2. Theoretical Background
The fact that the health affects the economic life of countries is well known. McMichael et al. [
15] stated that the health of the population should be one of the main criteria in the debate on sustainable development of countries. There is also an idea that a good health status of human capital plays an important role in terms of economic life [
16] and is a representative element of countries [
17]. This may be the main reason, why many studies dealt with the relationship between health and economic outcomes of countries [
18,
19,
20,
21]. The evidence showed that better health of population creates greater economic gains in the form of increased productivity and long-term income [
22]. Additionally, the improvements in mortality reduction may bring potential economic savings reflected in saved years of population lives [
23]. Concerning avoidable deaths of the population, the findings of a study by Alkire et al. [
24] demonstrated that the unjustified nature of these deaths results in economic losses in the form of countries’ GDP decline. All these findings clearly indicate that health outcomes have an economic impact, but it is also appropriate to focus on the economic effect of health inequalities.
First of all, it is important to clarify what health inequalities mean and what factors cause this phenomenon. A health inequality is a difference in health or in the most significant impacts on health that could potentially be influenced by policies; it is a disparity in which disadvantaged groups (such as the poor, racial/ethnic minorities, women or other) generate worse health outcomes or face a more serious health risk than more advantaged groups [
25]. These health inequalities represent unfair differences in the health status of the population and are determined by many social, socioeconomic and environmental factors that interact with each other. More and more emphasis is placed on social determinants that are the basis of health differences [
9], the importance of social determinants is also underlined by international organizations such as the WHO and the OECD that consider the health inequalities to be a serious problem [
26,
27]. Wilkinson and Marmot [
28] identified ten topics that are linked with social determinants: the social gradient, stress, early life, social exclusion, work, unemployment, social support, addiction, food and transport. On the other hand, Mackenbach et al. [
29] focused on the socioeconomic status as a factor that determines the health inequalities and the findings revealed that education, income, health-related behavior and access to health care are significant factors. There are also environmental factors of health inequalities [
30,
31], including green space that was examined by Richardson and Mitchell [
32], who dealt with gender differences in the relationship between urban green space and health indicators represented by cardiovascular disease mortality, respiratory disease mortality, self-reported limiting long-term illness and lung cancer mortality. Last but not least, the financing of health care systems can play an important role in achieving positive or less positive health outcomes [
33], while Michalski et al. [
34] recommended that non-profit organizations, including health facilities, should manage their funding with regard to efficiency in social and economic environment. In any case, funding in the health sector can be a significant factor that can contribute to improving the health status, achieving the health potential of the population, as well as reducing the health inequalities [
35,
36,
37].
All of the above-mentioned factors can cause health differences around the world. Braveman [
25] identified three basic components for measuring the health inequality: (i) an indicator of health or a modifiable determinant of health; (ii) an indicator of social position, i.e., a way of categorizing people into different groups and (iii) a method for comparing the health indicator (or health determinant) across the different social strata. Based on this, the present study includes the following selected components: (i) life expectancy, causes of mortality, avoidable mortality; (ii) gender status (males and females) and (iii) analysis of differences. The first two components are discussed in the next part of the literature review and findings.
The gender inequalities in health were examined in many studies [
38,
39,
40,
41] and the evidence revealed differences between women and men in several health indicators. Singh-Manoux et al. [
42] found excess among men in mortality and some excess among women in morbidity. There are findings that women show poorer outcomes in mobility than men [
43,
44]. Wijnhoven et al. [
45] argued that a female disadvantage in the musculoskeletal pain may be explained by sex differences in vulnerability to risk factors, i.e., overweight and older age were more associated with women, and pain catastrophizing was more common among men. With a focus on avoidable mortality, the gender inequality was confirmed in several studies [
46,
47]. The low rate of gender inequalities in avoidable mortality were confirmed by Westerling [
48], but the findings of other studies definitely revealed that men have a higher risk of death due to avoidable causes [
49,
50]. In general, male mortality is significantly higher than female mortality [
51]. This fact is evident not only in all-cause mortality, but also in terms of specific causes of mortality, namely COPD (chronic obstructive pulmonary disease), asthma, ACOS (asthma-COPD overlap syndrome) [
52,
53,
54] and cancer [
55,
56]. On the other hand, men have a lower rate of cardiovascular mortality [
57]. With regard to stroke, the research findings are debatable, women under 75 years have a lower risk of stroke compared to men [
58], but older women lose this advantage and have a higher stroke mortality, while the highest risk of stroke occurs at an older age [
59,
60]. Le et al. [
61] argued that efforts to reduce male mortality due to cancers, circulatory disease and respiratory diseases might decrease this gender gap in life expectancy. The authors also pointed out that the inequality in mortality in the 60–79 age category significantly contributes to the gender gap. Based on the results of another study, it can be concluded that life expectancy and healthy life expectancy are also shorter in men than in women, meaning that men are at greater risk of dying, they die earlier and live fewer disease- and disability-free years than women [
62]. Similar evidence was found in the research that dealt with differences in life expectancy and self-rated health. The results of this study revealed that women live longer but report poorer health than men [
63], this agrees with the findings of another study confirming that women report worse health but men’s mortality is higher [
64]. The fact that women live longer was confirmed in several studies [
61,
65]. On the other hand, other studies showed that women lived longer lives, but had more disabilities than men [
66,
67], these disabilities are reflected in a lower quality of life related to health and well-being in older life [
68]. At this point, it is necessary to refer to the findings by Oksuzyan et al. [
69], who also revealed that there are significant differences between the health status and survival of women and men. This phenomenon is called the male–female health–survival paradox. Men are physically stronger and less disabled, but have significantly higher mortality in all age categories than women. This phenomenon occurs for several reasons, including the biological differences such as immune system reactions, genetic factors, hormones and disease patterns. Differences in behavior, such as risk taking and unwillingness to seek and comply medical treatment, can also be an important reason. Another aspect is that part of the difference may be due to methodological challenges such as selective non-participation, insufficient reporting of health problems and delayed seeking of treatment in men [
69].
Based on the above-mentioned knowledge, it is possible to deepen the topic of health inequalities and focus on its association with economic prosperity. Health inequalities are well-examined, but their association with economic dimension has been investigated in few studies [
70]. Several studies were conducted in a similar field of research but with a focus on health inequalities in different socioeconomic perspectives. Concerning the health inequalities between groups with different socioeconomic status, the findings of a study by Politzer et al. [
12] confirmed a substantial economic impact of health inequalities in Israel, where the total cost of health inequalities was 0.7%-1.6% of GDP. These authors also highlighted the possible economic benefits of policies that will improve health outcomes of some groups of the population. From an economic point of view, the health inequalities were associated with high health care expenditure, social security costs and reduced labor productivity [
71]. Mackenbach et al. [
71] examined the inequalities in self-rated health and mortality in EU countries and confirmed that health inequalities are a huge economic burden in terms of the prosperity of economies. The inequality-related losses cause not only deaths, but also health care and social security costs or losses in GDP. On the other hand, the economic benefits of reducing health inequalities are reflected in economic savings [
11,
72]. Based on the above-mentioned, the health inequalities represent a huge economic burden and the efforts to close this gap have long-term potential benefits for the economy [
73].
All the above-mentioned findings confirm two essential facts: the health inequalities affect many economic aspects of the country, including GDP; and there is a considerable gender inequality in health around the world. In this respect, it is considered necessary to examine the effect of gender inequalities in health on the economic prosperity represented by GDP. The purpose of this study is to fill this gap in scientific research and to highlight the link between gender inequalities in health and the economic prosperity represented by GDP. Simultaneously, the research offers a new perspective for policy makers, who focus on economic development and are not always aware of the important role of health and health inequalities in economic life. Last but not least, the study respects all recommendations of OECD and WHO that sensitively perceive the issue of health inequalities and urge the policy makers to address this serious issue [
27]. This is despite the fact that research findings show that health inequalities are gradually decreasing [
74]. Thus, it is important to point out the economic effect of this reduction and it can be discussed whether it is more effective to reduce inequalities on the part of women or men.
3. Materials and Methods
The primary aim of the research in this study was to evaluate the relations between gender health inequalities and the economic prosperity of OECD countries. This aim was met by a series of analytical procedures that were divided into three main parts. In the first part, a descriptive analysis, an analysis of differences in selected health indicators between males and females, and an analysis of relationships between selected health indicators and economic prosperity were applied. The aim of this first part was to point out the statistical characteristics of selected variables, the existence of gender differences (inequalities) in health and also the existence of a relationship between health indicators and the indicator of economic prosperity represented by GDP. For this purpose, the following two research questions were formulated: (RQ I-a) Is there a significant difference in selected health indicators between women and men? (RQ II-a) Is there a significant relation between economic prosperity and selected health indicators in terms of gender inequality? The aim of the second part was to use a regression analysis to evaluate the significance of the effect of female health indicators, male health indicators and gender inequalities in health on the economic prosperity represented by GDP. For this purpose, the following three research questions were formulated: (RQ I-b) Is there an effect of selected female health indicators on the economic prosperity of countries? (RQ II-b) Is there an effect of selected male health indicators on the economic prosperity of countries? (RQ III-b) Is there an effect of gender inequalities in selected health indicators on the economic prosperity of countries? The third part presents the outputs of a cluster analysis in which the visualizations determine and assess groups of countries based on the evaluation of the outcomes of gender inequalities in health and the economic prosperity of OECD countries. For this purpose, the following three research questions were formulated: (RQ I-c) Are there any homogeneous groups of OECD countries in the relations of indicators evaluating the gender inequalities in life expectancy and indicators evaluating the economic prosperity? (RQ II-c) Are there any homogeneous groups of OECD countries in the relations of indicators evaluating the gender inequalities in the causes of mortality and indicators evaluating the economic prosperity? (RQ III-c) Are there any homogeneous groups of OECD countries in the relations of indicators evaluating the gender inequalities in avoidable mortality and indicators evaluating the economic prosperity?
The analyses included data from the OECD database, while the Health and Productivity sub-databases were used for collection [
8]. These databases are internationally recognized in providing relevant data on their member countries. Four categories of data were used in the analytical procedures. Three categories consisted of male and female health indicators such as a life expectancy (LE), the causes of mortality (CE) and an avoidable mortality (AM). The fourth category consisted of the indicator of economic prosperity represented by GDP in USD per capita (current PPPs). The life expectancy category included 4 age-specific variables separately expressed for women and men: life expectancy at birth—LE_1, life expectancy at age 40 years—LE_2, life expectancy at age 60 years—LE_3, life expectancy at age 65 years—LE_4 and life expectancy at age 80 years—LE_5. The value of these variables represents the average number of years that a person at that age can be expected to live, assuming that age-specific mortality levels remain constant [
75]. The category of the causes of mortality included 13 specific variables reported in deaths per 100,000 population in standardized rates and separately expressed for women and men. This category was composed of variables that reflect age-standardized death rates per 100,000 population for chosen causes that were calculated by the OECD Secretariat, using the total OECD population for 2010 as the reference population [
76]: certain infectious and parasitic diseases—CM_1, neoplasms—CM_2, blood diseases and blood forming organs—CM_3, endocrine nutritional and metabolic diseases—CM_4, mental and behavioral disorders—CM_5, diseases of the nervous system—CM_6, diseases of the circulatory system—CM_7, diseases of the respiratory system—CM_8, diseases of the digestive system—CM_9, skin and subcutaneous tissue diseases—CM_10, diseases of the musculoskeletal system and connective tissue—CM_11, diseases of the genitourinary system—CM_12 and certain conditions originating in the perinatal period—CM_13. The third health category of avoidable mortality consisted of two variables separately expressed for women and men, namely: preventable mortality—AM_1 and treatable mortality—AM_2. Both indicators refer to premature mortality under age 75. The preventable mortality is defined as causes of death that can be mainly avoided through effective public health and primary prevention interventions (i.e., before the onset of diseases/injuries, to reduce incidence). The treatable (or amenable) mortality expresses the causes of death that can be mainly avoided through timely and effective health care interventions, including secondary prevention such as screening, and treatment (i.e., after the onset of diseases, to reduce case-fatality) [
77]. The economic prosperity was examined through GDP in USD per capita (current PPPs). All OECD countries were included in the analytical processes: Australia (AUS), Austria (AUT), Belgium (BEL), Canada (CAN), Czech Republic (CZE), Denmark (DNK), Estonia (EST), Finland (FIN), France (FRA), Germany (DEU), Greece (GRC), Hungary (HUN), Chile (CHL), Iceland (ISL), Ireland (IRL), Israel (ISR), Italy (ITA), Japan (JPN), Korea (KOR), Latvia (LVA), Lithuania (LTU), Luxembourg (LUX), Mexico (MEX), Netherlands (NDL), New Zealand (NZL), Norway (NOR), Poland (POL), Portugal (POR), Slovak Republic (SVK), Slovenia (SVN), Spain (ESP), Sweden (SWE), Switzerland (CHE), Turkey (TUR), United Kingdom (GBR) and United States (USA). The most recent data was from 2016 and the oldest since 2010, the time range was adapted to the large number of missing data. In some observations, the OECD reports limitations such as i—break (for LE and CM), ii—difference in methodology (for CM and AM—Turkey) or iii—provisional value (for LE); this was the number of observations that could not significantly affect the results.
In order to fulfill the main objective, the whole analytical process was decomposed into three sections. The content of the first part was a descriptive analysis showing the basic statistical characteristics of analyzed variables, i.e., central tendencies, variability and location. Subsequently, a difference analysis was used to examine the presence of differences in health indicators between women and men. For this purpose, the normality was tested by the Shapiro–Wilk normality test (SW). The Wilcoxon test (W) was also used as a non-parametric test of the difference of two independent samples. The content of the second part was a regression analysis, in which the health indicators in the specification of men, women and gender inequalities were used as independent variables. The gender differences were expressed in absolute values. The regression analysis was preceded by the selection of the most appropriate model based on testing of assumptions. The F test for individual and/or time effects was used to test the significance of the time series effects. The Bonferroni outlier test [
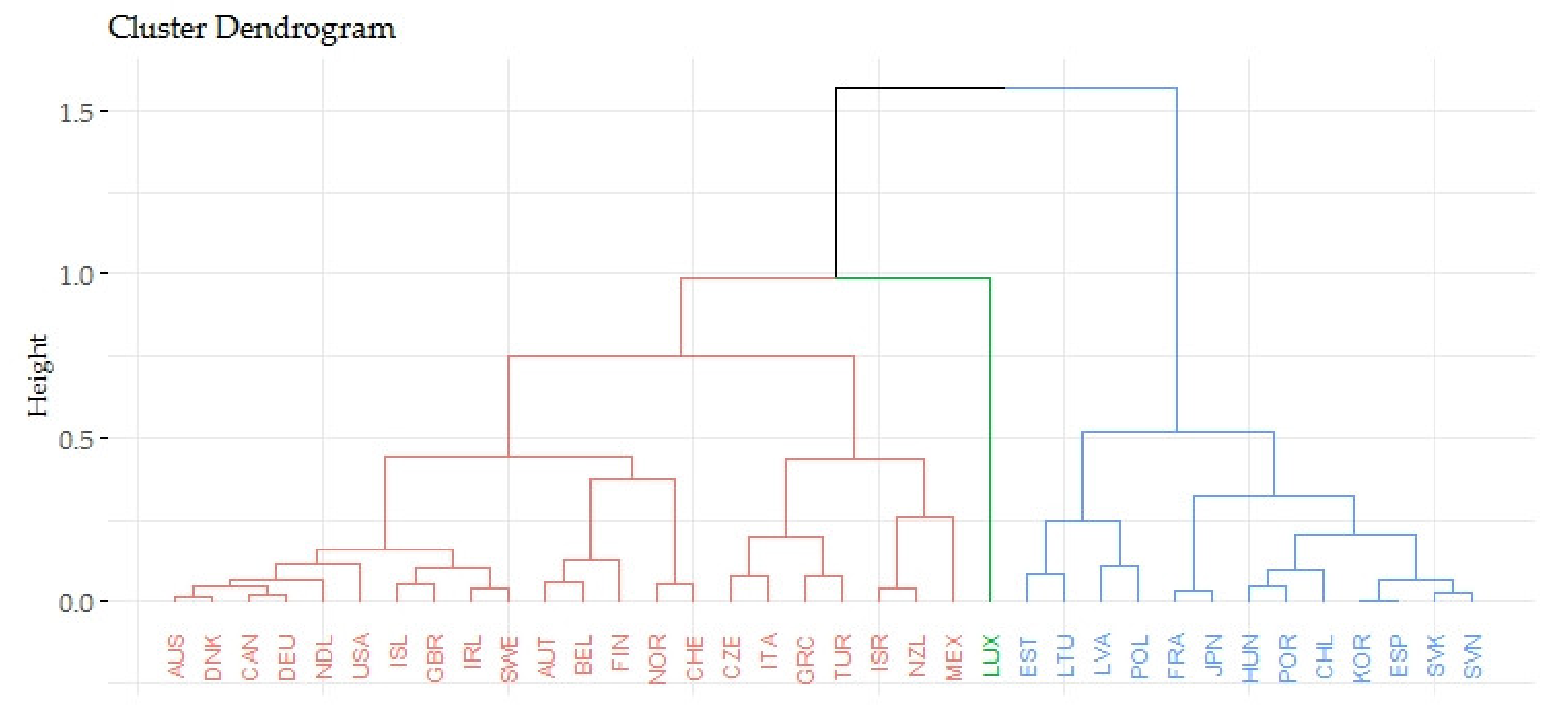
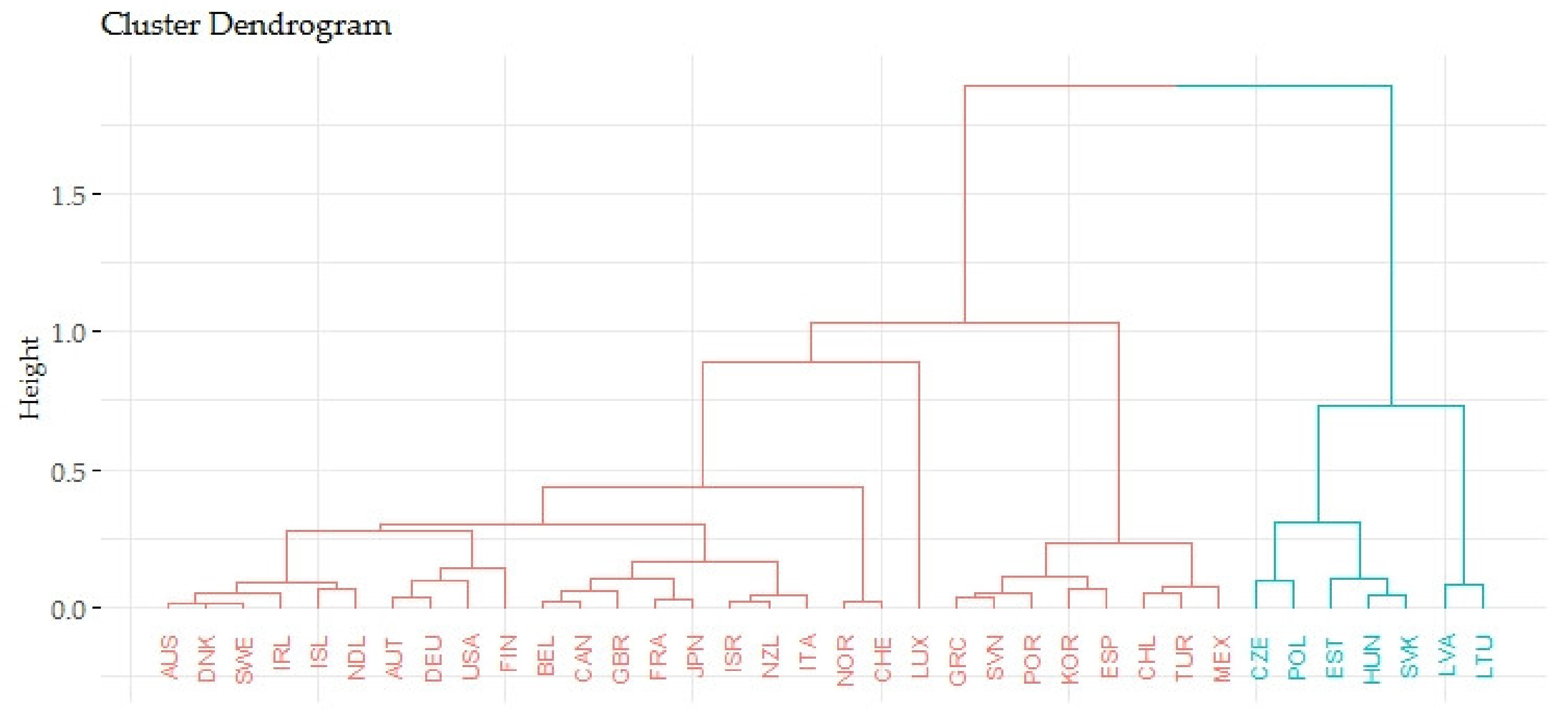
78] was used to test the presence of significant outliers. The variance inflation factors (VIF) method was applied to consider multicollinearity. The Breusch–Pagan test was applied to test the homogeneity of variability of residuals (homoscedasticity). The content of the third part was an analysis of impact that was carried out at two levels. The first was a multiple regression, followed by a simple regression as the second, while the panel models, the fixed and random effect model, and the Arrelano and White 1 methods were used to estimate the coefficients in the case of significant heteroscedasticity. The content of the last part was a cluster analysis (agglomerative hierarchical clustering), in which the selected indicators of gender health inequalities and economic prosperity (represented by GDP) were used. In the first step, these data were adjusted by the median for all years (2010–2016). Subsequently, the data were standardized. The standardization of the data had an output from 0 to 1, where 0 was the most negative value and 1 was the most positive value of the evaluation. After the standardization, the data were adjusted by the mean in each specific group of indicators and four new variables were created: three indicators evaluating the gender health inequalities (LE_eval, CM_eval and AM_eval) and one indicator evaluating the economic prosperity (GDPpc_eval). The quasi-optimal number of clusters was estimated using the Silhouette method (for average silhouette width). Based on the highest value of the agglomerative coefficient, the Ward’s method was used to estimate the clusters themselves. Dendrogram and two-dimensional cluster charts were used to visualize the individual clusters. The analytical data were processed in programming language R v. 3.6.2 in R Studio (RStudio, Inc., Boston, MA, U.S.) and the libraries such as lmtest, car, sandwich, plm, cluster, fclust and ggplo2 were used.
5. Discussion
Health of the population is a very valuable economic commodity of each country. For this reason, the health is an important source of comparative economic [
7]. Therefore, it is not surprising that many authors emphasized the importance of health in the economic dimension [
15,
18,
19,
21,
79]. On this basis, it can be considered that the efforts leading to better population health contribute to creating richer economies [
20]. The fact is that the population is aging, a very interesting idea is offered by Dziuba et al. [
80], who examined the use of modern digital technologies by the older generation, which can favorably prolong their life activities and make everyday life easier. Developed economies are interested in achieving the health potential of all groups of the population and therefore the policy makers should be focused on the inequalities in health outcomes. The health inequality is also an important element for assessing the countries [
9,
29]. The gender inequalities in health have been examined in several studies and the results revealed the differences between women and men in many health indicators reflecting morbidity or mortality [
41,
42]. The present study highlights the health in economic dimension and evaluates the relations between gender inequalities in health and the prosperity of economies.
In the first step of the analytical process, a descriptive analysis, a difference analysis and a relationship analysis were used. The output of descriptive analysis revealed that the most frequent causes of mortality were neoplasms (CM_2) and diseases of the circulatory system (CM_7). As evidenced by the research findings in many other studies [
38,
39,
40], this study also confirmed the gender inequalities in health. In the vast majority of analyzed health indicators, including a life expectancy, the causes of mortality and an avoidable mortality, there was a significant difference between men and women. In most of the indicators, more positive health outcomes were identified in women, thus it could be assumed that women were healthier in terms of selected indicators. A significant disadvantage of men was evident in mortality due to neoplasms (CM_2), while Ellison [
56] emphasized that male mortality is higher in 13 of the 18 types of cancer. The results showed that women lived longer and men died earlier and this is in accordance with the findings of several international studies [
51,
61,
62,
65] and the studies focused on the specific areas of causes of mortality [
52,
53,
54,
55]. In terms of the avoidable mortality, the results are in line with the findings of other studies by Lefevre et al. [
49] and de Abreu et al. [
50]. The only health indicator of more positive results in men was CM_11, diseases of the musculoskeletal system and connective tissue, and this result agreed with the fact that women have a disadvantage in musculoskeletal pain and mobility [
43,
44,
45]. From the point of view of the relationship analysis, it could be concluded that there was a significant relationship between the vast majority of health indicators and the economic prosperity represented by GDP.
In the next step of the analysis, a multiple regression analysis was used to assess the effect of selected health indicators (LE, CM and AM) on the prosperity of economies. Thus, three separate regression models were created. Each model was specific to one group of health indicators used as independent variables. The effect of male and female health indicators was evident, in general, it could be confirmed that the better the health indicators, the higher economic prosperity was expected and vice versa. These results may be supported by other claims that poor health outcomes are reflected in economic losses [
24,
81] and better health outcomes bring economic benefits [
22,
23]. Other results revealed a significant effect of gender inequalities in life expectancy at birth (LE_1) on the economic prosperity represented by GDP. A negative coefficient indicates that if the gender inequality is decreased in LE_1, the economic prosperity is expected to increase. It can be discussed whether it is more effective to reduce the inequalities on the part of women or men. The effect of life expectancy at birth on the economic prosperity was significant for both men and women, but the effect of men was statistically more significant. Based on this, it could be assumed that men are more productive, and therefore the efforts to increase life expectancy at birth of men would be more effective in terms of the economic prosperity. Regarding the gender inequalities in the causes of mortality, a significant effect on the economic prosperity was confirmed for two indicators, i.e., neoplasms (CM_2) and diseases of the circulatory system (CM_7). Both variables had a negative coefficient, thus if the gender inequality in these indicators decreases, an increase of the economic prosperity is expected. Based on the significance of the male and female coefficients, the results showed that the initiatives aimed at reducing the gender inequalities in mortality from neoplasms (CM_2) seem to be more effective on the part of men than women. In terms of gender inequalities in avoidable mortality, a significant effect on the economic prosperity was confirmed in preventable mortality (AM_1). Based on a negative coefficient, it could be concluded that if the gender inequality is decreased in AM_1, the economic prosperity is expected to increase. When assessing the significance of the effects of men and women, it could be considered that efforts to reduce the gender inequalities in preventable mortality should focus on men who showed a more significant coefficient. These findings confirmed the importance of efforts to close the gender gap in health in order to achieve economic gains. Similar results were found in the socioeconomic, racial and ethnic dimensions [
11,
12,
71,
72].
In the last part of the regression analysis, a simple regression model was used, in which the indicator of economic prosperity was used as a dependent variable and all health indicators in the specification of men, women and gender inequalities were used as independent variables. The univariate view of the effect of selected health indicators on the economic prosperity revealed that most health indicators in the specification of gender inequalities showed a significant effect on the prosperity of economies. The most significant effects were found in variables: life expectancy at birth (LE_1), neoplasms (CM_2), diseases of the circulatory system (CM_7), preventable mortality (AM_1) and treatable mortality (AM_2). All these health variables had a negative β coefficient. Thus, if the gender inequality in health decreases, the economic prosperity is expected to increase. In terms of the prosperity of economies, the efforts to reduce the negative values of these health indicators seem to be more effective on the part of men than women.
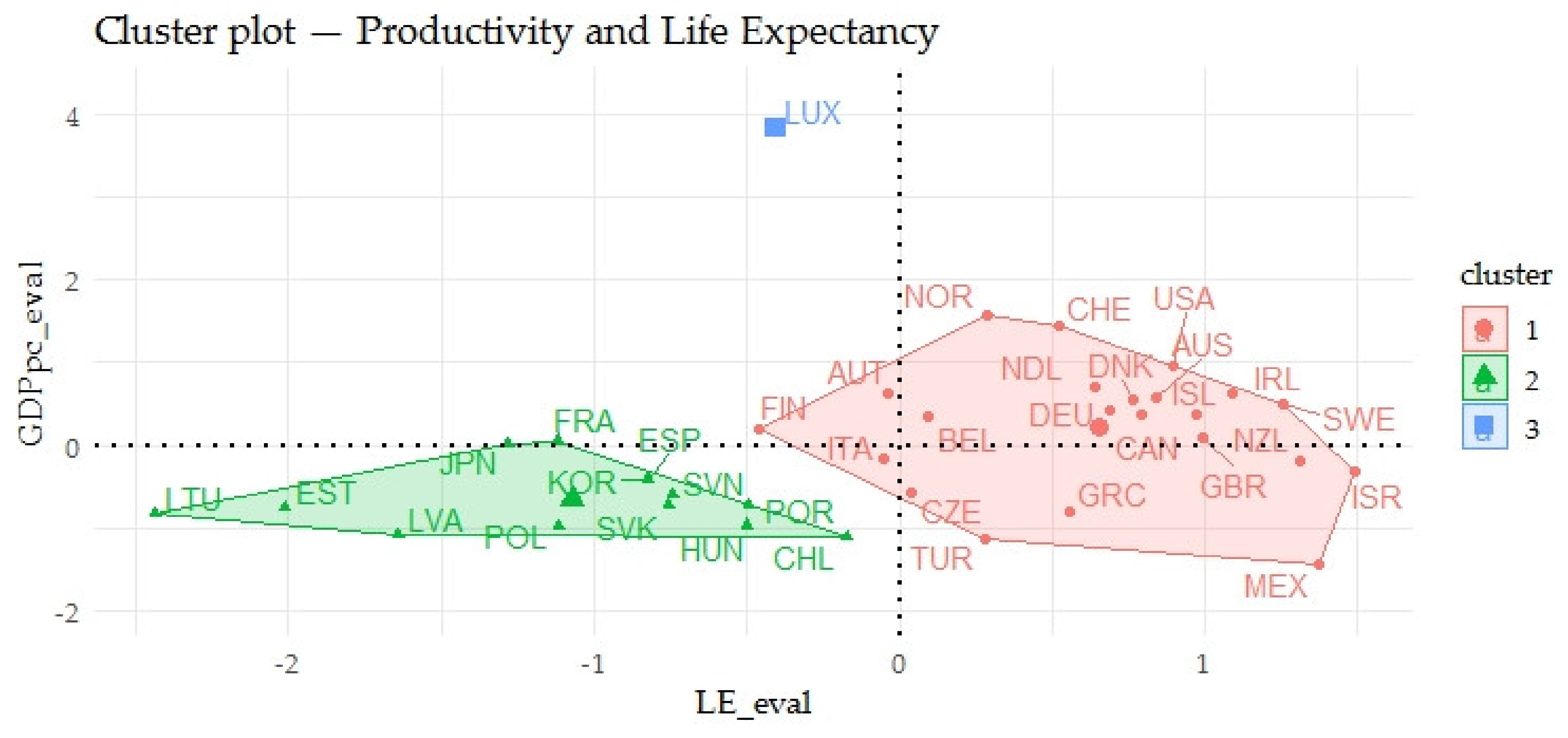
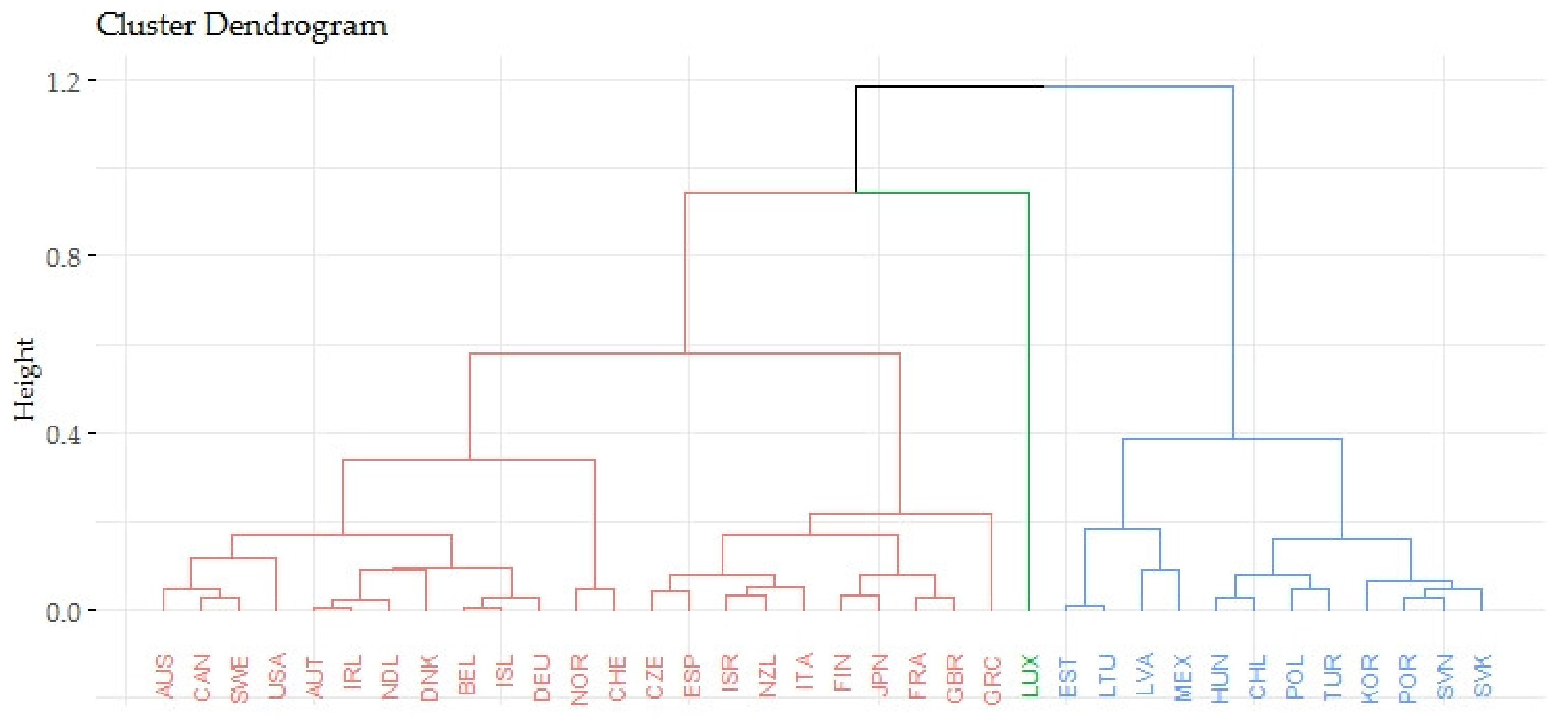
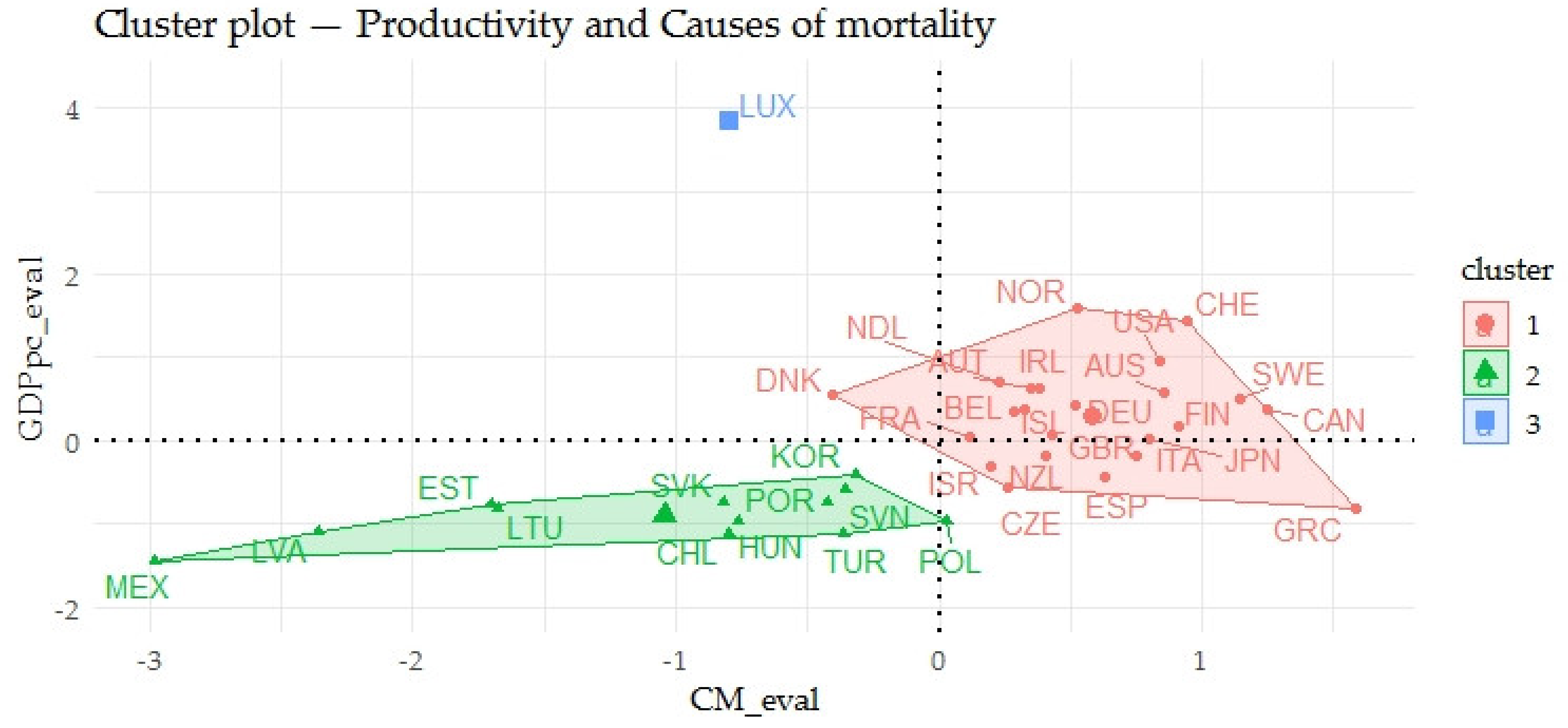
The last part of the analyses included the assessment of countries in terms of the links of the indicators evaluating the gender inequalities in health and indicators evaluating the economic prosperity of countries. Focusing on the indicators evaluating the gender inequalities in life expectancy (LE_eval) and indicators evaluating the prosperity of economies (GDPpc_eval), the OECD countries were divided into three clusters. From the point of view of these indicators, the Baltic countries such as Lithuania, Latvia and Estonia showed very negative outputs of the evaluation and Norway, Switzerland or the USA showed very positive outputs. With a focus on the links of the indicators evaluating the gender inequalities in the causes of mortality (CM_eval) and indicators evaluating the prosperity of economies (GDPpc_eval), the OECD countries were divided into three clusters. It can be concluded that Mexico and Latvia showed very negative outputs of the evaluation and the countries such as Norway, Switzerland or the USA showed very positive outputs. In the assessment of the relations of the indicators evaluating the gender inequalities in avoidable mortality (AM_eval) and those evaluating the prosperity of economies (GPPpc_eval), the OECD countries were divided into two clusters. In this evaluation, it can also be stated that Lithuania, Latvia and Estonia showed very negative outputs and the countries such as Luxembourg, Norway, Switzerland or the USA showed very positive outputs.
The application of cluster analysis pointed to individual countries that were identified in positive or negative optics in terms of the indicators evaluating the gender inequalities in health and those evaluating the prosperity of economies. It should be noted that most countries were identified in positive optics. The increased attention should be paid to countries such as Lithuania, Latvia, Estonia, Poland, Hungary or Slovakia in reducing regional disparities in this issue.
Based on the above-mentioned findings, it can be concluded the presence of gender inequalities in health between the selected developed countries. These findings support the recommendations of the OECD and the WHO, which urge the policy makers to address this serious issue in the field of health. At this point, it can be underlined that health inequalities are the result of many social, economic and environmental factors [
9,
29,
30,
32,
36]. Therefore, the public policies should address this global health problem from different perspectives and use all available tools to reduce these inequalities. These tools can be effective financing of health, health accessibility, quality health care, social protection, education support, as well as increasing the well-being of the population. All these tools should be focused on the population as a whole, but disadvantaged groups are at the greatest health risk. In general, more developed countries are supposed to have effective health care systems that are able to achieve the equity in health, but there are clear differences between population groups. Health inequalities can be considered as a defect in the health systems and it encourages the idea that the gender inequalities in health are an issue to be examined. The importance of this topic is highlighted by the findings of this study that confirmed the effect of gender inequalities on the economic prosperity. One of the main aims of public policies is to increase the economic prosperity of countries, therefore the policy makers should focus on the reduction of gender inequalities in health. The findings of the present research gave to the decision makers an additional information source to achieve economic gains. From this point of view, it could be recommended the reduction of gender inequalities on the part of men in terms of an effective increase of economic prosperity. These political implications represent a significant added value of the present study. In general, it can be assumed that reducing health inequalities between different groups of the population can bring various economic benefits. On this basis, it can be stated that the issue of health inequalities seems to be overlooked in countries, and the policy makers are not aware of the importance of health inequalities in terms of their economic effects. This study shows that the policy efforts to reduce health inequalities are beneficial not only in the life of the individual but also in the economic life. This could be a driving force for improving the health systems and improving the distribution of health care in developed countries, with the most pronounced effect expected for disadvantaged groups.
6. Conclusions
As the evidence shows, the health of the population is a representative element of the country and at the same time health has a significant effect on the prosperity of economies. Therefore, it is necessary to emphasize the health and economic outcomes of individual countries. The health inequalities are the results of the specificity of countries, their geographical location, social or economic aspects. On the other hand, the strategic policies of countries have a major impact on reducing or deepening the inequalities. Based on this, the policy makers should carefully assess the indicators of health and the inequalities in health, while these indicators should definitely not be missing in assessing the economic prosperity of countries. For this reason, this study is focused on analyzing the gender inequality in health and the economic prosperity represented by GDP.
The primary aim of the research in this study was to evaluate the relations between gender health inequalities and the economic prosperity of OECD countries. This purpose was decomposed into several research questions that are mentioned in the methodological part of this study. Based on the results of several analytical processes, the relationship between the health of the population and the prosperity of economies can be confirmed. The main purpose of the research was to prove the effect of selected health indicators (in the specification of men, women and gender inequalities) on the economic prosperity represented by GDP. In several cases, the significant effects were confirmed and it could be concluded that the main objective was met. Based on the research findings, it could be emphasized that the health policies should be more focused on reducing gender health inequalities on the part of men, in order to effectively increase the economic prosperity represented by the GDP. In general, it was also concluded that the effect of specific areas of causes of mortality could be explained by their frequency. As the indicators of avoidable mortality fundamentally affected the prosperity of economies, the policy makers should be interested in this issue and should take the necessary activities to reduce the avoidable mortality. Despite the fact that the reduction of regional health disparities is a proclaimed issue in both scientific and applied discussions, it can be stated that the significant gender differences were identified between OECD countries. Therefore, the health policies should be more proactive in order to reduce this gender inequality in health.
A potential limitation of this study might be a fact that the collected data represent the economically developed countries (OECD) and the findings could be generalized only to similar countries. Due to the high frequency of missing data since 2017, the comprehensive time series offered by the database did not enter the analysis. The lower bound was chosen with the respect to the effect of time; the larger the time series, the higher the likelihood of hidden effects. The sample size is considered adequate to support the formulated conclusions.
This study mapped the health areas, while future research will focus on analyzing the specific diagnoses and their effect on economic prosperity in terms of socioeconomic inequality. Future research will also focus on comparing countries with different level of economic development. Last but not least, future research will reveal the effect of health indicators on economic parameters other than the prosperity of countries.









{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}