not completed) | 38 (12.0%) | 20 (15.2%) | |
| High School (completed) | 66 (20.9%) | 14 (10.6%) | |
| TAFE/Trade | 42 (13.3%) | 17 (12.9%) | |
| Undergraduate | 87 (27.5%) | 38 (28.8%) | |
| Postgraduate | 17 (5.4%) | 15 (11.4%) | |
| Employment Status | |||
| Working / Studying | 14 (4.4%) | 9 (6.8%) | 1.51 (0.83) |
| Home duties | 39 (12.3%) | 14 (10.6%) | |
| Retired | 148 (46.8%) | 67 (50.8%) | |
| Permanently unable to work / Ill | 10 (3.2%) | 4 (3.0%) | |
| Other | 17 (5.4%) | 6 (4.5%) | |
| Self-reported Illness | |||
| Arthritis | 120 (38.0%) | 54 (40.9%) | 7.63 (0.27) |
| Diabetes | 94 (29.7%) | 37 (28.0%) | |
| Back pain | 92 (29.1%) | 42 (31.8%) | |
| Heart problems | 86 (27.2%) | 40 (30.3%) | |
| Depression / Anxiety | 68 (21.5%) | 25 (18.9%) | |
| Other | 146 (46.8%) | 58 (43.9%) | |
| None | 14 (4.4%) | 15 (11.4%) | |
| Private Health Insurance | |||
| Yes | 108 (34.2%) | 31 (23.5%) | 4.36 (0.04) |
| No | 185 (58.5%) | 90 (68.2%) | |
| Healthcare Card | |||
| Yes | 230 (72.7%) | 92 (69.7%) | 0.65 (0.42) |
| No | 59 (18.7%) | 30 (22.7%) | |
| Attended Hospital Emergency in the Past 12 Months | |||
| Yes | 65 (20.6%) | 28 (21.2%) | 0.02 (0.89) |
| No | 164 (51.9%) | 76 (57.6%) | |
| Teaching Group | |||
| Arabic | 6 (1.9%) | 3 (2.3%) | 75.59 (<0.001) |
| ATSI | 26 (8.2%) | 21 (15.9%) | |
| Australian and NZ | 4 (1.3%) | 4 (3.0%) | |
| Chinese (Cantonese) | 57 (18.0%) | 8 (6.1%) | |
| Chinese (Mandarin) | 54 (17.1%) | 33 (25.0%) | |
| Chinese (Traditional) | 9 (2.8%) | 3 (2.3%) | |
| English | 22 (7.0%) | 14 (10.6%) | |
| Filipino (Tagalong) | 1 (0.3%) | 16 (12.1%) | |
| Hindi | 63 (19.9%) | 14 (10.6%) | |
| Indian (English) | 12 (3.8%) | 9 (6.8%) | |
| Multicultural | 4 (1.3%) | 1 (0.8%) | |
| Tamil | 25 (7.9%) | 5 (3.8%) | |
| Turkish | 33 (10.4%) | 1 (0.8%) | |
| Required Help with Questionnaire | |||
| Yes | 46 (14.6%) | 21 (15.9%) | 0.04 (0.84) |
| No | 247 (78.2%) | 102 (77.3%) | |
Appendix B
| HLQ Domain | Completers’ Mean Score (SD) | Non-completers’ Mean Score (SD) | Mean Difference | P-value |
|---|---|---|---|---|
| 1. Feeling understood and supported by healthcare providers | 11.95 (2.23) | 12.18 (1.75) | 0.23 | 0.25 |
| 2. Having sufficient information to manage my health | 11.17 (2.31) | 11.28 (2.32) | 0.11 | 0.65 |
| 3. Actively managing my health | 15.06 (2.53) | 15.14 (2.25) | 0.08 | 0.73 |
| 4. Social support for health | 14.70 (2.75) | 14.83 (2.44) | 0.13 | 0.62 |
| 5. Appraisal of health information | 14.51 (2.33) | 14.64 (2.27) | 0.12 | 0.60 |
| 6. Ability to actively engage with healthcare providers | 17.36 (4.03) | 18.05 (3.86) | 0.68 | 0.09 |
| 7. Navigating the healthcare system | 19.87 (4.84) | 20.89 (4.84) | 1.02 | 0.04 |
| 8. Ability to find good health information | 16.39 (4.01) | 17.23 (3.88) | 0.85 | 0.04 |
| 9. Understand health information well enough to know what to do | 17.16 (3.93) | 17.94 (4.16) | 0.78 | 0.07 |
Appendix C
| Mean Score Change (SD) | |||||||||
|---|---|---|---|---|---|---|---|---|---|
| Characteristics | Domain 1: Healthcare provider support | Domain 2: Having Sufficient Information | Domain 3: Actively Managing Health | Domain 4: Social Support for Health | Domain 5: Active Appraisal of Health Information | Domain 6: Active Engagement with Healthcare | Domain 7: Navigating the Health Care System | Domain 8: Ability to Find Good Health Information | Domain 9: Understanding Health Information |
| Age group | P = 0.32 | P = 0.06 | P = 0.002 | P = 0.52 | P = 0.40 | P = 0.93 | P = 0.75 | P = 0.62 | P = 0.49 |
| <50 | 1.17 (1.64) | 2.33 (2.46) | 2.83 (2.82) | 0.25 (1.86) | 2.58 (2.31) | 0.75 (2.67) | 3.58 (3.87) | 2.50 (1.78) | 1.00 (2.17) |
| 50–59 | 0.69 (3.04) | 1.74 (3.32) | 2.05 (2.93) | 1.23 (3.39) | 1.46 (3.43) | 2.33 (4.66) | 2.69 (5.42) | 2.10 (4.38) | 1.72 (4.68) |
| 60–69 | 0.83 (2.15) | 1.43 (2.38) | 1.41 (2.38) | 1.12 (2.86) | 1.40 (2.65) | 1.45 (3.68) | 2.39 (4.50) | 2.33 (3.94) | 2.10 (3.75) |
| 70–79 | 0.55 (1.73) | 0.90 (2.14) | 0.43 (2.30) | 0.45 (2.42) | 0.66 (2.10) | 1.09 (3.32) | 2.07 (4.18) | 1.66 (3.36) | 0.96 (3.03) |
| ≥80 | 0.14 (2.49) | 0.38 (2.64) | 0.38 (3.20) | 0.34 (3.32) | 0.72 (3.36) | 1.28 (4.67) | 2.34 (6.63) | 0.97 (4.69) | 0.69 (4.50) |
| Gender | P = 0.85 | P = 0.33 | P = 0.84 | P = 0.47 | P = 0.05 | P = 0.46 | P = 0.67 | P = 0.82 | P = 0.27 |
| Female | 0.62 (2.16) | 1.15 (2.36) | 1.09 (2.39) | 0.76 (2.55) | 0.91 (2.50) | 1.38 (3.62) | 2.23 (4.32) | 1.83 (3.62) | 1.20 (3.46) |
| Male | 0.76 (2.21) | 1.41 (2.70) | 1.20 (2.93) | 0.98 (3.24) | 1.55 (2.91) | 1.44 (4.03) | 2.56 (5.33) | 2.17 (4.20) | 2.03 (4.05) |
| Live Alone | P = 0.03 | P = 0.94 | P = 0.21 | P = 0.15 | P = 0.50 | P = 0.84 | P = 0.24 | P = 0.05 | P = 0.49 |
| Yes | 1.12 (1.96) | 1.61 (2.23) | 1.30 (2.71) | 1.12 (2.91) | 1.25 (2.55) | 1.61 (3.96) | 3.16 (5.15) | 2.59 (3.20) | 1.88 (3.90) |
| No | 0.46 (2.12) | 1.03 (2.49) | 0.93 (2.44) | 0.63 (2.68) | 0.98 (2.57) | 1.30 (3.66) | 2.08 (4.54) | 1.68 (3.84) | 1.33 (3.51) |
| Country of Birth | N/A a | ||||||||
| Australia | 0.75 (2.24) | 1.96 (2.79) | 1.61 (2.55) | 0.86 (3.23) | 1.41 (2.88) | 1.35 (4.42) | 2.31 (5.67) | 2.37 (4.58) | 1.51 (3.95) |
| Mainland China | 0.22 (2.11) | 0.21 (2.52) | 0.47 (2.44) | 0.13 (2.42) | 0.29 (2.60) | 1.17 (3.96) | 1.71 (4.67) | 1.04 (4.04) | 0.26 (3.87) |
| India | 0.97 (2.40) | 1.87 (2.60) | 1.04 (3.01) | 1.14 (3.17) | 1.31 (3.00) | 2.07 (4.09) | 3.59 (5.16) | 3.17 (3.99) | 2.69 (4.24) |
| Hong Kong | 0.29 (2.22) | 0.88 (2.07) | 1.41 (2.20) | 0.62 (2.81) | 1.65 (2.62) | 1.56 (3.64) | 2.21 (3.90) | 1.94 (3.50) | 1.88 (3.04) |
| Turkey | 1.58 (1.89) | 2.58 (1.56) | 2.45 (2.03) | 1.85 (2.41) | 2.30 (1.86) | 1.21 (1.39) | 2.42 (2.97) | 1.91 (2.14) | 1.70 (2.58) |
| Sri Lanka | 0.76 (1.27) | 1.00 (1.50) | 0.76 (1.90) | 1.04 (2.05) | 1.08 (2.20) | −0.28 (2.59) | 0.52 (2.65) | 0.84 (2.53) | 0.80 (2.06) |
| Other | 0.68 (1.86) | 0.47 (1.84) | 1.00 (2.85) | 1.05 (2.63) | 0.95 (1.93) | 2.84 (3.66) | 3.68 (5.22) | 2.37 (3.35) | 2.63 (3.55) |
| English Spoken at Home | P = 0.996 | P = 0.68 | P = 0.52 | P = 0.36 | P = 0.50 | P = 0.19 | P = 0.28 | P = 0.14 | P = 0.85 |
| Yes | 0.76 (2.08) | 1.72 (2.47) | 1.20 (2.44) | 0.72 (2.82) | 1.32 (2.55) | 1.17 (3.98) | 2.28 (4.83) | 2.20 (4.05) | 1.57 (3.48) |
| No | 0.59 (2.08) | 1.02 (2.36) | 1.05 (2.50) | 0.80 (2.67) | 1.02 (2.56) | 1.40 (3.49) | 2.25 (4.45) | 1.78 (3.53) | 1.41 (3.61) |
| Education Level | P = 0.63 | P = 0.54 | P = 0.59 | P = 0.43 | P = 0.95 | P = 0.27 | P = 0.31 | P = 0.30 | P = 0.03 |
| Primary School or less | 0.59 (2.21) | 1.53 (2.93) | 1.31 (2.78) | 0.38 (3.44) | 1.06 (3.22) | 2.19 (4.79) | 3.72 (5.65) | 2.56 (4.19) | 2.91 (3.73) |
| High School (not completed) | 1.32 (2.59) | 1.97 (2.33) | 1.71 (1.84) | 1.58 (2.66) | 1.50 (2.30) | 1.71 (3.85) | 2.37 (4.96) | 2.95 (3.57) | 1.84 (3.61) |
| High School (completed) | 0.74 (2.23) | 1.26 (2.54) | 1.00 (2.98) | 0.55 (2.93) | 1.00 (2.73) | 1.38 (4.01) | 3.08 (4.65) | 1.67 (4.05) | 1.76 (4.12) |
| TAFE/Trade | 0.21 (2.32) | 0.57 (2.31) | 0.45 (2.70) | 0.57 (2.86) | 0.81 (2.96) | 1.24 (3.61) | 1.83 (5.06) | 1.24 (4.15) | 0.31 (3.22) |
| Undergraduate | 0.48 (2.03) | 0.94 (2.57) | 1.11 (2.67) | 0.75 (2.62) | 1.08 (2.65) | 1.26 (3.77) | 1.92 (4.65) | 1.85 (3.90) | 1.14 (3.75) |
| Postgraduate | 0.65 (1.73) | 1.00 (1.62) | 0.47 (1.70) | 0.88 (2.50) | 1.53 (2.40) | 0.00 (2.81) | 1.35 (3.32) | 1.71 (3.26) | 1.35 (2.83) |
| Employment | P = 0.77 | P = 0.59 | P = 0.29 | P = 0.33 | P = 0.60 | P = 0.06 | P = 0.23 | P = 0.12 | P = 0.23 |
| Working / Studying | 0.29 (2.30) | 0.93 (2.06) | 0.64 (2.82) | 0.29 (2.61) | 0.86 (2.71) | 0.93 (3.15) | 1.71 (3.41) | 0.71 (2.55) | 1.29 (2.05) |
| Home duties | 0.10 (2.43) | 0.38 (2.32) | 1.05 (2.09) | 0.38 (2.68) | 0.41 (2.59) | 0.69 (3.04) | 1.18 (3.97) | 0.79 (3.78) | 0.67 (3.03) |
| Retired | 0.65 (2.04) | 1.03 (2.53) | 0.91 (2.46) | 0.79 (2.70) | 1.03 (2.71) | 1.09 (3.80) | 2.03 (4.70) | 1.72 (3.90) | 1.11 (3.58) |
| Ill / Permanently unable to work | 0.80 (3.68) | 1.30 (1.83) | 1.30 (2.71) | 2.10 (3.38) | 1.10 (2.64) | 3.40 (4.33) | 3.00 (3.06) | 2.70 (2.63) | 2.70 (4.42) |
| Other | 0.88 (1.17) | 1.88 (2.37) | 2.29 (2.87) | 0.06 (2.19) | 2.12 (2.06) | 1.53 (3.79) | 2.94 (5.51) | 2.53 (4.47) | 1.47 (3.22) |
| Chronic Disease | |||||||||
| Arthritis | P = 0.87 | P = 0.53 | P = 0.29 | P = 0.07 | P = 0.16 | P = 0.10 | P = 0.003 | P = 0.07 | P = 0.13 |
| 0.66 (2.29) | 1.25 (2.64) | 1.07 (2.45) | 1.08 (2.84) | 1.05 (2.61) | 1.88 (4.21) | 3.04 (5.07) | 2.33 (4.17) | 1.75 (3.70) | |
| Diabetes | P = 0.10 | P = 0.68 | P = 0.46 | P = 0.11 | P = 0.91 | P = 0.59 | P = 0.65 | P = 0.91 | P = 0.26 |
| 0.49 (2.21) | 1.36 (2.70) | 1.31 (2.85) | 0.60 (2.87) | 1.33 (2.80) | 1.18 (4.06) | 2.13 (5.12) | 2.22 (4.07) | 1.67 (3.91) | |
| Back pain | P = 0.85 | P = 0.30 | P = 0.41 | P = 0.16 | P = 0.50 | P = 0.11 | P = 0.05 | P = 0.86 | P = 0.85 |
| 0.80 (2.16) | 1.55 (2.43) | 1.46 (2.52) | 1.18 (2.93) | 1.22 (2.46) | 2.26 (4.24) | 3.55 (5.67) | 2.39 (4.39) | 1.82 (3.65) | |
| Heart problems | P = 0.12 | P = 0.75 | P = 0.0005 | P = 0.08 | P = 0.03 | P = 0.86 | P = 0.26 | P = 0.65 | P = 0.43 |
| 0.86 (2.13) | 1.31 (2.56) | 1.65 (2.39) | 1.31 (2.63) | 1.56 (2.87) | 1.72 (4.26) | 2.79 (4.51) | 2.14 (3.73) | 1.83 (3.25) | |
| Depression / Anxiety | P = 0.88 | P = 0.90 | P = 0.53 | P = 0.64 | P = 0.74 | P = 0.62 | P = 0.75 | P = 0.73 | P = 0.28 |
| 0.91 (2.36) | 1.69 (2.80) | 1.87 (2.32) | 1.21 (3.07) | 1.41 (2.52) | 1.75 (4.17) | 3.28 (5.51) | 2.51 (4.09) | 1.91 (3.64) | |
| Other | P = 0.30 | P = 0.93 | P = 0.87 | P = 0.76 | P = 0.69 | P = 0.26 | P = 0.41 | P = 0.36 | P = 0.72 |
| 0.83 (2.00) | 1.38 (2.56) | 1.20 (2.44) | 0.80 (2.81) | 1.18(2.57) | 1.52(3.85) | 2.53(4.78) | 1.89(3.98) | 1.63(3.62) | |
| Private Health Insurance | P = 0.46 | P = 0.82 | P = 0.86 | P = 0.93 | P = 0.70 | P = 0.62 | P = 0.11 | P = 0.02 | P = 0.27 |
| Yes | 0.47 (2.10) | 1.11 (2.45) | 1.11 (2.47) | 0.59 (2.66) | 1.06 (2.67) | 1.15 (3.65) | 1.98 (4.37) | 2.13 (3.55) | 1.37 (3.43) |
| No | 0.80 (2.22) | 1.36 (2.49) | 1.14 (2.63) | 0.96 (2.87) | 1.19 (2.65) | 1.57 (3.93) | 2.64 (4.98) | 1.91 (4.07) | 1.66 (3.88) |
| Healthcare Card | P = 0.06 | P = 0.11 | P = 0.75 | P = 0.02 | P = 0.08 | P = 0.40 | P = 0.48 | P = 0.53 | P = 0.82 |
| Yes | 0.56 (2.12) | 1.10 (2.50) | 1.08 (2.46) | 0.63 (2.66) | 0.94 (2.59) | 1.29 (3.74) | 2.30 (4.50) | 1.86 (3.78) | 1.36 (3.53) |
| No | 0.92 (2.10) | 1.56 (2.25) | 0.98 (2.32) | 1.27 (2.72) | 1.47 (2.39) | 1.88 (3.33) | 2.64 (4.24) | 2.20 (3.30) | 2.19 (3.43) |
| Attended Hospital Emergency in the Past 12 Months | P = 0.67 | P = 0.29 | P = 0.96 | P = 0.69 | P = 0.23 | P = 0.86 | P = 0.60 | P = 0.90 | P = 0.998 |
| Yes | 0.62 (2.24) | 0.94 (2.57) | 1.22 (2.61) | 0.51 (2.94) | 0.95 (2.90) | 1.22 (4.12) | 2.49 (5.11) | 1.78 (4.11) | 1.45 (3.67) |
| No | 0.54 (2.12) | 1.06 (2.39) | 1.00 (2.37) | 0.73 (2.64) | 1.06 (2.50) | 1.21 (3.48) | 1.91 (4.34) | 1.70 (3.68) | 1.17 (3.31) |
| Help with Questionnaire | P = 0.65 | P = 0.08 | P = 0.50 | P = 0.77 | P = 0.13 | P = 0.33 | P = 0.06 | P = 0.98 | P = 0.43 |
| Yes | 1.02 (2.56) | 2.04 (3.20) | 1.39 (3.09) | 0.96 (3.63) | 1.59 (3.24) | 1.17 (4.55) | 2.70 (5.94) | 2.54 (4.73) | 1.93 (4.41) |
| No | 0.60 (2.13) | 1.09 (2.34) | 1.06 (2.48) | 0.78 (2.63) | 1.02 (2.56) | 1.51 (3.70) | 2.39 (4.53) | 1.92 (3.73) | 1.49 (3.62) |
| Teaching Group | P = 0.47 | P = 0.04 | P = 0.14 | P = 0.30 | P = 0.04 | P = 0.53 | P = 0.004 | P = 0.21 | P = 0.02 |
| Arabic | 1.17 (2.23) | 1.00 (2.10) | 1.33 (2.07) | 2.67 (2.80) | 1.33 (1.86) | 3.67 (1.86) | 2.83 (3.19) | 3.67 (2.34) | 3.17 (2.40) |
| ATSI | 1.12 (2.14) | 2.77 (2.42) | 1.96 (2.92) | 0.96 (2.90) | 2.31 (2.53) | 2.04 (3.55) | 3.69 (5.03) | 3.81 (3.81) | 2.50 (3.47) |
| Australian and NZ † | 0.00 (0.82) | 0.50 (1.00) | 0.50 (1.00) | 0.25 (1.71) | 0.00 (0.00) | −0.50 (2.08) | −2.25 (2.22) | −1.25 (2.75) | −1.50 (1.29) |
| Chinese (Cantonese) | 0.51 (2.11) | 0.65 (2.04) | 1.49 (2.15) | 0.63 (2.60) | 1.33 (2.43) | 1.74 (3.83) | 2.84 (4.34) | 2.14 (3.50) | 2.00 (3.12) |
| Chinese (Mandarin) | 0.04 (2.08) | 0.20 (2.64) | 0.11 (2.47) | 0.06 (2.39) | 0.13 (2.60) | 1.35 (4.09) | 1.74 (4.87) | 1.00 (4.09) | 0.15 (4.03) |
| Chinese (Traditional) | 0.11 (1.96) | −0.11 (2.15) | 1.00 (2.96) | 0.11 (2.26) | 0.33 (3.28) | −0.56 (3.40) | −1.33 (3.74) | −0.33 (4.36) | −1.78 (2.39) |
| English | 0.45 (2.52) | 1.27 (3.15) | 1.50 (2.26) | 0.95 (3.81) | 0.55 (3.17) | 0.82 (5.43) | 1.50 (6.28) | 1.14 (5.03) | 0.73 (4.31) |
| Filipino (Tagalong) b | 0.00 (0.00) | −1.00 (0.00) | −2.00 (0.00) | −3.00 (0.00) | 2.00 (0.00) | 0.00 (0.00) | −1.00 (0.00) | −3.00 (0.00) | −1.00 (0.00) |
| Hindi | 0.90 (2.49) | 1.94 (2.71) | 1.05 (3.11) | 1.08 (3.33) | 1.27 (3.12) | 2.27 (4.27) | 3.97 (5.44) | 3.44 (4.10) | 3.17 (4.48) |
| Indian (English) | 0.83 (1.80) | 1.33 (2.46) | 0.33 (2.64) | 1.08 (2.39) | 1.00 (2.00) | 1.25 (2.80) | 1.50 (2.28) | 1.33 (3.11) | 0.67 (2.87) |
| Multicultural † | 0.75 (1.50) | 1.00 (2.00) | 1.00 (0.82) | 0.00 (0.00) | 1.00 (2.00) | 1.00 (2.00) | 2.25 (2.06) | 2.25 (1.50) | 1.75 (2.22) |
| Tamil | 0.48 (1.73) | 0.88 (1.79) | 0.40 (2.25) | 0.88 (2.40) | 1.08 (2.33) | −0.36 (2.66) | 0.24 (2.71) | 0.48 (2.71) | 0.76 (2.30) |
| Turkish | 1.58 (1.89) | 2.58 (1.56) | 2.45 (2.03) | 1.85 (2.41) | 2.30 (1.86) | 1.21 (1.39) | 2.42 (2.97) | 1.91 (2.14) | 1.70 (2.58) |
References
- Institute for Health Metrics and Evaluation (IHME). Global Burden of Disease Study 2016 (GBD 2016) Results; IHME: Seattle, WA, USA, 2017. [Google Scholar]
- Australian Institute of Health and Welfare (AIHW). Australia’s Health 2018; AIHW: Canberra, Australia, 2018. [Google Scholar]
- Holman, H. Chronic disease—The need for a new clinical education. JAMA 2004, 292, 1057–1059. [Google Scholar] [CrossRef] [PubMed]
- Pimouguet, C.; Le Goff, M.; Thiébaut, R.; Dartigues, J.; Helmer, C. Effectiveness of disease-management programs for improving diabetes care: A meta-analysis. Can. Med. Assoc. J. 2011, 183, E115–E127. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Siantz, E.; Aranda, M.P. Chronic disease self-management interventions for adults with serious mental illness: A systematic review of the literature. Gen. Hosp. Psychiatry 2014, 36, 233–244. [Google Scholar] [CrossRef] [PubMed]
- Nolte, S.; Elsworth, G.; Newman, S.; Osborne, R. Measurement issues in the evaluation of chronic disease self-management programs. Qual. Life Res. 2013, 22, 1655–1664. [Google Scholar] [CrossRef]
- Nutbeam, D. Health promotion glossary. Health Promot. Int. 1998, 13, 349–364. [Google Scholar] [CrossRef]
- Glasgow, N.J.; Jeon, Y.-H.; Kraus, S.G.; Pearce-Brown, C.L. Chronic disease self-management support: The way forward for Australia. Med. J. Aust. 2008, 189, S14–S16. [Google Scholar] [CrossRef]
- Jordan, J.E.; Briggs, A.M.; Brand, C.A.; Osborne, R.H. Enhancing patient engagement in chronic disease self-management support initiatives in Australia: The need for an integrated approach. Med. J. Aust. 2008, 189, S9–S13. [Google Scholar] [CrossRef] [Green Version]
- van Der Heide, I.; Poureslami, I.; Mitic, W.; Shum, J.; Rootman, I.; Fitzgerald, J.M. Health literacy in chronic disease management: A matter of interaction. J. Clin. Epidemiol. 2018, 102, 134–138. [Google Scholar] [CrossRef]
- Nguyen, T.H.; Paasche-Orlow, M.K.; McCormack, L.A. The state of the science of health literacy measurement. Stud. Health Technol. Inform. 2017, 240, 17–33. [Google Scholar] [CrossRef] [Green Version]
- Jordan, J.E.; Buchbinder, R.; Osborne, R.H. Conceptualising health literacy from the patient perspective. Patient Educ. Couns. 2010, 79, 36–42. [Google Scholar] [CrossRef]
- Osborne, R.; Batterham, R.; Elsworth, G.; Hawkins, M.; Buchbinder, R. The grounded psychometric development and initial validation of the Health Literacy Questionnaire (HLQ). BMC Public Health 2013, 13, 658–675. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Sørensen, K.; Van Den Broucke, S.; Pelikan, J.; Fullam, J.; Doyle, G.; Slonska, Z.; Kondilis, B.; Stoffels, V.; Osborne, R.; Brand, H. Measuring health literacy in populations: Illuminating the design and development process of the European Health Literacy Survey Questionnaire (HLS-EU-Q). BMC Public Health 2013, 13, 948. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Western Sydney Local Health District (WSLHD). Western Sydney Local Health District Year in Review 2017-18; WSLHD: Wentworthville, NSW, Australia, 2018. [Google Scholar]
- Western Sydney Primary Health Network (WSPHN) and Western Sydney Local Health District (WSLHD). The New Frontier of Healthcare: Western Sydney Integrated Care Demonstrator 2014-2017; WSLHD & WSPHN: Sydney, Australia, 2018. [Google Scholar]
- Lorig, R.K.; Ritter, L.P.; Stewart, S.A.; Sobel, M.D.; William-Brown, D.B.; Bandura, R.A.; Gonzalez, R.V.; Laurent, R.D.; Holman, R.H. Chronic Disease Self-Management Program: 2-Year health status and health care utilization outcomes. Med. Care 2001, 39, 1217–1223. [Google Scholar] [CrossRef] [PubMed]
- Kennedy, A.; Reeves, D.; Bower, P.; Lee, V.; Middleton, E.; Richardson, G.; Gardner, C.; Gately, C.; Rogers, A. The effectiveness and cost effectiveness of a national lay-led self care support programme for patients with long-term conditions: A pragmatic randomised controlled trial. J Epidemiol. Community Health 2007, 61, 254–261. [Google Scholar] [CrossRef] [PubMed]
- Jonker, A.A.; Comijs, H.C.; Knipscheer, K.C.; Deeg, D.J. Promotion of self-management in vulnerable older people: A narrative literature review of outcomes of the Chronic Disease Self-Management Program (CDSMP). Eur. J. Ageing 2009, 6, 303–314. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Dongbo, F.; Ding, Y.; McGowan, P.; Fu, H. Qualitative evaluation of Chronic Disease Self Management Program (CDSMP) in Shanghai. Patient Educ. Couns. 2006, 61, 389–396. [Google Scholar] [CrossRef] [PubMed]
- Walker, C.; Weeks, A.; McAvoy, B.; Demetriou, E. Exploring the role of self-management programmes in caring for people from culturally and linguistically diverse backgrounds in Melbourne, Australia. Health Expect. 2005, 8, 315–323. [Google Scholar] [CrossRef] [PubMed]
- Detaille, S.; Heerkens, Y.; Engels, J.; Gulden, J.; Dijk, F. Effect evaluation of a self-management program for dutch workers with a chronic somatic disease: A randomized controlled trial. J. Occup. Rehabil. 2013, 23, 189–199. [Google Scholar] [CrossRef]
- Haslbeck, J.; Zanoni, S.; Hartung, U.; Klein, M.; Gabriel, E.; Eicher, M.; Schulz, P.J. Introducing the chronic disease self-management program in Switzerland and other German-speaking countries: Findings of a cross-border adaptation using a multiple-methods approach. BMC Health Serv. Res. 2015, 15, 576. [Google Scholar] [CrossRef] [Green Version]
- Lorig, K.R.; Sobel, D.S.; Ritter, P.L.; Laurent, D.; Hobbs, M. Effect of a self-management program on patients with chronic disease. Eff. Clin. Pract. 2001, 4, 256–262. [Google Scholar]
- Swerissen, H.; Belfrage, J.; Weeks, A.; Jordan, L.; Walker, C.; Furler, J.; McAvoy, B.; Carter, M.; Peterson, C. A randomised control trial of a self-management program for people with a chronic illness from Vietnamese, Chinese, Italian and Greek backgrounds. Patient Educ. Couns. 2006, 64, 360–368. [Google Scholar] [CrossRef] [PubMed]
- Jerant, A.; Moore-Hill, M.; Franks, P. Home-based, peer-led chronic illness self-management training: Findings from a 1-year randomized controlled trial. Ann. Fam. Med. 2009, 7, 319–327. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Cheng, F.; Xu, Q.; Dai, X.-D.; Yang, L.-L. Evaluation of the Expert Patient Program in a chinese population with permanent colostomy. Cancer Nurs. 2012, 35, E27–E33. [Google Scholar] [CrossRef] [PubMed]
- Hevey, D.; Wilson O’Raghallaigh, J.; O’Doherty, V.; Lonergan, K. Pre-post effectiveness evaluation of Chronic Disease Self-Management Program (CDSMP) participation on health, well-being and health service utilization. Chronic Illness 2018. [Google Scholar] [CrossRef]
- Lorig, R.K.; Sobel, S.D.; Stewart, L.A.; Brown, W.B.; Bandura, M.A.; Ritter, D.P.; Gonzalez, R.V.; Laurent, R.D.; Holman, R.H. Evidence suggesting that a chronic disease self-management program can improve health status while reducing hospitalization: A randomized trial. Med. Care 1999, 37, 5–14. [Google Scholar] [CrossRef]
- Lorig, K.; Ritter, P.; Pifer, C.; Werner, P. Effectiveness of the Chronic Disease Self-Management Program for persons with a serious mental illness: A translation study. Community Ment. Health J. 2014, 50, 96–103. [Google Scholar] [CrossRef]
- Ory, M.G.; Ahn, S.; Jiang, L.; Smith, M.L.; Ritter, P.L.; Whitelaw, N.; Lorig, K. Successes of a national study of the chronic disease self-management program: Meeting the triple aim of health care reform. Med. Care 2013, 51, 992–998. [Google Scholar] [CrossRef]
- Wilson, P.M.; Kendall, S.; Brooks, F. The Expert Patients Programme: A paradox of patient empowerment and medical dominance. Health Soc. Care Community 2007, 15, 426–438. [Google Scholar] [CrossRef] [Green Version]
- Johnston, S.; Irving, H.; Mill, K.; Rowan, M.; Liddy, C. The patient’s voice: An exploratory study of the impact of a group self-management support program. BMC Fam. Pract. 2012, 13, 65. [Google Scholar] [CrossRef] [Green Version]
- Ammerlaan, J.; van Os-Medendorp, H.; Scholtus, L.; de Vos, A.; Zwier, M.; Bijlsma, H.; Kruize, A.A. Feasibility of an online and a face-to-face version of a self-management program for young adults with a rheumatic disease: Experiences of young adults and peer leaders. Pediatr. Rheumatol. Online J. 2014, 12, 10. [Google Scholar] [CrossRef] [Green Version]
- Jessup, R.; Osborne, R.; Beauchamp, A.; Bourne, A.; Buchbinder, R. Health literacy of recently hospitalised patients: A cross-sectional survey using the Health Literacy Questionnaire (HLQ). BMC Health Serv. Res. 2017, 17, 52. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Brainard, J.; Wilsher, S.H.; Salter, C.; Loke, Y.K. Methodological review: Quality of randomized controlled trials in health literacy. BMC Health Serv. Res. 2016, 16, 246. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Australian Bureau of Statistics (ABS). National Health Survey: First Results, 2017–2018; ABS: Canberra, Australia, 2018. [Google Scholar]
- Western Sydney Local Health District (WSLHD). Health Services Plan; WSLHD: Sydney, Australia, 2018. [Google Scholar]
- Dodson, S.; Beauchamp, A.; Batterham, R.W.; Osborne, R.H. Information sheet 10: About the Health Literacy Questionnaire (HLQ). In Ophelia Toolkit: A Step-by-Step Guide for Identifying and Responding to Health Literacy Needs within Local Communities. 2014. Available online: http://citeseerx.ist.psu.edu/viewdoc/download?doi=10.1.1.726 (accessed on 3 November 2019).
- Marciano, L.; Camerini, A.-L.; Schulz, P. The role of health literacy in diabetes knowledge, self-care, and glycemic control: A meta-analysis. J. Gen. Intern. Med. 2019, 34, 1007–1017. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Harris, M.; Williams, A.; Dennis, S.; Zwar, N.; Powell Davies, G. Chronic disease self-management: Implementation with and within Australian general practice. Med. J. Aust. 2008, 189, S17–S20. [Google Scholar] [CrossRef]



| Characteristics | n (%) |
|---|---|
| Age (years) | |
| <50 | 12 (3.8%) |
| 50–59 | 39 (12.3%) |
| 60–69 | 123 (38.9%) |
| 70–79 | 104 (32.9%) |
| ≥80 | 29 (9.1%) |
| No Response | 9 (2.8%) |
| Gender | |
| Female | 196 (62.0%) |
| Male | 115 (36.4%) |
| No Response | 5 (1.6%) |
| Live Alone | |
| Yes | 56 (17.7%) |
| No | 235 (74.4%) |
| No Response | 25 (7.9 %) |
| Country of Birth | |
| Australia | 51 (16.1%) |
| Mainland China | 78 (24.7%) |
| India | 71 (22.5%) |
| Hong Kong | 34 (10.8%) |
| Turkey | 33 (10.4%) |
| Sri Lanka | 25 (7.9%) |
| Other | 19 (6.0 %) |
| No Response | 5 (1.6%) |
| English Spoken at Home | |
| Yes | 88 (27.8%) |
| No | 222 (70.3%) |
| No Response | 6 (1.9%) |
| Education Level | |
| Primary School or Less | 32 (10.1%) |
| High School (not completed) | 38 (12.0%) |
| High School (completed) | 66 (20.9%) |
| TAFE/Trade | 42 (13.3%) |
| Undergraduate | 87 (27.5%) |
| Postgraduate | 17 (5.4%) |
| No Response | 34 (10.8%) |
| Employment | |
| Working / Studying | 14 (4.4%) |
| Home duties | 39 (12.3%) |
| Retired | 148 (46.8%) |
| Ill / Permanently unable to work | 10 (3.2%) |
| Other | 17 (5.4%) |
| No response | 88 (27.8%) |
| Illness (participants could list more than one condition) | |
| Arthritis | 120 (38.0%) |
| Diabetes | 94 (29.7%) |
| Back pain | 92 (29.1%) |
| Heart problems | 86 (27.2%) |
| Depression / Anxiety | 68 (21.5%) |
| Other | 160 (50.6%) |
| No response | 28 (8.6%) |
| Private health insurance | |
| Yes | 108 (34.2%) |
| No | 185 (58.5%) |
| No Response | 23 (7.3%) |
| Have Healthcare Card a | |
| Yes | 230 (72.7%) |
| No | 59 (18.7%) |
| No Response | 27 (8.5%) |
| Attended Hospital Emergency in the Past 12 Months | |
| Yes | 65 (20.6%) |
| No | 164 (51.9%) |
| No Response | 87 (27.5%) |
| Required help completing Questionnaire | |
| Yes | 46 (14.6%) |
| No | 247 (78.2%) |
| No Response | 23 (7.3%) |
| Teaching Group | |
| Arabic | 6 (1.9%) |
| ATSI | 26 (8.2%) |
| Australian and New Zealander | 4 (1.3%) |
| Chinese (Cantonese) | 57 (18.0%) |
| Chinese (Mandarin) | 54 (17.1%) |
| Chinese (Traditional) | 9 (2.8%) |
| English | 22 (7.0%) |
| Filipino (Tagalong) | 1 (0.3%) |
| Hindi | 63 (19.9%) |
| Indian (English) | 12 (3.8%) |
| Multicultural | 4 (1.3%) |
| Tamil | 25 (7.9%) |
| Turkish | 33 (10.4%) |
| HLQ Domain (Range) | Pre-intervention Mean (SD) | Post-intervention Mean (SD) | Mean Score Change (SD) | 95%CI | Effect Sizes |
|---|---|---|---|---|---|
| 1. Feeling understood and supported by healthcare providers (4–16) | 11.95 (2.23) | 12.62 (1.89) | 0.67 (2.16) | (0.43, 0.91) | 0.32 |
| 2. Having sufficient information to manage my health (4–16) | 11.17 (2.31) | 12.45 (2.12) | 1.28 (2.50) | (1.00, 1.55) | 0.58 |
| 3. Actively managing my health (4–20) | 15.06 (2.53) | 16.19 (2.19) | 1.13 (2.59) | (0.84, 1.42) | 0.48 |
| 4. Social support for health (4–20) | 14.70 (2.75) | 15.53 (2.45) | 0.84 (2.81) | (0.52, 1.15) | 0.32 |
| 5. Appraisal of health information (4–20) | 14.51 (2.33) | 15.67 (2.29) | 1.16 (2.66) | (0.87, 1.46) | 0.50 |
| 6. Ability to actively engage with healthcare providers (5–25) | 17.36 (4.03) | 18.79 (3.69) | 1.43 (3.76) | (1.01, 1.84) | 0.37 |
| 7. Navigating the healthcare system (6–30) | 19.87 (4.84) | 22.22 (4.55) | 2.35 (4.68) | (1.83, 2.87) | 0.50 |
| 8. Ability to find good health information (5–25) | 16.39 (4.01) | 18.37 (3.82) | 1.99 (3.83) | (1.56, 2.41) | 0.51 |
| 9. Understand health information well enough to know what to do (5–25) | 17.16 (3.93) | 18.71 (3.93) | 1.55 (3.73) | (1.14, 1.96) | 0.39 |
© 2019 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Muscat, D.M.; Song, W.; Cvejic, E.; Ting, J.H.C.; Medlin, J.; Nutbeam, D. The Impact of the Chronic Disease Self-Management Program on Health Literacy: A Pre-Post Study Using a Multi-Dimensional Health Literacy Instrument. Int. J. Environ. Res. Public Health 2020, 17, 58. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph17010058
Muscat DM, Song W, Cvejic E, Ting JHC, Medlin J, Nutbeam D. The Impact of the Chronic Disease Self-Management Program on Health Literacy: A Pre-Post Study Using a Multi-Dimensional Health Literacy Instrument. International Journal of Environmental Research and Public Health. 2020; 17(1):58. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph17010058
Chicago/Turabian StyleMuscat, Danielle Marie, Wenbo Song, Erin Cvejic, Jie Hua Cecilia Ting, Joanne Medlin, and Don Nutbeam. 2020. "The Impact of the Chronic Disease Self-Management Program on Health Literacy: A Pre-Post Study Using a Multi-Dimensional Health Literacy Instrument" International Journal of Environmental Research and Public Health 17, no. 1: 58. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph17010058