Incidence and Risk Assessment for Atrial Fibrillation at 5 Years: Hypertensive Diabetic Cohort

 , , ,
, , ,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Design
2.2. Setting and Study Population
2.3. Research Ethics
2.4. Study Variables
2.5. Statistical Analysis
3. Results
3.1. Baseline Characteristics
3.2. Independent Prognostic Factors for New AF
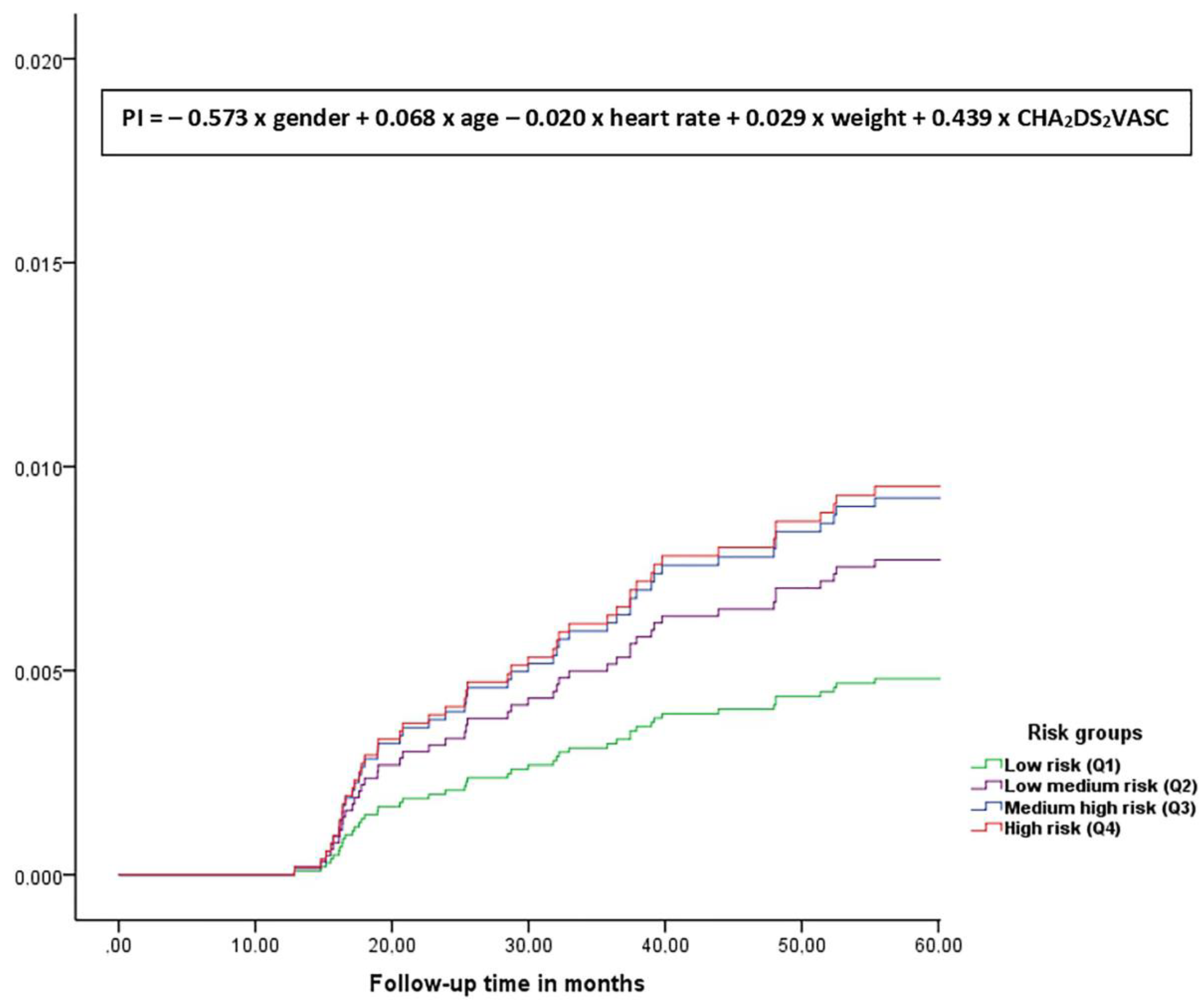
3.3. Risk Score for New Atrial Fibrillation (AF) (Prognostic Index, PI)
- Q1 (PI ≤ 6.88). Lowest risk group for AF: ID rate 2.95/1000 people/years (95% CI 1.69–4.80).
- Q2 (PI 6.89 ≤ 7.71). Median-low risk group for AF: ID rate 8.85/1000 people/years (95% CI 6.54–11.70).
- Q3 (PI 7.72 ≤ 8.39). Median-high risk group for AF: ID rate 15.70/1000 people/years (95% CI 12.47–19.52).
- Q4 (PI > 8.39). Highest risk group for AF: ID rate 22.45/1000 people/years (95% CI 18.41–27.10).
4. Discussion
4.1. Main Findings
4.2. Interpretation of the Study Results
4.3. Strengths and Limitations
5. Conclusions
6. Patents
Supplementary Materials
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- King’s College London for the Stroke Alliance for Europe. Atrial Fibrillation. The Burden of Stroke in Europe. Available online: https://strokeeurope.eu/ (accessed on 1 January 2019).
- Clua-Espuny, J.L.; Lechuga-Durán, Í.; Bosch, R.; Roso-Llorach, A.; Panisello-Tafalla, A.; Lucas-Noll, J.; López-Pablo, C.; Queralt-Tomas, L.; Giménez-Garcia, E.; Gonzalez-Rojas, N.; et al. Prevalencia de la fibrilación auricular desconocida y la no tratada con anticoagulantes. Estudio AFABE. Rev. Española de Cardiol. 2013, 66, 545–552. [Google Scholar] [CrossRef]
- Alkhouli, M.; Alqahtani, F.; Aljohani, S.; Alvi, M.; Holmes, D.R. Burden of Atrial Fibrillation–Associated Ischemic Stroke in the United States. JACC: Clin. Electrophysiol. 2018, 4, 618–625. [Google Scholar] [CrossRef] [PubMed]
- Wang, A.; Green, J.B.; Halperin, J.L.; Piccini, J.P. Atrial Fibrillation and Diabetes Mellitus: JACC Review Topic of the Week. J. Am. Coll. Cardiol. 2019, 74, 1107–1115. [Google Scholar] [CrossRef] [PubMed]
- Echouffo-Tcheugui, J.B.; Shrader, P.; Thomas, L.; Gersh, B.J.; Kowey, P.R.; Mahaffey, K.W.; Singer, D.E.; Hylek, E.M.; Go, A.S.; Peterson, E.D.; et al. Care Patterns and Outcomes in Atrial Fibrillation Patients With and Without Diabetes. J. Am. Coll. Cardiol. 2017, 70, 1325–1335. [Google Scholar] [CrossRef] [PubMed]
- Welton, N.J.; McAleenan, A.; Thom, H.; Davies, P.; Hollingworth, W.; Higgins, J.P.T.; Okoli, G.; Sterne, J.; Feder, G.; Eaton, D.; et al. Screening strategies for atrial fibrillation: A systematic review and cost-effectiveness analysis. Heal. Technol. Assess. 2017, 21, 1–236. [Google Scholar] [CrossRef] [Green Version]
- Zethelius, B.; Gudbjörnsdottir, S.; Eliasson, B.; Eeg-Olofsson, K.; Svensson, A.-M.; Cederholm, J. Risk factors for atrial fibrillation in type 2 diabetes: Report from the Swedish National Diabetes Register (NDR). Diabetologia 2015, 58, 2259–2268. [Google Scholar] [CrossRef]
- Staerk, L.; Preis, S.R.; Lin, H.; Casas, J.P.; Lunetta, K.; Weng, L.-C.; Anderson, C.D.; Ellinor, P.T.; Lubitz, S.A.; Benjamin, E.J.; et al. Novel Risk Modeling Approach of Atrial Fibrillation With Restricted Mean Survival Times: Application in the Framingham Heart Study Community-Based Cohort. Circ. Cardiovasc. Qual. Outcomes 2020, 13. [Google Scholar] [CrossRef]
- Meyre, P.; Aeschbacher, S.; Blum, S.; Coslovsky, M.; Beer, J.H.; Moschovitis, G.; Rodondi, N.; Baretella, O.; Kobza, R.; Sticherling, C.; et al. The Admit-AF risk score: A clinical risk score for predicting hospital admissions in patients with atrial fibrillation. Eur. J. Prev. Cardiol. 2020. [Google Scholar] [CrossRef]
- Rossello, X.; Dorresteijn, J.A.; Janssen, A.; Lambrinou, E.; Scherrenberg, M.; Bonnefoy-Cudraz, E.; Cobain, M.; Piepoli, M.F.; Visseren, F.L.; Dendale, P.; et al. Risk prediction tools in cardiovascular disease prevention: A report from the ESC Prevention of CVD Programme led by the European Association of Preventive Cardiology (EAPC) in collaboration with the Acute Cardiovascular Care Association (ACCA) and the Association of Cardiovascular Nursing and Allied Professions (ACNAP). Eur. J. Prev. Cardiol. 2019, 26, 1534–1544. [Google Scholar] [CrossRef]
- Yang, P.; Zhao, Y.; Wong, N.D. Development of a Risk Score for Atrial Fibrillation in Adults With Diabetes Mellitus (from the ACCORD Study). Am. J. Cardiol. 2020, 125, 1638–1643. [Google Scholar] [CrossRef]
- Saliba, W.; Gronich, N.; Barnett-Griness, O.; Rennert, G. Usefulness of CHADS2 and CHA2DS2-VASc Scores in the Prediction of New-Onset Atrial Fibrillation: A Population-Based Study. Am. J. Med. 2016, 129, 843–849. [Google Scholar] [CrossRef] [Green Version]
- Ictus: Action Plan in Europe (2018–2030). Ed Stroke Alliance For Europe (SAFE). Available online: https://eso-stroke.org/action-plan-stroke-europe-2018-2030-2/ (accessed on 24 June 2019).
- Moran, P.S.; Teljeur, C.; Ryan, M.; Smith, S.M. Systematic screening for the detection of atrial fibrillation. Cochrane Database Syst. Rev. 2016, 3, CD009586. [Google Scholar] [CrossRef] [PubMed]
- Clua-Espuny, J.L.; Muñoz-Perez, M.A.; Bustamante-Rangel, A. Stepwise High Risk Individuals Screening for Atrial Fibrillation Using Sequential Clinical-electro-biological Register: The AFRICAT Study (Atrial Fibrillation Research In CATalonia); NCT03188484; ClinicalTrials.gov Identifier. Available online: https://clinicaltrials.gov/ct2/show/NCT03188484?term=africat&draw=2&rank=1/ (accessed on 12 November 2019).
- Hess, P.L.; Healey, J.; Granger, C.B.; Connolly, S.; Ziegler, P.D.; Alexander, J.H.; Kowey, P.R.; Ruff, C.; Flaker, G.; Halperin, J.L.; et al. The Role of Cardiovascular Implantable Electronic Devices in the Detection and Treatment of Subclinical Atrial Fibrillation. JAMA Cardiol. 2017, 2, 324. [Google Scholar] [CrossRef] [PubMed]
- Attia, Z.I.; Noseworthy, P.A.; Lopez-Jimenez, F.; Asirvatham, S.J.; Deshmukh, A.J.; Gersh, B.J.; Carter, R.E.; Yao, X.; Rabinstein, A.A.; Erickson, B.J.; et al. An artificial intelligence-enabled ECG algorithm for the identification of patients with atrial fibrillation during sinus rhythm: A retrospective analysis of outcome prediction. Lancet 2019, 394, 861–867. [Google Scholar] [CrossRef]
- Freedman, B.; Camm, J.; Calkins, H.; Healey, J.S.; Rosenqvist, M.; Wang, J.; Albert, C.M.; Anderson, C.S.; Antoniou, S.; Benjamin, E.J.; et al. Screening for Atrial Fibrillation. Circulation 2017, 135, 1851–1867. [Google Scholar] [CrossRef] [PubMed]
- Ballesta-Ors, J.; Clua-Espuny, J.L.; Gentille-Lorente, D.I.; Lechuga-Duran, I.; Fernández-Saez, J.; Muria-Subirats, E.; Blasco-Mulet, M.; Lorman-Carbo, B.; Alegret, J.M. Results, barriers and enablers in atrial fibrillation case finding: Barriers in opportunistic atrial fibrillation case finding-a cross-sectional study. Fam. Pr. 2020. [Google Scholar] [CrossRef]
- Reinke, F.; Bettin, M.; Ross, L.S.; Kochhäuser, S.; Kleffner, I.; Ritter, M.; Minnerup, J.; Dechering, D.; Eckardt, L.; Dittrich, R. Refinement of detecting atrial fibrillation in stroke patients: Results from the TRACK-AF Study. Eur. J. Neurol. 2018, 25, 631–636. [Google Scholar] [CrossRef]
- Chan, N.-Y. Systematic Screening for Atrial Fibrillation in the Community: Evidence and Obstacles. Arrhythmia Electrophysiol. Rev. 2018, 7, 39–42. [Google Scholar] [CrossRef]
- Lowres, N.; Olivier, J.; Chao, T.-F.; Chen, S.-A.; Chen, Y.; Diederichsen, A.; Fitzmaurice, D.A.; Gomez-Doblas, J.J.; Harbison, J.; Healey, J.S.; et al. Estimated stroke risk, yield, and number needed to screen for atrial fibrillation detected through single time screening: A multicountry patient-level meta-analysis of 141,220 screened individuals. PLoS Med. 2019, 16, e1002903. [Google Scholar] [CrossRef] [Green Version]
- Lip, G.Y.; Banerjee, A.; Boriani, G.; Chiang, C.-E.; Fargo, R.; Freedman, B.; Lane, D.A.; Ruff, C.; Turakhia, M.; Werring, D.; et al. Antithrombotic Therapy for Atrial Fibrillation. Chest 2018, 154, 1121–1201. [Google Scholar] [CrossRef] [Green Version]
- Vermond, R.A.; Geelhoed, B.; Verweij, N.; Tieleman, R.G.; Van Der Harst, P.; Hillege, H.L.; Van Gilst, W.H.; Van Gelder, I.C.; Rienstra, M. Incidence of Atrial Fibrillation and Relationship With Cardiovascular Events, Heart Failure, and Mortality. J. Am. Coll. Cardiol. 2015, 66, 1000–1007. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Einarson, T.R.; Acs, A.; Ludwig, C.; Panton, U.H. Prevalence of cardiovascular disease in type 2 diabetes: A systematic literature review of scientific evidence from across the world in 2007–2017. Cardiovasc. Diabetol. 2018, 17, 83. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Bernet, W.; Gregory, N.; Öngider; Reay, K.M.; Rohner, R.P. An Objective Measure of Splitting in Parental Alienation: The Parental Acceptance-Rejection Questionnaire. J. Forensic Sci. 2017, 63, 776–783. [Google Scholar] [CrossRef] [PubMed]
- Pallisgaard, J.L.; Schjerning, A.-M.; Lindhardt, T.B.; Procida, K.; Hansen, M.L.; Torp-Pedersen, C.; Gislason, G. Risk of atrial fibrillation in diabetes mellitus: A nationwide cohort study. Eur. J. Prev. Cardiol. 2015, 23, 621–627. [Google Scholar] [CrossRef] [PubMed]
- Tadic, M.; Cuspidi, C. Type 2 diabetes mellitus and atrial fibrillation: From mechanisms to clinical practice. Arch. Cardiovasc. Dis. 2015, 108, 269–276. [Google Scholar] [CrossRef] [Green Version]
- Docherty, K.F.; Shen, L.; Castagno, D.; Petrie, M.C.; Abraham, W.T.; Böhm, M.; Desai, A.S.; Dickstein, K.; Køber, L.V.; Packer, M.; et al. Relationship between heart rate and outcomes in patients in sinus rhythm or atrial fibrillation with heart failure and reduced ejection fraction. Eur. J. Hear. Fail. 2020, 22, 528–538. [Google Scholar] [CrossRef]
- Holmqvist, F.; Kim, S.; Steinberg, B.A.; Reiffel, J.A.; Mahaffey, K.W.; Gersh, B.J.; Fonarow, G.C.; Naccarelli, G.V.; Chang, P.; Freeman, J.V.; et al. Heart rate is associated with progression of atrial fibrillation, independent of rhythm. Heart 2015, 101, 894–899. [Google Scholar] [CrossRef]
- Rosenberg, M.A.; Gottdiener, J.S.; Heckbert, S.R.; Mukamal, K.J. Echocardiographic diastolic parameters and risk of atrial fibrillation: The Cardiovascular Health Study. Eur. Hear. J. 2011, 33, 904–912. [Google Scholar] [CrossRef] [Green Version]
- Wang, T.J.; Parise, H.; Levy, D.; D’Agostino, R.B.; Wolf, P.; Vasan, R.S.; Benjamin, E.J. Obesity and the Risk of New-Onset Atrial Fibrillation. JAMA 2004, 292, 2471–2477. [Google Scholar] [CrossRef] [Green Version]
- Nalliah, C.J.; Sanders, P.; Kottkamp, H.; Kalman, J.M. The role of obesity in atrial fibrillation. Eur. Hear. J. 2015, 37, 1565–1572. [Google Scholar] [CrossRef]
- Magnussen, C.; Niiranen, T.; Ojeda, F.M.; Gianfagna, F.; Blankenberg, S.; Njølstad, I.; Vartiainen, E.; Sans, S.; Pasterkamp, G.; Hughes, M.; et al. Sex Differences and Similarities in Atrial Fibrillation Epidemiology, Risk Factors, and Mortality in Community Cohorts: Results From the BiomarCaRE Consortium (Biomarker for Cardiovascular Risk Assessment in Europe). Circulation 2017, 136, 1588–1597. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Wu, V.C.-C.; Wu, M.; Aboyans, V.; Chang, S.-H.; Chen, S.-W.; Chen, M.-C.; Wang, C.-L.; Hsieh, I.-C.; Chu, P.-H.; Lin, Y.-S. Female sex as a risk factor for ischaemic stroke varies with age in patients with atrial fibrillation. Heart 2019, 106, 534–540. [Google Scholar] [CrossRef] [PubMed]
- Kaplan, R.M.; Koehler, J.; Ziegler, P.D.; Sarkar, S.; Zweibel, S.; Passman, R.S. Stroke Risk as a Function of Atrial Fibrillation Duration and CHA 2 DS 2 -VASc Score. Circulation 2019, 140, 1639–1646. [Google Scholar] [CrossRef]
- Morillas, P.; Pallares, V.; Rubio, L.F.; Llisterri, J.L.; Sebastián, M.E.; Gómez, M.; Castilla, E.; Camarasa, R.; Sandín, M.; García-Honrubia, A. La puntuación CHADS2 como predictor de riesgo de ictus en ausencia de fibrilación auricular en pacientes hipertensos de 65 o más años. Rev. Española de Cardiol. 2015, 68, 485–491. [Google Scholar] [CrossRef]
- Linker, D.T.; Murphy, T.B.; Mokdad, A.H. Selective screening for atrial fibrillation using multivariable risk models. Heart 2018, 104, 1492–1499. [Google Scholar] [CrossRef]
- Wilke, T.; Groth, A.; Müller, S.; Pfannkuche, M.; Verheyen, F.; Linder, R.; Maywald, U.; Bauersachs, R.; Breithardt, G. Incidence and prevalence of atrial fibrillation: An analysis based on 8.3 million patients. Europace. 2012, 15, 486–493. [Google Scholar] [CrossRef]
- Zungsontiporn, N.; Link, M.S. Newer technologies for detection of atrial fibrillation. BMJ 2018, 363, k3946. [Google Scholar] [CrossRef]


{kind=link}
| No AF a | AF a | pb | |
|---|---|---|---|
| N (%) | 7809 (94.8%) | 428 (5.2%) | <0.001 |
| Average time tracking (years) ( ± ds c) | 4.89 ± 0.71 | 4.61 ± 1.08 | <0.001 |
| Age (years) ( ± ds) | 77.83 ± 12.01 | 81.36 ± 8.59 | <0.001 |
| Women n (%) | 3856 (49.4%) | 178 (41.6%) | 0.001 |
| Weight (kg) ( ± ds) | 81.04 ± 16.18 | 84.15 ± 16.98 | 0.005 |
| BMI d (kg/m2) ( ± ds) | 31.10 ± 5.62 | 32.12 ± 5.77 | 0.010 |
| Systolic blood pressure (mmHg) ( ± ds) | 138.87 ± 14.32 | 140.02 ± 14.66 | 0.127 |
| Diastolic blood pressure (mmHg) ( ± ds) | 76.23 ± 8.65 | 74.71 ± 8.9 | 0.001 |
| Hypercholesterolemia n (%) | 2237 (28.6%) | 128 (29.9%) | 0.583 |
| Heart rate (bpm) | 75.70 ± 11.45 | 72.44 ± 10.77 | 0.001 |
| HbA1c e n (%) | 7.09 ± 1.26 | 6.95 ± 1.07 | 0.035 |
| Myocardial infarction n (%) | 185 (2.4%) | 6 (1.4%) | 0.247 |
| Peripheral vascular disease n (%) | 323 (4.1%) | 29 (6.8%) | 0.013 |
| Valvular disease n (%) | 232 (3%) | 22 (5.1%) | 0.02 |
| Heart failure n (%) | 186 (2.4%) | 9 (2.1%) | 0.87 |
| Thromboembolism n (%) | 73 (0.9%) | 1 (0.2%) | 0.185 |
| CHA2DS2VASc f ( ± ds) | 4.03 ± 0.99 | 4.26 ± 0.83 | 0.005 |
| Chronic renal insufficiency n (%) | 249 (3.2%) | 20 (4.7%) | 0.094 |
| Dementia n (%) | 203 (2.6%) | 7 (1.6%) | 0.278 |
| Insulin n (%) | 1221 (15.6%) | 76 (17.8%) | 0.246 |
| Oral antidiabetic’s n (%) | 5164 (66.1%) | 338 (79%) | <0.001 |
| Beta-blockers n (%) | 1383 (17.7%) | 112 (26.2%) | <0.001 |
| Calcium antagonist’s n (%) | 1511 (19.3%) | 124 (29%) | <0.001 |
| ACE inhibitors-ARBs g (%) | 5188 (66.4%) | 353 (82.5%) | <0.001 |
| Diuretics n (%) | 1961 (25.1%) | 154 (36%) | <0.001 |
| CHA₂DS₂VASc | Number of Patients | Number of AF | ID a Total (95% Confidence Interval, CI) | ID Men | ID Women | pb |
|---|---|---|---|---|---|---|
| 0 | 0 | 0 | 0 | 0 | 0 | |
| 1 | 0 | 8 | 0 | 0 | 0 | |
| 2 | 693 | 6 | 2.31(1.0–4.26) | 2.31 | 0 | |
| 3 | 1533 | 62 | 8.21 (6.30–10.53) | 10.8 | 1.05 | <0.001 |
| 4 | 2988 | 183 | 12.77 (10.99–14.77) | 16.09 | 4.7 | <0.001 |
| 5 | 2792 | 161 | 12.18 (10.37–14.21) | 113.9 | 1.56 | <0.001 |
| 6 | 221 | 12 | 11.7 (6.07–20.53) | 0 | 11.7 | |
| 7 | 10 | 2 | 40 (4.84–144.50) | 0 | 40 | |
| 8 | 0 | 0 | 0 | 0 | 0 | |
| 9 | 0 | 0 | 0 | 0 | 0 |
| HR a | 95% CI b | pc | |
|---|---|---|---|
| Gender | |||
| Men | 1 | ||
| Women | 0.55 | 0.37–0.82 | 0.004 |
| Age | 1.07 | 1.05–1.09 | <0.001 |
| Weight | 1.03 | 1.02–1.04 | <0.001 |
| Heart rate | 0.98 | 0.97–0.99 | <0.001 |
| CHA₂DS₂VASc | 1.57 | 1.16–2.13 | 0.003 |
| ID a /1000/People/Years | Q1 | Q2 | Q3 | Q4 | All |
|---|---|---|---|---|---|
| MEN | |||||
| Atrial Fibrillation (95% CI) | 3.8 (2.1–6.2) | 12.4 (8.9–16.7) | 24.4 (18.6–31.4) | 37.6 (25.0–54.4) | 13.7 (11.6–16.1) |
| NNS b | 53 | 16 | 9 | 6 | 15 |
| Stroke (95% CI) | 0.3 (0.0–1.4) | 0.9 (0.2–2.6) | 1.6 (0.4–4.2) | 8.1 (3.0–17.6) | 1.3 (0.7–2.2) |
| WOMEN | |||||
| Atrial Fibrillation (95% CI) | 0.7 (0.0–3.9) | 3.3 (1.3–6.7) | 7.4 (4.5–11.5) | 19.7 (15.6–24.5) | 10.4 (8.6–12.6) |
| NNS b | 284 | 60 | 27 | 10 | 20 |
| Stroke (95% CI) | - | 0.5 (0.0–2.6) | 0.4 (0.0–2.1) | 2.7 (1.4–4.8) | 1.3 (0.7–2.2) |
| IQR c limits | ≤6.88 | ≤7.71 | ≤8.39 | >8.39 | |
| Atrial Fibrillation (95% CI) | 3.0 (1.7–4.5) | 8.9 (6.5–11.7) | 15.5 (12.3–19.3) | 22.5 (18.4–27.1) | 12.1 (10.7–13.7) |
| NNS b | 67 | 22 | 13 | 9 | 17 |
| Stroke (95% CI) | 0.2 (0.0–1.0) | 0.7 (0.2–1.9) | 1.0 (0.3–2.3) | 3.5 (2.1–5.7) | 1.3 (0.9–1.9) |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Muria-Subirats, E.; Clua-Espuny, J.L.; Ballesta-Ors, J.; Lorman-Carbo, B.; Lechuga-Duran, I.; Fernández-Saez, J.; Pla-Farnos, R.; on behalf members of AFRICAT Group. Incidence and Risk Assessment for Atrial Fibrillation at 5 Years: Hypertensive Diabetic Cohort. Int. J. Environ. Res. Public Health 2020, 17, 3491. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph17103491
Muria-Subirats E, Clua-Espuny JL, Ballesta-Ors J, Lorman-Carbo B, Lechuga-Duran I, Fernández-Saez J, Pla-Farnos R, on behalf members of AFRICAT Group. Incidence and Risk Assessment for Atrial Fibrillation at 5 Years: Hypertensive Diabetic Cohort. International Journal of Environmental Research and Public Health. 2020; 17(10):3491. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph17103491
Chicago/Turabian StyleMuria-Subirats, Eulalia, Josep Lluis Clua-Espuny, Juan Ballesta-Ors, Blanca Lorman-Carbo, Iñigo Lechuga-Duran, Jose Fernández-Saez, Roger Pla-Farnos, and on behalf members of AFRICAT Group. 2020. "Incidence and Risk Assessment for Atrial Fibrillation at 5 Years: Hypertensive Diabetic Cohort" International Journal of Environmental Research and Public Health 17, no. 10: 3491. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph17103491