Development and Validation of the EspaiJove.net Mental Health Literacy (EMHL) Test for Spanish Adolescents

 , , , and
, , , and
Abstract
:1. Introduction
2. Materials and Methods
2.1. The EMHL Test Score
2.2. Validation of the Psychometric Properties of the EMHL Test
2.2.1. Sample
2.2.2. Main Validity Measures
2.2.3. Known-Groups Validity Assessment
2.2.4. Statistical Analysis
Reliability
Convergent Validity
3. Results
3.1. Reliability
3.2. Convergent Validity
4. Discussion
4.1. Reliability of the EMHL Test
4.2. Convergent Validity of the EMHL Test
4.3. Strengths and Limitations
5. Conclusions
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
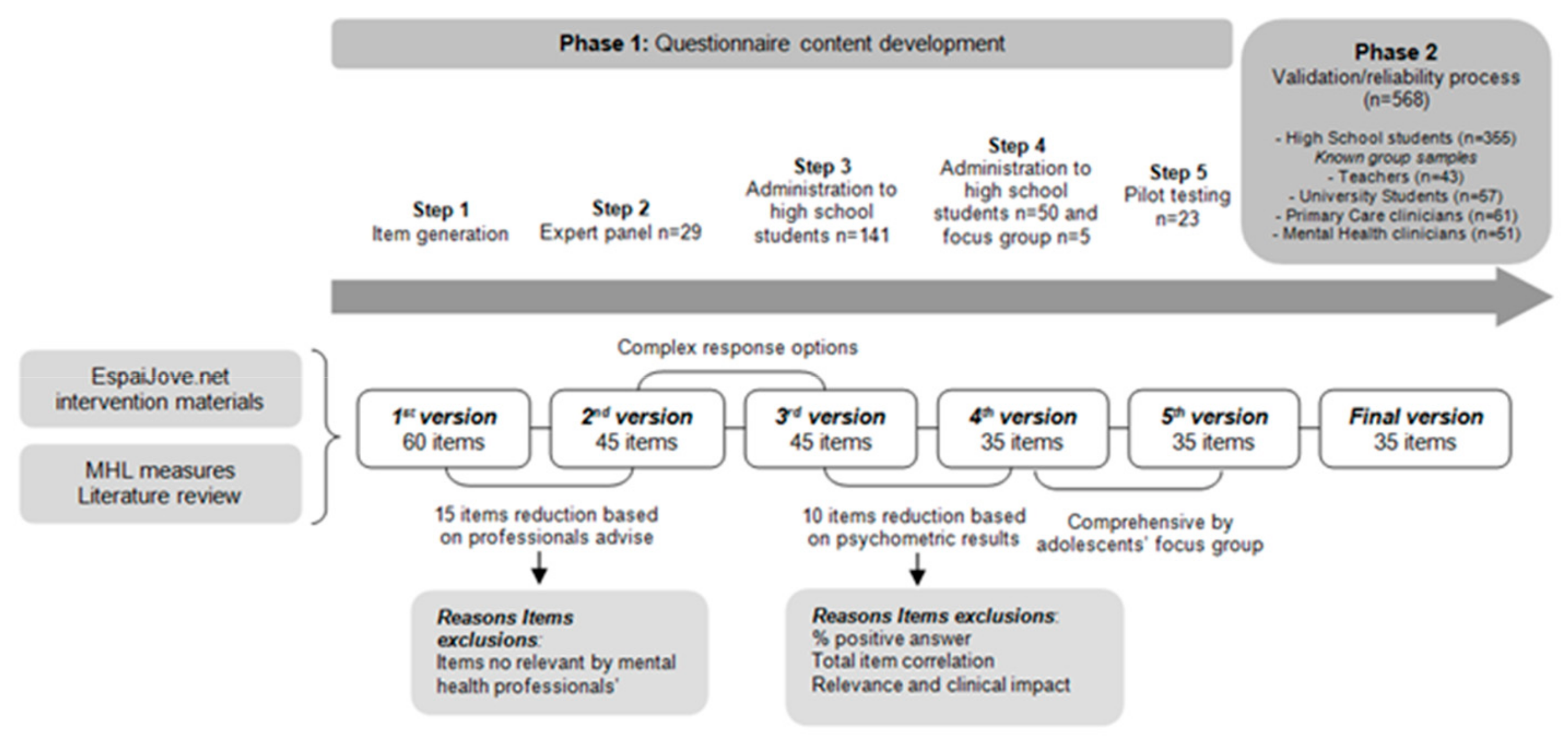
Appendix A. Phase 1: Questionnaire Content Development of the EMHL Test
- Step 1:
- Item pool generation. The first version of the EMHL test was developed from the thematic content of the EspaiJove.net program resulting in 60 items (version 1) (part 1: 15 items; part 2: 45 items). The part 1 consisted of a binary choice format (yes/no) for the recognition of mental disorders from a list of 15 different diseases (15 items), and part 2 has multiple choice questions with four possible answer options, in which only one is correct. Incorrect answers were considered as distracting items and were based on stereotypes, prejudices and erroneous statements about mental health. The distracting items were selected from focus groups held with adolescents (n = 39) and then developed by EspaiJove.net researchers and reviewed by mental health professionals.
- Step 2:
- We then conducted 6 focus groups with a total of 29 mental health professionals (expert panel) from four public child and juvenile mental health centers to explore: (i) clinical relevance; (ii) mistakes in wording (questions and answers for each item); and (iii) comprehensiveness and offensiveness. Semi-structured cognitive interviews were implemented to guide the discussions and were recorded. As a result, an initial selection of 45 items (version 2) (part 1: 15 items; part 2: 30 items) from the preliminary version 1 was developed.
- Step 3:
- The 45-item EMHL test version 2 (part 1: 15 items; part 2: 30 items) was used in five high school classrooms (n = 141) in three different public schools. The objective was to examine (i) item relevance by adolescents, (ii) its comprehensiveness and level of difficulty, (iii) its offensiveness, and (iv) the feasibility of the test (version 3).
- Step 4:
- Finally, the EMHL test was used with 3rd grade high school students (n = 50) and a focus group (n = 5) with the purpose of improving comprehensiveness and vocabulary. The last 35-item test (version 4) (part 1: 15 items; part 2: 20 items) was selected for the pilot study.
- Step 5:
- Pilot testing study. The final 35-item EMHL test version (part 1: 15 items; part 2: 20 items) was piloted among 3rd grade high school students (n = 23) to assess its comprehensiveness and vocabulary. A validation process was performed on this EMHL test version (version 5).
References
- Kessler, R.C.; Berglund, P.; Demler, O.; Jin, R.; Merikangas, K.R.; Walters, E.E. Lifetime prevalence and age-of-onset distributions of DSM-IV disorders in the National Comorbidity Survey Replication. Arch. Gen. Psychiatry 2005, 62, 593–602. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Jones, P.B. Adult mental health disorders and their age at onset. Br. J. Psychiatry 2013, 54, s5–s10. [Google Scholar] [CrossRef] [PubMed]
- Kessler, R.C.; Amminger, G.P.; Aguilar-Gaxiola, S.; Alonso, J.; Lee, S.; Ustun, T.B. Age of onset of mental disorders: A review of recent literature. Curr. Opin. Psychiatry 2007, 20, 359–364. [Google Scholar] [CrossRef] [PubMed]
- World Health Organization. Adolescent Mental Health: Mapping Actions of Nongovernmental Organizations and Other International Development Organizations. World Health Organization. Available online: https://apps.who.int/iris/handle/10665/44875 (accessed on 16 June 2012).
- Jorm, A.F. Mental health literacy: Empowering the community to take action for better mental health. Am. Psychol. 2012, 67, 231–243. [Google Scholar] [CrossRef] [Green Version]
- Zachrisson, H.D.; Rodje, K.; Mykletun, A. Utilization of health services in relation to mental health problems in adolescents: A population based survey. BMC Public Health 2006, 6, 34. [Google Scholar] [CrossRef] [Green Version]
- Birchwood, M.; Singh, S.P. Mental health services for young people: Matching the service to the need. Br. J. Psychiatry 2013, 54, s1–s2. [Google Scholar] [CrossRef] [Green Version]
- Chisholm, K.; Patterson, P.; Torgerson, C.; Turner, E.; Jenkinson, D.; Birchwood, M. Impact of contact on adolescents’ mental health literacy and stigma: The SchoolSpace cluster randomised controlled trial. BMJ Open 2016, 6, e009435. [Google Scholar] [CrossRef] [Green Version]
- Hodges, C.A.; O’Brien, M.S.; McGorry, P.D. Headspace: National Youth Mental Health Foundation: Making headway with rural young people and their mental health. Aust. J. Rural Health 2007, 15, 77–80. [Google Scholar] [CrossRef]
- Schulze, B.; Richter-Werling, M.; Matschinger, H.; Angermeyer, M.C. Crazy? So what! Effects of a school project on students’ attitudes towards people with schizophrenia. Acta Psychiatr. Scand. 2003, 107, 142–150. [Google Scholar] [CrossRef]
- Campos, L.; Dias, P.; Duarte, A.; Veiga, E.; Dias, C.C.; Palha, F. Is It Possible to “Find Space for Mental Health” in Young People? Effectiveness of a School-Based Mental Health Literacy Promotion Program. Int. J. Environ. Res. Public Health 2018, 15, 1426. [Google Scholar] [CrossRef] [Green Version]
- Casanas, R.; Arfuch, V.-M.; Castellvi, P.; Gil, J.-J.; Torres, M.; Pujol, A.; Castells, G.; Teixido, M.; San-Emeterio, M.T.; Sampietro, H.M.; et al. “EspaiJove.net”—A school-based intervention programme to promote mental health and eradicate stigma in the adolescent population: Study protocol for a cluster randomised controlled trial. BMC Public Health 2018, 18, 939. [Google Scholar] [CrossRef]
- Wei, Y.; McGrath, P.J.; Hayden, J.; Kutcher, S. Measurement properties of tools measuring mental health knowledge: A systematic review. BMC Psychiatry 2016, 16, 297. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hart, S.R.; Kastelic, E.A.; Wilcox, H.C.; Beaudry, M.B.; Musci, R.J.; Heley, K.M.; Ruble, A.E.; Swartz, K.L. Achieving Depression Literacy: The Adolescent Depression Knowledge Questionnaire (ADKQ). Sch. Ment. Health 2014, 6, 213–223. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Serra, M.; Lai, A.; Buizza, C.; Pioli, R.; Preti, A.; Masala, C.; Petretto, D.R. Beliefs and attitudes among Italian high school students toward people with severe mental disorders. J. Nerv. Ment. Dis. 2013, 201, 311–318. [Google Scholar] [CrossRef] [PubMed]
- Wei, Y.; McGrath, P.J.; Hayden, J.; Kutcher, S. Mental health literacy measures evaluating knowledge, attitudes and help-seeking: A scoping review. BMC Psychiatry 2015, 15, 291. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Abad, F.J.; García, C.; Gil, B.; Ponsoda, V.; Julio Olea Revuelta, J.J. Introducción a la Psicometría Teoría Clásica de los Tests y Teoría de la Respuesta al Ítem; Universidad autónoma de Madrid, Ed.; Universidad autónoma de Madrid: Madrid, Spain, 2016. [Google Scholar]
- Ochoa, S.; Martinez-Zambrano, F.; Vila-Badia, R.; Arenas, O.; Casas-Anguera, E.; Garcia-Morales, E.; Villellas, R.; Martin, J.R.; Perez-Franco, M.B.; Valduciel, T.; et al. Spanish validation of the social stigma scale: Community Attitudes towards Mental Illness. Rev. Psiquiatr. Salud Ment. 2016, 9, 150–157. [Google Scholar] [CrossRef]
- Evans-Lacko, S.; Rose, D.; Little, K.; Flach, C.; Rhydderch, D.; Henderson, C.; Thornicroft, G. Development and psychometric properties of the reported and intended behaviour scale (RIBS): A stigma-related behaviour measure. Epidemiol. Psychiatr. Sci. 2011, 20, 263–271. [Google Scholar] [CrossRef]
- Goodman, R. Psychometric properties of the strengths and difficulties questionnaire. J. Am. Acad. Child Adolesc. Psychiatry 2001, 40, 1337–1345. [Google Scholar] [CrossRef]
- Dolan, P. Modeling valuations for EuroQol health states. Med. Care 1997, 35, 1095–1108. [Google Scholar] [CrossRef]
- Group, T.E. EuroQol—A new facility for the measurement of health-related quality of life. Health Policy 1990, 16, 199–208. [Google Scholar]
- Badia, X.; Schiaffino, A.; Alonso, J.; Herdman, M. Using the EuroQoI 5-D in the Catalan general population: Feasibility and construct validity. Qual. Life Res. 1998, 7, 311–322. [Google Scholar] [CrossRef] [PubMed]
- Brennan, R.; Lockwood, R. A Comparison of the Nedelsky and Angoff Cutting Score Procedures Using Generalizability Theory. Appl. Psychol. Meas. 1980, 4, 219–240. [Google Scholar] [CrossRef] [Green Version]
- Traub, R.E. Book Review: A Guide to Criterion-Referenced Test Construction; Berk, R.A., Ed.; The Johns Hopkins University Press: Baltimore, MA, USA, 2007; Volume 9. [Google Scholar]
- Cronbach, L.J. Coefficient alpha and the internal structure of tests. Psychometrika 1951, 16, 297–334. [Google Scholar] [CrossRef] [Green Version]
- Cicchetti, D.V. Guidelines, Criteria, and Rules of Thumb for Evaluating Normed and Standardized Assessment Instrument in Psychology. Psychol. Assess. 1994, 6, 284–290. [Google Scholar] [CrossRef]
- Kazis, L.E.; Anderson, J.J.; Meenan, R.F. Effect sizes for interpreting changes in health status. Med. Care 1989, 27, S178–S189. [Google Scholar] [CrossRef]
- Cohen, A. Statistical Power for the Behavioral Sciences; Lawrence Eribaum, Ed.; Lawrence Eribaum: Hillsdale, NJ, USA, 1988. [Google Scholar]
- Evans, J.D. Straightforward Statistics for the Behavioral Sciences; Brooks/Cole Publishing: Pacific Grove, CA, USA, 1986. [Google Scholar]
- IBM Corp. IBM SPSS Statistics for Windows, Version 22.0; IBM Corp.: Armonk, NY, USA, 2013. [Google Scholar]
- Daltio, C.S.; Attux, C.; Ferraz, M.B. Knowledge in schizophrenia: The Portuguese version of KAST (Knowledge About Schizophrenia Test) and analysis of social-demographic and clinical factors’ influence. Schizophr. Res. 2015, 168, 168–173. [Google Scholar] [CrossRef]
- Compton, M.T.; Hankerson-Dyson, D.; Broussard, B. Development, item analysis, and initial reliability and validity of a multiple-choice knowledge of mental illnesses test for lay samples. Psychiatry Res. 2011, 189, 141–148. [Google Scholar] [CrossRef] [Green Version]
- Evans-Lacko, S.E.; Little, K.; Meltzer, H.; Rose, D.; Rhydderch, D.; Henderson, C.; Thornicroft, G. Development and psychometric properties of the Mental Health Knowledge Schedule. Can. J. Psychiatry 2010, 55, 440–448. [Google Scholar] [CrossRef] [Green Version]
- Gabriel, A.; Violato, C. The development of a knowledge test of depression and its treatment for patients suffering from non-psychotic depression: A psychometric assessment. BMC Psychiatry 2009, 9, 56. [Google Scholar] [CrossRef] [Green Version]
- Gulliver, A.; Griffiths, K.M.; Christensen, H.; Mackinnon, A.; Calear, A.L.; Parsons, A.; Bennett, K.; Batterham, P.J.; Stanimirovic, R. Internet-based interventions to promote mental health help-seeking in elite athletes: An exploratory randomized controlled trial. J. Med. Internet Res. 2012, 14, e69. [Google Scholar] [CrossRef]
- Wang, J.; He, Y.; Jiang, Q.; Cai, J.; Wang, W.; Zeng, Q.; Miao, J.; Qi, X.; Chen, J.; Bian, Q.; et al. Mental health literacy among residents in Shanghai. Shanghai Arch. Psychiatry 2013, 25, 224–235. [Google Scholar] [PubMed]
- Berk, R. A consumers’ guide to criterion-referenced test reliability. J. Educ. Meas. 1980, 17, 323–349. [Google Scholar] [CrossRef]



{kind=link}
{kind=link}
| Item | Floor N(%) | Ceiling N(%) | Item-Total Score Correlation |
|---|---|---|---|
| First part of the EMHL test | |||
| 1 (Schizophrenia) | 67(19.0) | 286(81.0) | 0.309 |
| 2 (Diabetes) | 12 (3.4) | 341 (96.6) | 0.337 |
| 3 (Phobia) | 60 (17.0) | 293 (83.0) | 0.272 |
| 4 (Asthma) | 13 (3.7) | 340 (96.3) | 0.405 |
| 5 (Bipolar disorder) | 24 (6.8) | 329 (93.2) | 0.340 |
| 6 (Bulimia) | 127 (36.0) | 226 (64.0) | 0.411 |
| 7 (Cerebral palsy) | 172 (48.7) | 181 (51.3) | 0.526 |
| 8 (Bronchitis) | 4 (1.1) | 349 (98.9) | 0.394 |
| 9 (Alzheimer disease) | 251 (71.1) | 102 (28.9) | 0.287 |
| 10 (Depression) | 38 (10.8) | 315 (89.2) | 0.374 |
| 11 (Chickenpox) | 8 (2.3) | 345 (97.7) | 0.408 |
| 12 (Down’s Syndrome) | 199 (56.4) | 154 (43.6) | 0.503 |
| 13 (Epilepsy) | 153 (43.3) | 200 (56.7) | 0.354 |
| 14 (Anorexia nervosa) | 79 (22.4) | 274 (77.6) | 0.437 |
| 15 (Substance dependence) | 85 (24.1) | 268 (75.9) | 0.162 |
| Total First Part | 2 (0.6) | 21 (5.9) | * 0.744 |
| +0.773 | |||
| Second part of the EMHL test | |||
| 1 (Definition of mental health) | 282 (79.9) | 71 (20.1) | 0.132 |
| 2 (Where to go for help) | 87 (24.6) | 266 (75.4) | −0.206 |
| 3 (Who develops a mental disorder) | 72 (20.4) | 281 (79.6) | 0.249 |
| 4 (Healthy Behaviors) | 257 (72.8) | 96 (27.2) | −0.133 |
| 5 (Night rest) | 102 (28.9) | 251 (71.1) | 0.268 |
| 6 (Cannabis / alcohol consumption) | 308 (87.3) | 45 (12.7) | 0.401 |
| 7 (Bullying) | 139 (39.4) | 214 (60.3) | 0.127 |
| 8 (Cyberbullying) | 110 (31.2) | 242 (68.6) | 0.229 |
| 9 (Social skills) | 191 (54.1) | 162 (45.9) | 0.236 |
| 10 (Suicidal ideation friend / family) | 151 (42.8) | 202 (57.2) | 0.144 |
| 11 (Self-injury) | 109 (30.9) | 244 (69.1) | 0.267 |
| 12 (Suicide Behavior Alert) | 60 (17.0) | 293 (83.0) | 0.178 |
| 13 (Depression) | 270(76.5) | 83 (23.5) | 0.407 |
| 14 (Eating Disorders) | 294 (83.3) | 59 (16.7) | 0.256 |
| 15 (Start of Eating Disorders) | 270 (76.5) | 83 (23.5) | 0.238 |
| 16 (Characteristics of Eating Disorders) | 281 (79.6) | 72 (20.4) | 0.411 |
| 17 (Symptoms Schizophrenia) | 269 (76.2) | 84 (23.8) | 0.301 |
| 18 (Delusions) | 261 (73.9) | 92 (26.1) | 0.039 |
| 19 (Psychotic episode) | 311 (88.1) | 42 (11.9) | 0.396 |
| 20 (Alcohol dependence) | 243 (68.8) | 110 (31.2) | 0.376 |
| Total Second Part | 1 (0.3) | 2 (0.6) | * 0.615 |
| +0.643 |
| Subgroups | N | Mean (SD) | Effect Size (ES) | p |
|---|---|---|---|---|
| First part of the EMHL test | ||||
| High school students (ref.) | 355 | 7.07 (4.96) | --- | <0.001 |
| Teachers | 43 | 11.56 (3.42) | 0.466 | <0.001 |
| University students | 57 | 12.44 (2.32) | 0.570 | <0.001 |
| Primary care physicians and nurses | 61 | 13.56 (1.90) | 0.654 | <0.001 |
| Mental health professionals | 51 | 13.55 (2.37) | 0.640 | <0.001 |
| Second part of the EMHL test | ||||
| High school students (ref.) | 355 | −1.06 (1.48) | <0.001 | |
| Teachers | 43 | 0.60 (1.52) | 0.485 | <0.001 |
| University students | 57 | 1.32 (1.34) | 0.645 | <0.001 |
| Primary care physicians and nurses | 61 | 1.86 (1.56) | 0.692 | <0.001 |
| Mental health professionals | 52 | 3.13 (1.53) | 0.812 | <0.001 |
| Validity Measures | First Part of the EMHL Test | Second Part of the EMHL Test | ||||
|---|---|---|---|---|---|---|
| N | Alpha Coefficient | Pearson Correlation | p-Value (2-Tailed) | Pearson Correlation | p-Value (2-Tailed) | |
| Stigma-related (CAMI) | 344 | 0.141 | −0.246** | <0.001 | −0.222** | <0.001 |
| Stigma-related (RIBS) | 352 | 0.794 | −0.094 | 0.079 | −0.201** | <0.001 |
| Emotional Symptoms (SDQ) | 352 | 0.140** | 0.009 | 0.032 | 0.553 | |
| Conduct Problems (SDQ) | 353 | −0.095 | 0.074 | −0.121* | 0.023 | |
| Hyperactivity/inattention (SDQ) | 353 | 0.044 | 0.406 | −0.028 | 0.596 | |
| Peer problems (SDQ) | 353 | −0.041 | 0.442 | 0.006 | 0.909 | |
| SDQ total difficulties score | 352 | 0.469 | 0.025 | 0.645 | −0.030 | 0.576 |
| Prosocial (SDQ) | 353 | 0.611 | 0.029 | 0.588 | −0.023 | 0.664 |
| Bully victim | 352 | 0.016 | 0.764 | 0.068 | 0.201 | |
| Bully perpetrator | 351 | −0.050 | 0.348 | −0.130* | 0.014 | |
| Mobility (EQ-5D-5L) | 353 | −0.045 | 0.401 | 0.000 | 0.995 | |
| Self-care (EQ-5D-5L) | 353 | 0.075 | 0.160 | 0.130* | 0.014 | |
| Usual activities (EQ-5D-5L) | 353 | −0.057 | 0.286 | 0.093 | 0.081 | |
| Pain/discomfort(EQ-5D-5L) | 353 | −0.021 | 0.696 | −0.051 | 0.341 | |
| Anxiety/depression (EQ-5D-5L) | 353 | −0.122* | 0.021 | −0.062 | 0.246 | |
| EQ-5D-5L total score | 353 | 0.596 | 0.018 | 0.741 | 0.070 | 0.193 |
| EQ-5D-VAS | 352 | −0.083 | 0.120 | −0.059 | 0.273 | |
| First Part of the EMHL Test | D |
| 1 (Schizophrenia) | 0.96 |
| 2 (Diabetes) | 0.85 |
| 3 (Phobia) | 0.92 |
| 4 (Asthma) | 0.88 |
| 5 (Bipolar disorder) | 0.88 |
| 6 (Bulimia) | 1.12 |
| 7 (Cerebral palsy) | 1.25 |
| 8 (Bronchitis) | 0.83 |
| 9 (Alzheimer disease) | 0.78 |
| 10 (Depression) | 0.93 |
| 11 (Chickenpox) | 0.86 |
| 12 (Down’s Syndrome) | 1.21 |
| 13 (Epilepsy) | 1.02 |
| 14 (Anorexia nervosa) | 1.07 |
| 15 (Substance dependence) | 0.83 |
| Second Part of the EMHL Test | D |
| 1 (Definition of mental health) | 0.52 |
| 2 (Where to go for help) | 0.53 |
| 3 (Who develops a mental disorder) | 1.03 |
| 4 (Healthy Behaviors) | 0.24 |
| 5 (Night rest) | 1.05 |
| 6 (Cannabis / alcohol consumption) | 0.76 |
| 7 (Bullying) | 0.87 |
| 8 (Cyberbullying) | 0.99 |
| 9 (Social skills) | 0.90 |
| 10 (Suicidal ideation friend / family) | 0.84 |
| 11 (Self-injury) | 1.06 |
| 12 (Suicide Behavior Alert) | 1.01 |
| 13 (Depression) | 0.87 |
| 14 (Eating Disorders) | 0.50 |
| 15 (Start of Eating Disorders) | 0.54 |
| 16 (Characteristics of Eating Disorders) | 0.71 |
| 17 (Symptoms Schizophrenia) | 0.66 |
| 18 (Delusions) | 0.33 |
| 19 (Psychotic episode) | 0.55 |
| 20 (Alcohol dependence) | 0.95 |
© 2019 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Castellvi, P.; Casañas, R.; Arfuch, V.-M.; Gil Moreno, J.J.; Torres Torres, M.; García-Forero, C.; Ruiz-Castañeda, D.; Alonso, J.; Lalucat-Jo, L. Development and Validation of the EspaiJove.net Mental Health Literacy (EMHL) Test for Spanish Adolescents. Int. J. Environ. Res. Public Health 2020, 17, 72. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph17010072
Castellvi P, Casañas R, Arfuch V-M, Gil Moreno JJ, Torres Torres M, García-Forero C, Ruiz-Castañeda D, Alonso J, Lalucat-Jo L. Development and Validation of the EspaiJove.net Mental Health Literacy (EMHL) Test for Spanish Adolescents. International Journal of Environmental Research and Public Health. 2020; 17(1):72. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph17010072
Chicago/Turabian StyleCastellvi, Pere, Rocío Casañas, Victoria-Mailen Arfuch, Juan José Gil Moreno, María Torres Torres, Carlos García-Forero, Dyanne Ruiz-Castañeda, Jordi Alonso, and Lluís Lalucat-Jo. 2020. "Development and Validation of the EspaiJove.net Mental Health Literacy (EMHL) Test for Spanish Adolescents" International Journal of Environmental Research and Public Health 17, no. 1: 72. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph17010072