A New Decision Model Approach for Health Technology Assessment and a Case Study for Dialysis Alternatives in Turkey


Abstract
:1. Introduction
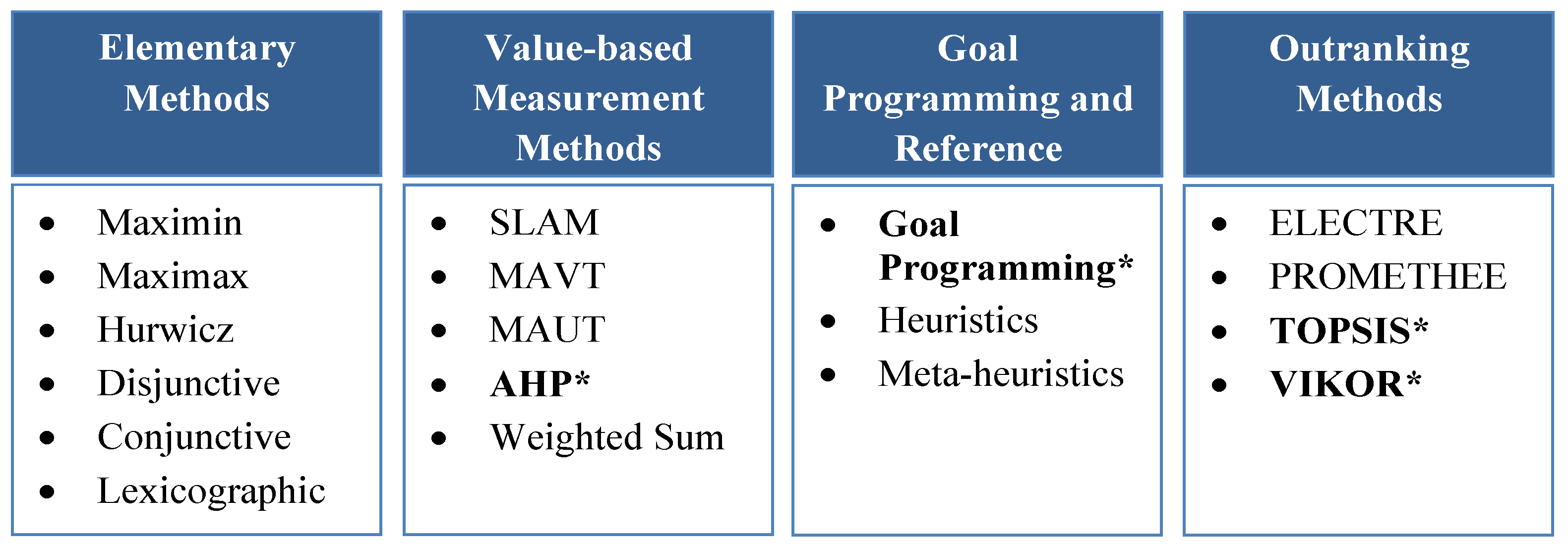
1.1. MCDA and Methods Used in Healthcare
1.1.1. The Analytic Hierarchy Process
1.1.2. Technique for Order Preference by Similarity to Ideal Solution (TOPSIS)
1.1.3. Vise Kriterijumska Optimizacija I Kompromisno Resenje (VIKOR)
1.1.4. Goal Programming
1.1.5. Fuzzy Set Theory and Fuzzy Methods
1.2. MCDA Applications for HTA
1.2.1. EVIDEM Framework
1.2.2. Bariatric Surgery Selection
2. Materials and Methods
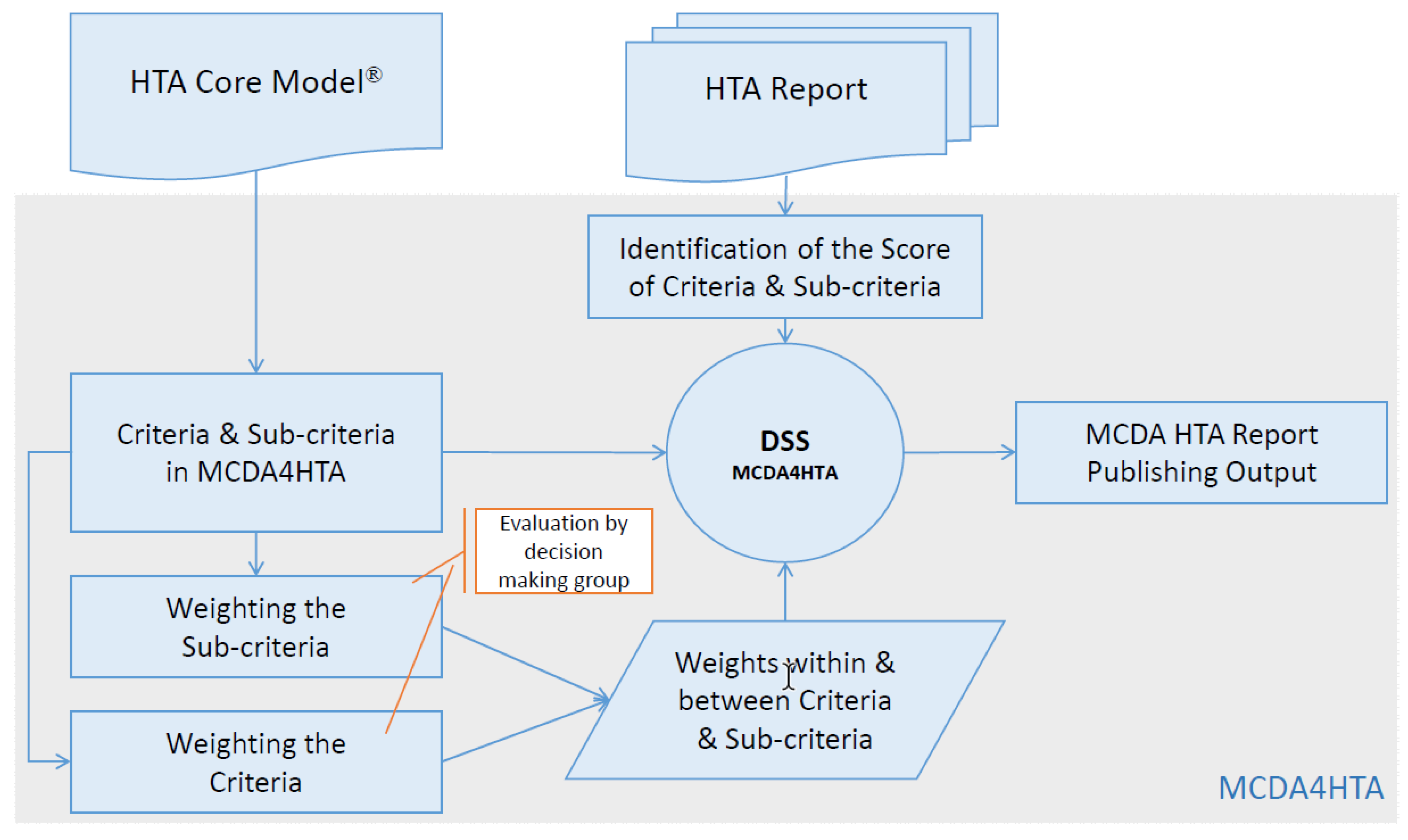
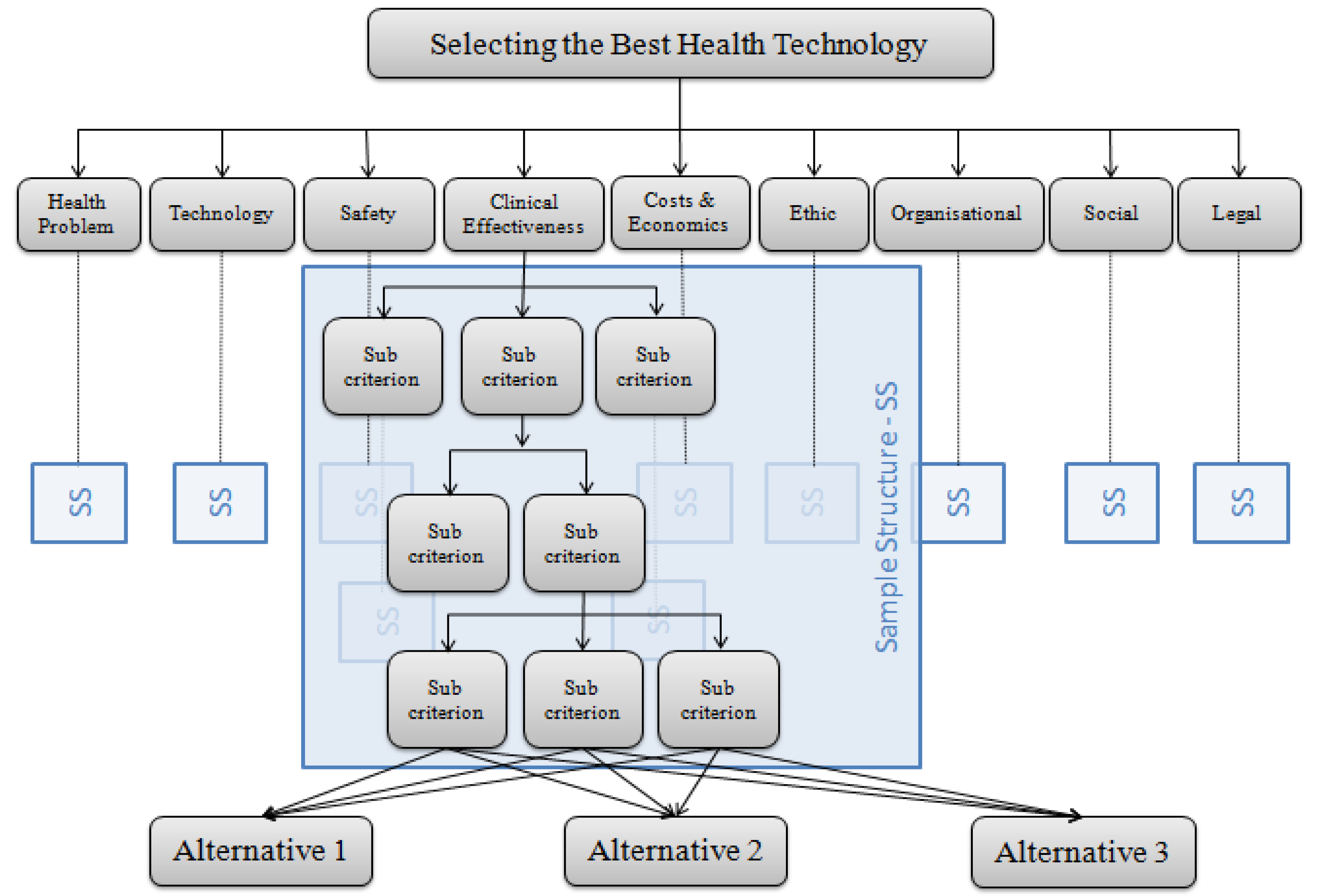
2.1. Description of MCDA4HTA
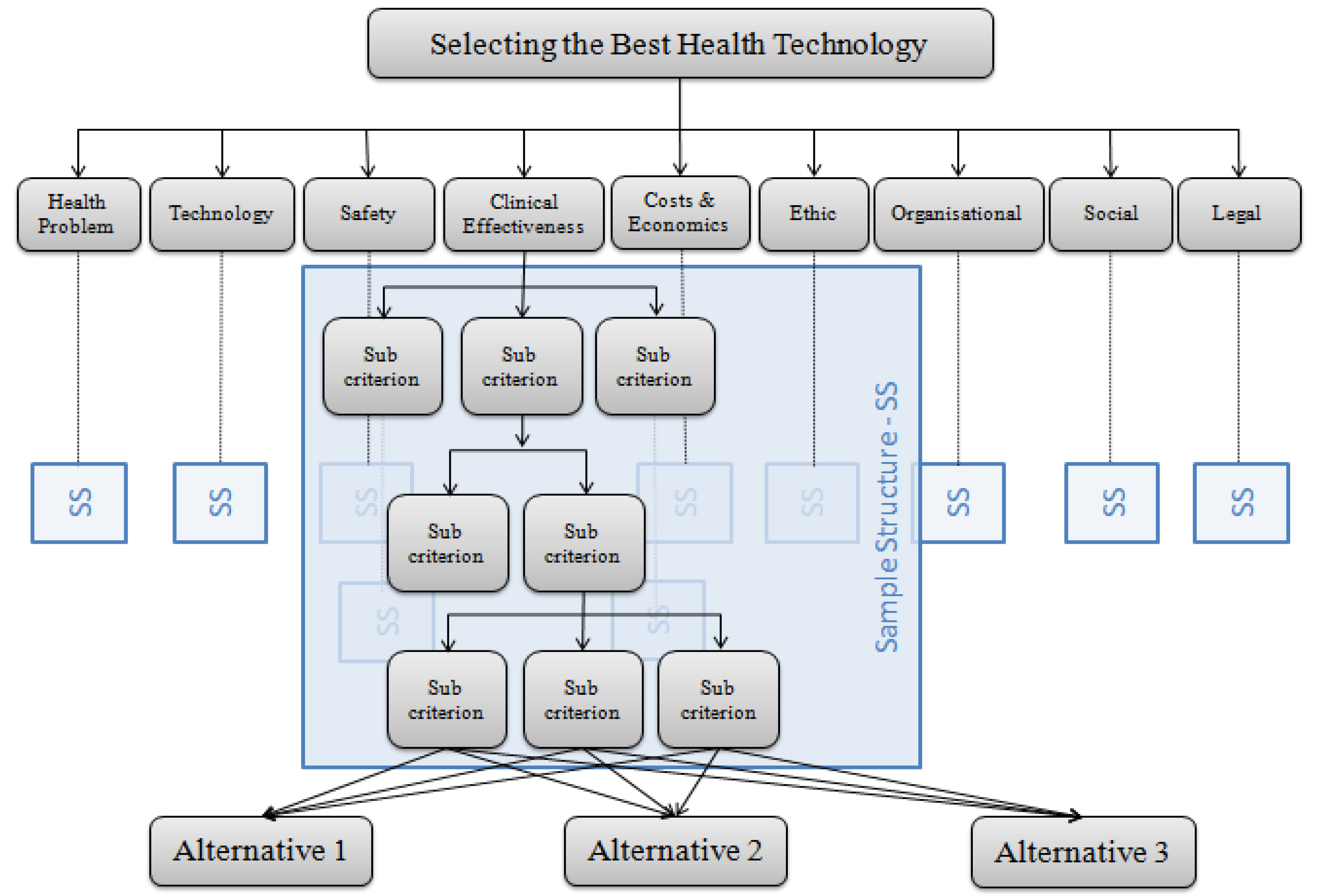
2.1.1. Structure of MCDA4HTA
2.1.2. Defining the Weight of Criteria
2.1.3. Defining the Scores of Criteria
2.2. Decision Support Systems and DEMATSEL
2.3. Application of MCDA4HTA in HTA
3. Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
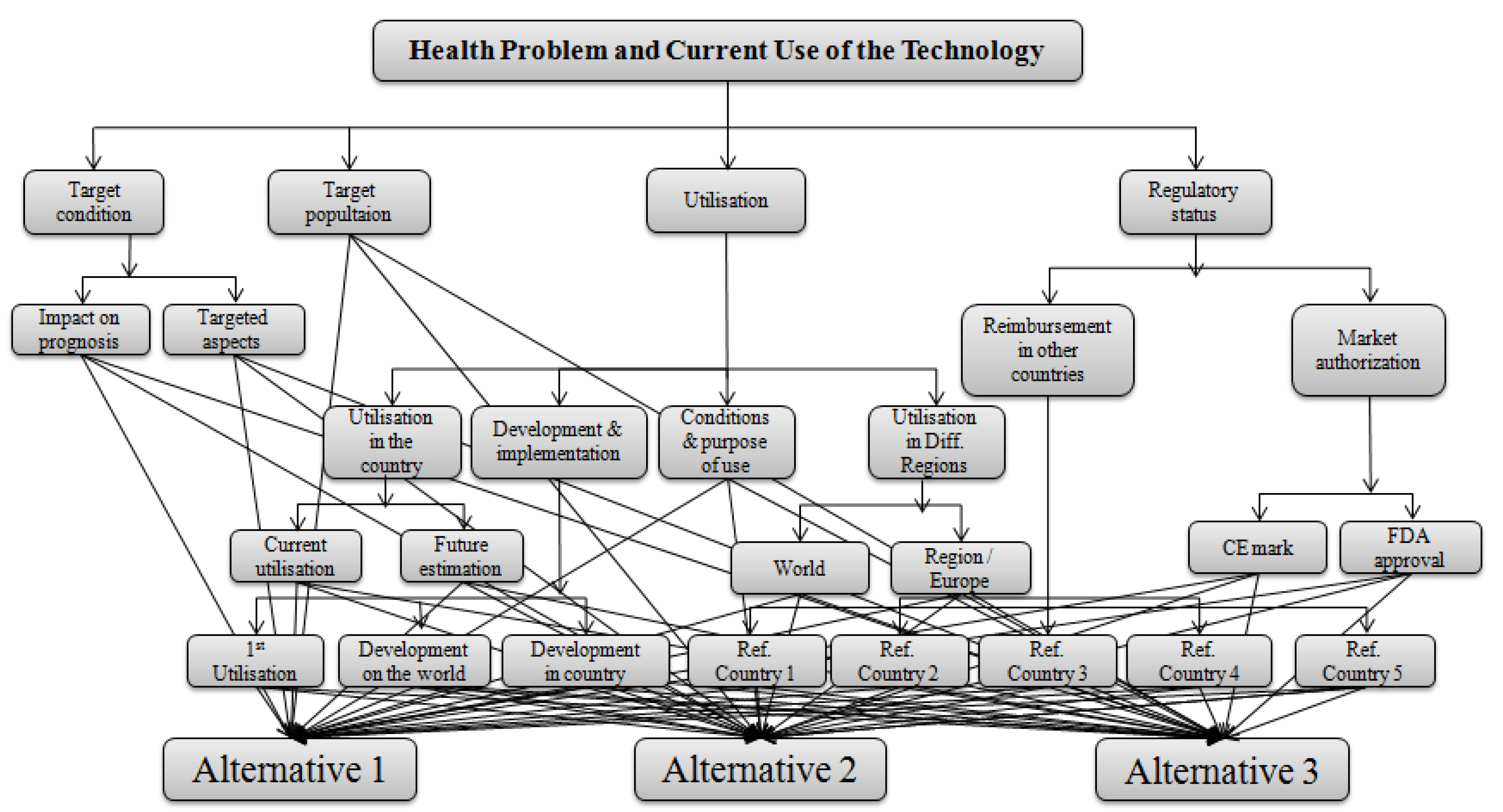
Appendix A. Hierarchical Structure of the Main Criteria
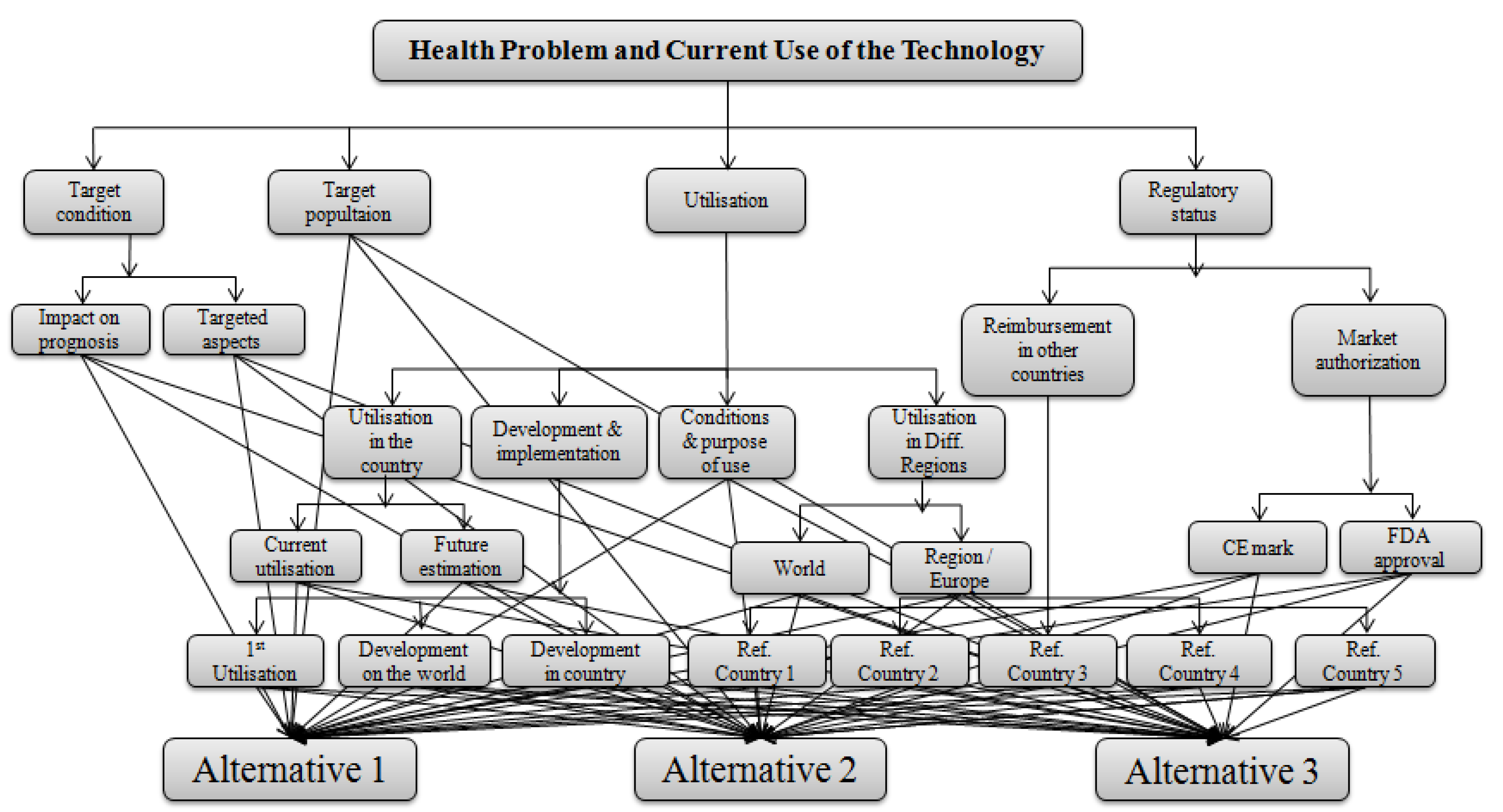
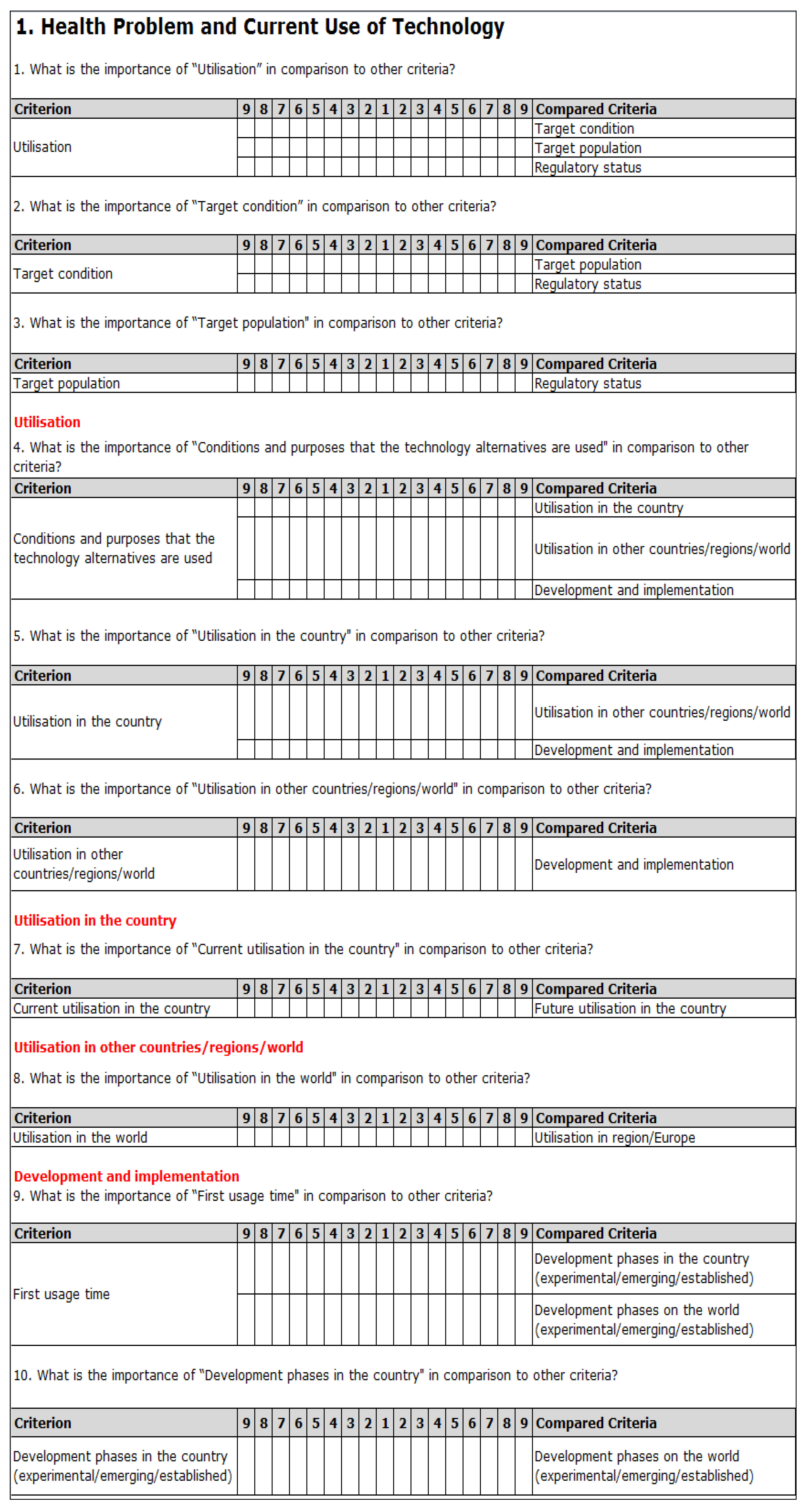
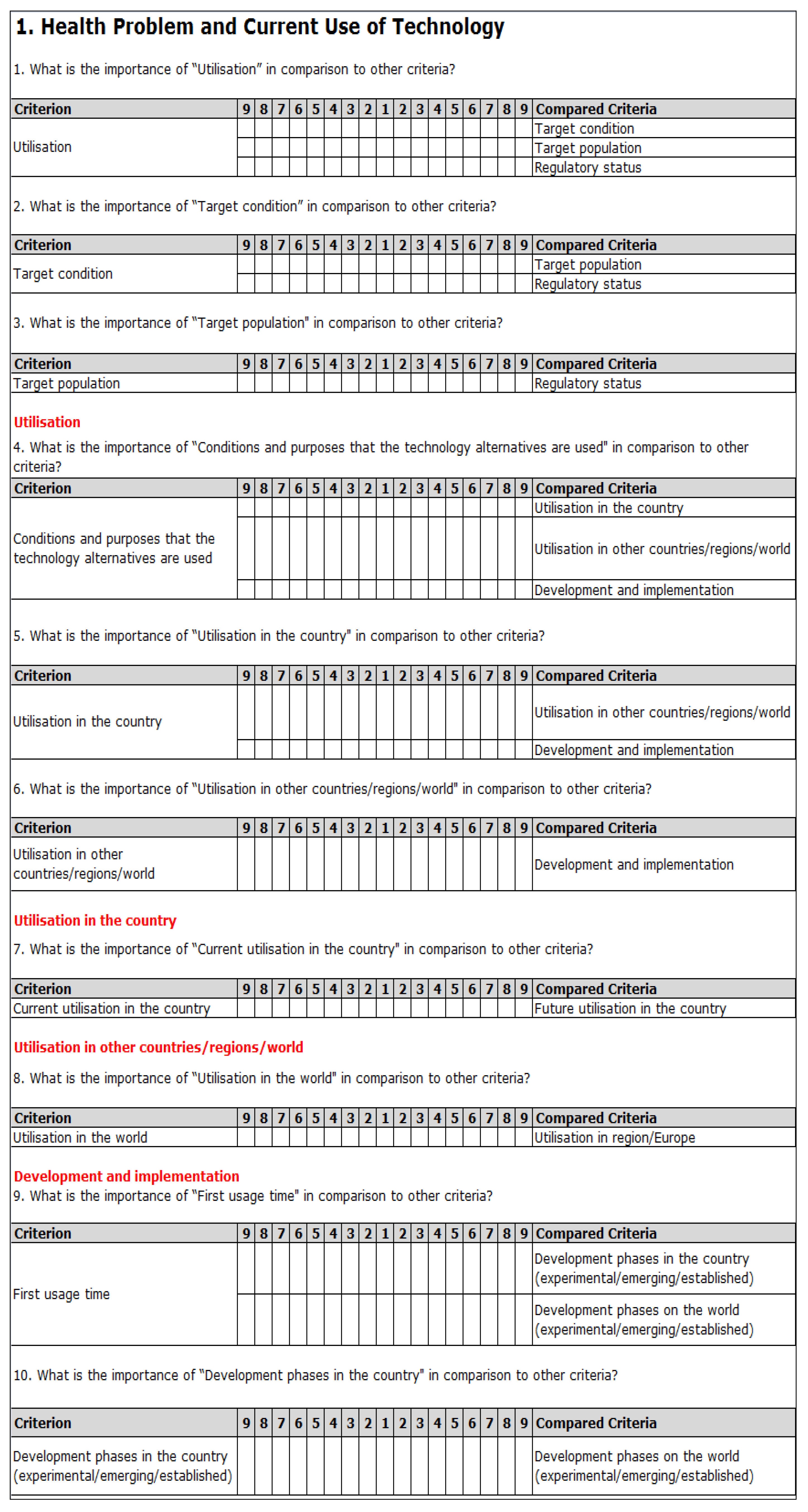
Appendix A.1. Health Problem and Current Use of Technology
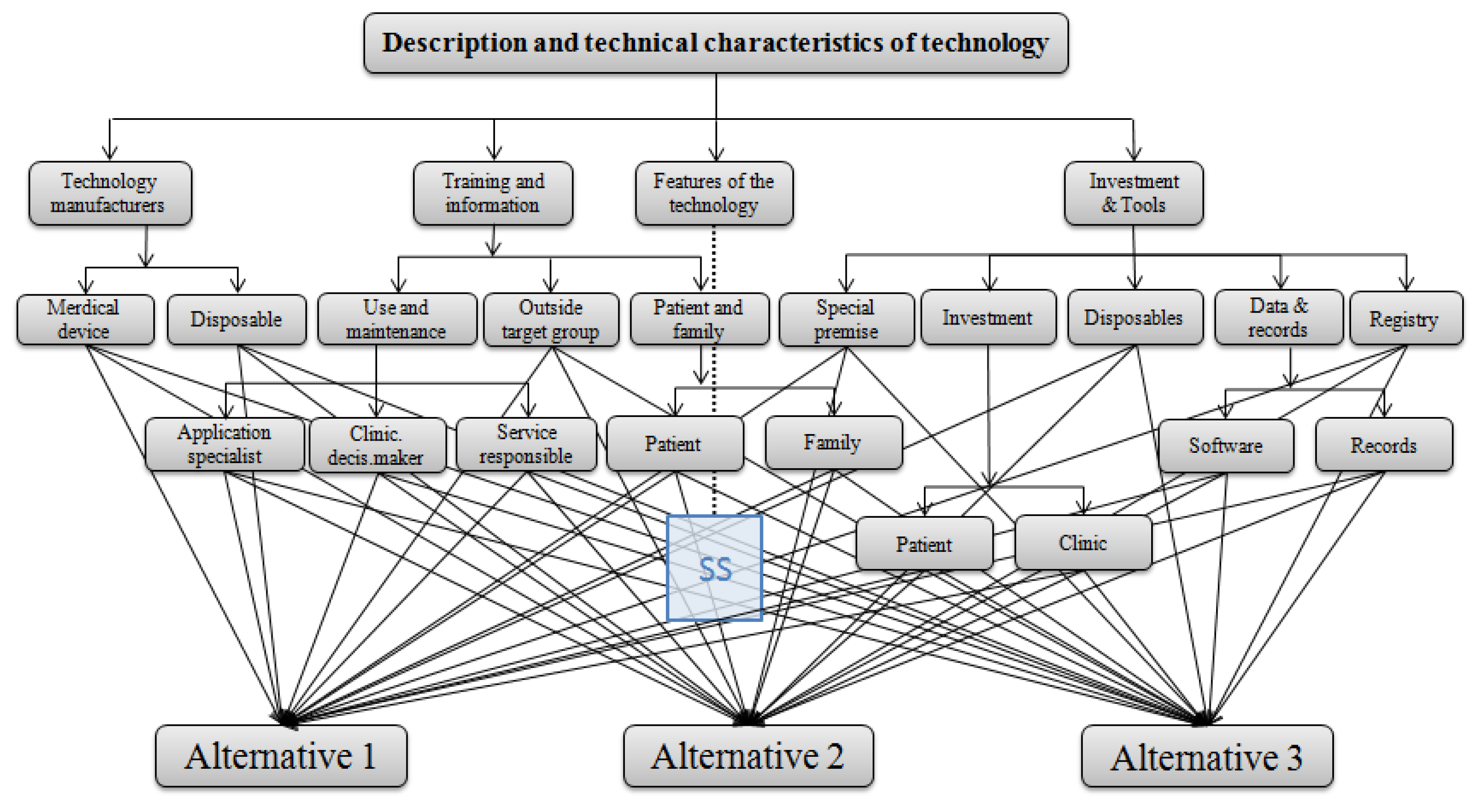
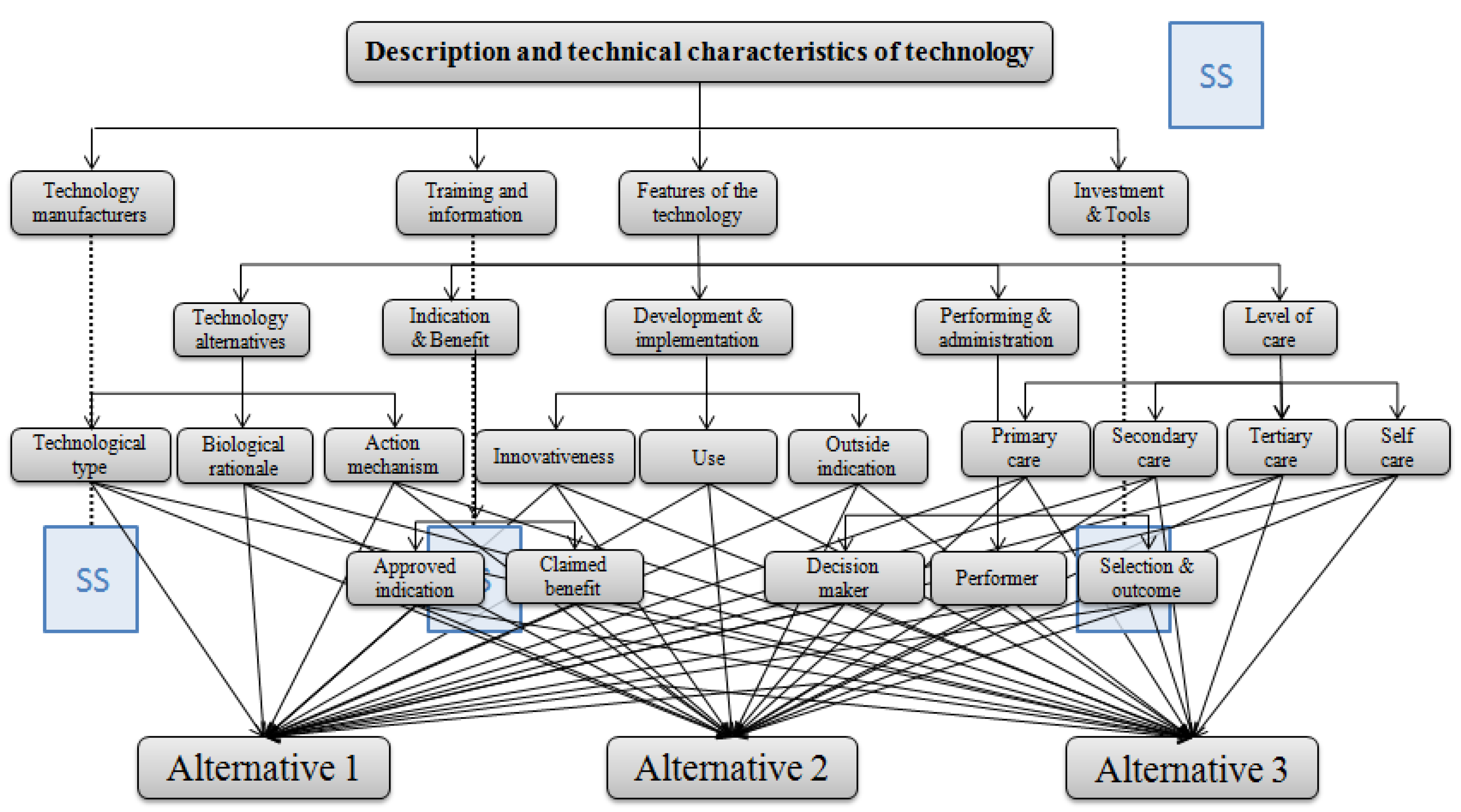
Appendix A.2. Description and Technical Characteristics of Technology


Appendix A.3. Safety

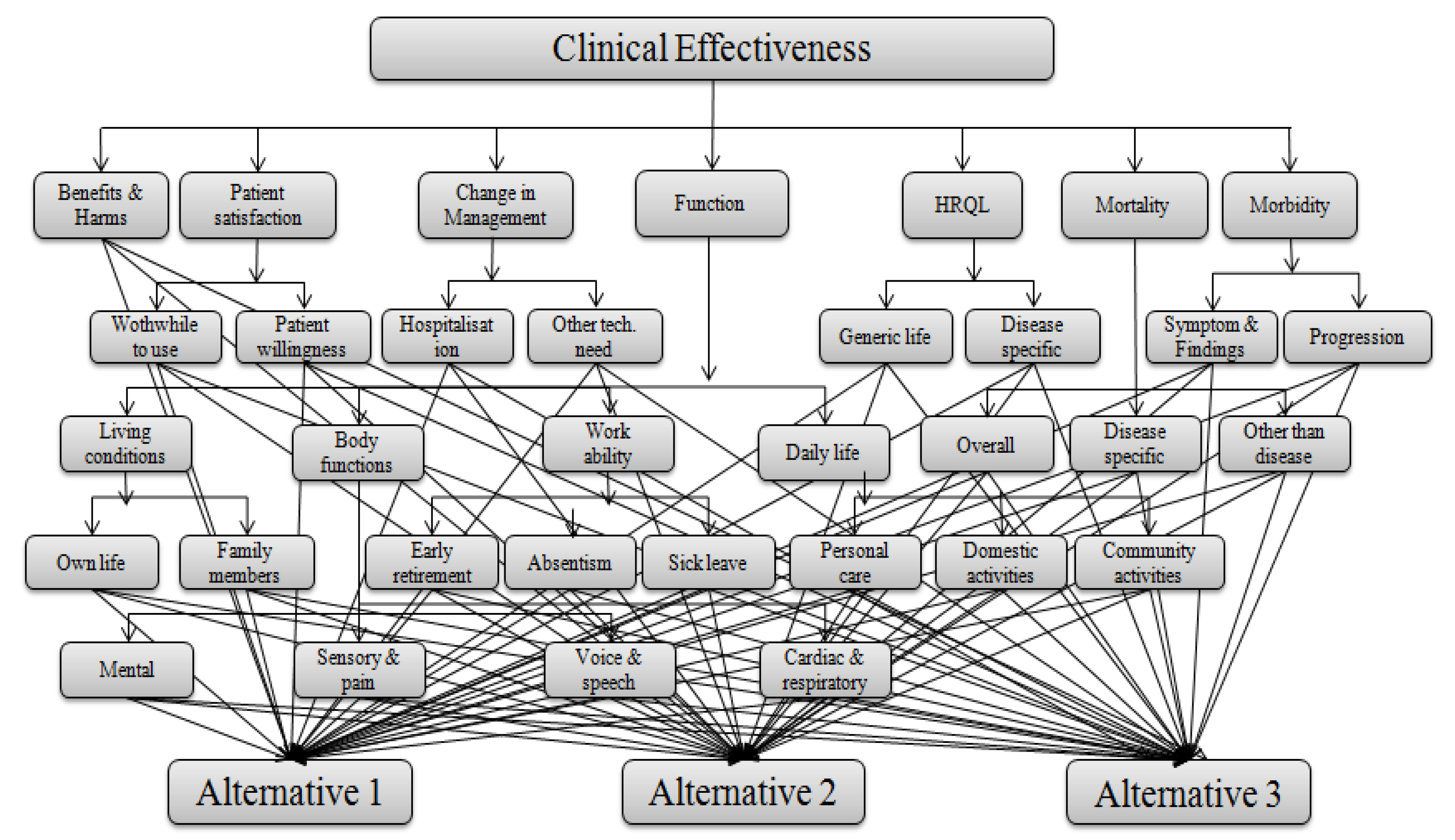
Appendix A.4. Clinical Effectiveness

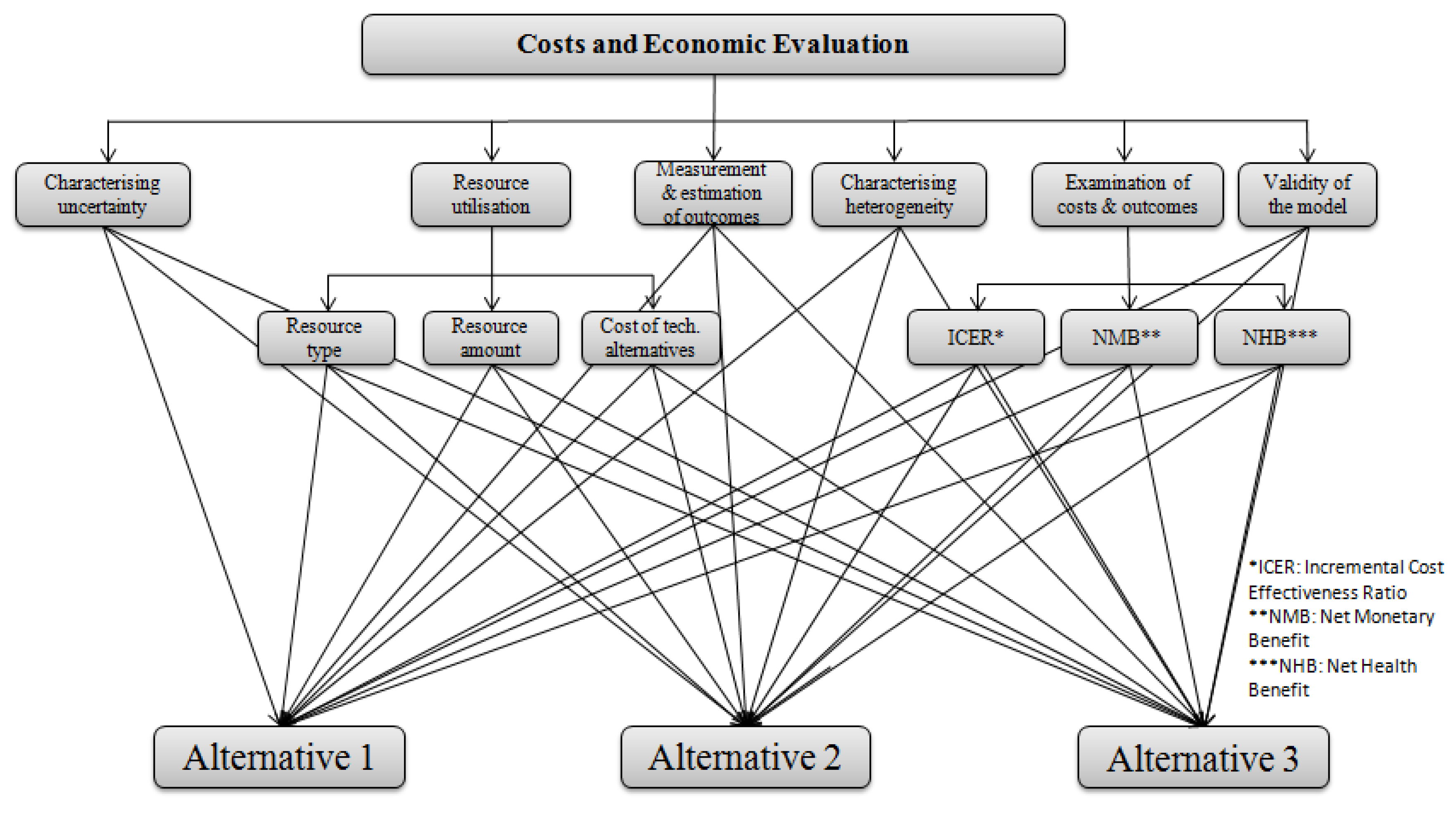
Appendix A.5. Costs and Economic Evaluation
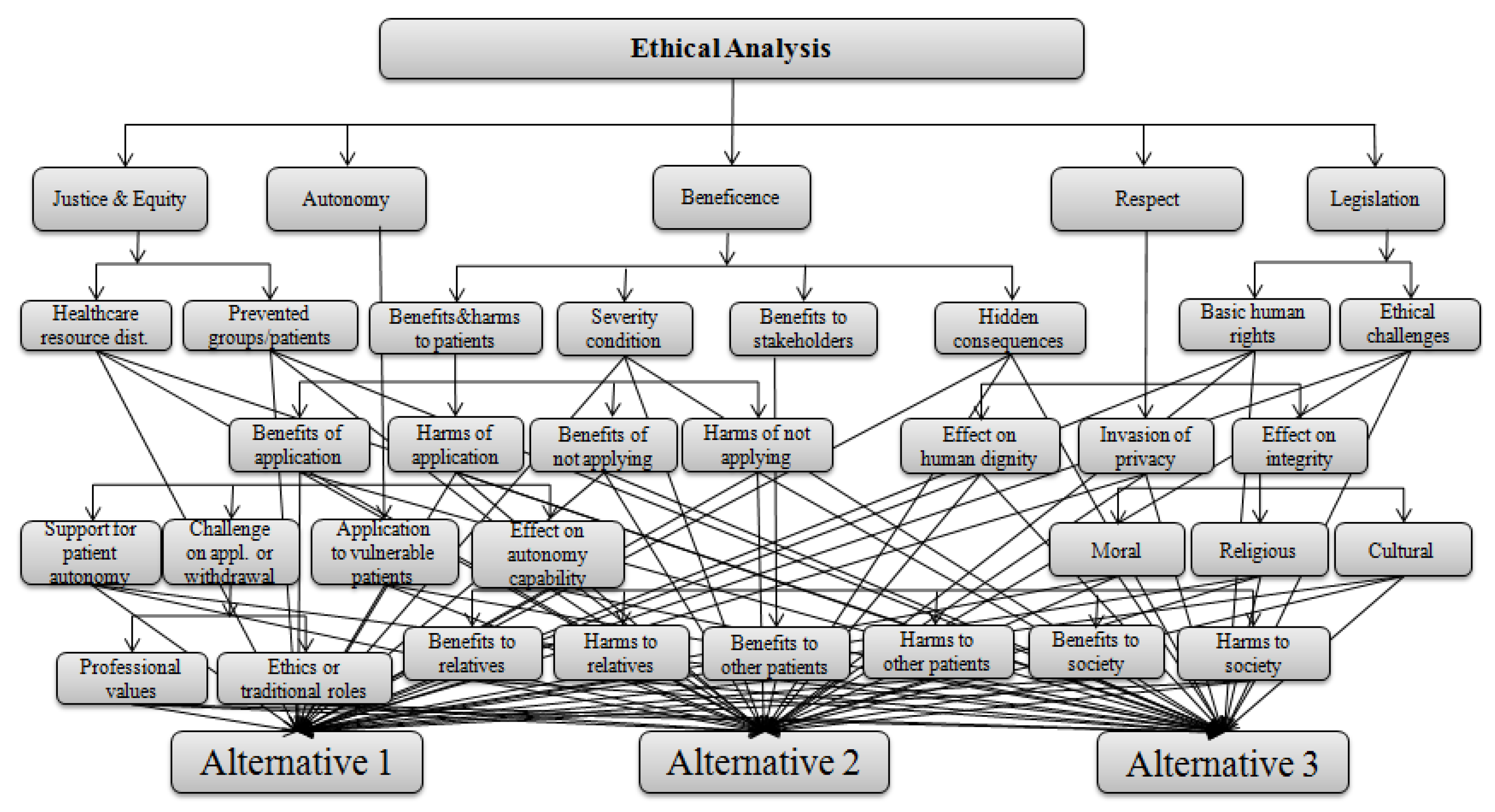
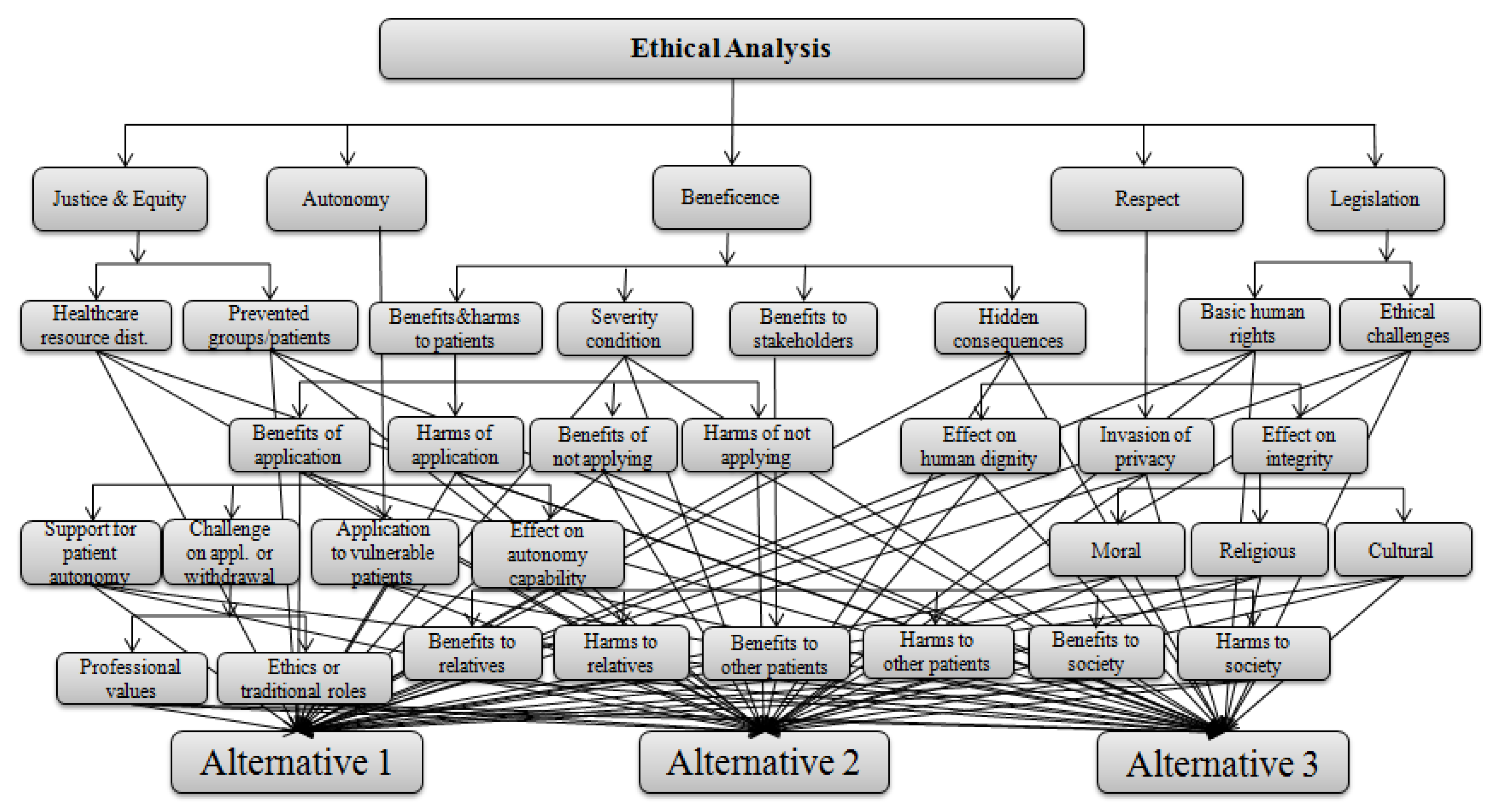
Appendix A.6. Ethical Analysis
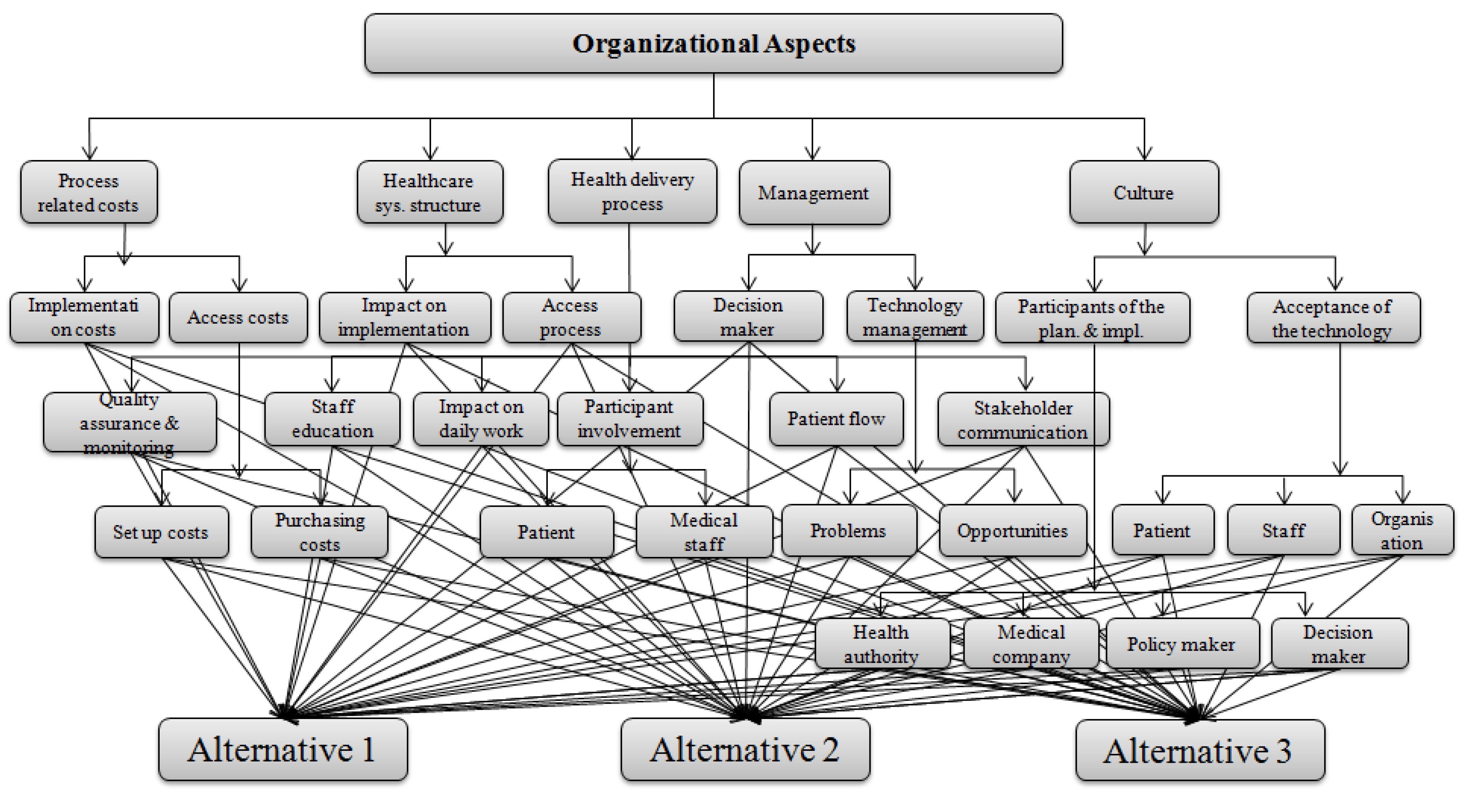
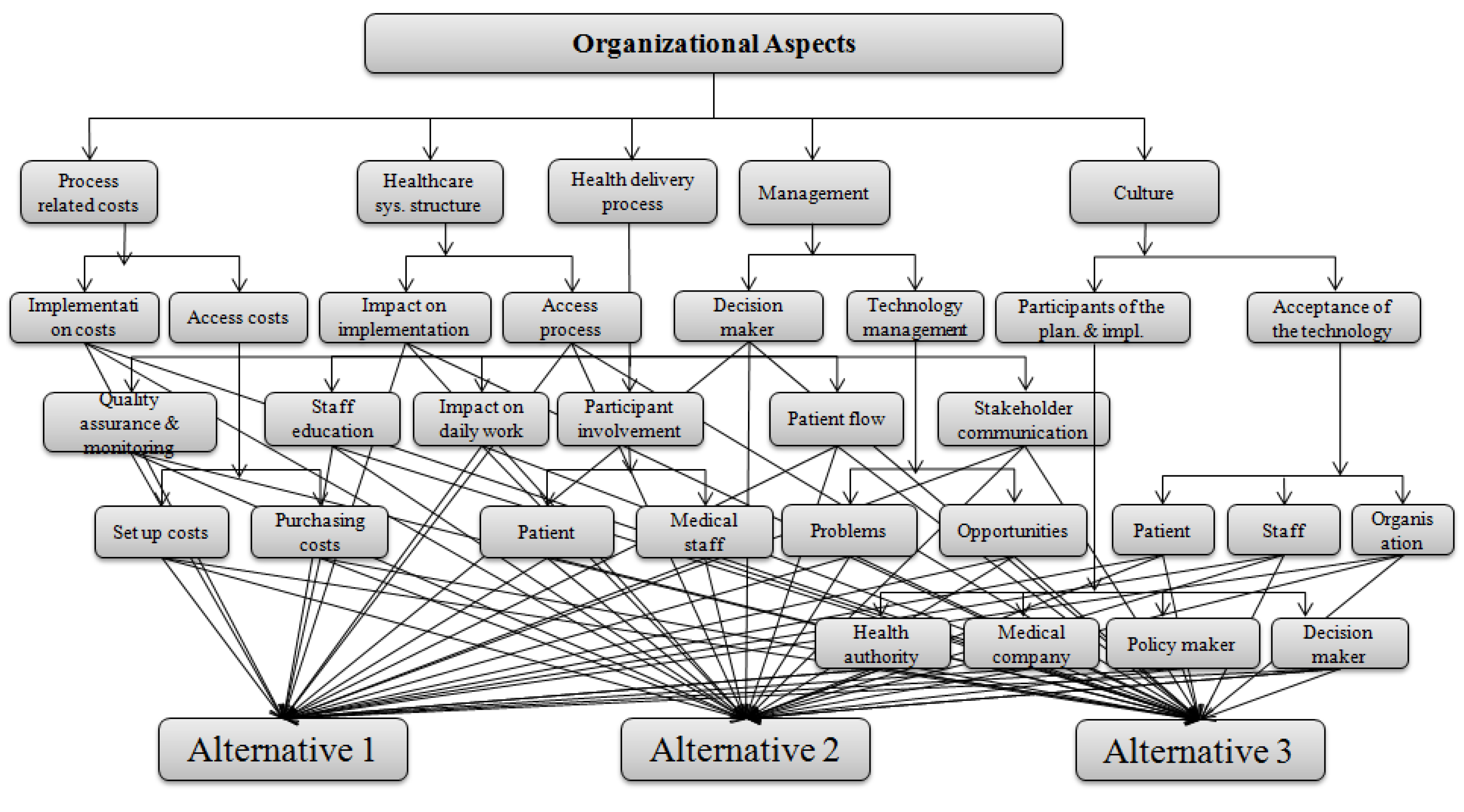
Appendix A.7. Organizational Aspects
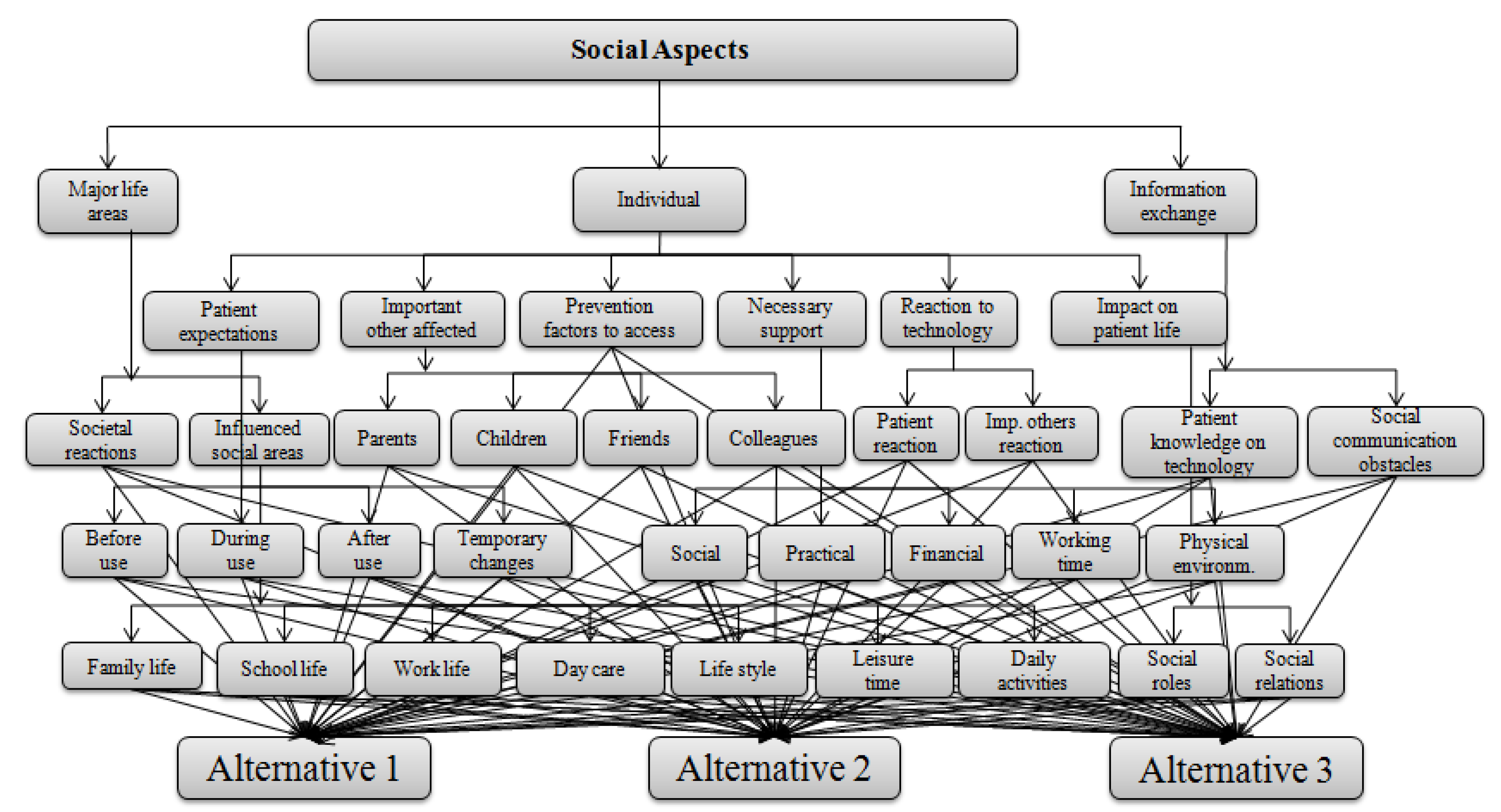
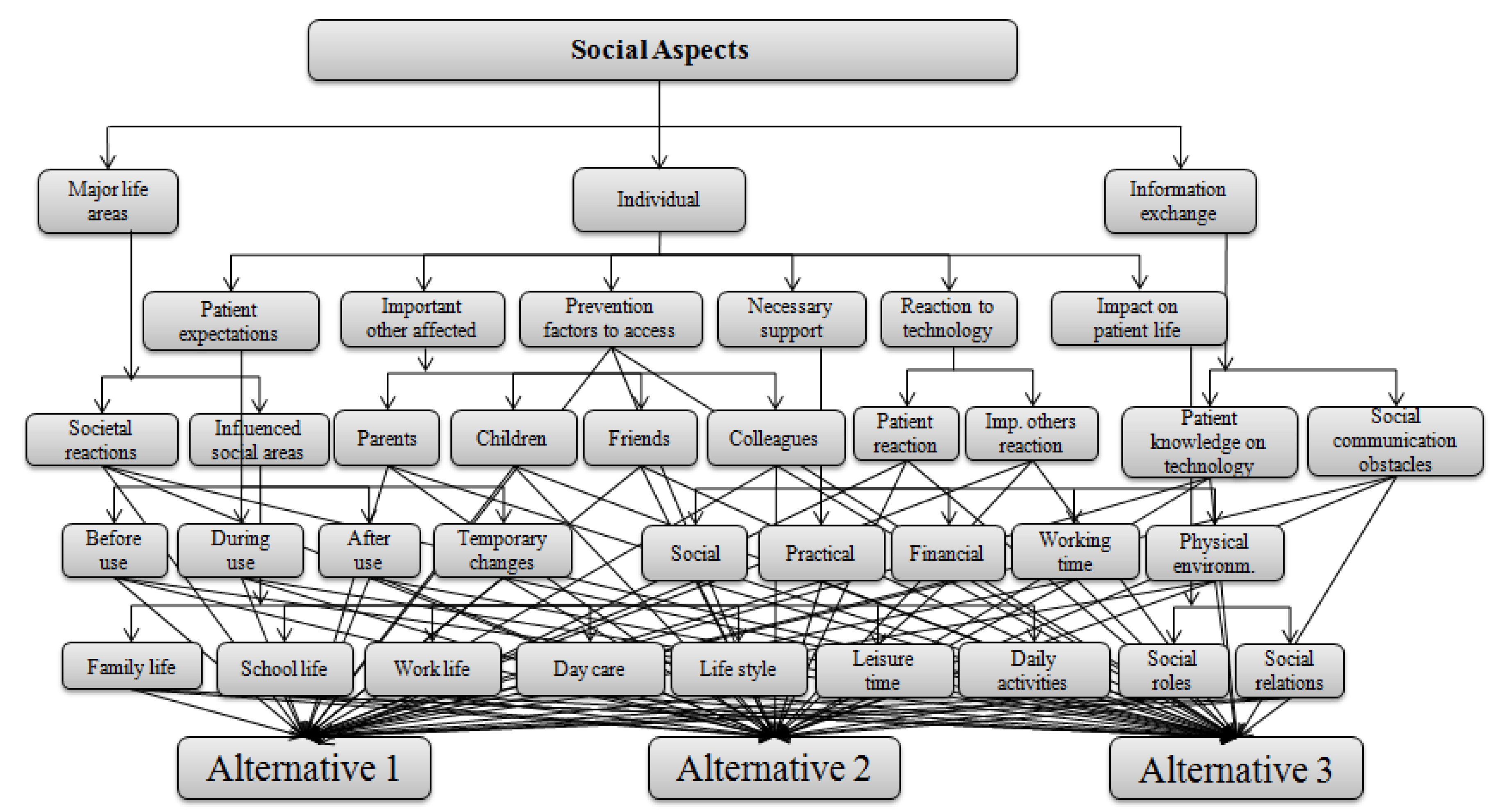
Appendix A.8. Social Aspects
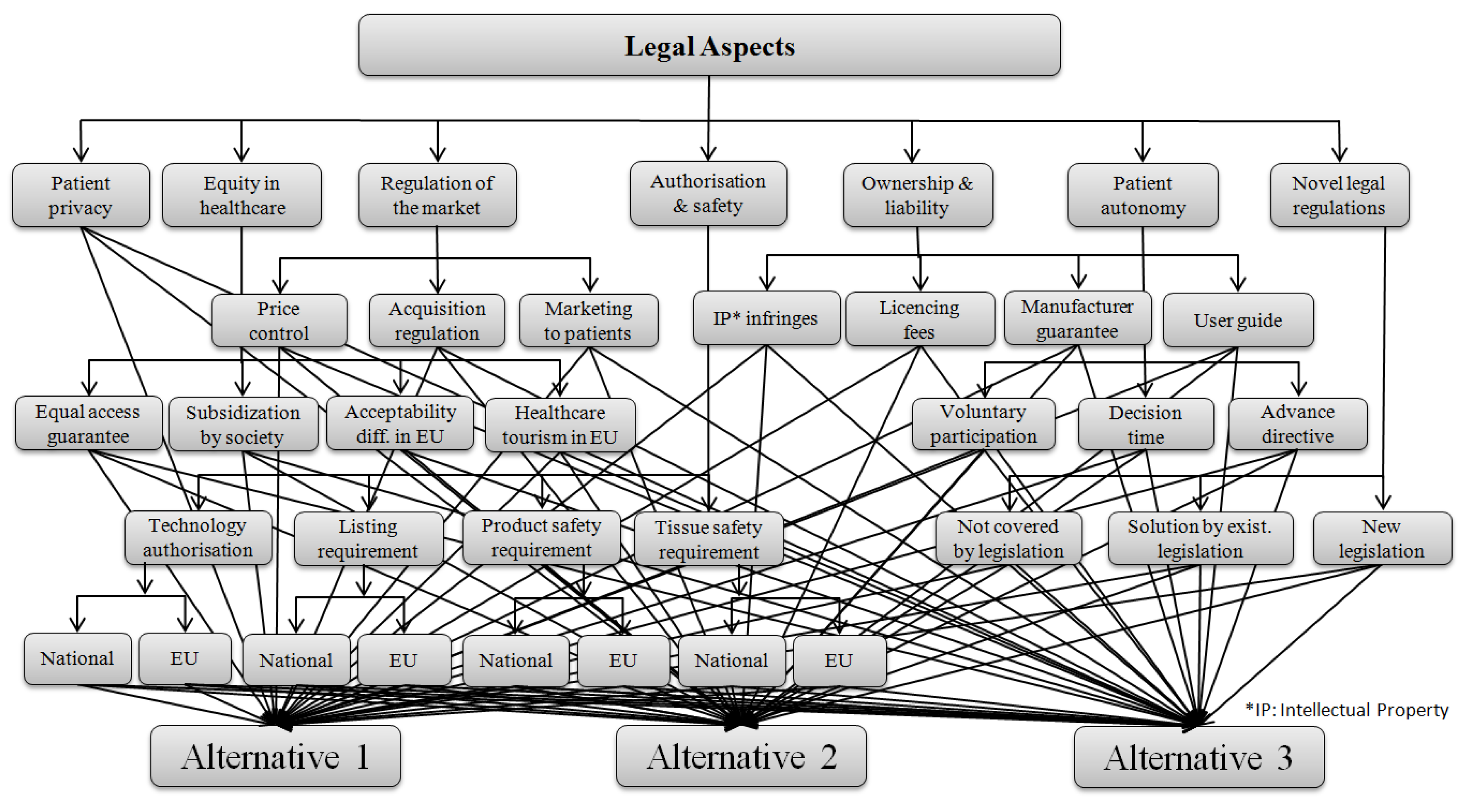
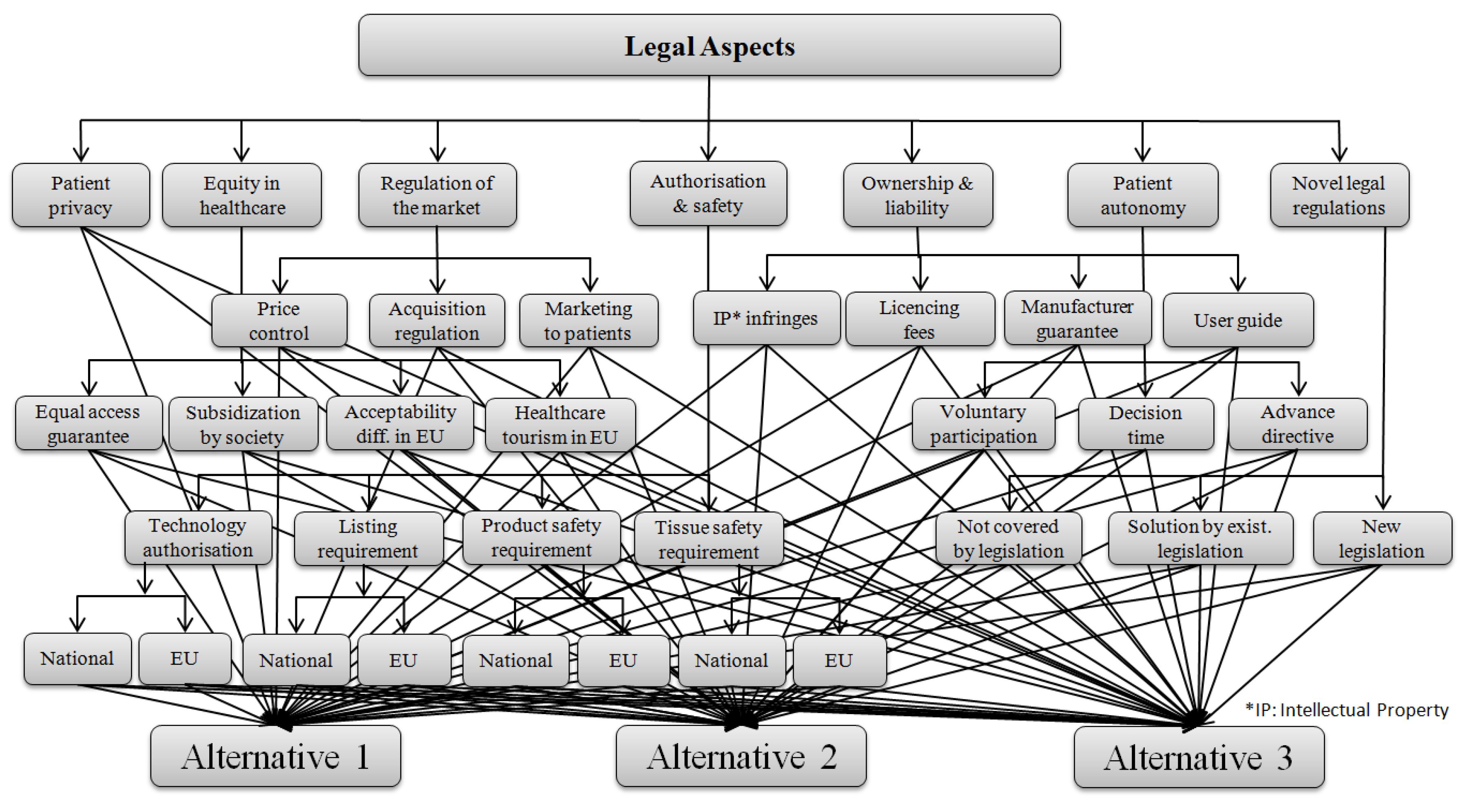
Appendix A.9. Legal Aspects
Appendix B. Performance Matrix and Normalized Main Criteria Weights of MCDA4HTA for the Role of Peritoneal Dialysis in Renal Care HTA Study

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Criterion | Criterion Description | Objective Function | Peritoneal Dialysis (PD) | Hemodialysis (HD) | Weights |
|---|---|---|---|---|---|
| 1.1.2 | Utilisation in the country 2016 | Maximize | 2871 | 57052 | 0.359% |
| 1.1.3.1 | Utilisation in other countries/regions—World 2008 | Maximize | 196000 | 1764000 | 0.062% |
| 1.1.3.2 | Utilisation in other countries/regions—USA 2014 | Maximize | 9.,70% | 90.30% | 0.077% |
| 1.2.1 | Target condition—Impact of technology alternatives on the prognosis and course of condition (Life saving YES or NO) | Maximize | 1 | 1 | 0.380% |
| 1.3 | Target population | Maximize | Very Good | Average | 0.843% |
| 1.4.1.1 | Market authorization—CE Mark | Maximize | Bad | Good | 0.458% |
| 1.4.2 | Reimbursement status | Maximize | Very Bad | Good | 0.180% |
| 1.4.2 | Reimbursement status | Minimize | 1225.00 | 537.24 | 0.180% |
| 2.1.1 | Technology manufacturers—Medical device manufacturers | Maximize | 2.00 | 4.00 | 0.183% |
| 2.1.2 | Technology manufacturers—Disposable manufacturers | Maximize | 2.00 | 15.00 | 0.183% |
| 2.2.1.1 | Training and information for Application specialists (nurse) | Minimize | 3.00 | 6.00 | 0.153% |
| 2.2.1.2 | Training and information for Clinical decision maker (Nephrologists) | Minimize | 3 | 3 | 0.379% |
| 2.2.1.3 | Training and information for Service and maintenance responsible (technician) | Maximize | Good | Bad | 0.153% |
| 2.2.2.1 | Training and information for patient | Maximize | Bad | Good | 0.304% |
| 2.2.2.2 | Training and information for his family | Maximize | 1 | 0 | 0.090% |
| 2.3.1.1 | Technology alternatives—Technological type | Maximize | Best | Worst | 0.017% |
| 2.3.1.2 | Technology alternatives—Biological rationale | Maximize | Best | Worst | 0.019% |
| 2.3.1.3 | Technology alternatives—Action mechanism | Maximize | Bad | Good | 0.019% |
| 2.3.2.2 | Claimed benefit | Maximize | Best | Average | 0.128% |
| 2.3.3.1 | Innovativeness | Maximize | Average | Very Good | 0.064% |
| 2.3.3.2 | Current use of technology | Maximize | 1 | 1 | 0.047% |
| 2.3.3.3 | Use outside in current indication | Maximize | 1 | 1 | 0.017% |
| 2.3.4.1 | Decision maker for starting and stopping the application | Maximize | Best | Very Bad | 0.061% |
| 2.3.4.2 | User performing the technology | Maximize | Best | Very Bad | 0.023% |
| 2.3.4.3 | User who selects the patients, interprets the outcome | Maximize | 1 | 1 | 0.083% |
| 2.3.5.1 | Level of care—Self care | Maximize | Best | Very Bad | 0.038% |
| 2.3.5.3 | Level of care—Secondary care | Minimize | 0 | 1 | 0.023% |
| 2.3.5.4 | Level of care—Tertiary care | Minimize | 0 | 1 | 0.023% |
| 2.4.1.1 | Required investment patients has to make | Maximize | Bad | Good | 0.041% |
| 2.4.1.2 | Required investment clinics has to make | Maximize | Bad | Worst | 0.124% |
| 2.4.2 | Required special premises | Maximize | 1 | 1 | 0.337% |
| 2.4.3 | Required disposable—amount | Maximize | Average | Very Bad | 0.084% |
| 2.4.3 | Required disposable—complexity | Maximize | Very Good | Bad | 0.084% |
| 2.4.4.1 | Data and records essential to monitor the use—Software | Maximize | Bad | Good | 0.054% |
| 2.4.4.2 | Data and records essential to monitor the use—Treatment records | Maximize | Best | Very Bad | 0.054% |
| 2.4.5 | National registry | Maximize | 2 | 2 | 0.093% |
| 3.1.1 | Harms technology can cause to the patient | Maximize | Very Bad | Bad | 1.123% |
| 3.2.1 | Occupational safety—Infection risk for user | Minimize | 0.03 | 0.0715 | 2.874% |
| 3.2.2 | Occupational safety—Radiation/contamination risk for user | Maximize | Good | Bad | 0.890% |
| 3.2.3 | Working position | Maximize | Good | Bad | 1.157% |
| 3.3.1 | Environmental safety—Domestic wastes | Maximize | Worst | Worst | 0.467% |
| 3.3.2 | Environmental safety—Chemical/medical wastes | Maximize | Average | Worst | 1.232% |
| 3.3.3 | Environmental safety—Radiation at the public level | Maximize | Average | Worst | 2.053% |
| 3.4.1 | Safety risk management—Training need for users | Maximize | Average | Very Bad | 2.260% |
| 3.4.2 | Safety risk management—Environmental circumstances for patients, citizens, and decision makers | Maximize | Average | Very Bad | 1.180% |
| 4.1.1.1 | Effect of technology on body functions—Mental | Minimize | 0.33 | 0.61 | 0.144% |
| 4.1.1.4 | Effect of technology on body functions—Cardiac & respiratory | Maximize | Bad | Worst | 0.225% |
| 4.1.1.5 | Effect of technology on body functions—Gastrointestinal | Maximize | Worst | Bad | 0.062% |
| 4.1.1.6 | Effect of technology on body functions—Skin functions | Maximize | Very Bad | Very Bad | 0.059% |
| 4.1.2 | Effect of technology on work ability | Maximize | 0.71 | 0.57 | 0.134% |
| 4.1.3.1 | Effect of technology on living conditions—own life | Maximize | Very Good | Bad | 0.224% |
| 4.1.3.2 | Effect of technology on living conditions—Family members | Maximize | Worst | Very Bad | 0.045% |
| 4.1.4.2 | Effect of technology on daily activities—Domestic activities | Maximize | Bad | Very Bad | 0.051% |
| 4.1.4.3 | Effect of technology on daily activities—Community activities | Maximize | Bad | Very Bad | 0.038% |
| 4.4.1 | Overall mortality—1st 3 years (HR) | Minimize | 0.92 | 0.94 | 1.722% |
| 4.4.1 | Overall mortality—Mortality decrease rate (2015 vs. 1996) | Maximize | 0.49 | 0.25 | 1.722% |
| 4.5.2 | Effect on progression—incident heart failure risk | Minimize | 1.00 | 1.56 | 0.415% |
| 4.5.2 | Effect on progression—prevalent heart failure risk | Minimize | 1.00 | 1.65 | 0.415% |
| 4.5.2 | Effect on progression—hip fractures | Minimize | 1.00 | 1.60 | 0.415% |
| 4.5.2 | Effect on progression—ischemic stroke risk (in 10,000 patient years) | Minimize | 100.10 | 61.60 | 0.415% |
| 4.5.2 | Effect on progression—hemorrhagic SVO (in 10,000 patient years) | Minimize | 74.70 | 59.40 | 0.415% |
| 4.5.2 | Effect on progression—physician visit due to psychological problems | Minimize | 0.08 | 0.09 | 0.415% |
| 4.6.1 | Hospitalization—all causes (in 1.25 years observation) | Minimize | 0.85 | 0.75 | 0.331% |
| 4.6.1 | Hospitalization—infection (in 1.25 years observation) | Minimize | 0.48 | 0.34 | 0.331% |
| 4.6.1 | Hospitalization in Australia over 1000 patients | Minimize | 2.26 | 2.80 | 0.331% |
| 4.6.1 | Hospitalization time in Australia over 1000 patients | Minimize | 13.30 | 10.30 | 0.331% |
| 4.7.2 | Patient satisfaction—Patient willingness on use of technology | Maximize | Good | Bad | 1.641% |
| 5.1.3 | Cost of technological alternatives (annual cost/session of treatment) | Minimize | 32098.81 | 26675.56 | 0.197% |
| 5.1.3 | Cost of technological alternatives (other direct costs excluding session costs) | Minimize | 4015.26 | 4505.23 | 0.197% |
| 5.1.3 | Cost of technological alternatives (indirect costs) | Minimize | 8825.42 | 7478.48 | 0.197% |
| 5.2 | Measurement and estimation of outcomes (QALYS) | Maximize | 0.71 | 0.68 | 2.128% |
| 5.3.1 | Incremental cost effectiveness ratio – ICER – costs for 5 years | Minimize | 185028.19 | 139226.60 | 0.285% |
| 5.3.1 | Incremental cost effectiveness ratio – ICER – effectiveness for 5 years | Maximize | 2.89 | 2.36 | 0.285% |
| 6.2.1 | Autonomy—Application to vulnerable patients—infant & children | Maximize | Best | Very Bad | 0.568% |
| 6.2.1 | Autonomy—Application to vulnerable patients—pregnant patients | Maximize | Best | Average | 0.568% |
| 6.2.2 | Autonomy—Effect on patients capability or possibility to exercise autonomy | Maximize | Best | Good | 0.494% |
| 6.2.3 | Autonomy—Need of additional information for patient autonomy | Maximize | Very Bad | Very Bad | 0.769% |
| 6.2.4.2 | Challenge or change with application or withdrawal on ethics or traditional roles | Maximize | Worst | Very Bad | 0.092% |
| 6.3.1 | Respect—Effects of technology on human dignity | Maximize | Worst | Worst | 0.563% |
| 6.3.2.1 | Respect—Effects of technology on users moral integrity | Maximize | Worst | Worst | 0.115% |
| 6.3.2.2 | Respect—Effects of technology on users religious integrity | Maximize | Good | Worst | 0.018% |
| 6.3.2.3 | Respect—Effects of technology on users cultural integrity | Maximize | Good | Good | 0.028% |
| 6.3.3 | Respect—Invasion of users privacy | Maximize | Good | Average | 0.618% |
| 6.4.1 | Justice and equity—Effect of technology implementation or withdrawal on health care resource distribution | Maximize | Very Bad | Worst | 1.482% |
| 7.1.1 | Health delivery process—Impact on daily work | Maximize | Bad | Worst | 0.135% |
| 7.1.2 | Health delivery process—Patient/participant flow with the new technology | Maximize | Bad | Worst | 0.122% |
| 7.1.3.1 | Health delivery process—Patient participation | Maximize | Best | Bad | 0.106% |
| 7.1.3.2 | Health delivery process—Healthcare professional participation | Maximize | Average | Worst | 0.038% |
| 7.1.4 | Health delivery process—Education and training for staff | Maximize | Worst | Average | 0.639% |
| 7.1.5 | Health delivery process—Stakeholder co—operation and communication | Maximize | Bad | Bad | 0.399% |
| 7.2.1 | Healthcare system structure—Impact on implementation in terms of centralization | Maximize | Average | Very Good | 0.708% |
| 7.2.2 | Healthcare system structure—Process in ensuring access of patients and participants to the technology | Maximize | Worst | Very Good | 1.415% |
| 7.3.1.1 | Purchasing process | Maximize | Average | Worst | 0.384% |
| 7.3.1.2 | Set up process | Maximize | Average | Very Bad | 0.313% |
| 7.3.2 | Budget impact of implementing the technology | Maximize | Very Bad | Very Bad | 0.702% |
| 7.4.1.1 | Management—Problems | Maximize | Good | Bad | 0.216% |
| 7.4.1.2 | Management—Opportunities | Maximize | Good | Bad | 0.210% |
| 7.4.2 | Decision maker on eligibility of people for the use of technology | Maximize | 1 | 1 | 0.709% |
| 7.5.1.1 | Acceptance of technology by organization | Maximize | Worst | Best | 0.102% |
| 7.5.1.2 | Acceptance of technology by staff | Maximize | Bad | Best | 0.042% |
| 7.5.1.3 | Acceptance of technology by patient | Maximize | Very Good | Bad | 0.279% |
| 7.5.2.1 | Health authority participation | Maximize | Worst | Average | 0.209% |
| 7.5.2.2 | Medical company participation | Maximize | Best | Good | 0.093% |
| 7.5.2.3 | Policy maker participation | Maximize | Worst | Average | 0.131% |
| 7.5.2.4 | Decision maker participation | Maximize | Worst | Best | 0.336% |
| 8.1.2.1 | Parents affected by use of the technology | Maximize | Worst | Very Bad | 0.070% |
| 8.1.2.2 | Children affected by use of the technology | Maximize | Very Bad | Bad | 0.183% |
| 8.1.2.3 | Friends affected by use of the technology | Maximize | Bad | Bad | 0.019% |
| 8.1.2.4 | People at work affected by use of the technology | Maximize | Very Bad | Worst | 0.036% |
| 8.1.3.1 | Social support needed by patients | Minimize | Best | Best | 0.094% |
| 8.1.3.2 | Practical support needed by patients | Minimize | Best | Very Good | 0.065% |
| 8.1.3.3 | Financial support needed by patients | Minimize | Best | Good | 0.353% |
| 8.1.3.4 | Working time support needed by patients | Minimize | Good | Best | 0.302% |
| 8.1.3.5 | Physical environment support needed by patients | Minimize | Best | Average | 0.268% |
| 8.1.4.1 | Change in social roles due to use of technology | Maximize | Very Bad | Very Bad | 0.971% |
| 8.1.4.2 | Maintenance of social relationships | Maximize | Bad | Very Bad | 1.111% |
| 8.1.5.1 | Patient action/reaction to use of technology | Maximize | Bad | Worst | 0.678% |
| 8.1.5.2 | Important others action/reaction to use of technology | Minimize | 1.00 | 4.50 | 0.103% |
| 8.1.6 | Factors preventing participation of a group or persons | Minimize | Average | Average | 1.870% |
| 8.2.1.1 | Influence on family life by use of technology | Maximize | Bad | Worst | 0.039% |
| 8.2.1.2 | Influence on school life by use of technology | Maximize | Very Bad | Worst | 0.039% |
| 8.2.1.3 | Influence on work life by use of technology | Maximize | Very Bad | Worst | 0.039% |
| 8.2.1.4 | Influence on day care by use of technology | Maximize | Worst | Very Bad | 0.039% |
| 8.2.1.5 | Influence on life style by use of technology | Maximize | Worst | Worst | 0.039% |
| 8.2.1.6 | Influence on daily activities by use of technology | Maximize | Worst | Very Bad | 0.039% |
| 8.2.1.7 | Influence on leisure time by use of technology | Maximize | Worst | Very Bad | 0.039% |
| 8.2.2 | Impact on overall social level by introduction of the technology | Maximize | Worst | Worst | 0.429% |
| 8.3.1 | Knowledge and understanding of the technology in patients | Maximize | Very Bad | Worst | 0.806% |
| 8.3.2 | Social obstacles or prospects in the communication about the technology | Maximize | Worst | Very Bad | 0.240% |
| 9.1.1 | Authorization of the technology alternatives | Maximize | Best | Best | 0.296% |
| 9.1.2 | Listing of technology in national or European Union registries | Maximize | Best | Best | 0.214% |
| 9.1.3 | Product safety requirement fulfillment of technology | Maximize | Best | Best | 0.425% |
| 9.2.3 | Content of manufacturers guarantee | Maximize | Best | Best | 0.213% |
| 9.2.4 | Comprehensiveness of the technology user guide | Maximize | Very Good | Best | 0.154% |
| 9.4 | Privacy of the patient | Maximize | Best | Bad | 3.277% |
| Criteria | Main Criteria (1st Level) | Normalized Weight |
|---|---|---|
| 1 | Health problem and current use of technology | 4.93% |
| 2 | Description and technical characteristics of technology | 3.58% |
| 3 | Safety | 18.86% |
| 4 | Clinical effectiveness | 22.37% |
| 5 | Cost and economic evaluation | 7.28% |
| 6 | Ethical analysis | 11.76% |
| 7 | Organizational aspects | 7.68% |
| 8 | Social aspects | 10.26% |
| 9 | Legal aspects | 13.27% |
| Total | 100% |
Appendix C. Scale Used to Interpret the Linguistic Terms for the Given Definitions in the HTA Report
| Linguistic Terms | Worst | Very Bad | Bad | Average | Good | Very Good | Best | |
|---|---|---|---|---|---|---|---|---|
| Definition | Positive | Worse Not interested Very negative effect Lowest | Very bad Low interest Negative effect | Bad Negative signs | Average Neutral | Good Positive signs Some tendency | Very good Some involvement Positive effect | Best Completely involved Excellent effect Very high |
| Negative | More problems | Less problems More needs | Too much needs | At most needs | ||||
Appendix D. An Example for MCDA4HTA Questionnaires

References
- Banta, H.D.; Luce, B.R. Health Care Technology and Its Assessment: An International Perspective; Oxford University Press: New York, NY, USA, 1993. [Google Scholar]
- Simoens, S. Health Economic Assessment: A Methodological Primer. Int. J. Environ. Res. Public Health 2009, 6, 2950–2966. [Google Scholar] [CrossRef] [PubMed]
- Battista, R.N.; Hodge, M.J. The evolving paradigm of health technology assessment: Reflections for the millennium. Can. Med Assoc. J. 1999, 160, 1464–1467. [Google Scholar]
- Merino, G.A.; Lema, L.V. Needs and demands of policy-makers. In Health Technology Assessment and Health Policy-Making in Europe; Observatory Studies Series No. 14; Garrido, M.V., Kristensen, V.B., Nielsen, C.B., Eds.; World Healthcare Organization: Copenhagen, Denmark, 2008. [Google Scholar]
- Sullivan, S.D.; Watkins, J.; Sweet, B.; Ramsey, S.D. Health technology assessment in health-care decisions in the United States. Value Health 2009, 12, S39–S44. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Goetghebeur, M.M.; Wagner, M.; Khoury, H.; Levitt, R.J.; Erickson, L.J.; Rindress, D. Bridging health technology assessment (HTA) and efficient health care decision making with multicriteria decision analysis (MCDA): Applying the EVIDEM framework to medicines appraisal. Int. J. Soc. Med Decis. Mak. 2012, 32, 376–388. [Google Scholar] [CrossRef] [PubMed]
- Johnson-Masotti, A.P.; Eva, K. A decision-making framework for the prioritization of health technologies. In Health Services Restructuring in Canada: New Evidence and New Directions; Beach, C.M., Chaykowski, R.P., Shortt, S., St-Hilaire, F., Sweetman, A., Eds.; John Deutsch Institute, Queen’s University: Kingston, Australia, 2006. [Google Scholar]
- Diaby, V.; Goeree, R. How to use multi-criteria decision analysis methods for reimbursement decision-making in healthcare: A step-by-step guide. Expert Rev. Pharmacoecon. Outcomes Res. 2014, 14, 81–99. [Google Scholar] [CrossRef] [PubMed]
- Diaby, V.; Laurier, C.; Lachaine, J. A Proposed Framework for Formulary Listing in Low-Income Countries: Incorporating Key Features from Established Drug Benefit Plans. Pharm. Med. 2011, 25, 71–82. [Google Scholar] [CrossRef]
- Daniels, N.; Sabin, J. Limits to health care: Fair procedures, democratic deliberation, and the legitimacy problem for insurers. Philos. Public Aff. 1997, 26, 303–350. [Google Scholar] [CrossRef]
- Dhalla, I.; Laupacis, A. Moving from opacity to transparency in pharmaceutical policy. CMAJ 2008, 178, 428–431. [Google Scholar] [CrossRef] [Green Version]
- Tony, M.; Wagner, M.; Khoury, H.; Rindress, D.; Papastavros, T.; Oh, P.; Goetghebeur, M.M. Bridging health technology assessment (HTA) with multicriteria decision analyses (MCDA): Field testing of the EVIDEM framework for coverage decisions by a public payer in Canada. BMC Health Serv. Res. 2011, 11, 329. [Google Scholar] [CrossRef] [Green Version]
- EUnetHTA. The HTA Core Model for Medical and Surgical Interventions (2.1). The HTA Core Model Assessment Table. Available online: http://corehta.info/model/AE-tables-interventions-2.1.pdf (accessed on 5 February 2018).
- Kristensen, F.B. Development of European HTA: From Vision to EUnetHTA. Michael 2012, 9, 147–156. [Google Scholar]
- Kristensen, F.B.; Lampe, K.; Chase, D.L.; Lee-Robin, S.H.; Wild, C.; Moharra, M.; Garrido, M.V.; Nielsen, C.P.; Rottingen, J.A.; Neikter, S.A.; et al. Practical tools and methods for health technology assessment in Europe: Structures, methodologies, and tools developed by the European Network for Health Technology Assessment, EUnetHTA. Int. J. Technol. Assess. Health Care 2009, 2, 1–8. [Google Scholar] [CrossRef] [Green Version]
- Lampe, K.; Makela, M.; Garrido, M.V.; Anttila, H.; Autti-Ramo, I.; Hicks, N.J.; Hofmann, B.; Koivisto, J.; Kunz, R.; Karki, P.; et al. The HTA core model: A novel method for producing and reporting health technology assessments. Int. J. Technol. Assess. Health Care 2009, 2, 9–20. [Google Scholar] [CrossRef] [Green Version]
- Emami, M.; Nazari, K.; Fardmanesh, H. Application of Fuzzy TOPSIS Technique for Strategic Management Decision. J. Basic Appl. Sci. Res. 2012, 2, 685–689. [Google Scholar]
- Deshmukh, A.; Millet, I. An Analytic Hierarchy Process Approach to Assessing the Risk of Management Fraud. J. Appl. Bus. Res. 1999, 15, 87–102. [Google Scholar] [CrossRef]
- Baykasoglu, A.; Owen, S.; Gindy, N. A Taboo search based approach to find the pareto optimal set in multiple objective optimization. Eng. Optim. 1999, 31, 731–748. [Google Scholar] [CrossRef]
- Celano, G.; Fichera, S.; Grasso, V.; La Commare, U.; Perrone, G. An evolutionary approach to multi-objective scheduling of mixed model assembly lines. Comput. Ind. Eng. 1999, 37, 69–73. [Google Scholar] [CrossRef]
- Clı’maco, J.C.N.; Antunes, C.H. TRIMAP—An interactive tricriteria linear programming package. Found. Control Eng. 1998, 12, 101–120. [Google Scholar]
- Alvarez-Guerra, M.; Canis, L.; Voulvoulis, N.; Viguri, J.R.; Linkov, I. Prioritization of sediment management alternatives using stochastic multicriteria acceptability analysis. Sci. Total Environ. 2010, 408, 4354–4367. [Google Scholar] [CrossRef] [PubMed]
- Linkov, I.; Bates, M.E.; Canis, L.J.; Seager, T.P.; Keisler, J.M. A decision-directed approach for prioritizing research into the impact of nanomaterials on the environment and human health. Nat. Nanotechnol. 2011, 6, 784–787. [Google Scholar] [CrossRef] [PubMed]
- Linkov, I.; Varghese, A.; Jamil, S. Multicriteria decision analysis: A framework for structuring remedial decisions at contaminated sites. In Comparative Risk Assessment and Environmental Decision Making; Linkov, I., Ramadan, A., Eds.; Kluwer Academic Publishers: Dordrecht, The Netherlands, 2004. [Google Scholar]
- Ozturk, N.; Tozan, H. A Fuzzy-Based Decision Support Model for Selecting the Best Dialyser Flux in Haemodialysis. J. Healthc. Eng. 2015, 6, 303–324. [Google Scholar] [CrossRef] [PubMed]
- Turgut, B.T.; Tas, G.; Herekoglu, A.; Tozan, H.; Vayvay, O. A fuzzy AHP based decision support system for disaster center location selection and a case study for Istanbul. Disaster Prev. Manag. 2011, 20, 499–520. [Google Scholar] [CrossRef]
- Temucin, T.; Tozan, H.; Vayvay, O.; Harnicarova, M.; Valicek, J. A fuzzy based decision model for nontraditional machining process selection. Int. J Adv. Manuf. Technol. 2014, 70, 2275–2282. [Google Scholar] [CrossRef]
- Belton, V.; Stewart, T.J. Multiple Criteria Decision Analysis: An Integrated Approach; Kluwer Academic: Boston, MA, USA, 2002. [Google Scholar]
- Dolan, J.G. Multi-criteria clinical decision support: A primer on the use of multiple criteria decision making methods to promote evidence-based, patient-centered healthcare. Patient 2010, 3, 229–248. [Google Scholar] [CrossRef]
- Marjan Hummel, J.M.; Van Rossum, W.; Verkerke, G.J.; Rakhorst, G. Medical Technology Assessment: The use of the Analytic Hierarchy process as a Tool for Multidisciplinary Evaluation of Medical Devices. Int. J. Artif. Organs 2000, 23, 782–787. [Google Scholar] [CrossRef]
- Thokala, P.; Duenas, A. Multiple criteria decision analysis for health technology assessment. Value Health 2012, 15, 1172–1181. [Google Scholar] [CrossRef] [Green Version]
- Rao, R.V. Decision Making in the Manufacturing Environment Using Graph Theory and Fuzzy Multiple Attribute Decision Making Methods; Springer: London, UK, 2013. [Google Scholar]
- Aouni, B.; Kettani, O. Goal Programming Model: A Glorious History and a Promising Future. Eur. J. Oper. Res. 2001, 133, 225–231. [Google Scholar] [CrossRef]
- Wind, Y.; Saaty, T.L. Marketing Applications of the Analytic Hierarchy Process. Manag. Sci. 1980, 26, 641–658. [Google Scholar] [CrossRef]
- Vaidya, O.S.; Kumar, S. Analytic hierarchy process: An overview of applications. Eur. J. Oper. Res. 2006, 169, 1–29. [Google Scholar] [CrossRef]
- Saaty, T.L. The Analytic Hierarchy Process; McGraw Hill: New York, NY, USA, 1980. [Google Scholar]
- Saaty, T.L. Fundamental of Decision Making and Priority Theory with the Analytic Hierarchy Process; RWS Publications: Pittsburg, CA, USA, 2000. [Google Scholar]
- Hwang, C.L.; Yoon, K. Multiple Attribute Decision Making: Methods and Applications: A State-of-the-Art Survey; Springer: London, UK, 1981. [Google Scholar]
- Rao, R.V. Decision Making in the Manufacturing Environment; Springer: London, UK, 2007. [Google Scholar]
- Opricovic, S. Programski Paket VIKOR za Visekriterijumsko Kompromisno Rangiranje. In Proceedings of the 17th International Symposium on Operational Research SYM-OP-IS, Dubrovnik-Kupari, Croatia, 9–12 October 1990. [Google Scholar]
- Yu, P.L. A Class of Solutions for Group Decision Problems. Manag. Sci. 1973, 19, 936–946. [Google Scholar] [CrossRef]
- Zeleny, M. Multiple Criteria Decision Making; McGraw-Hill: New York, NY, USA, 1982. [Google Scholar]
- Opricovic, S.; Tzeng, G.H. Multicriteria Planning of Post-Earthquake Sustainable Reconstruction. Comput. Aided Civ. Infrastruct. Eng. 2002, 17, 211–220. [Google Scholar] [CrossRef]
- Opricovic, S.; Tzeng, G.H. Compromise solution by MCDM methods: A comparative analysis of VIKOR and TOPSIS. Eur. J. Oper. Res. 2004, 156, 445–455. [Google Scholar] [CrossRef]
- Charnes, A.; Cooper, W.W. Management Models and Industrial Applications of Linear Programming; Wiley: New York, NY, USA, 1961. [Google Scholar]
- Lee, J.; Kang, S.H.; Rosenberger, J.; Kim, S.B. A hybrid approach of goal programming for weapon systems selection. Comput. Ind. Eng. 2010, 58, 521–527. [Google Scholar] [CrossRef]
- Bertolini, M.; Bevilacqua, M. A combined goal programming—AHP approach to maintenance selection problem. Reliab. Eng. Syst. Saf. 2006, 91, 839–848. [Google Scholar] [CrossRef]
- Sayadi, M.K.; Heydari, M.; Shahanaghi, K. Extension of VIKOR method for decision making problem with interval numbers. Appl. Math. Model. 2009, 33, 2257–2262. [Google Scholar] [CrossRef]
- Zadeh, L.A. Outline of a New Approach to the Analysis of Complex Systems and Decision Processes. IEEE Trans. Syst. Manand Cybern. 1973, SMG-3, 28–44. [Google Scholar] [CrossRef] [Green Version]
- Baltussen, R.; Niessen, L. Priority setting of health interventions: The need for multi-criteria decision analysis. Cost Eff. Resour. Alloc. 2006, 4, 14. [Google Scholar] [CrossRef] [Green Version]
- Karatas, M.; Karacan, I.; Tozan, H. An integrated multi-criteria decision making methodology for health technology assessment. Eur. J. Ind. Eng. 2018, 12, 504–534. [Google Scholar] [CrossRef]
- Goetghebeur, M.M.; Wagner, M.; Khoury, H.; Levitt, R.J.; Erickson, L.J.; Rindress, D. Evidence and Value: Impact on DEcisionMaking—The EVIDEM framework and potential applications. BMC Health Serv. Res. 2008, 8, 270–280. [Google Scholar] [CrossRef] [Green Version]
- Goetghebeur, M.M.; Wagner, M.; Khoury, H.; Rindress, D.; Grégoire, J.P.; Deal, C. Combining multicriteria decision analysis, ethics and health technology assessment: Applying the EVIDEM decision-making framework to growth hormone for Turner syndrome patients. Cost Eff. Resour. Alloc. 2010, 8, 1478–7547. [Google Scholar] [CrossRef] [Green Version]
- Miot, J.; Wagner, M.; Khoury, H.; Rindress, D.; Goetghebeur, M.M. Field testing of a multicriteria decision analysis (MCDA) framework for coverage of a screening test for cervical cancer in South Africa. Cost Eff. Resour. Alloc. 2012, 10, 1478–7547. [Google Scholar] [CrossRef] [Green Version]
- Garau, M.; Marsden, G.; Devlin, N.; Mazzanti, N.A.; Profico, A. Applying a Multicriteria Decision Analysis (MCDA) Approach to Elicit Stakeholders’ Preferences in Italy: The Case of Obinutuzumab for Rituximab-Refractory Indolent Non-Hodgkin Lymphoma (iNHL). PharmacoEconomics-Open 2018, 2, 153–163. [Google Scholar] [CrossRef] [Green Version]
- Badia, X.; Gil, A.; Shepher, J. MCDA EVIDEM reference value framework for drug evaluation and decision making in Spain. Value Health 2018, 21, S179. [Google Scholar] [CrossRef] [Green Version]
- Bhatt, G.D.; Zaveri, J. The enabling role of decision support systems in organizational learning. Decis. Support Syst. 2002, 32, 297–309. [Google Scholar] [CrossRef]
- Sprague, R.H. A Framework for the Development of Decision Support Systems. MIS Q. 1980, 4, 1–26. [Google Scholar] [CrossRef]
- STD Periton Diyalizinin Böbrek Yetmezliği Tedavisindeki Yeri. Sağlık Teknolojisi Değerlendirme Raporu. Available online: http://www.hta.gov.tr/pdf/PD%20STD-Raporu-ISBN-9789755906515.pdf (accessed on 29 September 2019).
- Marsh, K.; Goetghebeur, M.K.; Thokala, P.; Baltussen, R. Multi-Criteria Decision Analysis to Support Healthcare Decisions; Springer: Berlin/Heidelberg, Germany, 2017. [Google Scholar]
- Angelis, A.; Kanavos, P. Multiple Criteria Decision Analysis (MCDA) for evaluating new medicines in Health Technology Assessment and beyond: The Advance Value Framework. Soc. Sci. Med. 2017, 188, 137–156. [Google Scholar] [CrossRef] [Green Version]



| Main Criteria (1st Level) | 2nd Level | 3rd Level | 4th Level |
|---|---|---|---|
| Health problem and current use of technology | 4 | 8 | 14 |
| Description and technical characteristics of technology | 4 | 15 | 24 |
| Safety | 4 | 11 | 3 |
| Clinical effectiveness | 7 | 15 | 12 |
| Cost and economic evaluation | 6 | 6 | - |
| Ethical analysis | 5 | 15 | 15 |
| Organizational aspects | 5 | 14 | 13 |
| Social aspects | 3 | 10 | 24 |
| Legal aspects | 7 | 21 | 8 |
| Alternatives | Fuzzy Vikor | Fuzzy Topsis | Goal Programming |
|---|---|---|---|
| Peritoneal dialysis (PD) | 0.018 | 0.309 | 0.191 |
| Hemodialysis (HD) | 0.978 | 0.677 | 0.327 |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Öztürk, N.; Tozan, H.; Vayvay, Ö. A New Decision Model Approach for Health Technology Assessment and a Case Study for Dialysis Alternatives in Turkey. Int. J. Environ. Res. Public Health 2020, 17, 3608. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph17103608
Öztürk N, Tozan H, Vayvay Ö. A New Decision Model Approach for Health Technology Assessment and a Case Study for Dialysis Alternatives in Turkey. International Journal of Environmental Research and Public Health. 2020; 17(10):3608. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph17103608
Chicago/Turabian StyleÖztürk, Necla, Hakan Tozan, and Özalp Vayvay. 2020. "A New Decision Model Approach for Health Technology Assessment and a Case Study for Dialysis Alternatives in Turkey" International Journal of Environmental Research and Public Health 17, no. 10: 3608. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph17103608