Experience in Developing an FHIR Medical Data Management Platform to Provide Clinical Decision Support

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Abstract
:1. Introduction
2. Methods
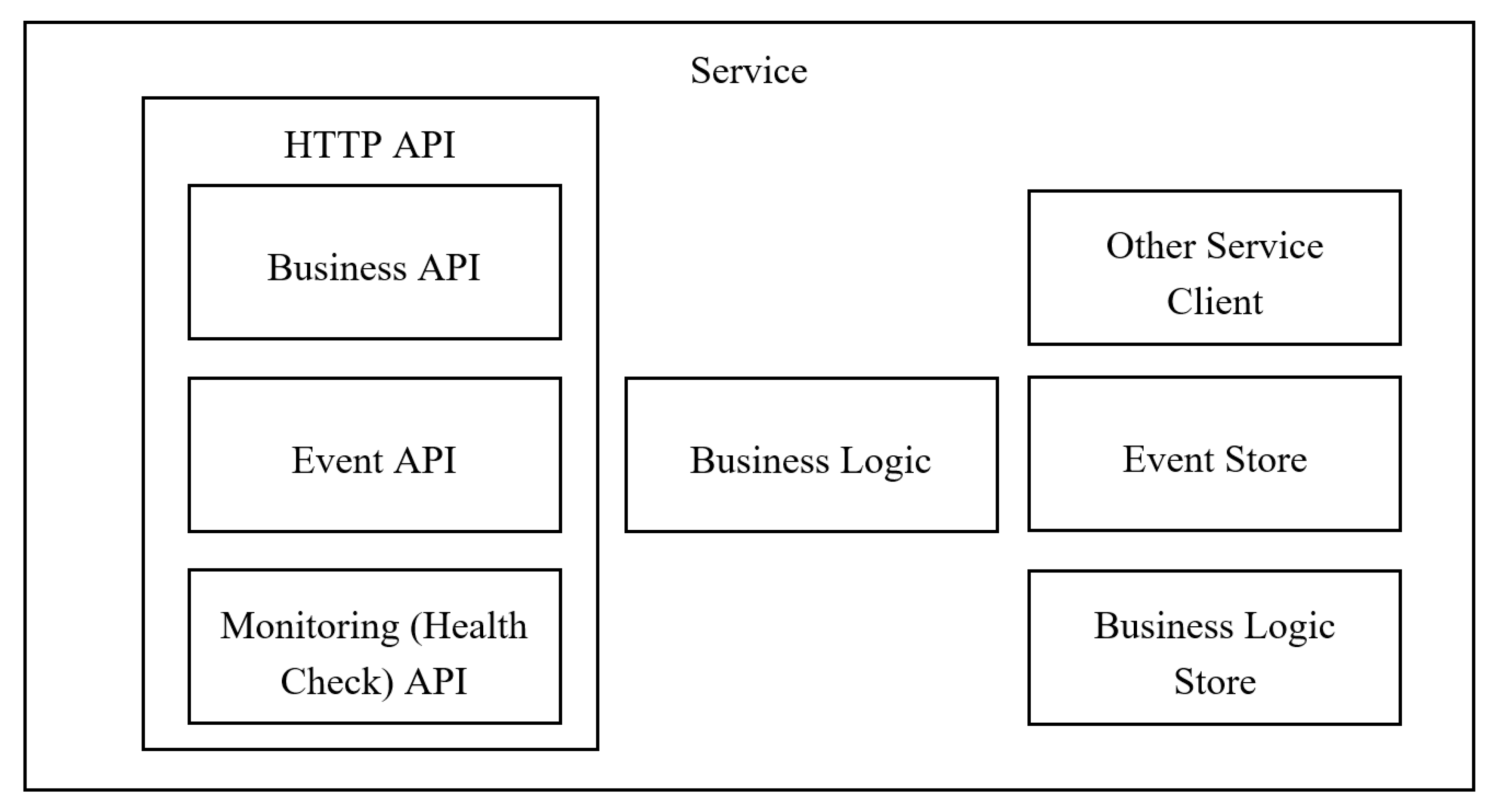
2.1. Platform Architecture
2.2. Services
- the status of the connections to the infrastructure services used by the service instance;
- the status of the host, for example, disk space;
- application-specific logic.
2.3. Clinical Modelling
- CarePlan
- MedicationRequest
- ActivityDefinition
- DetectedIssue
- RiskAssessment
- Questionnaire
- QuestionnaireResponse
- ResearchDefinition
- PlanDefinition
- Goal
- Observation
- Condition
- FamilyMemberHistory
- DiagnosticReport
- Group
- RequestGroup
- AllergyIntolerance
- Immunization
- Procedure
- Encounter
- Appointment
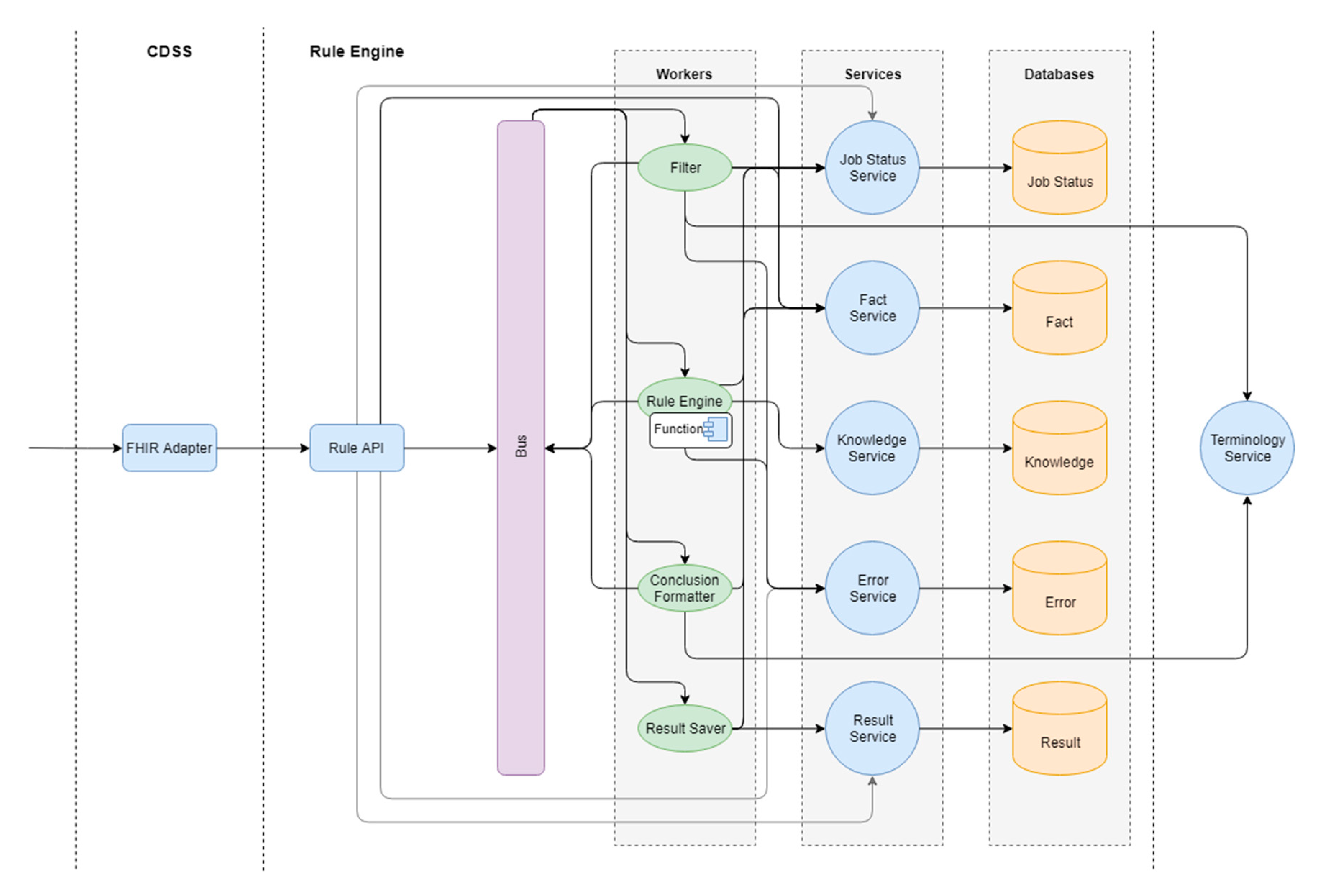
2.4. Rule Engine
- Definition_1. Value >1. Definition_2. Value = 0
- Operation Rule has the following structure:
- ○
- Definition ID
- ○
- Nomenclature
- ○
- Code
- ○
- Name
- ○
- Operation
- ○
- Value
- Scale is used for the results of evaluation scales, questionnaires (as a coded value of the result or as a number);
- Risk is used to determine if there is a risk of any disease or condition;
- Diagnosis is used to evaluate the possible diagnosis based on laboratory or instrumental studies;
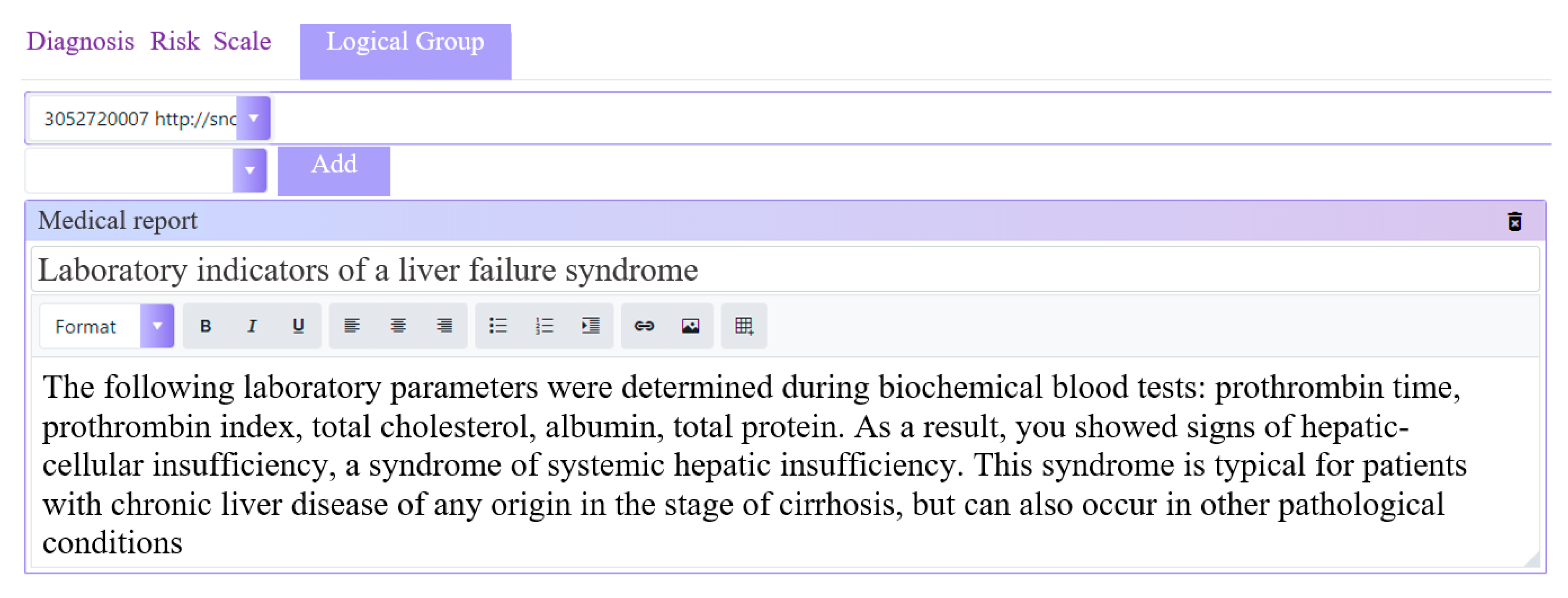
- DiagnosticReport is used for coded logic groups to interpret clinical observations;
- ReferralRequest is used to recommend specialist appointment and routing of patients;
- ProcedureRequest is used to recommend instrumental examinations;
- DiagnosticRequest is used to recommend laboratory tests;
- Description is used to describe the conclusions drawn (e.g., an explanation of the identified risk level);
- Recommendation is used for free text recommendations;
- BehaviorRecommendation is used for coded lifestyle recommendations.
- Calculation of risks of disease;
- Interpretation and monitoring of clinical observations;
- Analysis of medical services provided to a patient for compliance with the standards of the insurance company;
- Treatment plan management;
- Analysis of prescriptions for drug interactions and contraindications for prescribing.
- FHIR Adapter: the service converts data from the FHIR format into the internal Rule Engine format. This service also provides the possibility of Rule Engine invocation according to the CDS Hooks specification.
- Rule API: the service performs internal routing and saves processed data for further analysis.
- Filter: the service is responsible for filtering the data to the actual state, applicable to the mechanism of logical output.
- Rule Engine: the service is responsible for the logical inference mechanism based on the rules.
- Formatter: the service is responsible for formatting the results of logical inference.
- Api.KnowledgeService: the knowledge service is responsible for CRUD operations with the graphical knowledge base. Is used by the Rule Engine to search for rules, artifacts, and definitions.
- Api.FactService: fact service is responsible for preserving and providing facts at all stages of inference.
- Api.JobStatusService: the status service is responsible for creating new tasks and saving statuses.
- Api.ErrorService: the error service is responsible for saving and reporting errors that occur during the inference process.
- Api.ResultService: the result service is responsible for saving and providing the results obtained by the Rule Engine inference.
- TerminologyService is responsible for the storage and provision of medical terminology.
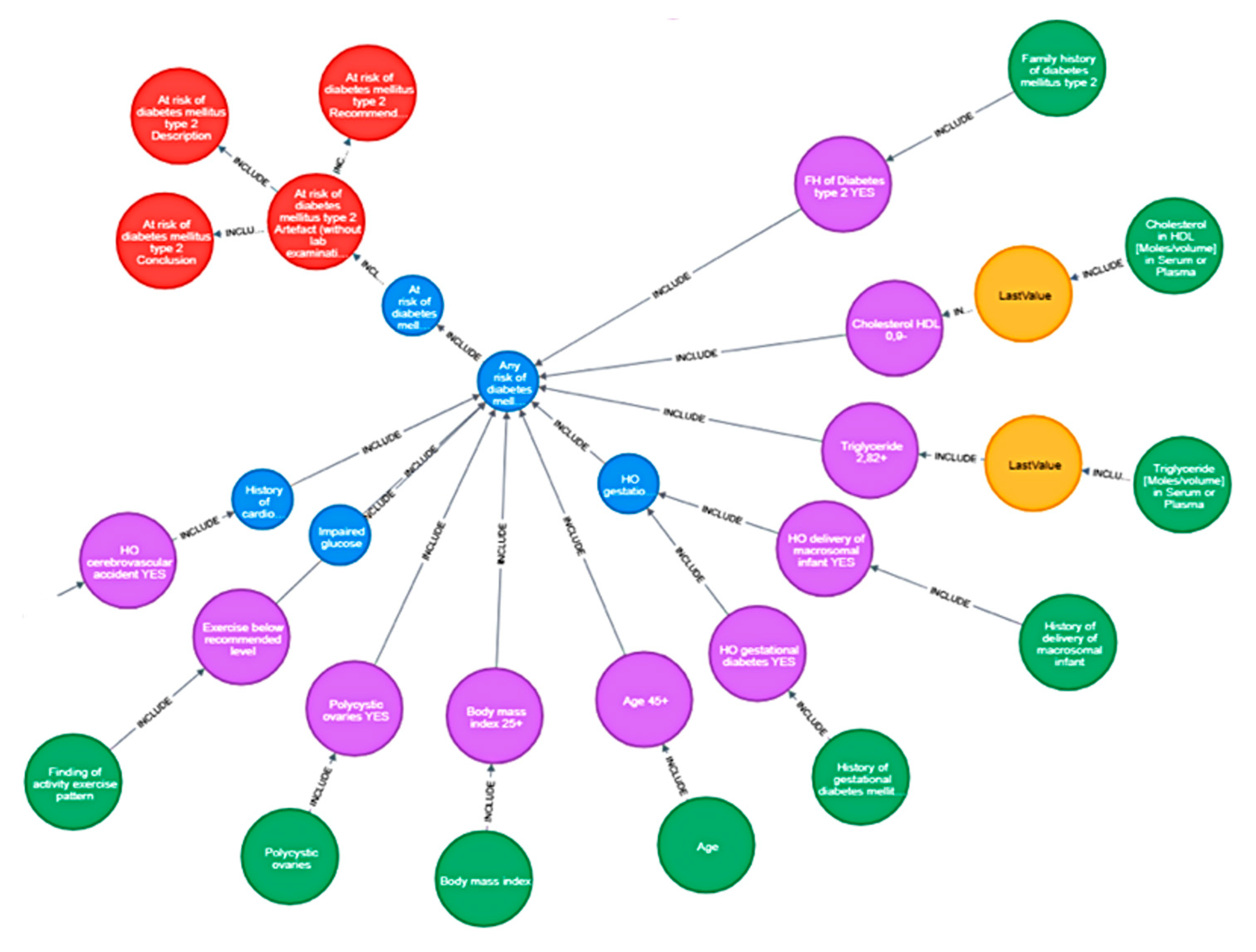
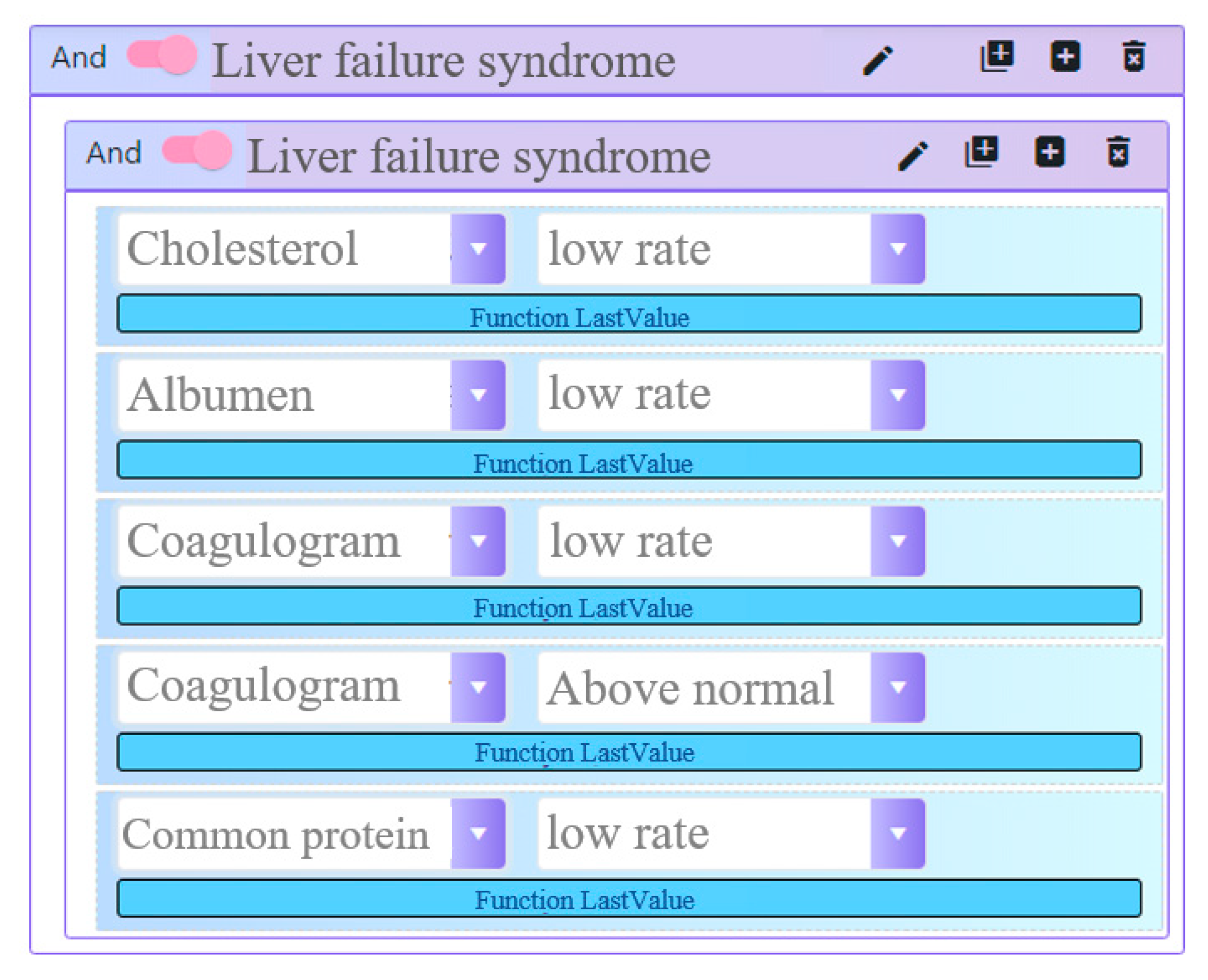
Rule Editor
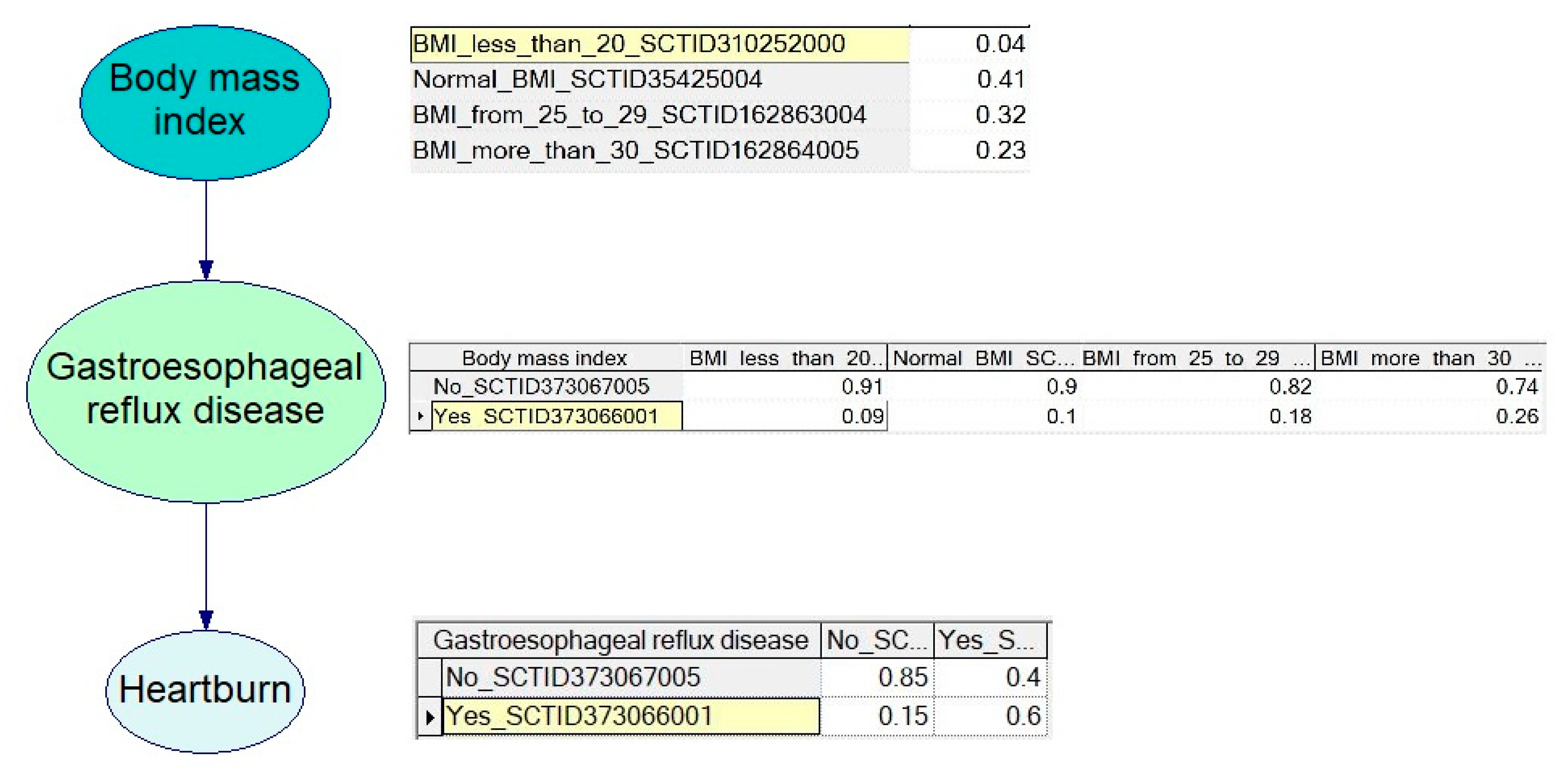
2.5. Bayes Engine
- C# + .net core 2.2 for the core logic;
- asp.net core 2.2—for the web interface;
- Infer.NET (ML.net)—a framework for running Bayesian inference in graphical models. In our case it was used for probabilistic programming.
- PostgreSQL 11 for data storage.
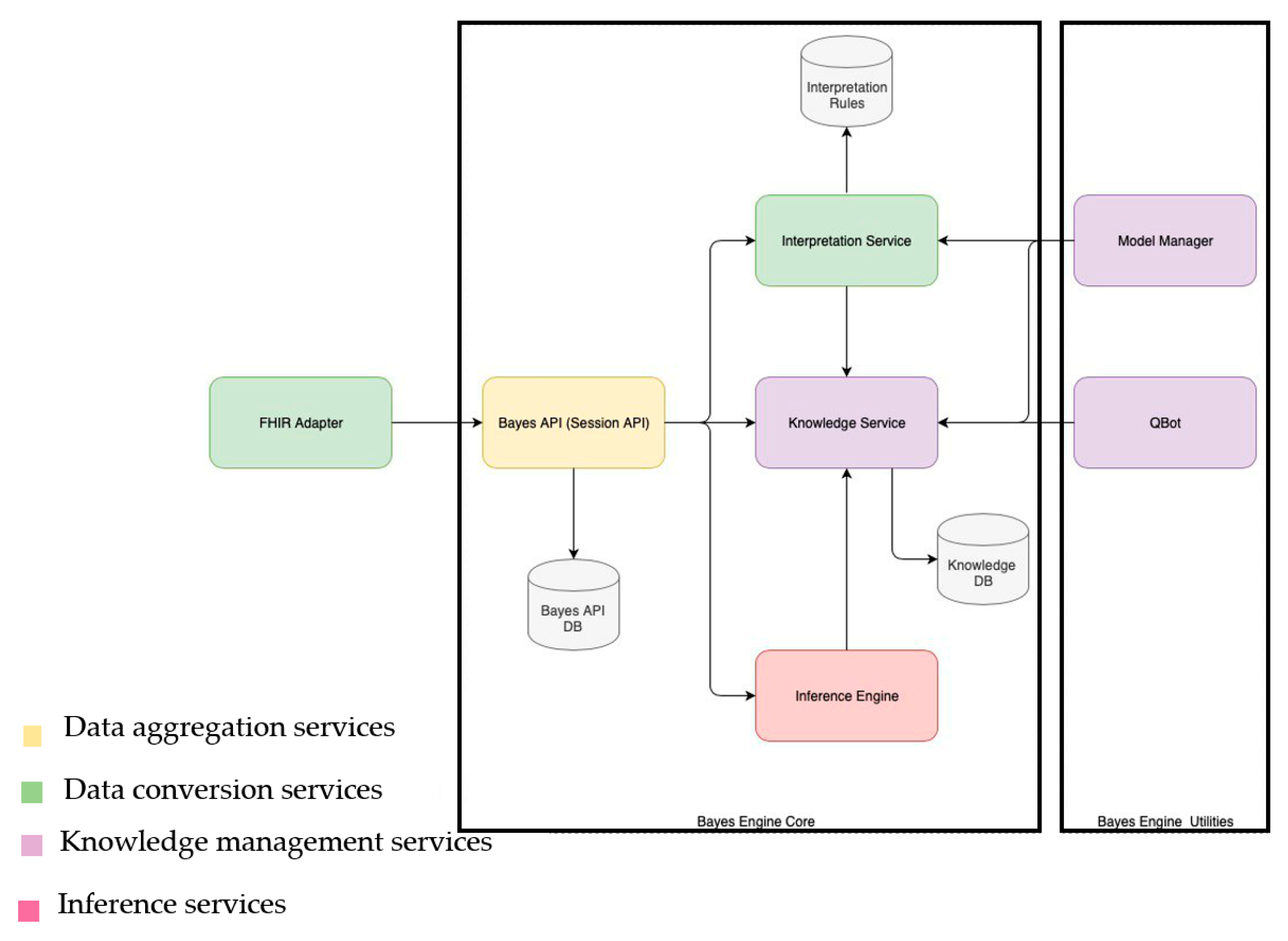
- FHIR Adapter: the service converts data from the FHIR format into the internal Bayes Engine format. Furthermore, this service provides the possibility of Rule Engine invocation according to the CDS Hooks specification.
- Bayes API: the service performs internal routing and stores processed data for further analysis;
- Interpretation Service: the service performs data processing before calculation on Bayesian networks;
- Knowledge Service: the service stores Bayesian models created by experts and collects probabilities used for calculations;
- Inference Engine: the service performs inference on the basis of Bayesian models;
- Qbot: the service validates inference results and models with experts in the learning mode;
- Model Manager: supports model management in the Knowledge Service (CRUD on models).
- Creating a model prototype;
- Model structure validation by experts;
- Improvement of the model structure;
- Definition of probabilities;
- Validation of the model by experts using real validated clinical cases.
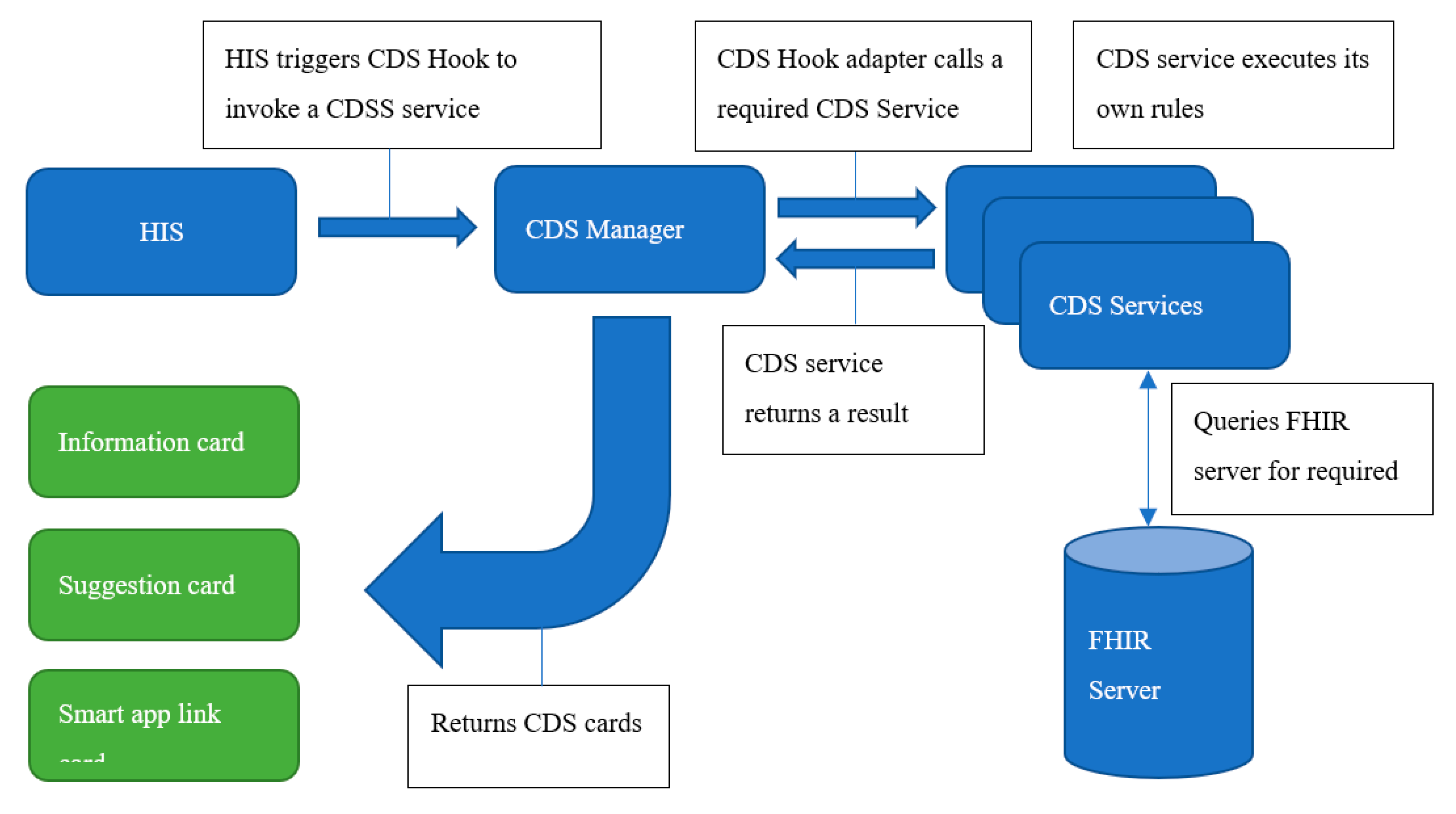
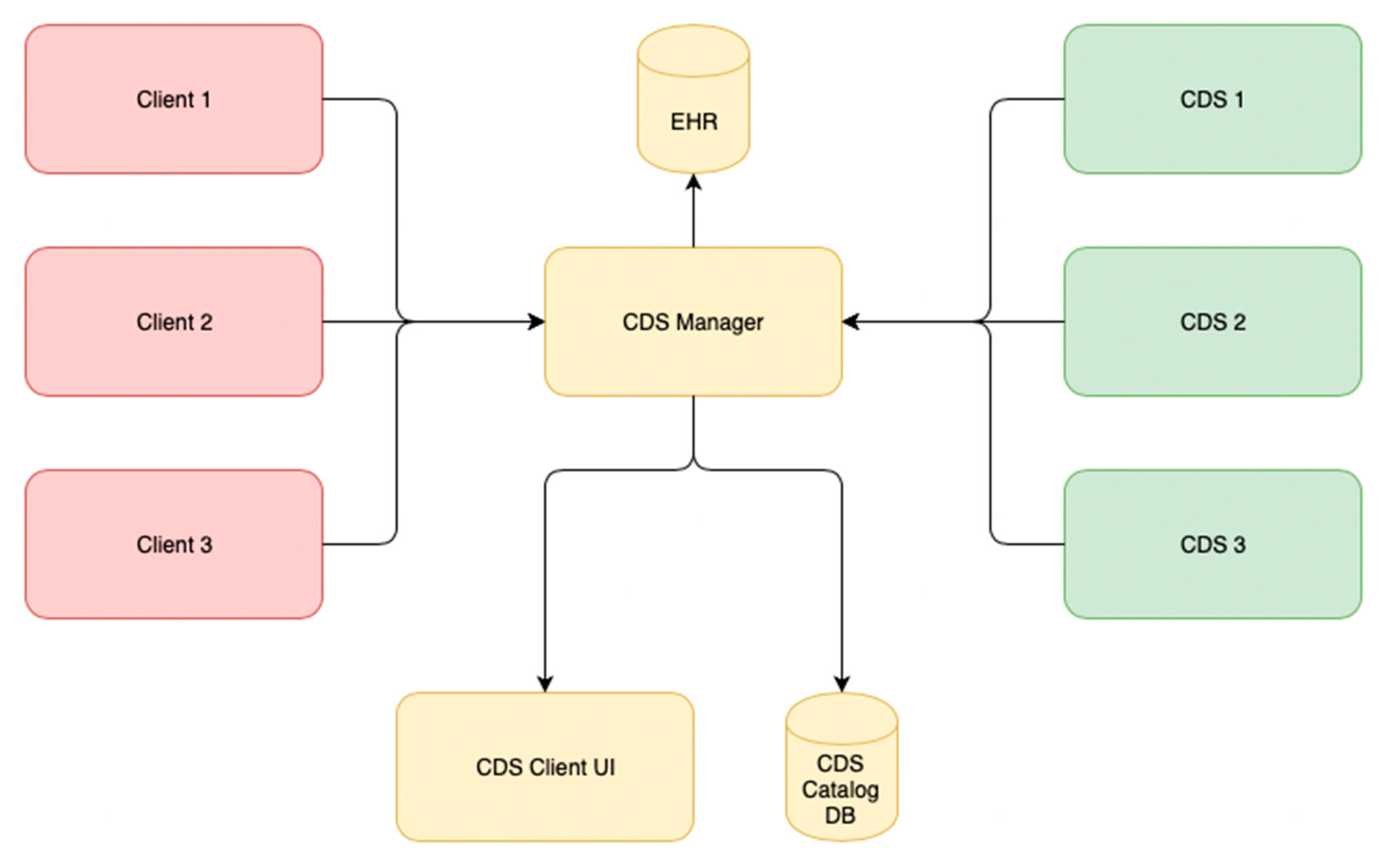
2.6. CDS Hooks
- Store a directory of available CDSS services on the platform, provide registration, and allow the client application to configure which CDSS to use for specific needs.
- Provide proxying calls from the client to the selected CDSS and collect usage statistics.
- RESTful interface based on the CDS Hooks specification. This included support of the defined format of the RESTful body and the return of the CDS results as cards;
- A FHIR platform adaptor was adjusted to support individual FHIR connection for each EHR session;
- Implementation of the data points required by the CDS Hooks API. This included the management of hooks and the data points that needed to be pre-fetched by the calling HIS.
3. Results
3.1. Rule Engine
3.2. Bayes Engine
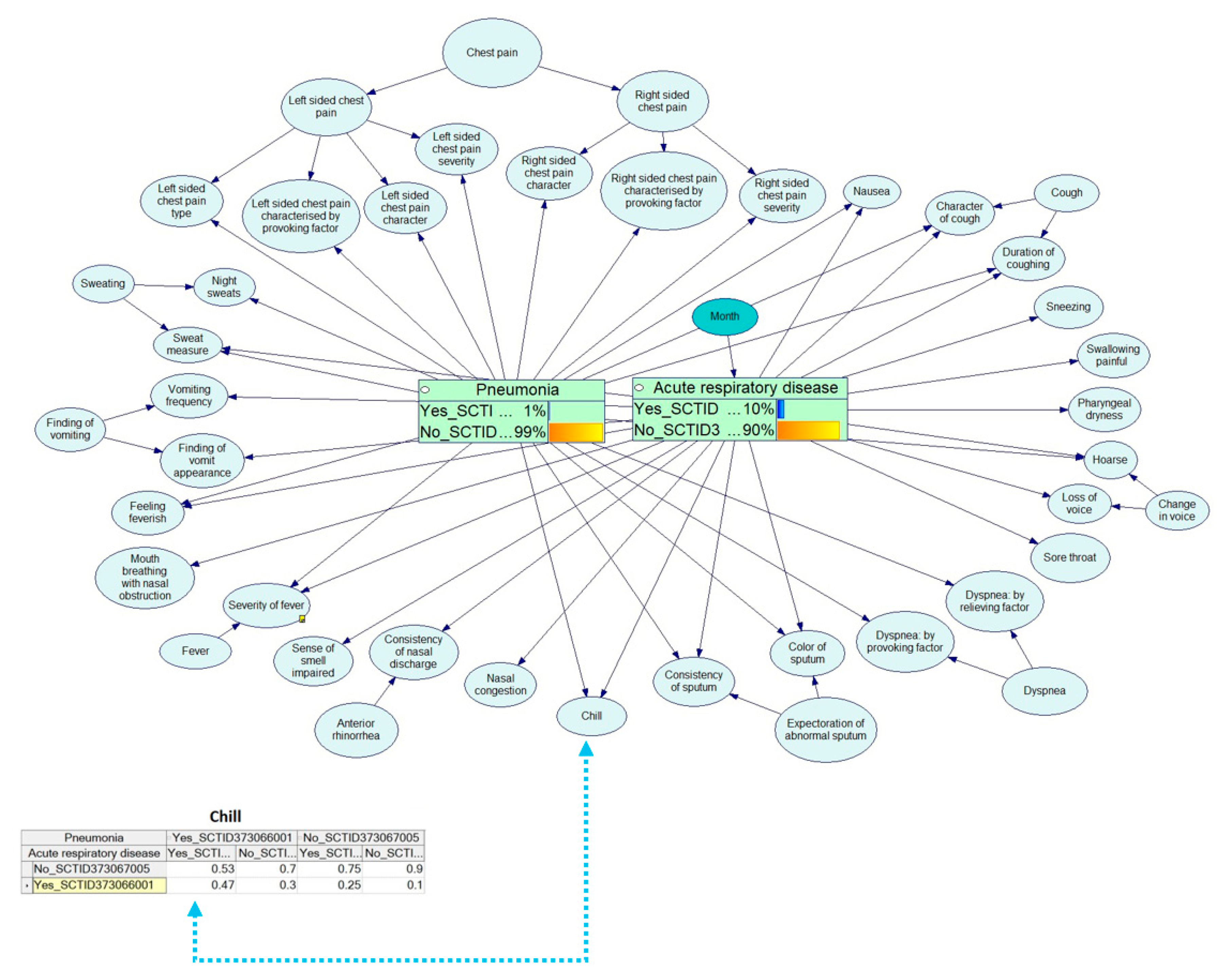
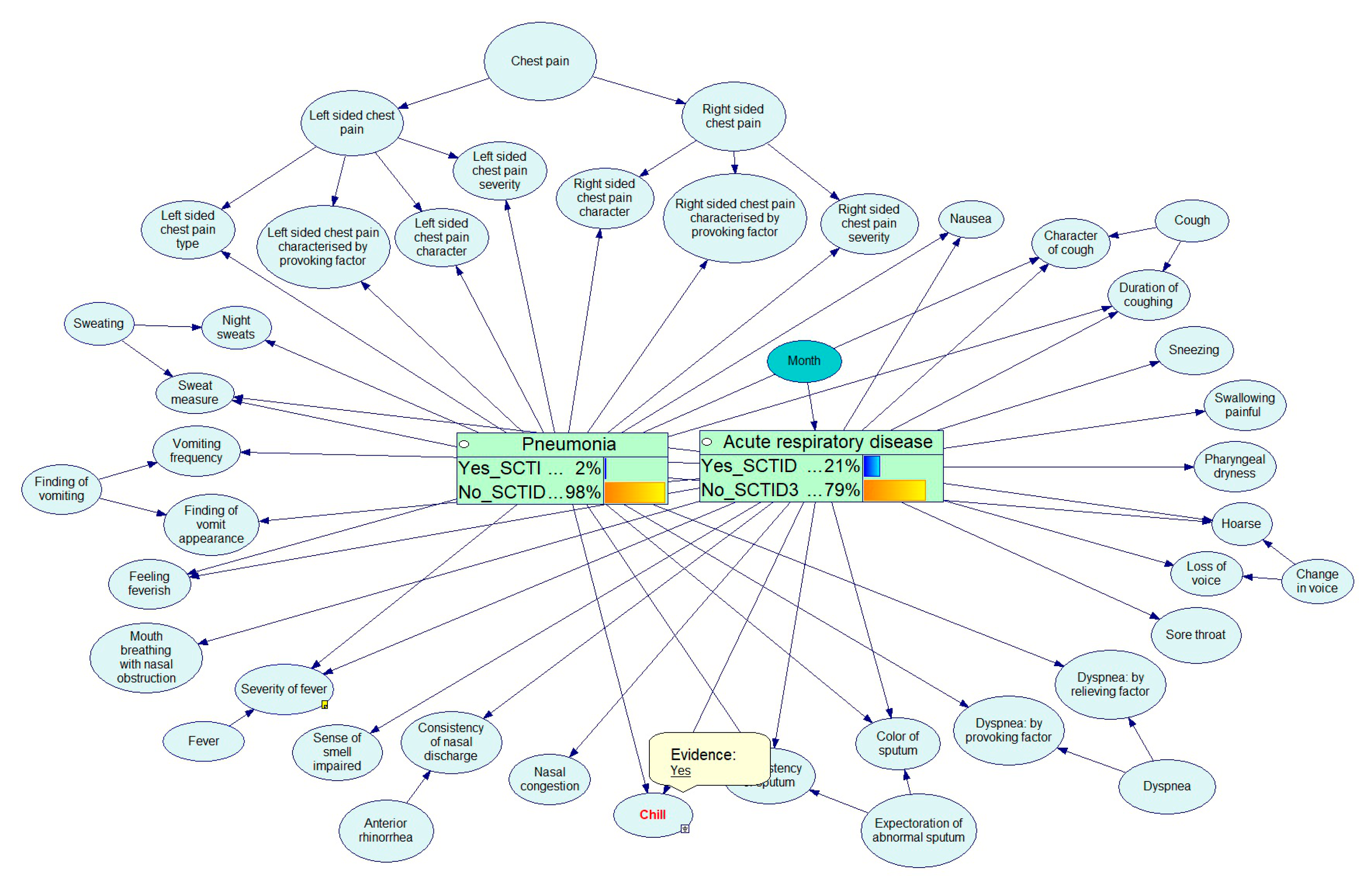
Bayes Engine Workflow Example
4. Discussion
4.1. Architecture
4.2. Implications and Future Use
4.3. Operation
5. Conclusions
Author Contributions
Funding
Conflicts of Interest
References
- Kopanitsa, G. Microservice Architecture to Provide Medical Data Management for Decision Support. Stud. Health Technol. Inform. 2019, 261, 230–235. [Google Scholar] [PubMed]
- Pan, H.; Deal, B. Reporting on the Performance and Usability of Planning Support Systems—Towards a Common Understanding. Appl. Spat. Anal. Policy 2019. [Google Scholar] [CrossRef]
- Pan, H.; Page, J.; Zhang, L.; Chen, S.; Cong, C.; Destouni, G.; Kalantari, Z.; Deal, B. Using comparative socio-ecological modeling to support Climate Action Planning (CAP). J. Clean. Prod. 2019, 232, 30–42. [Google Scholar] [CrossRef]
- Dao Phuoc, T.; Khuong Quynh, L.; Vien Dang Khanh, L.; Ong Phuc, T.; Le Sy, H.; Le Ngoc, T.; Phung Khanh, L. Clinical prognostic models for severe dengue: A systematic review protocol. Wellcome Open Res. 2019, 4, 12. [Google Scholar] [CrossRef]
- Bose, R. Knowledge management-enabled health care management systems: Capabilities, infrastructure, and decision-support. Expert Syst. Appl. 2003, 24, 59–71. [Google Scholar] [CrossRef]
- Marco-Ruiz, L.; Pedrinaci, C.; Maldonado, J.A.; Panziera, L.; Chen, R.; Bellika, J.G. Publication, discovery and interoperability of Clinical Decision Support Systems: A Linked Data approach. J. Biomed. Inform. 2016, 62, 243–264. [Google Scholar] [CrossRef]
- Khalifa, M.; Zabani, I. Improving Utilization of Clinical Decision Support Systems by Reducing Alert Fatigue: Strategies and Recommendations. Stud. Health Technol. Inform. 2016, 226, 51–54. [Google Scholar]
- Chi, C.L.; Nick Street, W.; Robinson, J.G.; Crawford, M.A. Individualized patient-centered lifestyle recommendations: An expert system for communicating patient specific cardiovascular risk information and prioritizing lifestyle options. J. Biomed. Inform. 2012, 45, 1164–1174. [Google Scholar] [CrossRef] [Green Version]
- Owens, D.K. Improving practice guidelines with patient-specific recommendations. Ann. Intern. Med. 2011, 154, 638–639. [Google Scholar] [CrossRef] [Green Version]
- Kopanitsa, G.; Semenov, I. Patient facing decision support system for interpretation of laboratory test results. BMC Med. Inform. Decis. Mak. 2018, 18, 68. [Google Scholar] [CrossRef] [Green Version]
- Kam, H.J.; Kim, J.A.; Cho, I.; Kim, Y.; Park, R.W. Integration of heterogeneous clinical decision support systems and their knowledge sets: Feasibility study with Drug-Drug Interaction alerts. AMIA Annu. Symp. Proc. 2011, 2011, 664–673. [Google Scholar]
- Lee, J.; Kim, J.; Cho, I.; Kim, Y. Integration of workflow and rule engines for clinical decision support services. Stud. Health Technol. Inform. 2010, 160, 811–815. [Google Scholar]
- Weber, S.; Crago, E.A.; Sherwood, P.R.; Smith, T. Practitioner approaches to the integration of clinical decision support system technology in critical care. J. Nurs. Adm. 2009, 39, 465–469. [Google Scholar] [CrossRef]
- Leroux, H.; Metke-Jimenez, A.; Lawley, M.J. Towards achieving semantic interoperability of clinical study data with FHIR. J. Biomed. Semant. 2017, 8, 41. [Google Scholar] [CrossRef] [Green Version]
- Atalag, K.; Yang, H.Y.; Tempero, E.; Warren, J. Model driven development of clinical information sytems using openEHR. Stud. Health Technol. Inform. 2011, 169, 849–853. [Google Scholar]
- Kopanitsa, G. Evaluation Study for an ISO 13606 Archetype Based Medical Data Visualization Method. J. Med. Syst. 2015, 39, 82. [Google Scholar] [CrossRef]
- Barros Castro, J.; Lamelo Alfonsin, A.; Prieto Cebreiro, J.; Rimada Mora, D.; Carrajo Garcia, L.; Vazquez Gonzalez, G. Development of ISO 13606 archetypes for the standardisation of data registration in the Primary Care environment. Stud. Health Technol. Inform. 2015, 210, 877–881. [Google Scholar]
- Paun, I.D.; Sauciuc, D.G.; Iosif, N.O.; Stan, O.; Perse, A.; Dehelean, C.; Miclea, L. Local EHR management based on openEHR and EN13606. J. Med. Syst. 2011, 35, 585–590. [Google Scholar] [CrossRef]
- Pecoraro, F.; Luzi, D.; Ricci, F.L. Data Warehouse Design from HL7 Clinical Document Architecture Schema. Stud. Health Technol. Inform. 2015, 213, 139–142. [Google Scholar]
- Boussadi, A.; Zapletal, E. A Fast Healthcare Interoperability Resources (FHIR) layer implemented over i2b2. BMC Med. Inform. Decis. Mak. 2017, 17, 120. [Google Scholar] [CrossRef]
- Marcos, M.; Maldonado, J.A.; Martinez-Salvador, B.; Bosca, D.; Robles, M. Interoperability of clinical decision-support systems and electronic health records using archetypes: A case study in clinical trial eligibility. J. Biomed. Inform. 2013, 46, 676–689. [Google Scholar] [CrossRef] [Green Version]
- Kashfi, H. An openEHR-based clinical decision support system: A case study. Stud. Health Technol. Inform. 2009, 150, 348. [Google Scholar]
- Khalilia, M.; Choi, M.; Henderson, A.; Iyengar, S.; Braunstein, M.; Sun, J. Clinical Predictive Modeling Development and Deployment through FHIR Web Services. AMIA Annu. Symp. Proc. 2015, 2015, 717–726. [Google Scholar]
- Wang, L.L.; Thomas Hayman, G.; Smith, J.R.; Tutaj, M.; Shimoyama, M.E.; Gennari, J.H. Predicting instances of pathway ontology classes for pathway integration. J. Biomed. Semant. 2019, 10, 11. [Google Scholar] [CrossRef]
- Ruokolainen, J. Mobile Microservice Architecture for Patients Self-Care. Stud. Health Technol. Inform. 2017, 244, 106. [Google Scholar]
- Spineth, M.; Rappelsberger, A.; Adlassnig, K.P. Implementing CDS Hooks Communication in an Arden-Syntax-Based Clinical Decision Support Platform. Stud. Health Technol. Inform. 2018, 255, 165–169. [Google Scholar]
- Wulff, A.; Montag, S.; Marschollek, M.; Jack, T. Clinical Decision-Support Systems for Detection of Systemic Inflammatory Response Syndrome, Sepsis, and Septic Shock in Critically Ill Patients: A Systematic Review. Methods Inform. Med. 2019. [Google Scholar] [CrossRef]
- Sakurai, R.; Ohe, K. Effects of Computerized Guideline-Oriented Clinical Decision Support System on Antithrombotic Therapy in Patients with Atrial Fibrillation: A Systematic Review and Meta-Analysis. Stud. Health Technol. Inform. 2019, 264, 768–772. [Google Scholar] [CrossRef]
- Hussain, M.I.; Reynolds, T.L.; Zheng, K. Medication safety alert fatigue may be reduced via interaction design and clinical role tailoring: A systematic review. J. Am. Med. Inform. Assoc. 2019, 26, 1141–1149. [Google Scholar] [CrossRef] [Green Version]
- Semenov, I.; Kopanitsa, G.; Denisov, D.; Alexandr, Y.; Osenev, R.; Andreychuk, Y. Patients Decision Aid System Based on FHIR Profiles. J. Med. Syst. 2018, 42, 166. [Google Scholar] [CrossRef]
- Sittig, D.F.; Wright, A.; Osheroff, J.A.; Middleton, B.; Teich, J.M.; Ash, J.S.; Campbell, E.; Bates, D.W. Grand challenges in clinical decision support. J. Biomed. Inform. 2008, 41, 387–392. [Google Scholar] [CrossRef] [Green Version]
- Šelih, J.; Kne, A.; Srdić, A.; Žura, M. Multiple-criteria decision support system in highway infrastructure management. Transport 2008, 23, 299–305. [Google Scholar] [CrossRef] [Green Version]
- Stram, M.; Gigliotti, T.; Hartman, D.; Pitkus, A.; Huff, S.M.; Riben, M.; Henricks, W.H.; Farahani, N.; Pantanowitz, L. Logical Observation Identifiers Names and Codes for Laboratorians. Arch. Pathol. Lab. Med. 2019. [Google Scholar] [CrossRef] [Green Version]
- Arbabi, A.; Adams, D.R.; Fidler, S.; Brudno, M. Identifying Clinical Terms in Medical Text Using Ontology-Guided Machine Learning. JMIR Med. Inform. 2019, 7, e12596. [Google Scholar] [CrossRef]
- Zhang, X.A.; Yates, A.; Vasilevsky, N.; Gourdine, J.P.; Callahan, T.J.; Carmody, L.C.; Danis, D.; Joachimiak, M.P.; Ravanmehr, V.; Pfaff, E.R.; et al. Semantic integration of clinical laboratory tests from electronic health records for deep phenotyping and biomarker discovery. NPJ Digit. Med. 2019, 2. [Google Scholar] [CrossRef] [Green Version]
- Nguyen, B.P.; Reese, T.; Decker, S.; Malone, D.; Boyce, R.D.; Beyan, O. Implementation of Clinical Decision Support Services to Detect Potential Drug-Drug Interaction Using Clinical Quality Language. Stud. Health Technol. Inform. 2019, 264, 724–728. [Google Scholar] [CrossRef]
- Odigie, E.; Lacson, R.; Raja, A.; Osterbur, D.; Ip, I.; Schneider, L.; Khorasani, R. Fast Healthcare Interoperability Resources, Clinical Quality Language, and Systematized Nomenclature of Medicine-Clinical Terms in Representing Clinical Evidence Logic Statements for the Use of Imaging Procedures: Descriptive Study. JMIR Med. Inform. 2019, 7, e13590. [Google Scholar] [CrossRef]
- Dolin, R.H.; Boxwala, A.; Shalaby, J. A Pharmacogenomics Clinical Decision Support Service Based on FHIR and CDS Hooks. Methods Inform. Med. 2018, 57, e115–e123. [Google Scholar] [CrossRef] [Green Version]
- Kopanitsa, G. Integration of Hospital Information and Clinical Decision Support Systems to Enable the Reuse of Electronic Health Record Data. Methods Inform. Med. 2017, 56, 238–247. [Google Scholar] [CrossRef]
- Emami Khoonsari, P.; Moreno, P.; Bergmann, S.; Burman, J.; Capuccini, M.; Carone, M.; Cascante, M.; de Atauri, P.; Foguet, C.; Gonzalez-Beltran, A.N.; et al. Interoperable and scalable data analysis with microservices: Applications in metabolomics. Bioinformatics 2019, 35, 3752–3760. [Google Scholar] [CrossRef] [Green Version]
- Li, Z.; Seco, D.; Sánchez Rodríguez, A.E. Microservice-Oriented Platform for Internet of Big Data Analytics: A Proof of Concept. Sensors 2019, 19, 1134. [Google Scholar] [CrossRef] [Green Version]
- Williams, C.L.; Sica, J.C.; Killen, R.T.; Balis, U.G. The growing need for microservices in bioinformatics. J. Pathol. Inform. 2016, 7, 45. [Google Scholar] [CrossRef]
















© 2019 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Semenov, I.; Osenev, R.; Gerasimov, S.; Kopanitsa, G.; Denisov, D.; Andreychuk, Y. Experience in Developing an FHIR Medical Data Management Platform to Provide Clinical Decision Support. Int. J. Environ. Res. Public Health 2020, 17, 73. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph17010073
Semenov I, Osenev R, Gerasimov S, Kopanitsa G, Denisov D, Andreychuk Y. Experience in Developing an FHIR Medical Data Management Platform to Provide Clinical Decision Support. International Journal of Environmental Research and Public Health. 2020; 17(1):73. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph17010073
Chicago/Turabian StyleSemenov, Ilia, Roman Osenev, Sergey Gerasimov, Georgy Kopanitsa, Dmitry Denisov, and Yuriy Andreychuk. 2020. "Experience in Developing an FHIR Medical Data Management Platform to Provide Clinical Decision Support" International Journal of Environmental Research and Public Health 17, no. 1: 73. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph17010073